15 March 2024: Database Analysis
Evaluating the Internal Anatomy of Maxillary Premolars in an Adult Saudi Subpopulation Using 2 Classifications: A CBCT-Based Retrospective Study
Mubashir Baig MirzaDOI: 10.12659/MSM.943455
Med Sci Monit 2024; 30:e943455






Abstract
BACKGROUND: Understanding the root canal morphology is important for successful endodontic treatment. This retrospective cone-beam computed tomography (CBCT) study aimed to compare the adult maxillary premolars (MP), root, and canal morphology among a Saudi Arabian subpopulation based on Vertucci and Ahmed classifications.
MATERIAL AND METHODS: Scans of 1336 MP – 656 first premolars (MFP) and 680 second premolars (MSP) – were analyzed for the number of roots, morphology of the canals, and symmetry among them. The data were grouped based on the traditional preestablished Vertucci system and newer instantaneous code-based Ahmed classification. Comparative analysis was done using the chi-square test.
RESULTS: Two roots were common in MFP with 84.4% of the population, followed by those with 1 root and those with 3 roots. In MSP, single roots were more common. The results were non-significant with P values of 0.859 and 0.471, respectively. Most of these MFP had Type IV Vertucci configuration/²TNB¹P¹ Ahmed et al code (TN-tooth number, B-buccal canal, P-palatal canal). In MSP, Type I Vertucci/¹TN¹ Ahmed et al code was most common. However, the results were not statistically significant for the PM with P values of 0.997 and 0.732, respectively. Sex-based difference among them for the roots and root canals was also non-significant. Symmetry among PM in opposite quadrants was 87.1% in MFP and 90% in MSP.
CONCLUSIONS: Two roots with Type IV (²TNB¹P¹) and 1 root with Type I (¹TN¹) were most common in MFP and MSP, respectively. Symmetry among opposing PM was high.
Keywords: Cone-Beam Computed Tomography, Dental Pulp Cavity, Endodontics, Root Canal Therapy, Bicuspid, Spiral Cone-Beam Computed Tomography, Retrospective Studies, Saudi Arabia, Tooth Root, Maxilla
Introduction
Many teeth undergo root canal treatment (RCT) worldwide with a high level of success owing to improved endodontic training and technological advancements [1]. Consistently updating knowledge is necessary because endodontics has seen some remarkable recent advances [1]. Increased use of nickel titanium alloys and simultaneous mechanized shaping of root canals have led many dentists to perform RCT [2]. Unfortunately, disparities related to knowledge, skill, and experience may lead to a high failure rate, especially in teeth with more complex root canal anatomies [2]. Moreover, missed root canals are one of the single greatest reasons for endodontists needing to perform retreatment [3]. Such situations can be handled better if the dentist is familiar with internal canal anatomies and variations seen in each tooth [4].
Different methods have been used to study the internal and external anatomies of the teeth, including in-vitro procedures like sectioning, staining, tooth clearing, micro-computed tomography, and in vivo procedures like radiography and cone-beam computed tomography (CBCT) [5]. However, the advent of CBCT has enhanced the diagnostic ability by providing a detailed 3D view of the internal structures, coupled with other advantages like non-invasiveness and ability to view the teeth and surrounding anatomy coronally, sagitally, and axially [6]. This has resulted in the widespread use of CBCT for diagnostic, prognostic, and research purposes, especially in the field of endodontics [6].
Vertucci identified 8 different canal morphologies (Types I–VIII) in 1974 based on the divisions of the main root canal starting from the pulp chamber to the apex [7]. In Type I, there is 1 canal starting from the chamber and ending as 1 canal at the apex. In Type II, 2 canals start from the chamber and merge into 1 before exiting the root at the apex. Type III has 1 canal starting from the chamber, splitting into 2 along its course, and merging into 1 before exiting the root at the apex. Type IV has 2 canals starting from the chamber and exiting as 2 at the apex. In Type V, there is 1 canal starting from the chamber, splitting into 2 along its course, and exiting as 2. Type VI has 2 canals starting from the chamber, merging into 1 along its path and then redividing into 2 before exiting the apex. Type VII has 1 canal starting from the chamber, splitting into 2 along its course, merging into 1 before splitting again into 2, then exiting the apex. Type VIII has 3 canals starting from the chamber, continuing, and exiting as 3 [7]. To accommodate additional morphologies to this classification, 14 new types (Type IX–XXII) were added to the Vertucci classification by Sert and Bayirli in 2004 [8]. Although widely accepted and straightforward in single-rooted teeth, it is more difficult to classify multi-rooted teeth with complex anatomies, which could result in misinterpretations [9]. Additionally, in many studies the morphology determined has been deemed to be non-classifiable [10].
The root canal morphologies have been extensively researched in populations throughout the world [11]. Even in Saudi Arabia, there is ample information on this topic, with various authors publishing in-depth analyses [12,13]. Although this classification still holds great significance and is followed throughout the world, newer classifications have evolved, which do not follow a predetermined type of canal configuration [14]. One such new classification system, created by Ahmed and Dummer in 2018, is more inclusive, specifying the number of roots along with the number of canals in each root from coronal to apical third without having to memorize the classification system per se [14,15]. This new classification system is promising and can describe the root and canal anatomy using a single code more accurately [16]. In the Vertucci system, single- and 2-rooted teeth with 2 canals from the orifice to the apex are classified as Type IV, whereas in the Ahmed et al system a code 1TN2 is given for single-rooted teeth having 2 canals, and a code 2TNB1P1 is given for teeth with 2 roots. TN represents the tooth number in the FDI system, the superscripted prefixed number represents the number of roots, B represents the buccal canal, with a superscripted number indicating the canal pattern from the orifice to the apex, and P represents the palatal canal with canal pattern number superscripted [17].
Most published research on root canal morphologies in Saudi Arabia compared and classified the teeth according to the Vertucci classification and only a few used the Ahmed et al classification [5,18–21]. Therefore, the present study aimed to identify and classify the canal morphologies of maxillary premolars (MP), compare the Vertucci and Ahmed classification systems, and check for symmetry among them in relation to opposing quadrants.
Material and Methods
ETHICS APPROVAL AND SAMPLE COLLECTION:
Prior to conducting the study, ethics approval was obtained from the Standing Committee of Bioethics Research (SCBR) SCBR-019-2022, Prince Sattam bin Abdulaziz University (PSAU). The record of all the patients treated between August 2016 to February 2023 who had previously undergone CBCT scans in the College of Dentistry, PSAU, for various diagnostic or prognostic reasons, were accessed with prior permissions from relevant authorities. The patients undergoing treatment at the dental college signed an informed consent for use of their radiographs for research purposes. A total of 1336 CBCT images of maxillary premolars were evaluated – 656 of those were first premolars and 680 were second premolars.
CBCT EXAMINATION:
All the images were taken using Carestream CS9300 CBCT (Carestream Dent LLC, Atlanta, GA, USA) with tube potential settings at 90 KV and current at 5.6 mA. The images had a 10x10 cm field of view (FOV) and a voxel size of 180–300 μm. The images were read using the RadiAnt Dicom viewer 2022.1.1 (Medixant, Poznan, Poland). Two endodontists with previous experience reading and classifying the root canal morphologies based on CBCT examined the scans. If a consensus was not reached between the 2 evaluators, a third evaluator who was an oral and maxillofacial radiologist opinion resolved the conflict.
INCLUSION CRITERIA:
Inclusion criteria were patients age 18–60 years, who had maxillary premolars that were not endodontically treated or restored with metallic/non-metallic/full coverage restorations.
EXCLUSION CRITERIA:
Exclusion criteria were internal resorptions and large periapical lesions resulting in apical root resorptions.
STATISTICAL ANALYSIS:
Cohens Kappa test used for checking the intra-operator variability, showing a value of 0.81, indicating a near perfect agreement. Comparative evaluation of the data related to the number of roots and canal morphologies according to both classifications as well as sex-based differences among them was done using the chi-square test. A
Results
MP ROOTS:
Table 1 shows the distribution of teeth according to the number of roots. The maxillary first premolars (MFP) were 2-rooted in 66.6% of the scans, followed by those with single roots in 31.7%, and 3 roots in 1.67% of the scans. Among the maxillary second premolars (MSP), 83.08% of the scans showed the presence of a single root, followed by 2 roots in 16.47%, and 3 roots in 0.45%. However, the results were not statistically significant. Regarding distribution of roots based on sex, single-rooted and 2-rooted teeth were more common in females, and males tended to have 3 roots in both MP, although the results were not statistically significant (Table 2).
ROOT CANAL MORPHOLOGY SEEN IN MFP:
The distribution of teeth according to Vertucci and Ahmed classification is seen in Table 3. In the MFP, 15.68% of the teeth were classified as Type I according to Vertucci classification and 1TN1 according to Ahmed classification, as seen in Figure 1A. We found that 6.7% of the teeth were classified as Type II according to Vertucci and 1TN2-1 according to Ahmed et al, as seen in Figure 1B. There were 1.06% of the teeth classified as Type III according to Vertucci and 1TN1-2-1 according to Ahmed et al as seen in Figure 1C. Type IV Vertucci accounted for 6.55% in single-rooted teeth and 66.35% in teeth with 2 roots, with a combined percentage of 72.9%, as seen in Figure 1D. These 2 are easily understood using the Ahmed et al classification, which classifies them as 1TN2 for single-rooted teeth and 2TNB1P1 for those with 2 roots. We found 1.67% of the teeth were classified as Type V according to Vertucci and 1TN1-2 according to Ahmed et al, as seen in Figure 1E. We found 0.3% of the teeth were classified as 2TNB1-2P1 according to Ahmed and Type XVI according to Sert and Bayirli (who added 14 new additions to the 8 types proposed by Vertucci), as seen in Figure 1F. We found 1.67% of the teeth were classified as Type VIII according to Vertucci and 3TNMB1DB1P1 according to Ahmed et al, as seen in Figure 1G.
ROOT CANAL MORPHOLOGY SEEN IN MSP:
In the MSP, a classification similar to MFP was reported. However, their percentages varied as seen in Table 3. Type I Vertucci, reported as 1TN1 by Ahmed et al was seen in 71.33% of the teeth. Type II Vertucci, classified by Ahmed et al. as 1TN2-1 was seen in 7.35% of the teeth. Type III Vertucci, classified as 1TN1-2-1 by Ahmed et al was seen in 0.87% of the teeth. Type IV Vertucci was seen in 1.47% in single-rooted teeth presented as 1TN2 by Ahmed et al and 16.74% in teeth with 2 roots presented as 2TNB1P1, with a combined percentage of 18.2%. Type V Vertucci, classified as 1TN1-2 by Ahmed et al, was seen in 1.16% of the teeth. Type XVI by Sert and Bayirli, classified as 2TNB1-2P1 by Ahmed et al was seen in 0.29% of the teeth and Type VIII Vertucci, classified as 3TNMB1DB1P1 by Ahmed et al was seen in 0.73% of the teeth.
SEX-BASED DIFFERENCES OF ROOT CANAL MORPHOLOGIES:
Although differences were seen between males and females when comparing the root canal classifications, the results were not statistically significant as seen in Table 4. Nonetheless, Types I, II and IV, pertaining to 1TN1, 1TN1-2, 1TN2, and 2TNB1P1 types showed greater tendency to occur in females compared to males in both MPs.
NECESSITY FOR USE OF NEW CLASSIFICATION:
The difference between 2TNB1P1 and 1TN2, which is classified as Type IV by Vertucci, can be appreciated better using the Ahmed classification system, as seen in Figure 2. The presence of the extra root and single canals in both the roots, as seen with 2TNB1P1, could be misinterpreted as a single-rooted teeth with 2 canals from orifice to apex. Similarly, 3TNMB1DB1P1 by Ahmed et al is interpreted as Type VIII by Vertucci, which could be misinterpreted as a single-rooted tooth with 3 canals. For the teeth classified as 214B1-2P1 by Ahmed, the Sert and Bayirli classification system is used and classified as Type XVI, which again does not take into consideration the presence of 2 roots.
SYMMETRY:
The scans with bilateral presence of MFP and MSP were evaluated; 318 scans included bilateral MFP, of which 87.1% were symmetrical. Similarly, 322 scans had bilateral MSP, of which 90% were symmetrical. A more detailed description of the symmetry regarding each classification is provided in Table 5. A CBCT image representation for the same is shown in Figure 3.
Discussion
In the present study 66.6% of the MFP were visualized to have 2 roots, 1 on the buccal side and the other in the palatal side. The results are in accordance to studies in India, Iraq, Poland, Qatar, and Brazil [22–26]. Lower percentages were reported in South Africans and Egyptians, with the lowest percentage (44.4%) reported in Yemen [27–29]. Among studies in Saudi Arabia, the presence of 2-rooted MFP was 54.5–75.1% [20,21,30]. These disparities could be related to the sample size, with only 69 MFP evaluated in 1 of the studies [21]. In addition, differences have also been previously reported among different subpopulations due to regional differences within the same population and diverse ethnicities [18]. The lower incidence of MFP with single roots seen in this study agrees with most other studies [22].
In MSP, 82.2% of the CBCT images had a single root, similar to Iraqi, Qatari, South African, Egyptian, Polish, and Spanish populations [23,25–28,31,32]. In other studies, among Saudis, the prevalence of single-rooted MSP is 71.5–83.2% [20,21,30]. The highest reported incidence of single-rooted MSP (96.7%) was seen among Pakistanis, but 54% was reported in Jordan [33,34]. However, this was a clinical study utilizing digital periapical radiographs and magnification with low power, which could explain the contrasting results. The incidence of 3-rooted MSP in this study was 0.45%, similar to those reported among Saudis [35]. Complete absence of 3 roots were noticed in Pakistani and Chinese populations [33,36].
In this study, Type IV and Type I Vertucci, pertaining to codes 2TNB1P1 and 1TN1 by Ahmed et al, was the most commonly seen in MFP and MSP, respectively. Similar results have been shown by Buchanon et al in South Africa, Aljawhar et al in Iraq, and Olczak et al in Poland when comparing the 2 classification systems [23,24,27,31]. Although Saber et al in Egypt reported a similar Type IV Vertucci and 2TNB1P1 Ahmed classification system in the MFP, their results differ from the aforementioned studies, which reported Type IV Vertucci with Ahmed et al codes 2TN2, 2TN1-2, 2TN2-1 were more common in MSP [28]. In other studies, which only reported classification by Vertucci, Type IV was the most commonly seen in MFP and Type I in MSP. However, unlike the Ahmed classification, it is difficult to predict whether the Type IV is in single-rooted teeth or 2-rooted ones. In a more recent critical evaluation of the classification systems, Ahmed et al reported that Ahmed and Vertucci classifications were identical for single-rooted teeth but differed in teeth with more than 1 root [16]. This problem was previously highlighted by Mirza et al in their study on maxillary molars and canines in the same population [5,18].
Although rare, both the maxillary premolars in this study had 3 canals, MFP 1.97%, and MSP 1.02%, which coincides closely with the data from a recent systematic analysis of studies in Saudi Arabia [13]. They were assigned either type VIII Vertucci and 3TNMB1DB1P1 code according to Ahmed et al for those with 3 roots or XVI Sert and Bayirli modification of Vertucci and 2TNB1-2P1 code according to Ahmed where 2 canals were present in the buccal root and a single canal in the palatal root. 3TNMB1DB1P1 was also previously reported in South African and Egyptian populations and 2TNB1-2P1 was reported in Poland and Egypt [24,27,28]. Additionally, Buchanon reported the presence of PM with 3 canals in fused roots and 3 canals with a C type configuration among South Africans [27].
Comparing between males and females, although higher percentages of single-rooted and 2-rooted premolars were seen in females and 3-rooted maxillary premolars were more common in males, but the difference was not statistically significant. The results agree with studies in Poland, Qatar, Spain, and in Saudi Arabia, where sex-based difference between the number of root and types of canals were not significant [24,25,30,32]. In contrast, differences were seen in a Chinese population, where the MP in males were 2-rooted more commonly than in females, and in the study by AlZubaidi et al among Saudis [20,37].
When the scans displaying bilateral symmetry in MFP were evaluated, 87.1% symmetry was observed among them with regards to root and canal morphology. The remaining 12.9% were asymmetrical. Similarly, when the scans for MSP were evaluated, 90% symmetry was observed. Comparable higher percentages of symmetry were reported in previous studies from Saudi Arabia [20,30].
The availability of a very large amount of data to analyze the root canal anatomies of the given population is a positive aspect of the study. However, this was a single-center study, and multi-center analysis would have given a wider prospective. The voxel size of 180–300 μm and 10×10 FOV of the scans present in the database are also limitations of the study, as higher voxel sizes reduce the diagnostic quality of scans. Clinically, the Ahmed et al classification of the root and canal anatomy is easily understood and defining the number of roots can help guide decision-making in various clinical endodontic treatment procedures.
Conclusions
MFP are usually 2-rooted, with Type IV Vertucci and 2TNB1P1 Ahmed et al classification being more common. In the MSP, single roots with Type I Vertucci 1TN1 were more common. Sex-based differences were not significant in the evaluated subpopulation in either the number of roots or types of root canals. Both classifications clearly described single-rooted teeth, but the Ahmed classification was better able to describe the teeth with more than 1 root. Bilateral symmetry was 87.1% in MFP and slightly higher (90%) in MSP.
Figures
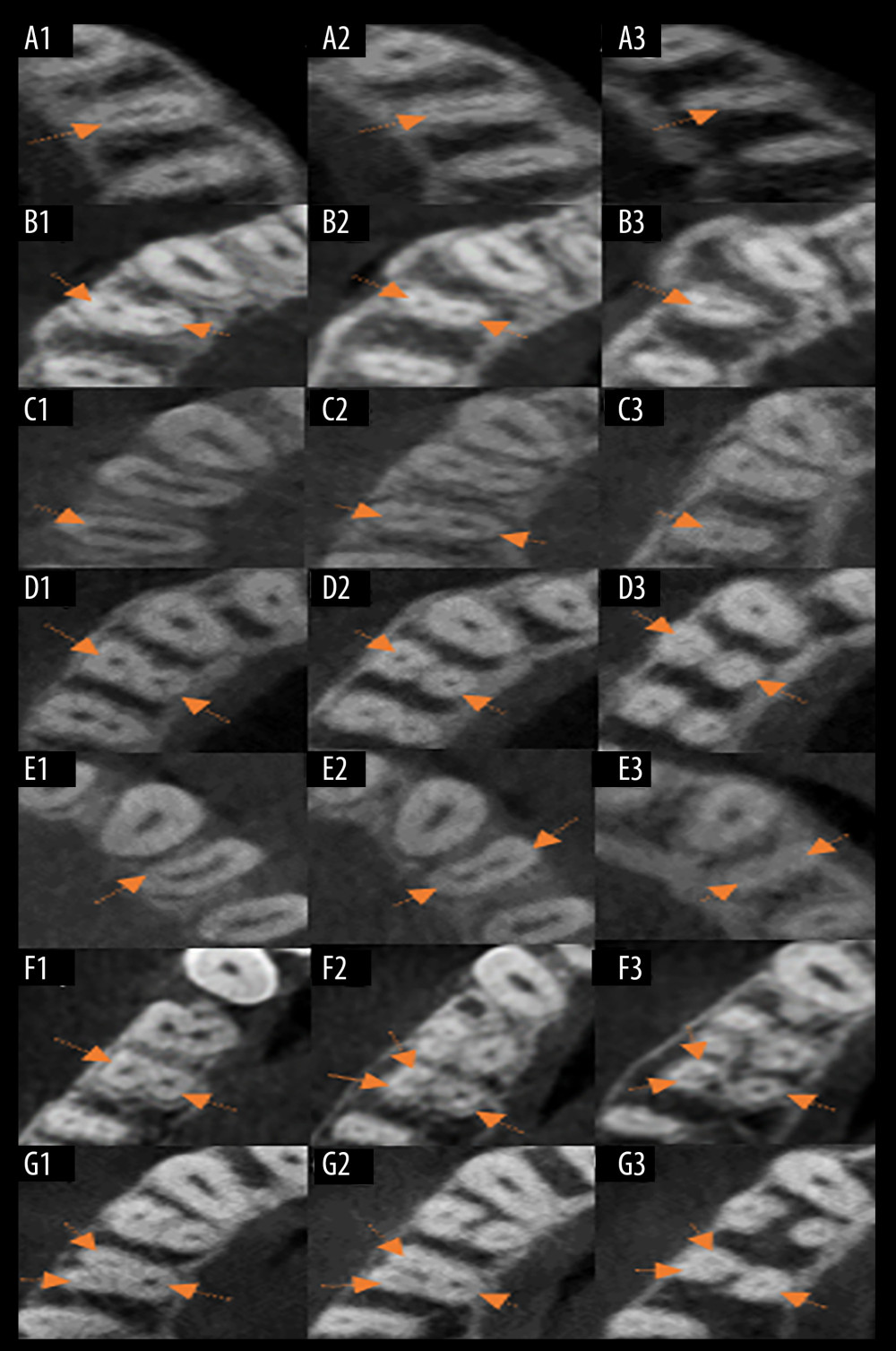 Figure 1. Representation of root canal classifications on axial view of CBCT. (A1–A3) Presence of single canals in the coronal, middle, and apical thirds indicated by arrows, classified as Vertucci Type I and 1TN1 Ahmed. (B1, B2) Two canals in the coronal and middle third. (B3) Only 1 canal in the apical third, indicated by arrows, classified as Type II Vertucci and 1TN2-1 Ahmed. (C1) One canal in the coronal third. (C2) Two canals in the middle third. (C3) One canal in the apical third indicated by arrows, classified as Type III Vertucci and 1TN1-2-1 Ahmed. (D1–D3) Two canals in the coronal, middle, and apical thirds indicated by arrows, classified as Type IV Vertucci and 2TNB1P1 Ahmed. (E1) One canal in the coronal third. (E2, E3) Two canals in the middle and apical third indicated by arrows, classified as Type V Vertucci and 1TN1-2 Ahmed. (F1) Two canals buccal and palatal in coronal third. (F2, F3) Two canals in buccal and 1 canal in palatal root in middle and apical thirds, indicated by arrows, classified as 2TNB1-2P1 according to Ahmed and Type XVI according to Sert and Bayirli. (G1–G3) Three canals in coronal, middle, and apical third indicated by arrows, classified as Type VIII Vertucci and 3TNMB1DB1P1Ahmed.
Figure 1. Representation of root canal classifications on axial view of CBCT. (A1–A3) Presence of single canals in the coronal, middle, and apical thirds indicated by arrows, classified as Vertucci Type I and 1TN1 Ahmed. (B1, B2) Two canals in the coronal and middle third. (B3) Only 1 canal in the apical third, indicated by arrows, classified as Type II Vertucci and 1TN2-1 Ahmed. (C1) One canal in the coronal third. (C2) Two canals in the middle third. (C3) One canal in the apical third indicated by arrows, classified as Type III Vertucci and 1TN1-2-1 Ahmed. (D1–D3) Two canals in the coronal, middle, and apical thirds indicated by arrows, classified as Type IV Vertucci and 2TNB1P1 Ahmed. (E1) One canal in the coronal third. (E2, E3) Two canals in the middle and apical third indicated by arrows, classified as Type V Vertucci and 1TN1-2 Ahmed. (F1) Two canals buccal and palatal in coronal third. (F2, F3) Two canals in buccal and 1 canal in palatal root in middle and apical thirds, indicated by arrows, classified as 2TNB1-2P1 according to Ahmed and Type XVI according to Sert and Bayirli. (G1–G3) Three canals in coronal, middle, and apical third indicated by arrows, classified as Type VIII Vertucci and 3TNMB1DB1P1Ahmed. 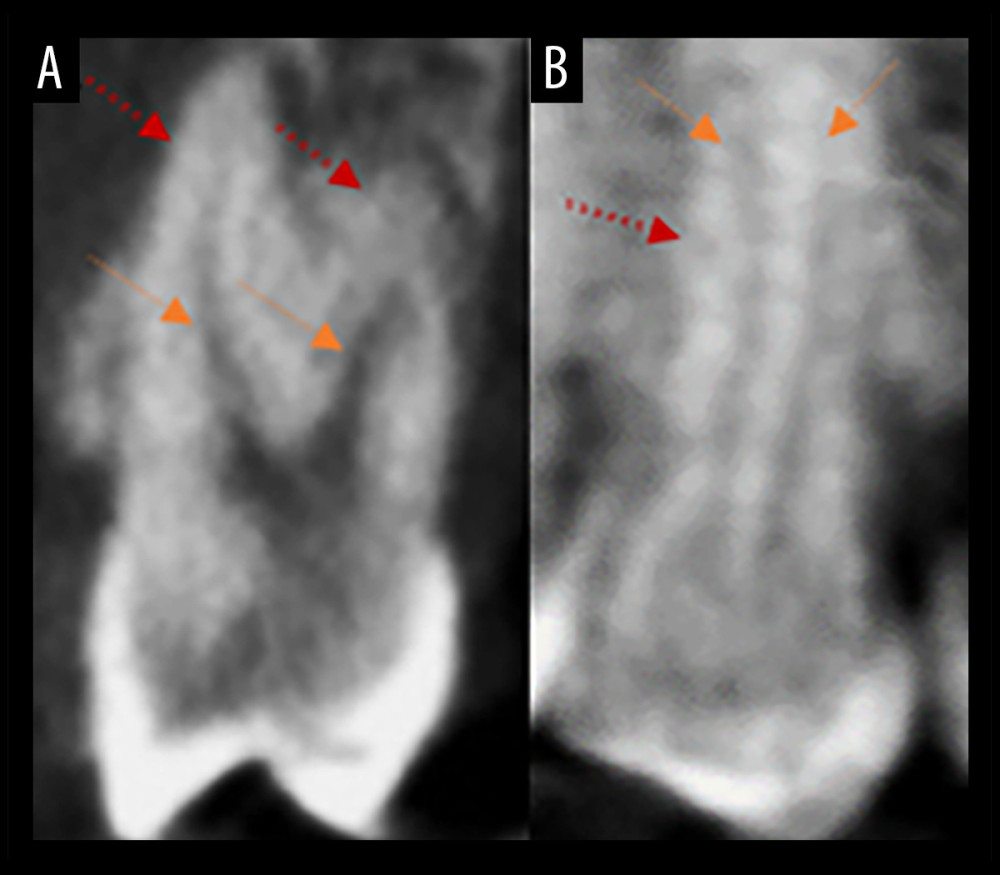 Figure 2. Need for use of Ahmed classification. (A) Two roots with 2 canals. (B) Two 2 canals in 1 root (root indicated by red arrows and canals indicated by orange arrows).
Figure 2. Need for use of Ahmed classification. (A) Two roots with 2 canals. (B) Two 2 canals in 1 root (root indicated by red arrows and canals indicated by orange arrows). 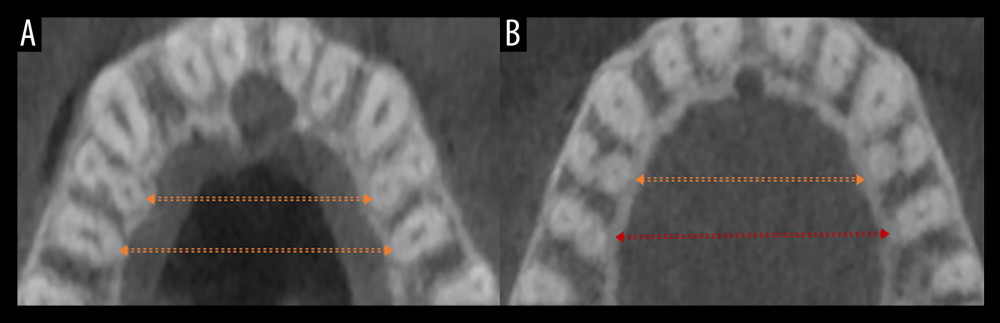 Figure 3. Bilateral symmetry among opposing quadrants. (A) Symmetrical root and root canal classification in both maxillary first premolars (MFP) and maxillary second premolars (MSP). (B) Symmetry among MFP but asymmetrical root and canal classification among bilateral MSP. The arrows (orange) indicate symmetry and arrow (Red) indicates asymmetry.
Figure 3. Bilateral symmetry among opposing quadrants. (A) Symmetrical root and root canal classification in both maxillary first premolars (MFP) and maxillary second premolars (MSP). (B) Symmetry among MFP but asymmetrical root and canal classification among bilateral MSP. The arrows (orange) indicate symmetry and arrow (Red) indicates asymmetry. Tables
Table 1. Distribution of maxillary premolars according to number of roots.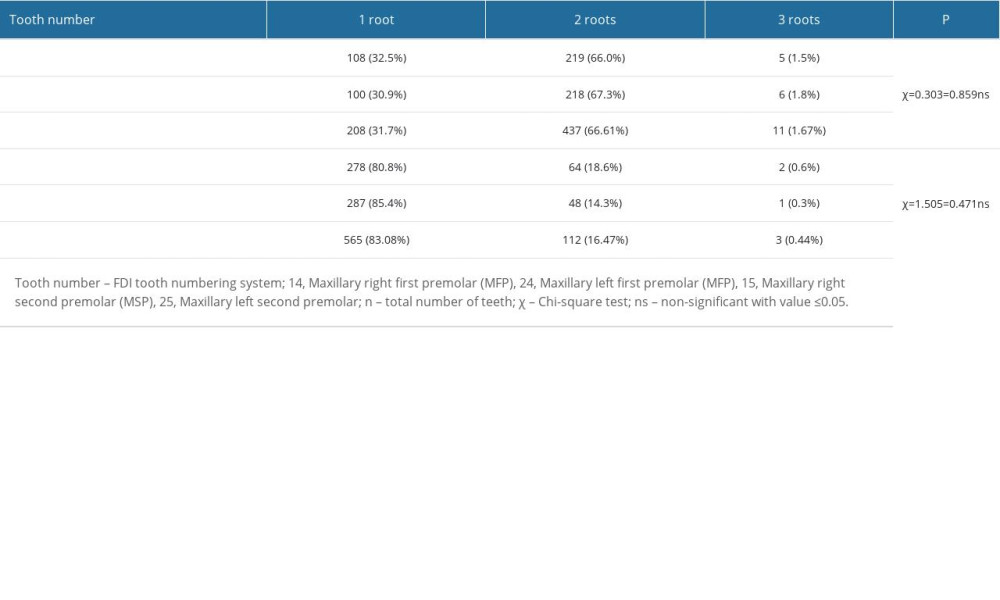 Table 2. Sex-based distribution of maxillary premolars according to number of roots.
Table 2. Sex-based distribution of maxillary premolars according to number of roots.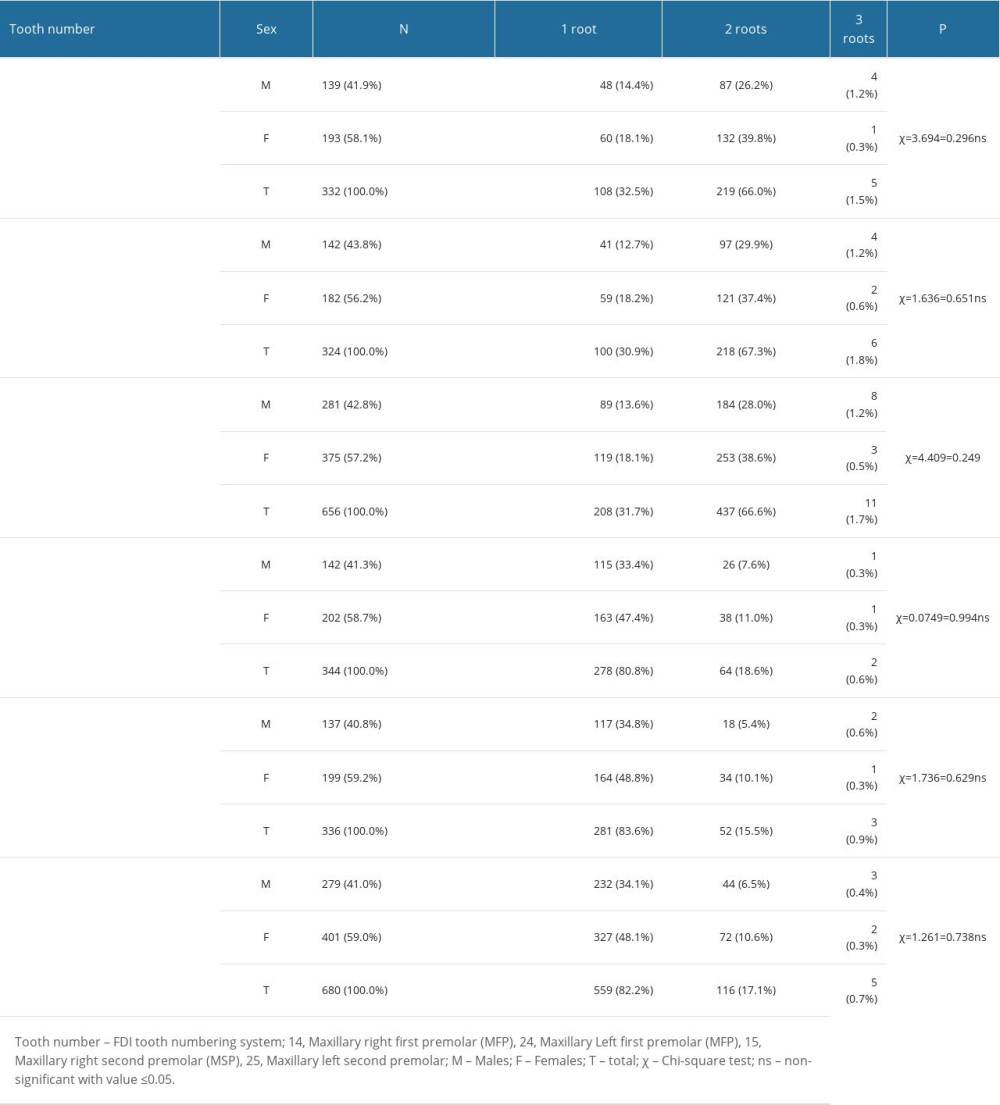 Table 3. Classification of root canal morphology of Maxillary Premolars – Ahmed et al and Vertucci.
Table 3. Classification of root canal morphology of Maxillary Premolars – Ahmed et al and Vertucci.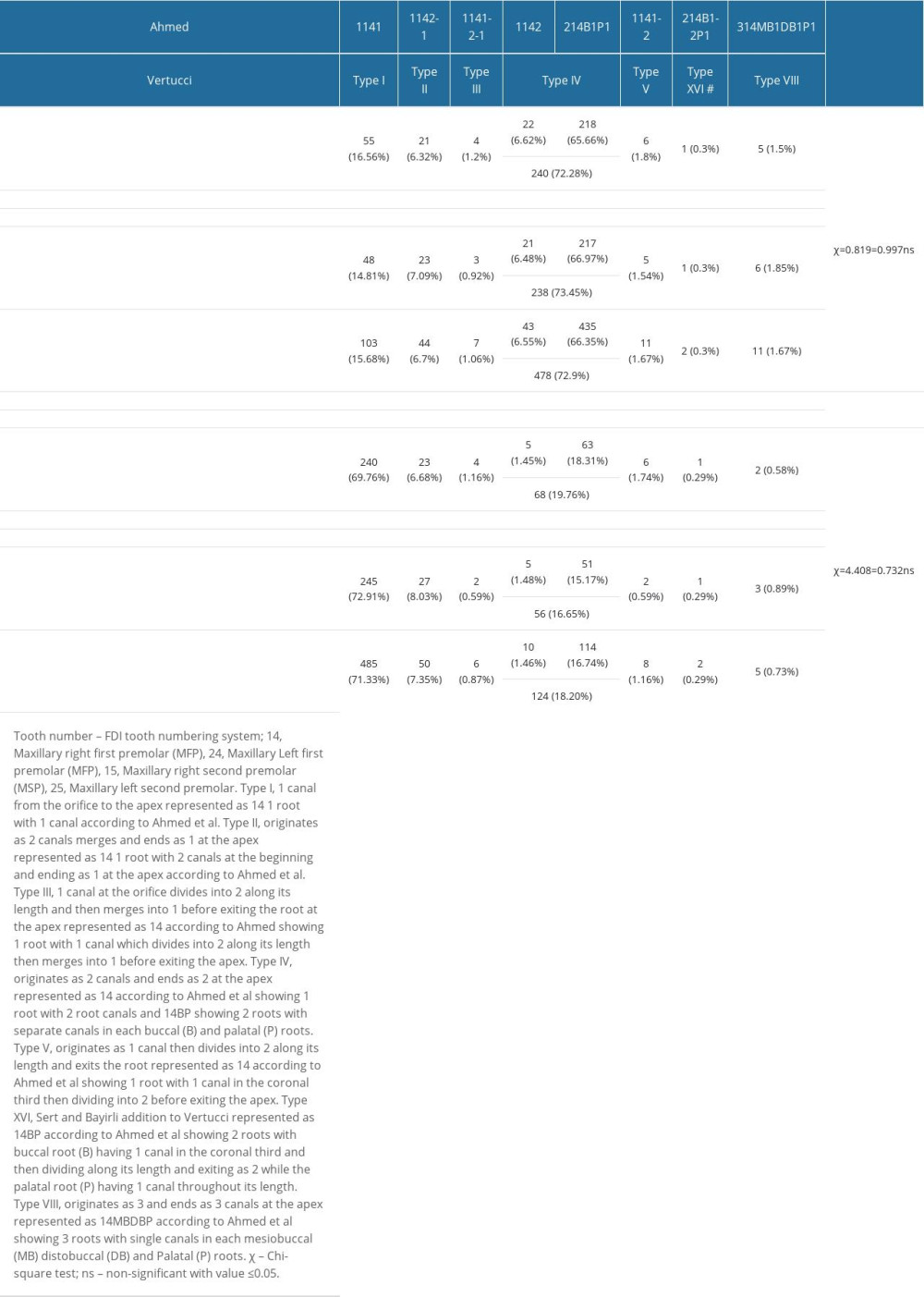 Table 4. Sex-based distribution of root canal morphology of maxillary premolars – Ahmed et al and Vertucci.
Table 4. Sex-based distribution of root canal morphology of maxillary premolars – Ahmed et al and Vertucci.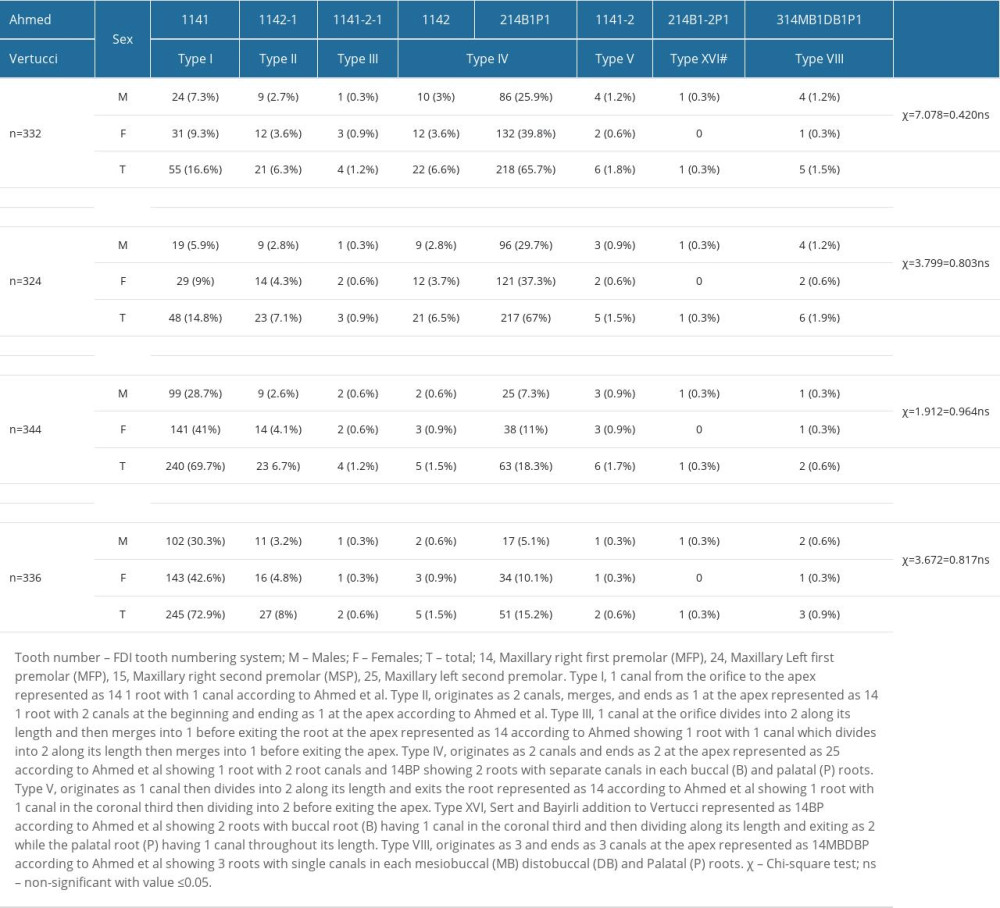 Table 5. Bilateral symmetry of maxillary premolars.
Table 5. Bilateral symmetry of maxillary premolars.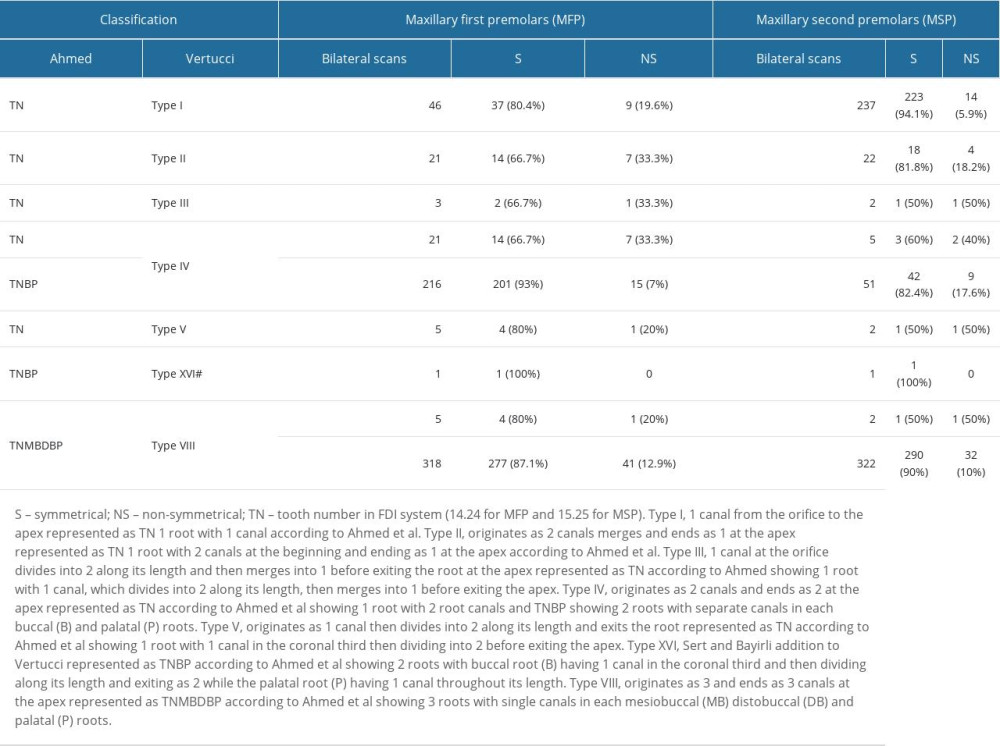
References
1. Kishen A, Peters OA, Zehnder M, Advances in endodontics: Potential applications in clinical practice: J Conserv Dent, 2016; 19; 199-206
2. Fezai H, Al-Salehi S, The relationship between endodontic case complexity and treatment outcomes: J Dent, 2019; 85; 88-92
3. Witherspoon DE, Small JC, Regan JD, Missed canal systems are the most likely basis for endodontic retreatment of molars: Tex Dent J, 2013; 130; 127-39
4. Yang H, Tian C, Li G, A cone-beam computed tomography study of the root canal morphology of mandibular first premolars and the location of root canal orifices and apical foramina in a Chinese subpopulation: J Endod, 2013; 39; 435-38
5. Mirza MB, Evaluation of root and canal morphologies of permanent canines in a Saudi Arabian sub population using cone-beam computed tomography: J Dent Sci, 2022; 17; 1626-33
6. Patel S, Brown J, Pimentel T, Cone beam computed tomography in Endodontics – a review of the literature: Int Endod J, 2019; 52; 1138-52
7. Vertucci F, Seelig A, Gillis R, Root canal morphology of the human maxillary second premolar: Oral Surg Oral Med Oral Pathol, 1974; 38; 456-64
8. Sert S, Bayirli GS, Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population: J Endod, 2004; 30; 391-98
9. Ahmed HMA, Che Ab Aziz ZA, Azami NH, Application of a new system for classifying root canal morphology in undergraduate teaching and clinical practice: A national survey in Malaysia: Int Endod J, 2020; 53; 871-79
10. Filpo-Perez C, Bramante CM, Villas-Boas MH, Micro-computed tomographic analysis of the root canal morphology of the distal root of mandibular first molar: J Endod, 2015; 41; 231-36
11. Karobari MI, Parveen A, Mirza MB, Root and root canal morphology classification systems: Int J Dent, 2021; 2021; 6682189
12. Mashyakhy M, AlTuwaijri N, Alessa R, Anatomical evaluation of root and root canal morphology of permanent mandibular dentition among the Saudi Arabian population: A systematic review: Biomed Res Int, 2022; 2022; 2400314
13. Mashyakhy M, Awawdeh M, Abu-Melha A, Anatomical evaluation of root and root canal configuration of permanent maxillary dentition in the population of the Kingdom of Saudi Arabia: Biomed Res Int, 2022; 2022; 3428229
14. Ahmed HMA, Dummer PMH, A new system for classifying tooth, root and canal anomalies: Int Endod J, 2018; 51; 389-404
15. Ahmed HMA, Versiani MA, De-Deus G, Dummer PMH, A new system for classifying root and root canal morphology [published erratum appears in Int Endod J. 2018;51:1184]: Int Endod J, 2017; 50; 761-70
16. Ahmed HMA, Rossi-Fedele G, Dummer PMH, Critical analysis of a new system to classify root and canal morphology – a systematic review: Aust Endod J, 2023; 10; 12780
17. Ahmed HM, Keleş A, Martins JN, Dummer PM: Tooth, root, and canal anatomy endodontic advances and evidence-based clinical guidelines, 2022; 1-50, John Wiley & Sons Ltd
18. Mirza MB, Gufran K, Alhabib O, CBCT based study to analyze and classify root canal morphology of maxillary molars – a retrospective study: Eur Rev Med Phar Sci, 2022; 26; 6550-60
19. Karobari MI, Iqbal A, Syed J, Evaluation of root and canal morphology of mandibular premolar amongst Saudi subpopulation using the new system of classification: A CBCT study: BMC Oral Health, 2023; 23; 291
20. Al-Zubaidi SM, Almansour MI, Al Mansour NN, Assessment of root morphology and canal configuration of maxillary premolars in a Saudi subpopulation: A cone-beam computed tomographic study: BMC Oral Health, 2021; 21; 397
21. Alshammari SM, Ganji KK, Albulayhid AA, Prevalence of second root and root canal in mandibular and maxillary premolars based on two classification systems in sub-population of Northern Region (Saudi Arabia) assessed using cone beam computed tomography (CBCT): A retrospective study: Diagnostics (Basel), 2023; 13; 498
22. Khanna S, Jobanputra L, Mehta J, Revisiting premolars using cone-beam computed tomography analysis and classifying their roots and root canal morphology using newer classification: Cureus, 2023; 15; e38623
23. Aljawhar AM, Ibrahim N, Abdul Aziz A, Characterization of the root and canal anatomy of maxillary premolar teeth in an Iraqi subpopulation: A cone beam computed tomography study: Odontology, 2023 [Online ahead of print]
24. Olczak K, Pawlicka H, Szymański W, Root form and canal anatomy of maxillary first premolars: a cone-beam computed tomography study: Odontology, 2022; 110; 365-75
25. Diab H, Al-Sheeb F, Diab A, Marouf N, A cone-beam computed tomography (CBCT) study of root anatomy, canal morphology and bilateral symmetry of permanent maxillary premolar teeth among the Qatari subpopulation: Open Dent J, 2022; 16; e187421062204260
26. Lemos MC, Coutinho TM, Perez AR, Root canal morphology of 1316 premolars from Brazilian individuals: An in vivo analysis using c1-beam computed tomography: Acta Odontol Latinoam, 2022; 35; 105-10
27. Buchanan GD, Gamieldien MY, Tredoux S, Vally ZI, Root and canal configurations of maxillary premolars in a South African subpopulation using cone beam computed tomography and two classification systems: J Oral Sci, 2020; 62; 93-97
28. Saber SEDM, Ahmed MHM, Obeid M, Ahmed HMA, Root and canal morphology of maxillary premolar teeth in an Egyptian subpopulation using two classification systems: A cone beam computed tomography study: Int Endod J, 2019; 52; 267-78
29. Senan EM, Alhadainy HA, Genaid TM, Madfa AA, Root form and canal morphology of maxillary first premolars of a Yemeni population: BMC Oral Health, 2018; 18; 94
30. Alqedairi A, Alfawaz H, Al-Dahman Y, Cone-beam computed tomographic evaluation of root canal morphology of maxillary premolars in a Saudi population: Biomed Res Int, 2018; 2018; 8170620
31. Olczak K, Pawlicka H, Szymański W, Root and canal morphology of the maxillary second premolars as indicated by cone beam computed tomography: Aus Endod J, 2023; 49; 92-103
32. Abella F, Teixidó LM, Patel S, Cone-beam computed tomography analysis of the root canal morphology of maxillary first and second premolars in a Spanish population: J Endod, 2015; 41; 1241-47
33. Alkahtany MF, Ali S, Khabeer A, A microcomputed tomographic evaluation of root canal morphology of maxillary second premolars in a Pakistani cohort: Applied Sciences, 2021; 11; 5086
34. Al-Ghananeem MM, Haddadin K, Al-Khreisat AS, The number of roots and canals in the maxillary second premolars in a group of Jordanian population: Int J Dent, 2014; 2014; 797692
35. Chourasia HR, Odabi AI, Owis AA, Evaluation of root canal morphology of maxillary second premolars and its relation to maxillary sinus in a Saudi Arabian population: J Contemp Dent Pract, 2023; 24; 35-41
36. Shi ZY, Hu N, Shi XW, Root canal morphology of maxillary premolars among the elderly: Chin Med J, 2017; 130; 2999-3000
37. Cheng Xiao L, Weng YL, Observation of the roots and root canals of 442 maxillary first premolars: Shanghai J Stomatol, 2008; 17; 525-28
Figures
Figure 1. Representation of root canal classifications on axial view of CBCT. (A1–A3) Presence of single canals in the coronal, middle, and apical thirds indicated by arrows, classified as Vertucci Type I and 1TN1 Ahmed. (B1, B2) Two canals in the coronal and middle third. (B3) Only 1 canal in the apical third, indicated by arrows, classified as Type II Vertucci and 1TN2-1 Ahmed. (C1) One canal in the coronal third. (C2) Two canals in the middle third. (C3) One canal in the apical third indicated by arrows, classified as Type III Vertucci and 1TN1-2-1 Ahmed. (D1–D3) Two canals in the coronal, middle, and apical thirds indicated by arrows, classified as Type IV Vertucci and 2TNB1P1 Ahmed. (E1) One canal in the coronal third. (E2, E3) Two canals in the middle and apical third indicated by arrows, classified as Type V Vertucci and 1TN1-2 Ahmed. (F1) Two canals buccal and palatal in coronal third. (F2, F3) Two canals in buccal and 1 canal in palatal root in middle and apical thirds, indicated by arrows, classified as 2TNB1-2P1 according to Ahmed and Type XVI according to Sert and Bayirli. (G1–G3) Three canals in coronal, middle, and apical third indicated by arrows, classified as Type VIII Vertucci and 3TNMB1DB1P1Ahmed.Figure 2. Need for use of Ahmed classification. (A) Two roots with 2 canals. (B) Two 2 canals in 1 root (root indicated by red arrows and canals indicated by orange arrows).Figure 3. Bilateral symmetry among opposing quadrants. (A) Symmetrical root and root canal classification in both maxillary first premolars (MFP) and maxillary second premolars (MSP). (B) Symmetry among MFP but asymmetrical root and canal classification among bilateral MSP. The arrows (orange) indicate symmetry and arrow (Red) indicates asymmetry. Tables
Table 1. Distribution of maxillary premolars according to number of roots.Table 2. Sex-based distribution of maxillary premolars according to number of roots.Table 3. Classification of root canal morphology of Maxillary Premolars – Ahmed et al and Vertucci.Table 4. Sex-based distribution of root canal morphology of maxillary premolars – Ahmed et al and Vertucci.Table 5. Bilateral symmetry of maxillary premolars.Table 1. Distribution of maxillary premolars according to number of roots.Table 2. Sex-based distribution of maxillary premolars according to number of roots.Table 3. Classification of root canal morphology of Maxillary Premolars – Ahmed et al and Vertucci.Table 4. Sex-based distribution of root canal morphology of maxillary premolars – Ahmed et al and Vertucci.Table 5. Bilateral symmetry of maxillary premolars. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387