01 March 2024: Clinical Research
Diagnostic Accuracy of Ileocolic Artery and Vein Diameter for Acute Appendicitis
Bahadir KartalDOI: 10.12659/MSM.943846
Med Sci Monit 2024; 30:e943846






Abstract
BACKGROUND: Regional inflammation-induced local vasodilation may exist in cases of appendicitis. In this study, the diameters of the ileocolic artery (ICA) and ileocolic vein (ICV) were measured using contrast-enhanced abdominal computed tomography (CT) scans in acute appendicitis cases. The study aimed to measure the diagnostic value of these measurements in the diagnosis of acute appendicitis.
MATERIAL AND METHODS: A total of 508 patients, including those with a diagnosis of acute appendicitis and a control group without appendicitis, were systematically evaluated. In all cases, the appendix was analyzed simultaneously on axial and coronal CT sections, and all measurement procedures were conducted with an electronic ruler after the actual images were magnified. Measurements of the ICA and ICV diameters were taken from the proximal 2-cm segments of the superior mesenteric artery and superior mesenteric vein in the axial plane. Demographic information, sex distribution, and ICA and ICV diameters were collected.
RESULTS: Of the 508 patients, 53.74% were men, and 46.26% were women. ICA and ICV diameters were significantly increased in the appendicitis group (P<0.001). Binomial logistic regression confirmed the independent predictive value of ICA and ICV diameters. Receiver operating characteristic curve analysis determined optimal cut-off values for distinguishing between the non-appendicitis and appendicitis groups (ICA: 2.475 mm, ICV: 3.885 mm) with high sensitivity and specificity.
CONCLUSIONS: ICA and ICV diameter measurements, in conjunction with major radiological findings, can enhance diagnostic accuracy in acute appendicitis cases. The use of ICA and ICV diameter measurements in diagnosing acute appendicitis offers a novel perspective in clinical practice.
Keywords: appendicitis, Abdomen, Acute, Diagnosis, Mesenteric Artery, Superior, Mesenteric Veins, computed tomography angiography
Background
Situated in the lower right quadrant of the abdomen, the appendix is a tubular, cul-de-sac structure connected to the posteromedial extremity of the cecum [1]. A healthy appendix typically exhibits a diameter below 6 mm, although it has the potential to measure up to 11 mm [2]. The appendicular artery, a terminal branch of the ileocolic artery (ICA), serves as the blood supply to the appendix, while venous drainage is facilitated by appendicular veins that converge into the ileocolic vein (ICV) [3].
Appendicitis is most frequently observed between the ages of 5 and 45 years, with a mean age of 28 years and an incidence of around 233 per 100 000 individuals. Male patients exhibit a slightly higher predisposition than do female patients, with lifetime incidence rates of 8.6% and 6.7%, respectively [4].
Acute appendicitis typically occurs due to an obstruction in the appendiceal lumen, often caused by an appendicolith or other mechanical factors, such as tumors, parasites, or hypertrophied lymphatic tissue. Obstruction in appendicitis causes increased pressure within the appendix, leading to vessel occlusion and lymphatic stasis [5]. Without treatment, inflammation progresses, risking perforation and abscess formation. The treatment of acute appendicitis is surgical.
Acute appendicitis stands out as a prevalent cause of sudden abdominal pain, constituting a prominent condition necessitating abdominal surgery [6]. While historical, physical, and laboratory assessments play pivotal roles in diagnosing acute appendicitis, imaging techniques are instrumental in achieving precise diagnoses and mitigating mortality and morbidity by steering clear of unwarranted surgeries in patients without acute appendicitis [6–8].
Computed tomography (CT) findings signaling acute appendicitis involve an increased transverse diameter of the appendix (surpassing 6 mm from outer wall to outer wall), thickening with contrast enhancement in the appendix wall, and identification of periappendicular inflammation [9,10]. This includes heightened periappendicular density, the formation of abscesses, and the enlargement of pericecal lymph nodes [9–11]. In instances of acute appendicitis, CT examinations can also assess hyperemia and vascular congestion in the periappendicular region, stemming from regional inflammation [9].
Infection causes blood flow in the appendix wall and periappendiceal tissue to increase. It is hypothesized that the diameter of the ileocolic artery and vein might be increased in acute appendicitis due to increased blood flow in the appendix wall in case of acute appendicitis.
Therefore, this study aimed to evaluate ICA and ICV diameter measured using contrast-enhanced CT in 508 patients with and without acute appendicitis.
Material and Methods
PATIENT CHARACTERISTICS:
This study received ethical approval from the Institutional Review Board of the Hitit University Faculty of Medicine Clinical Research Ethics Committee (protocol number: 2023–57). Informed consent was acquired from all participants involved in the research.
A systematic evaluation was conducted on patients who received a diagnosis of appendicitis and were treated by the Department of General Surgery at Erol Olçok Training and Research Hospital, as well as participants in the control group, between January 2022 and December 2023. The appendicitis group comprised individuals aged between 18 and 70 years who presented to the Emergency Department with abdominal pain, received a diagnosis of acute appendicitis, underwent surgery, had no known hematological, oncological, vascular, or endothelial diseases, and exhibited radiological imaging findings. The control group consisted of individuals under 18 and over 70 years of age who presented to the Emergency Department with abdominal pain but not acute appendicitis, had no known hematological, oncological, vascular, or endothelial diseases, and exhibited radiological CT imaging findings. Individuals over 18 and under 70 years of age, those with known hematological, oncological, vascular, or endothelial diseases, and patients without available radiological imaging findings were excluded from the study. A total of 508 patients were included in the study after applying these exclusion criteria. Demographic information, sex distribution, and measurements of the ICA and ICV diameters of patients with appendicitis were collected during the retrospective analysis.
CT EXAMINATION:
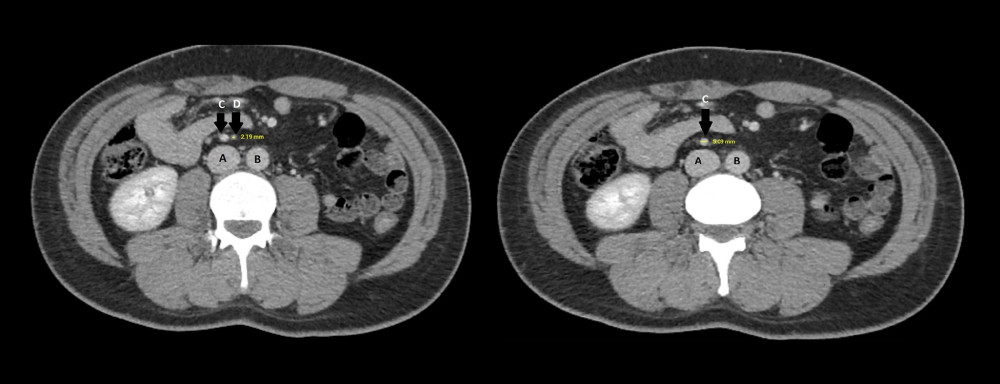
We obtained postoperative appendicitis pathology results from the archival system. The CT images of patients with appendicitis were reviewed through the hospital picture archiving and communication system (Akgün Healthcare, Çorum, Turkey). CT scans were administered to all patients following intravenous injection of contrast material; the injection rate averaged 2 to 3 mL/s, and portal venous phase images were obtained with a delay of 50 to 60 mL/s after the initiation of contrast injection. CT scans were performed from the hepatic dome to the pelvic floor using online dose modulation with a 128×0.6-mm collimation, 5-mm slice thickness, a pitch of 1.0, and 120 or 140 kVp tube voltage. In all cases, the appendix was concurrently examined on axial and coronal CT sections, and all measurement procedures were conducted using an electronic ruler after magnifying the actual images. The ICA and ICV diameters were measured in the axial plane from the proximal 2-cm segments of the superior mesenteric artery and superior mesenteric vein, respectively (Figure 1).
STATISTICAL ANALYSIS:
This study was designed retrospectively. All statistical analyses were conducted using IBM SPSS Statistics for Windows software (version 26; IBM Corp, Armonk, NY, USA). Descriptive statistics were reported for categorical variables as counts and percentages and for numerical variables as median±interquartile range. The normal distribution of data was assessed using the Shapiro-Wilk test. Correlations between variables were evaluated using Pearson and Spearman correlation coefficients, depending on the data distribution. Comparisons of numerical measurements between independent groups according to research groups, such as age, artery diameter, and vein diameter, were assessed using the Mann-Whitney U test, considering the distribution of the data. Sex, a categorical variable, was evaluated for ratio comparisons between research groups using the chi-square test. The interaction between variables was assessed using binomial logistic regression analysis, and the independent predictive value of ICA and ICV diameter was evaluated. Receiver operating characteristic (ROC) curves were used to demonstrate the discriminative ability of statistically significant variables. Cut-off values for these markers were determined using the area under the curve and the Youden index. Sensitivity, specificity, positive predictive value, negative predictive value, and accuracy values were calculated based on these cut-off values. Odds ratio (OR) values were computed for these cut-off points. A significance level of
Results
DESCRIPTIVE ANALYSIS:
Of the total 508 patients, 273 (53.74%) were men, and 235 (46.26%) were women. The median age was 36±22 years. Patients were categorized into 2 groups: non-appendicitis (n=250) and appendicitis (n=258). A statistically significant difference was observed in the sex distribution between the 2 groups, with a female percentage of 59.20% in the non-appendicitis group and 33.72% in the appendicitis group (P<0.001). When assessed in terms of mean ages, the median age in the non-appendicitis group was 36±22 years, while in the appendicitis group, it was 37±21 years; however, no statistically significant difference was observed (P=0.820; Table 1).
The ICA median diameter for the non-appendicitis group was 1.93±0.41 mm, while the median for the appendicitis group was 3.2±0.71 mm, indicating a statistically significant difference (
MULTIVARIATE ANALYSIS:
In a multivariate analysis incorporating age, sex, ICA diameter, and ICV diameter as covariates, no significant differences in sex between the groups were observed (P=0.576). Although age demonstrated significance in the univariate analysis, it was not significant in the multivariate analysis (P=0.992; Table 1). The binomial logistic regression model accurately classified 94.5% of cases (Nagelkerke R2=0.898, P<0.001). ICA and ICV remained as independent predictors even after adjusting for potential confounders in the multivariate analysis (OR with 95% CI 128.901 (29.51–563.038), P<0.001 for ICA, and 12.687 (4.775–33.706), P<0.001 for ICV).
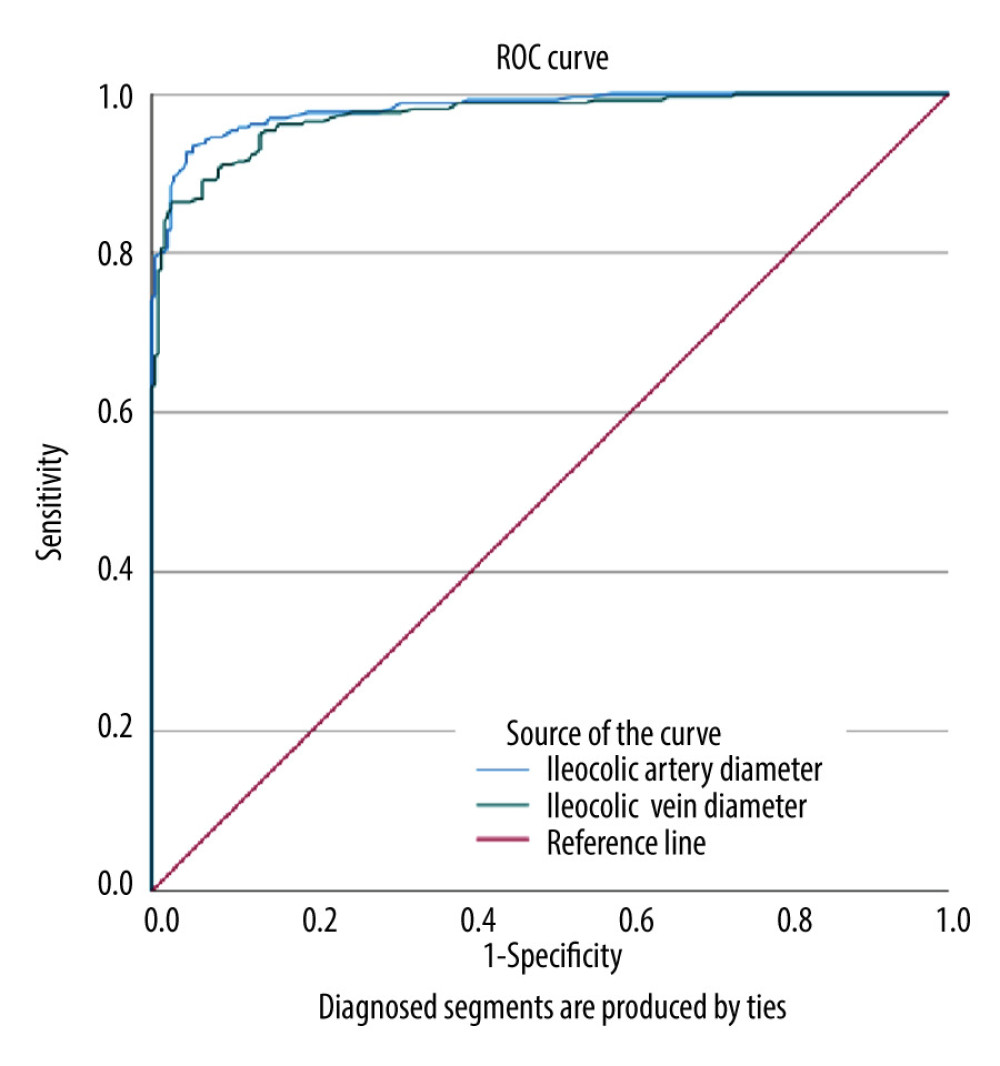
To assess the optimal values of ICA and ICV diameters for distinguishing between non-appendicitis and appendicitis groups, the area under the curve and the Youden index were employed in ROC analysis (Table 2). For the diagnosis of appendicitis, the most suitable ICA cut-off value was determined to be 2.475 mm, with 92.6% sensitivity, 95.6% specificity, 95.6% positive predictive value, 92.6% negative predictive value, and 94.09% test accuracy (OR 273.306, 95% CI 127.318–586.691, P<0.001). Similarly, the optimal ICV cut-off value was 3.885 mm with 86.4% sensitivity, 97.6% specificity, 97.4% positive predictive value, 87.5% negative predictive value, and 91.92% test accuracy (OR 259.105, 95% CI 106.952–627.716, P<0.001).
The use of both cut-off values as criteria for a positive diagnosis of appendicitis demonstrated an ability to diagnose the condition with 83.3% sensitivity, 99.2% specificity, 99.1% positive predictive value, 85.2% negative predictive value, and 91.14% test accuracy (OR 620, 95% CI 148.448–2589.448, P<0.001; Figure 2). An ICA exceeding 2.475 mm increased the likelihood of appendicitis by approximately 272 times, while an ICV exceeding 3.885 mm increased this likelihood by approximately 258 times. The simultaneous positivity of both criteria increased the likelihood by 619 times.
Discussion
In our study, the measurements of ICA and ICV diameters were statistically significantly higher in patients with acute appendicitis than in those without. We believe that these measurements could be a valuable addition to the tomographic findings in patients suspected of having acute appendicitis.
Acute appendicitis is one of the most commonly encountered and important diseases requiring emergency surgery in cases referred to the Emergency Department because of abdominal pain [12]. In cases presenting with typical clinical signs, a diagnosis of acute appendicitis can be made based on clinical and laboratory findings. However, if there are atypical clinical and examination signs, screening methods are necessary to support the diagnosis. Acute appendicitis diagnosis is challenging, as the sensitivity of diagnosis based solely on clinical evaluation ranges from 39% to 74%, with a specificity of 57% to 84% [6]. The most commonly used imaging method for diagnosing acute appendicitis is CT, which has been reported to exhibit high sensitivity (91% to 98.5%) and specificity (90% to 98%) in diagnosing acute appendicitis [13,14].
The delay in diagnosing acute appendicitis is considered a top priority among emergencies, which could lead to significant complications. In recent times, routine laboratory tests have been investigated as predictive measures in cases of acute appendicitis in which the diagnosis is not clearly established, and this method has become quite popular [15,16]. However, there is no clinical or laboratory test with both high sensitivity and high specificity. Relying solely on these parameters requires a delicate balance between the risk of delaying treatment (due to insufficient sensitivity for complicated appendicitis) and the risk of negative surgical interventions (due to inadequate specificity for complicated appendicitis). Standard imaging enhances diagnostic accuracy for both confirming and excluding appendicitis. Imaging can be integrated into scoring systems or used in conjunction with them. Additionally, imaging plays a crucial role in distinguishing between appendicitis, where there is suspicion of a cause requiring treatment, and other abdominal pathologies in cases of abdominal pain. Even if a clinical scoring model can exclude acute appendicitis, imaging is still necessary in most cases to accurately diagnose the cause of abdominal pain. Furthermore, in cases of appendicitis, imaging is still needed to differentiate between complicated and uncomplicated appendicitis [17].
The onset of acute appendicitis is attributed to the accumulation of fluid within the appendix lumen, leading to luminal distension. The appendix diameter increases due to the elevated intraluminal pressure, and this diameter increase has been assessed in various studies to be within the range of 4 to 12.8 mm [18]. Given the wide range of normal appendix diameters, the threshold for appendix diameter should be evaluated through clinical symptoms, laboratory values, and imaging methods [19]. In addition, an increase in appendix wall thickness, contrast material retention, and peri appendiceal inflammatory changes are of significance [20]. In our study, based on these insights, an increase in diameter has been anticipated in cases of appendicitis due to impaired venous drainage, resulting in the elevation of various cytokines and chemokines, as well as the occurrence of vascular vasodilation. ICA and ICV were used in our study to assess local vasodilation in cases of acute appendicitis.
The acute phase of inflammation comprises 3 main components: structural changes in the microvascular structure allowing leukocyte extravasation, emigration of leukocytes from the microcirculation, and changes in vascular caliber leading to increased blood flow [21]. Increased levels of cytokines and chemokines have been detected in serum in cases of acute appendicitis, which are associated with increased vascular permeability and local vasodilation [21]. Consequently, there is an increase in blood flow to the appendix wall and surrounding tissues. It can be anticipated that there may be an increase in the structures of the ileocolic artery and vein that supply the appendix as a result of this condition. In addition, Barac et al [22] have determined that ileocolic artery and vein diameters increase proportionally with body mass index. It has been established that cut-off values of the diameters can also be reliably used without considering the body mass index.
In the literature, studies demonstrating the relationship between ileocolic vessels and appendicitis are limited [23,24]. In the study conducted by Sirik et al [25], the average diameter of the ICA was 3.79±0.7 in the appendicitis group, while it was 2.75±0.31 mm in the control group, showing a statistically significant increase in cases of appendicitis. Similarly, when looking at the ICV, it was 5.21±0.9 mm in the appendicitis group, and 4.17±0.45 mm in the control group, with the difference being statistically significant. In the study by Kuzan et al [26], the diameter of the ICA was 3.28±0.60 mm in the acute appendicitis group and 2.72±0.48 mm in the control group, with a statistically significant difference. Likewise, the ICV diameter was 5.12±1.03 mm in the acute appendicitis group and 4.02±1.05 mm in the control group, and the difference was statistically significant. These results were consistent with the findings in our study.
In our study, unlike other investigations, cut-off values were explored for both arterial and venous diameters. Cut-off values of 2.475 mm for ICA diameter and 3.885 mm for ICV diameter were found to be highly specific and sensitive. These values were considered highly useful for establishing a diagnosis of appendicitis. In contrast to Kuzan et al [26], the area under the ROC curve analysis for artery and vein were 0.982 and 0.972, respectively. This suggests the possibility of reaching a diagnosis without the need for an additional measurement of abdominal aorta and inferior vena cava diameters.
Our study achieved high sensitivity and specificity values, which can complement conventional techniques. Arterial and venous diameters were measured by a single physician using the same technique to mitigate bias. An important advantage of our study is that it includes a larger number of patients than do previous studies. However, due to the retrospective nature of the study, there are inherent limitations. Additionally, body mass index was not included as a criterion in our study, which can introduce variability in arterial and venous diameters. Moreover, a separate study comparing acute appendicitis and complicated appendicitis patients was not conducted.
Conclusions
According to our study, measurements of ICA and ICV diameters can play a critical role in the accurate diagnosis of acute appendicitis cases. When used in conjunction with major radiological findings, these measurements have the potential to enhance diagnostic accuracy and contribute valuable insights to clinical management processes. Therefore, the use of ICA and ICV diameter measurements in the diagnosis of acute appendicitis may provide a novel perspective in clinical practice, leading to a more effective approach to patient management.
References
1. Krzyzak M, Mulrooney SM, Acute appendicitis review: Background, epidemiology, diagnosis, and treatment: Cureus, 2020; 12; 8562
2. Bursali A, Araç M, Oner AY, Evaluation of the normal appendix at low-dose non-enhanced spiral CT: Diagn Interv Radiol, 2005; 11; 45-50
3. Bhasin SK, Khan AB, Kumar V, Vermiform appendix and acute appendicitis: JK Sci, 2007; 9; 167-70
4. Addiss DG, Shaffer N, Fowler BS, Tauxe RV, The epidemiology of appendicitis and appendectomy in the United States: Am J Epidemiol, 1990; 132; 910-25
5. Khan MS, Chaudhry MBH, Shahzad N, Risk of appendicitis in patients with incidentally discovered appendicoliths: J Surg Res, 2018; 221; 84-87
6. Moris D, Paulson EK, Pappas TN, Diagnosis and management of acute appendicitis in adults: A review: JAMA, 2021; 326; 2299-311
7. Ishikawa H, Diagnosis and treatment of acute appendicitis: Japan Med Assoc J, 2003; 46; 217-21
8. Podda M, Pisanu A, Sartelli M, Diagnosis of acute appendicitis based on clinical scores: is it a myth or reality?: Acta Biomed, 2021; 92; 2021231
9. Balthazar EJ, Birnbaum BA, Yee J, Acute appendicitis: CT and US correlation in 100 patients: Radiol, 1994; 190; 31-35
10. Ashraf K, Ashraf O, Bari V, Role of focused appendiceal computed tomography in clinically equivocal acute appendicitis: J Pak Med Assoc, 2006; 56; 200-3
11. Moteki T, Horikoshi H, New CT criterion for acute appendicitis: Maximum depth of intraluminal appendiceal fluid: Am J Roentgenol, 2007; 188; 1313-19
12. Patel SV, Zhang L, Mir ZM, Delayed versus early laparoscopic appendectomy for adult patients with acute appendicitis: A randomized controlled trial: Ann Surg, 2024; 279; 88-93
13. Paulson EK, Kalady MF, Pappas TN, Clinical practice. Suspected appendicitis: N Engl J Med, 2003; 348; 236-42
14. Akıncı Ö, Predictive value of sphericity index and other multidetector computed tomography findings in perforated acute appendicitis: Ulus Travma Acil Cerrahi Derg, 2023; 29; 590-95
15. Sippola S, Virtanen J, Tammilehto V, The accuracy of low-dose computed tomography protocol in patients with suspected acute appendicitis: The OPTICAP Study: Ann Surg, 2020; 271; 332-38
16. Bedel C, Diagnostic value of basic laboratory parameters for simple and perforated acute appendicitis: Turk Clin Lab, 2018; 9; 266-71
17. Ulukent SC, Şahbaz NA, Özyürek EŞ, Evaluation of laboratory parameters in the diagnosis of acute appendicitis: Turkish J Biochem, 2018; 43; 64-70
18. Kwan KY, Nager AL, Diagnosing pediatric appendicitis: Usefulness of laboratory markers: Am J Emerg Med, 2010; 28; 1009-15
19. Bom WJ, Scheijmans JCG, Salminen P, Boermeester MA, Diagnosis of uncomplicated and complicated appendicitis in adults: Scand J Surg, 2021; 110; 170-79
20. Pinto Leite N, Pereira JM, Cunha R, CT evaluation of appendicitis and its complications: Imaging techniques and key diagnostic findings: Am J Roentgenol, 2005; 185; 406-17
21. Pober JS, Sessa WC, Inflammation and the blood microvascular system: Cold Spring Harb Perspect in Biol, 2015; 7; a016345
22. Barac Y, Agridag B, Ozkurt H, Retrospective evaluation of ileocolic artery and vein diameters according to body mass index in the diagnosis of acute appendicitis on multislice computerized tomography: Med Bull Sisli Etfal Hosp, 2021; 55; 18
23. Willekens I, Peeters E, De Maeseneer M, de Mey J, The normal appendix on CT: Does size matter?: PLoS One, 2014; 9; 96476
24. Martin M, Lubrano J, Azizi A, Inflammatory appendix mass in patients with acute appendicitis: CT diagnosis and clinical relevance: Emerg Radiol, 2015; 22; 7-12
25. Sirik M, Olt S, The value of the ileocolic vessels in acute appendicitis – a cross sectional study: Ann Med Res, 2021; 25; 656-59
26. Kuzan BN, Kuzan TY, Ergelen R, A new parameter in the diagnosis of acute appendicitis: Ileocolic artery and vein diameter measurements: Ann Med Res, 2021; 26; 2082-87
Figures
Tables
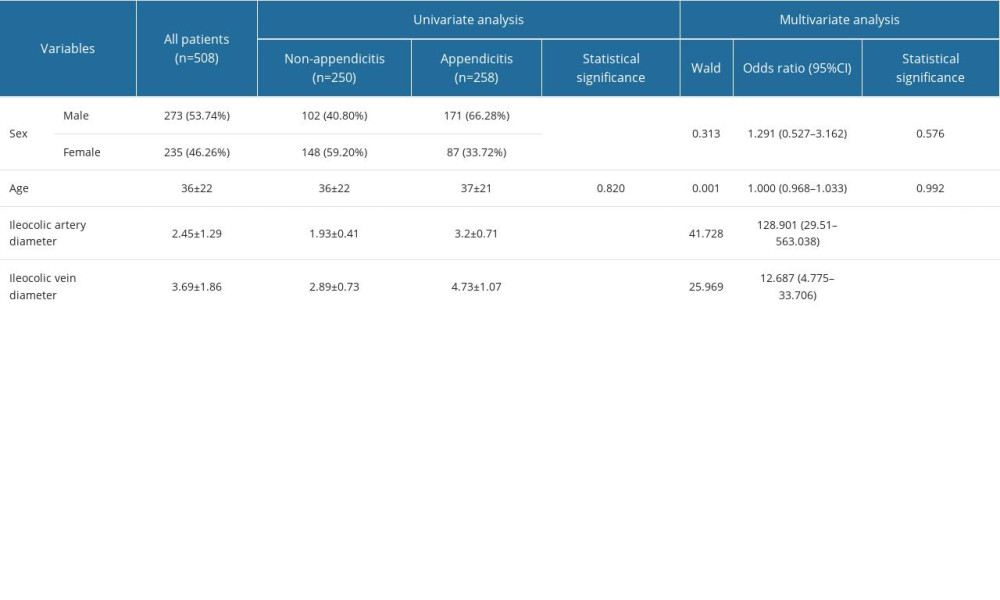 Table 1. Comparison of variables between groups and results of univariate and multivariate analysis.
Table 1. Comparison of variables between groups and results of univariate and multivariate analysis.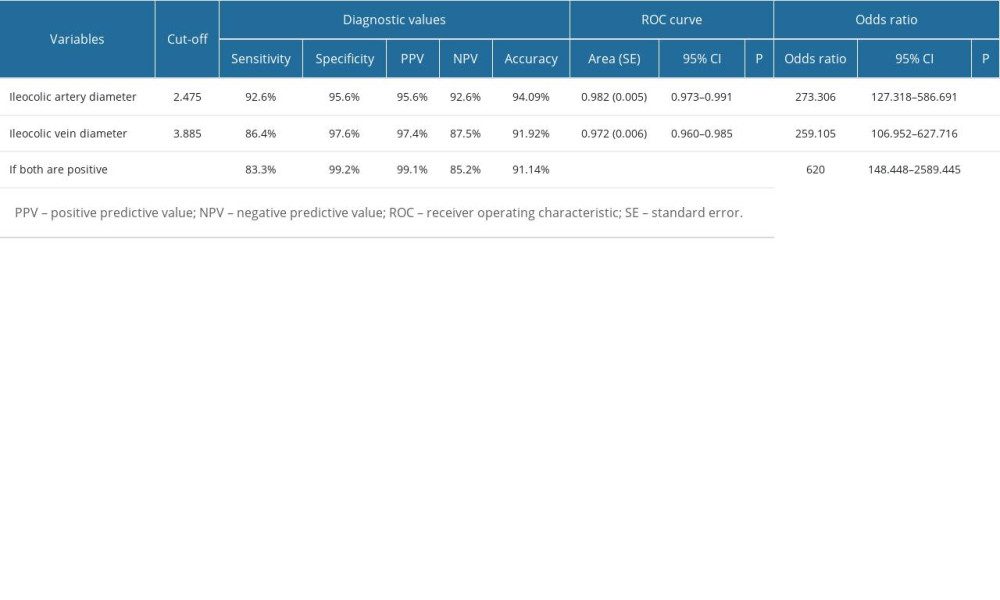 Table 2. Cut-off points and diagnostic values of variables for the distinction between non- appendicitis patients and appendicitis patients.Table 1. Comparison of variables between groups and results of univariate and multivariate analysis.Table 2. Cut-off points and diagnostic values of variables for the distinction between non- appendicitis patients and appendicitis patients.
Table 2. Cut-off points and diagnostic values of variables for the distinction between non- appendicitis patients and appendicitis patients.Table 1. Comparison of variables between groups and results of univariate and multivariate analysis.Table 2. Cut-off points and diagnostic values of variables for the distinction between non- appendicitis patients and appendicitis patients. In Press
11 Mar 2024 : Clinical Research
Enhancement of Frozen-Thawed Human Sperm Quality with Zinc as a Cryoprotective AdditiveMed Sci Monit In Press; DOI: 10.12659/MSM.942946
12 Mar 2024 : Database Analysis
Risk Factors of Age-Related Macular Degeneration in a Population-Based Study: Results from SHIP-TREND-1 (St...Med Sci Monit In Press; DOI: 10.12659/MSM.943140
12 Mar 2024 : Clinical Research
Preoperative Blood Transfusion Requirements for Hemorrhoidal Severe Anemia: A Retrospective Study of 128 Pa...Med Sci Monit In Press; DOI: 10.12659/MSM.943126
12 Mar 2024 : Clinical Research
Tissue Inhibitors of Metalloproteinase 1 (TIMP-1) and 3 (TIMP-3) as New Markers of Acute Kidney Injury Afte...Med Sci Monit In Press; DOI: 10.12659/MSM.943500
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952