31 May 2024: Clinical Research
Effectiveness of Shoulder Taping in Treating Hemiplegic Shoulder Subluxation: A Randomized Controlled Study of 35 Patients
JongEun Yim1ACDEF, Beomryong Kim2ABCDEF*DOI: 10.12659/MSM.944222
Med Sci Monit 2024; 30:e944222






Abstract
BACKGROUND: Shoulder subluxation in patients with stroke impairs recovery and quality of life. Kinesiology tape is elastic and water-resistant, is commonly used to prevent musculoskeletal injury, and is increasing in use for rehabilitation of patients requiring neurological or physical rehabilitation. This study included 35 patients with shoulder subluxation following stroke and aimed to compare outcomes from standard physical therapy with and without shoulder kinesiology taping.
MATERIAL AND METHODS: This randomized controlled study involved 35 participants. The patients were randomized into a shoulder kinesiology taping group (n=18) or sham taping group (n=17). All patients underwent a conventional rehabilitation exercise program 5 days a week for 6 weeks. Half of the patients underwent shoulder kinesiology taping, and the other half underwent sham taping. Pre- and post-assessment scores were recorded for all participants for shoulder subluxation distance (SSD), active range of motion (AROM), visual analog scale (VAS), shoulder pain and disability index (SPADI), and modified Barthel index (MBI).
RESULTS: After the intervention, SSD, AROM, VAS, SPADI, and MBI improved significantly in the shoulder kinesiology taping and sham taping groups (P<0.05). Also, the shoulder kinesiology taping group showed more effective changes in SSD, AROM, VAS, SPADI, and MBI than the sham taping group (P<0.05).
CONCLUSIONS: These results suggest that the shoulder kinesiology taping is effective in improving SSD, AROM, VAS, SPADI, and MBI in patients with hemiplegic shoulder subluxation.
Keywords: Athletic Tape, Shoulder Dislocation, Stroke, Upper Extremity, Humans, Male, Female, Middle Aged, Hemiplegia, Range of Motion, Articular, Treatment Outcome, stroke rehabilitation, Aged, Shoulder, adult, Quality of Life, Exercise Therapy, Shoulder Joint
Introduction
The incidence of hemiplegic shoulder pain is approximately 63% in patients with acute and chronic stroke [1]. Hemiplegic shoulder pain delays upper extremity rehabilitation, negatively affects patient quality of sleep and performance of daily activities, obstructs functional motor recovery of the affected limbs, and prolongs hospitalization [2–4]. The causes of shoulder subluxation can be classified into neuromuscular, traumatic, and non-traumatic causes [5]. Stroke can cause shoulder subluxation due to neuromuscular causes [6]. In the case of nerve roots, shoulder inferior subluxation occurs due to weakness of the shoulder girdle and rotator cuff muscles. Spasticity of internal rotation muscles (pectoralis major, latissimus dorsi, and subscapularis muscles) causes shoulder posterior subluxation [7]. The degree of shoulder subluxation can be quantified as the distance from the acromion to the humeral head using fingerbreadth, tape, or caliper [8]. Tests to check shoulder relaxation include the load and shift test, drawer test, sulcus test, hyperabduction test, and push-and-pull test [9,10]. In cases in which subluxation and shoulder pain are accompanied by a history of stroke, physical examination for subacromial impingement, acromioclavicular arthropathy, and rotator cuff tendinopathy are helpful in identifying the cause of shoulder pain [11]. Additionally, 50% of patients after stroke present proprioceptive deficits in the upper extremity [12]. According to previous studies, patients with stroke have a clear relationship between affected shoulder proprioception and movement, and hemiplegic shoulder pain was observed. To determine the risk of developing hemiplegic shoulder pain, attention should be paid to a patient’s shoulder proprioception and movement [13], which are related to the grade of shoulder subluxation [14]. Moreover, these proprioceptive shortages are associated with upper extremity motor recovery and functional performance [15], limiting activity and participation [16]. Therefore, treating proprioceptive impairments and managing shoulder pain are main objectives of rehabilitation exercise programs for patients with stroke [17,18].
With this in mind, some rehabilitation exercise programs, including correct positioning [19], arm sling and shoulder strapping [20,21], electric stimulation therapy [22], traditional manual acupuncture [23], and local injections [24], have been proposed to maintain normal joint alignment and motion, treat pain, and improve muscle strength in hemiplegic shoulders. Kinesiology and shoulder taping have been proposed to decrease the incidence of shoulder subluxation or pain, improve shoulder motion and function, and prevent further shoulder injury in hemiplegic shoulders [25–29].
Taping involves an assistant method that uses elastic adhesive tape over the skin to stimulate mechanical receptors by continuous skin compression and stretching during joint motion [30,31]. Based on acknowledged principles in neuroscience, it can be hypothesized that these afferent stimuli are conveyed to the contralateral zone of the somatosensory cortex, which integrates information from various motor and sensory modalities [32]. The kinesiology taping method was developed by Kenzo-Kase in the 1970s and has gradually gained popularity in clinical practice for managing musculoskeletal disorders [33]. According to Jaraczewska and Long [34], taping can inhibit or facilitate muscle function, reduce pain, support joint structure, and deliver proprioceptive feedback to attain and continue favored body alignment. Some studies have suggested that taping can decrease pain and subluxation and improve range of motion (ROM) and motor performance in patients with stroke [27,35].
Herein, we compared the effects of a 6-week program of shoulder kinesiology taping or sham taping on the shoulder subluxation distance (SSD), active ROM (AROM), visual analog scale (VAS), shoulder pain and disability index (SPADI), and modified Barthel index (MBI) in patients with stroke. The research hypothesis was that the use of the shoulder kinesiology taping would better improve hemiplegic shoulder pain and functional outcomes, compared with sham taping, in patients with stroke. Therefore, this study included 35 patients with shoulder subluxation following stroke and aimed to compare outcomes from standard physical therapy with and without shoulder kinesiology taping.
Material and Methods
RESEARCH DESIGN:
This double-blind, placebo-controlled clinical study was performed at the Design Hospital in Jeonju City between July 2019 and August 2021. Patients were randomly assigned to 2 groups: a study group (shoulder kinesiology taping and rehabilitation exercise, n=18) and a control group (sham taping and rehabilitation exercise, n=17). Blinded allocation was performed using a computer-generated random table of numbers, which was created before data collection by a physical therapist who was not involved in the evaluation or intervention of the patients. Before and after 6 weeks of intervention, evaluation was performed by an uninvolved physical therapist who was blinded to the group allocation and patient medical information. A separate form for result assessment was given to the evaluator during the assessment. Taping was performed by a certified physical therapist directly following primary measurements. Taping in the study and control groups was performed by the same physical therapist, who was not involved in the intervention or outcome evaluation. None of the patients previously underwent shoulder kinesiology taping. The patients were evaluated in a separate room, and the tape was detached before the result assessment. SSD, AROM, VAS, SPADI, and MBI were the primary outcomes. This study was conducted with the approval of the Research Ethics Committee of Sahmyook University (2-7001793-AB-N-012018140HR), and the approved date was December 17, 2018.
STUDY PARTICIPANTS:
Of the 124 patients with stroke admitted to the Design Hospital Rehabilitation Center for inpatient rehabilitation exercise, 42 patients with a hemiplegic shoulder met the inclusion criteria, and 35 patients completed all procedures in the study. Study participants provided informed consent, following an explanation of the study purpose and procedures (Figure 1).
The following were the inclusion criteria: (1) unilateral infarction or hemorrhage stroke lesions identified using computed tomography or magnetic resonance imaging; (2) >6 months since the occurrence of stroke; (3) at least 9.5 mm (0.37 inch) of shoulder subluxation in the affected upper extremity; (4) pain in the subluxated shoulder; (5) spasticity for shoulder flexor and abductor level of <1+ on the modified Ashworth scale; (6) age between 50 and 70 years; (7) appropriate trunk control, defined as the ability to maintain a sitting position without support for the trunk and/or of the arms for 1 min; and (8) intact cognitive function and adequate communication skills (Mini-Mental Status Examination-Korean version score of ≥24 points). Exclusion criteria were as follows: (1) shoulder pain or history of neurological diseases or other orthopedic injuries in the affected shoulder before the onset of stroke; (2) communication or cognitive impairments; (3) infection, skin problems, or wounds in the affected shoulder; and (4) a history of skin allergy (redness and itching) to tape. A summary of the participants’ clinical information is presented in Table 1.
SSD MEASUREMENT: This study used a jig measuring instrument to evaluate shoulder subluxation in hemiplegic patients. The jig-measuring instrument was used to measure shoulder subluxation. It comprised an L-shaped rod and an adjustable mover. The acromion process was marked with a pen by drooping the affected arm and then marking the point 20 cm above the olecranon with the pen while passively flexing the elbow joint. The rod was then placed on the acromion, and the length of the end of the mover was measured against the point marked with the pen. The subluxation of the patient was then re-measured after the reduction. The degree of subluxation was determined by comparing the differences before and after the reduction. This measuring instrument has intra-rater (intraclass correlation coefficient [ICC]=0.89) and inter-rater reliability (ICC=0.74) [36].
AROM OF THE SHOULDER: AROM was assessed using smartphone clinometer application measurements for shoulder flexion and abduction. Shoulder flexion and abduction were measured with the patient in the standing position. This test tool has intra- and inter-rater reliability (ICC=0.80–0.89) and is appropriate for measuring the ROM of the shoulder [37].
SHOULDER PAIN: Pain level was assessed using the VAS as the degree of subjective pain to assess the level of shoulder joint pain in patients with hemiplegia. The VAS is an 11-point scale displayed on a 10-cm horizontal line, ranging from 0 (no pain) to 10 (worst pain imaginable) [38]. This test tool has intra- and inter-rater reliability (ICC=0.99–1.00) [39].
SPADI MEASUREMENT: SPADI, a self-administered evaluation tool, was used to measure pain and disability related to shoulder pathology. The SPADI is a 13-item form that comprises 2 subscale measures of 5 items on pain and 8 items on disability, which is scored by taking an average of the 2 lower measures. Pain and disability subscales were calculated as the mean of the matching items on a scale of 0 to 100, with the uppermost score representing the most severe pain and disability. The total result score used for statistical analysis was the sum of the pain and disability subscales. This test tool has test-retest reliability (ICC=0.99) and Cronbach’s alpha value of 0.96 [40].
MBI MEASUREMENT: The MBI measures the functional ability to perform activities of daily living and the degree of independence of patients with a disease. The 10 items comprise personal hygiene, self-bathing, feeding, toilet use, stair climbing, dressing, bladder and bowel control, ambulation, and chair or bed transfer. The maximum score is 100, indicating that the patient is fully independent in physical functioning. The lowest score is 0, indicating a completely dependent incapacitated state. This test tool has intra-rater (ICC=0.87–1.00) and inter-rater reliability (ICC=0.93–0.98) and Cronbach’s alpha value of 0.84 [41].
SHOULDER KINESIOLOGY AND SHAM TAPING: The taping method in this study was a modification of the California tri-pull taping introduced by Hayner [26]. Taping was applied using non-elastic tape (Battlewin C tape, Nichiban, Japan) and elastic tape (Benefact tape, Nippon Sigmax, Japan). This method is known as shoulder kinesiology taping. Before the first day of intervention, the patients with hair on their shoulders were asked to shave the area. For better adherence, the skin was scrubbed with a skin preparation (a defensive skin barrier smear) before applying the tape, and if needed, a tape remover was used before the skin preparation to remove the remaining tape from a previous taping. For tape application, the patient was seated in the neutral position with the affected upper extremity side sideways, and the elbow joint was comfortably placed on the table, resulting in a reduced subluxation condition. The first elastic tape was attached from the middle part of the deltoid insertion (deltoid tuberosity) to the acromion process. The second elastic tape was attached from the posterior part of the deltoid insertion to the spine of the scapula. The third elastic tape was attached from the anterior part of the deltoid insertion to the humeral head and over the coracoid process. Next, the non-elastic tape was attached with firm pressure. Three tapes were attached to the deltoid insertion (deltoid tuberosity), middle part of the deltoid, and acromion process in the direction of internal rotation (Figure 2).
For patients allocated to the control group, sham taping was performed using elastic tape. Three pieces of tape were attached to the same position without repositioning the joint (Figure 3).
Every Monday, Wednesday, and Friday, the tape was removed, and new tape was attached. This was repeated for 6 successive weeks. Attachment of elastic and non-elastic tape was performed by a physical therapist who had completed 5 years of related training.
REHABILITATION EXERCISE PROGRAM:
The study and control groups underwent the same conventional rehabilitation exercise program, including physical and occupational therapy sessions. All other physical therapy measures, such as positioning, ROM exercises, and handling techniques, were performed in the study and control groups. Rehabilitation exercise was performed for 6 weeks, 5 days a week for 60 min. The therapists were trained to refrain from commenting on the taping when performing the daily rehabilitation exercises.
STATISTICAL ANALYSIS:
Statistical analysis was performed using SPSS/PC Statistics software (version 18.0; IBM Corp, Armonk, NY, USA) for Windows. The Shapiro-Wilk test was used to check the normal distribution of the data. A paired
Results
COMPARISON OF SSD CHANGES:
Within-group changes in SSD were significant in the shoulder (t=24.952,
COMPARISON OF AROM CHANGES:
Within-group changes in AROM of shoulder flexion were significant in the shoulder (t=−12.550,
COMPARISON OF VAS CHANGES:
Within-group changes in the VAS scores were significant in the shoulder (t=11.854,
COMPARISON OF SPADI CHANGES:
Within-group changes in the SPADI scores were significant in the shoulder (t=16.007,
COMPARISON OF MBI CHANGES:
Within-group changes in the MBI scores were significant in the shoulder (t=−10.564,
Discussion
In this study, we aimed to investigate the effect of the shoulder kinesiology taping method on the SSD, AROM, pain, function of the upper extremity, and activities of daily living in stroke patients with a subluxated shoulder.
Brunnstrom [42] described fixation movement by combining the movement pattern and spasticity of the limbs seen in patients with stroke in the synergy pattern. Conversely, the pattern of muscle weakness that occurs after a stroke has been reported by several researchers. Muscles weakened mainly in the upper extremity are the extensors of the fingers, wrist, and elbow and muscles involved in shoulder internal rotation, abduction, and extension. The weakness of these muscles is closely related to various functions [43]. Calliet [44] reported the role of the supraspinatus, deltoid, and other muscles, which prevent the head of the humerus from moving inferiorly due to the initial flaccid paralysis after stroke. The scapula is also rotated, and the glenoid fossa of the scapula is directed inferiorly, making subluxation easier. Therefore, as reported by de Kroon et al [43], the external rotator of the shoulder and weakness of the abductor and extensor muscles are related to subluxation. Shoulder kinesiology taping, used as an interventional method in the present study, attaches tape to the middle, posterior, and anterior fibers of the deltoid, which cannot perform abduction and extension of the shoulder, using elastic and non-elastic tape. The tape was attached in the direction of external rotation, which is the role of the supraspinatus. These tape attachments consistently generate sensory impulses in the skin and muscles to increase muscle activity and improve the proprioceptive sense, thereby stabilizing the shoulder joint [45–47]. Therefore, the shoulder kinesiology taping group showed improvement in SSD, increased ROM during active flexion and abduction, decrease in shoulder pain, improved function of the upper extremity, and improvement in activities of daily living, compared with the sham taping group. Hayner [26] showed improved results in AROM, pain, and SSD by applying deltoid and external rotator taping to a subluxated shoulder after stroke, and Pandian et al [48] reported improvement in pain and function of the upper extremity by applying deltoid and external rotator taping to the shoulder in patients with stroke. Chatterjee et al [35] reported improvement in ROM, pain, SSD, and function of the upper extremity by applying deltoid and external rotator taping to a subluxated shoulder after stroke. In addition, Chatterjee et al [25] reported improvement in AROM, pain, and function of the upper extremity by applying deltoid and external rotator taping to a subluxated shoulder after stroke. Yang et al [49] reported that kinesiology taping is effective in reducing pain and SSD and increasing muscle activity and AROM for patients with hemiplegic shoulder pain. Huang et al [27] found that patients with hemiplegic shoulder pain can experience greater reductions in SPADI, pain, and improvement in shoulder ROM after 3 weeks of kinesiology taping, compared with sham taping. Kinesiology taping can be an alternative intervention for patients with hemiplegic shoulder pain. According to a meta-analysis by Wang et al [50], kinesiology taping can be recommended to improve pain, SSD, disability, upper extremity function, and ROM. Thus, previous studies support the shoulder kinesiology taping method that was used to perform the role of the deltoid and external rotator in the present study.
The body function of shoulder kinesiology taping showed a decrease in SSD, an increase in AROM, and pain reduction in stroke patients with subluxation. In addition, the improvement in body function and activity by shoulder kinesiology taping improved upper extremity function and activities of daily living, which are the goals of patient treatment. The background for improving body function and activity in the present study was as follows: first, the elasticity of the tape stimulated the skin and muscle so that the muscle that was taped returned to its original state; thus, the function of the muscle appeared to be normalized. In 1 case, the muscle was torn, and the joint was shifted. Attaching the tape seemed to prevent the joint from shifting, because the tone of the muscle returned to the normal state. Second, it seemed that the tape lifted the skin to form wrinkles so that the tissue fluid, which had accumulated locally, was discharged quickly, and the smooth flow of blood or lymph improved various problems. Third, it seemed to have had the effect of neurologically eliminating pain, by the attaching of tape to the area of concern.
In the present study, shoulder kinesiology taping was effective in improving SSD, shoulder joint AROM, pain, upper extremity function, and activities of daily living in stroke patients with subluxation. Although, with subluxations limited to a single hospital, this study is not generalizable to all stroke patients, the results of this study are expected to be more meaningful if we increase the number of patients and compare them with other methods in future studies. Neurodevelopmental treatment applied to patients with stroke is also good; however, if taping is performed, more effective results will be obtained.
Conclusions
The shoulder kinesiology taping method reduced subluxation and pain and improved active shoulder flexion, upper extremity functional ability, and activities of daily living. This appears to be a potential early adjunctive intervention for patients who have experienced a stroke and demonstrate pain in a subluxated shoulder, to increase shoulder flexion and extension and upper extremity functional ability. Moreover, this taping method allows patients to participate in all active upper extremity exercises as well as all activities of daily living.
Figures
 Figure 1. Flow diagram of the study.
Figure 1. Flow diagram of the study. 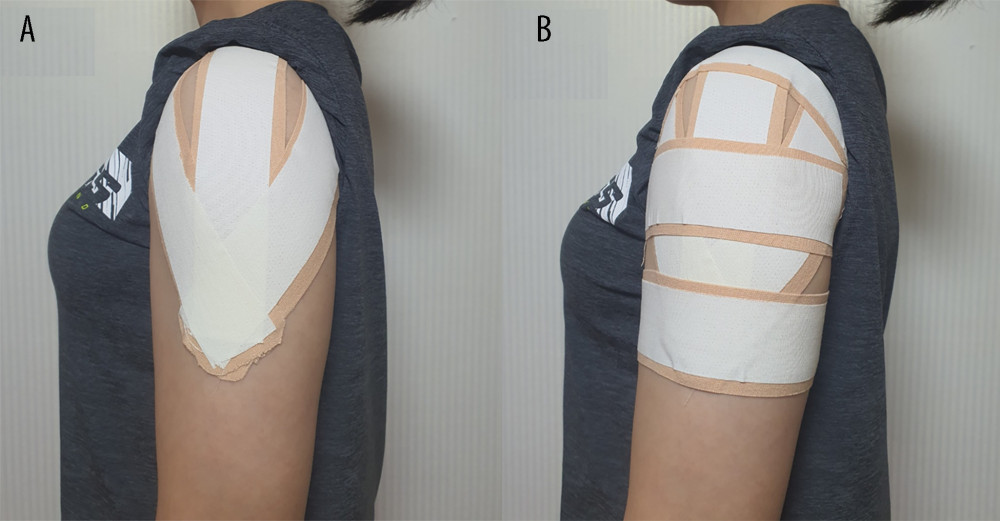 Figure 2. Sequence of shoulder kinesiology taping. (A) The first elastic tape was attached from the middle part of the deltoid tuberosity to the acromion process. The second elastic tape was attached from the posterior part of the deltoid insertion to the spine of the scapula. The third elastic tape was attached from the anterior part of the deltoid insertion to the humeral head and over the coracoid process. The non-elastic tape was attached with firm pressure. (B) Three tapes were attached to the deltoid tuberosity, the middle part of the deltoid, and the acromion process in the direction of internal rotation. The non-elastic tape was attached with firm pressure.
Figure 2. Sequence of shoulder kinesiology taping. (A) The first elastic tape was attached from the middle part of the deltoid tuberosity to the acromion process. The second elastic tape was attached from the posterior part of the deltoid insertion to the spine of the scapula. The third elastic tape was attached from the anterior part of the deltoid insertion to the humeral head and over the coracoid process. The non-elastic tape was attached with firm pressure. (B) Three tapes were attached to the deltoid tuberosity, the middle part of the deltoid, and the acromion process in the direction of internal rotation. The non-elastic tape was attached with firm pressure.  Figure 3. Sham taping. Three pieces of tape were attached to the deltoid without repositioning the joint. Figure was created with Presentation (PowerPoint 2016, Microsoft).
Figure 3. Sham taping. Three pieces of tape were attached to the deltoid without repositioning the joint. Figure was created with Presentation (PowerPoint 2016, Microsoft). References
1. Wanklyn P, Forster A, Young J, Hemiplegic shoulder pain (HSP): Natural history and investigation of associated features: Disabil Rehabil, 1996; 18(10); 497-501
2. Lindgren I, Jonsson AC, Norrving B, Shoulder pain after stroke: A prospective population-based study: Stroke, 2007; 38(2); 343-48
3. Chae J, Mascarenhas D, David TY, Poststroke shoulder pain: Its relationship to motor impairment, activity limitation, and quality of life: Arch Phys Med Rehabil, 2007; 88(3); 298-301
4. Gilmore PE, Spaulding SJ, Vandervoort AA, Hemiplegic shoulder pain: Implications for occupational therapy treatment: Can J Occup Ther, 2004; 71(1); 36-46
5. Eljabu W, Klinger H, Von Knoch M, The natural course of shoulder instability and treatment trends: A systematic review: J Orthop Traumatol, 2017; 18(1); 1-8
6. Paci M, Nannetti L, Rinaldi LA, Glenohumeral subluxation in hemiplegia: An overview: J Rehabil Res Dev, 2005; 42(4); 557-68
7. Murie-Fernández M, Iragui MC, Gnanakumar V, Painful hemiplegic shoulder in stroke patients: Causes and management: Neurología, 2012; 27(4); 234-44
8. Huang SW, Liu SY, Tang HW, Relationship between severity of shoulder subluxation and soft-tissue injury in hemiplegic stroke patients: J Rehabil Med, 2012; 44(9); 733-39
9. Guerrero P, Busconi B, Deangelis N, Congenital instability of the shoulder joint: Assessment and treatment options: J Orthop Sports Phys Ther, 2009; 39(2); 124-34
10. Hippensteel K, Brophy R, Smith MV, Comprehensive review of provocative and instability physical examination tests of the shoulder: J Am Acad Orthop Surg, 2019; 27(11); 395-404
11. Treister AK, Hatch MN, Cramer SC, Demystifying poststroke pain: From etiology to treatment: PM R, 2017; 9(1); 63-75
12. Dukelow SP, Herter TM, Moore KD, Quantitative assessment of limb position sense following stroke: Neurorehabil Neural Repair, 2010; 24(2); 178-87
13. Niessen MH, Veeger DH, Meskers CG, Relationship among shoulder proprioception, kinematics, and pain after stroke: Arch Phys Med Rehabil, 2009; 90(9); 1557-64
14. dos Santos GL, Salazar LFG, Lazarin AC, Joint position sense is bilaterally reduced for shoulder abduction and flexion in chronic hemiparetic individuals: Top Stroke Rehabil, 2015; 22(4); 271-80
15. Meyer S, Karttunen AH, Thijs V, How do somatosensory deficits in the arm and hand relate to upper limb impairment, activity, and participation problems after stroke? A systematic review: Phys Ther, 2014; 94(9); 1220-31
16. Dukelow SP, Herter TM, Bagg SD, The independence of deficits in position sense and visually guided reaching following stroke: J Neuroeng Rehabil, 2012; 9(1); 72
17. Colombo R, Sterpi I, Mazzone A, Improving proprioceptive deficits after stroke through robot-assisted training of the upper limb: A pilot case report study: Neurocase, 2016; 22(2); 191-200
18. Poduri KR, Shoulder pain in stroke patients and its effects on rehabilitation: J Stroke Cerebrovasc Dis, 1993; 3(4); 261-66
19. Ada L, Goddard E, McCully J, Thirty minutes of positioning reduces the development of shoulder external rotation contracture after stroke: A randomized controlled trial: Arch Phys Med Rehabil, 2005; 86(2); 230-34
20. Lambrecht G, Oostra K, Vanderstraeten G, A randomized controlled trial on the immediate and long-term effects of arm slings on shoulder subluxation in stroke patients: Eur J Phys Rehabil Med, 2017; 53(3); 400-9
21. Comley-White N, Mudzi W, Musenge E, Effects of shoulder strapping in patients with stroke: A randomised control trial: S Afr J Physiother, 2018; 74(1); 430
22. Chuang LL, Chen YL, Chen CC, Effect of EMG-triggered neuromuscular electrical stimulation with bilateral arm training on hemiplegic shoulder pain and arm function after stroke: A randomized controlled trial: J Neuroeng Rehabil, 2017; 14(1); 122
23. Peng L, Zhang C, Zhou L, Traditional manual acupuncture combined with rehabilitation therapy for shoulder hand syndrome after stroke within the Chinese healthcare system: A systematic review and meta-analysis: Clin Rehabil, 2018; 32(4); 429-39
24. Jang MH, Lee CH, Shin YI, Effect of intra-articular hyaluronic acid injection on hemiplegic shoulder pain after stroke: Ann Rehabil Med, 2016; 40(5); 835-44
25. Chatterjee S, Hayner KA, Arumugam N, The California tri-pull taping method in the treatment of shoulder subluxation after stroke: A randomized clinical trial: N Am J Med Sci, 2016; 8(4); 175-82
26. Hayner KA, Effectiveness of the California tri-pull taping method for shoulder subluxation poststroke: A single-subject ABA design: Am J Occup Ther, 2012; 66(6); 727-36
27. Huang YC, Chang KH, Liou TH, Effects of Kinesio taping for stroke patients with hemiplegic shoulder pain: A double-blind, randomized, placebo-controlled study: J Rehabil Med, 2017; 49(3); 208-15
28. Kalichman L, Frenkel-Toledo S, Vered E, Effect of kinesio tape application on hemiplegic shoulder pain and motor ability: A pilot study: Int J Rehabil Res, 2016; 39(3); 272-76
29. Huang YC, Leong CP, Wang L, Effect of kinesiology taping on hemiplegic shoulder pain and functional outcomes in subacute stroke patients: A randomized controlled study: Eur J Phys Rehabil Med, 2016; 52(6); 774-81
30. Röijezon U, Clark NC, Treleaven J, Proprioception in musculoskeletal rehabilitation. Part 1: Basic science and principles of assessment and clinical interventions: Man Ther, 2015; 20(3); 368-77
31. Clark NC, Röijezon U, Treleaven J, Proprioception in musculoskeletal rehabilitation. Part 2: Clinical assessment and intervention: Man Ther, 2015; 20(3); 378-87
32. Kandel ER, Schwartz JH, Jessell TM: Principles of neural science, 2000, New York, McGraw-Hill
33. Kase K, Clinical therapeutic applications of the Kinesio taping method: Albuquerque, 2003
34. Jaraczewska E, Long C, Kinesio taping in stroke: Improving functional use of the upper extremity in hemiplegia: Top Stroke Rehabil, 2006; 13(3); 31-42
35. Chatterjee S, Arumugam N, Midha D, Effect of California tri-pull taping method on shoulder subluxation, pain, active range of motion and upper limb functional recovery after stroke – a pretest post test design: Am J Psychiatry Neurosci, 2015; 3(5); 98-103
36. Hayes KW, Sullivan JE, Reliability of a new device used to measure shoulder subluxation: Phy Ther, 1989; 69(9); 762-67
37. Werner BC, Holzgrefe RE, Griffin JW, Validation of an innovative method of shoulder range-of-motion measurement using a smartphone clinometer application: J Shoulder Elbow Surg, 2014; 23(11); e275-e82
38. Farrar JT, Young JP, LaMoreaux L, Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale: Pain, 2001; 94(2); 149-58
39. Wagner DR, Tatsugawa K, Parker D, Reliability and utility of a visual analog scale for the assessment of acute mountain sickness: High Alt Med Biol, 2007; 8(1); 27-31
40. Torres-Lacomba M, Sánchez-Sánchez B, Prieto-Gómez V, Spanish cultural adaptation and validation of the shoulder pain and disability index, and the oxford shoulder score after breast cancer surgery: Health Qual Life Outcomes, 2015; 13(1); 63
41. Jung HY, Park BK, Shin HS, Development of the Korean version of Modified Barthel Index (K-MBI): Multi-center study for subjects with stroke: Ann Rehabil Med, 2007; 31(3); 283-97
42. Brunnstrom S: Movement therapy in hemiplegia: A neurophysiological approach, 1970, New York, Medical Dept
43. de Kroon JR, IJzerman MJ, Chae J, Relation between stimulation characteristics and clinical outcome in studies using electrical stimulation to improve motor control of the upper extremity in stroke: J Rehabil Med, 2005; 37(2); 65-74
44. Calliet R: Shoulder pain, 1991, Philadelphia, FA Davis Co
45. Lee SE, Cho SH, The effect of McConnell taping on vastus medialis and lateralis activity during squatting in adults with patellofemoral pain syndrome: J Exerc Rehabil, 2013; 9(2); 326-30
46. Choi YK, Nam CW, Lee JH, The effects of taping prior to PNF treatment on lower extremity proprioception of hemiplegic patients: J Phys Ther Sci, 2013; 25(9); 1119-22
47. Faghri PD, Rodgers MM, Glaser RM, The effects of functional electrical stimulation on shoulder subluxation, arm function recovery, and shoulder pain in hemiplegic stroke patients: Arch Phys Med Rehabil, 1994; 75(1); 73-79
48. Pandian JD, Kaur P, Arora R, Shoulder taping reduces injury and pain in stroke patients Randomized controlled trial: Neurology, 2013; 80(6); 528-32
49. Yang L, Yang J, He C, The effect of kinesiology taping on the hemiplegic shoulder pain: A randomized controlled trial: J Healthc Eng, 2018; 2018; 8346432
50. Wang Y, Li X, Sun C, Effectiveness of kinesiology taping on the functions of upper limbs in patients with stroke: A meta-analysis of randomized trial: Neurol Sci, 2022; 43(7); 4145-56
Figures
Figure 1. Flow diagram of the study.Figure 2. Sequence of shoulder kinesiology taping. (A) The first elastic tape was attached from the middle part of the deltoid tuberosity to the acromion process. The second elastic tape was attached from the posterior part of the deltoid insertion to the spine of the scapula. The third elastic tape was attached from the anterior part of the deltoid insertion to the humeral head and over the coracoid process. The non-elastic tape was attached with firm pressure. (B) Three tapes were attached to the deltoid tuberosity, the middle part of the deltoid, and the acromion process in the direction of internal rotation. The non-elastic tape was attached with firm pressure.Figure 3. Sham taping. Three pieces of tape were attached to the deltoid without repositioning the joint. Figure was created with Presentation (PowerPoint 2016, Microsoft). Tables
 Table 1. Clinical characteristics of the stroke patients in the shoulder kinesiology taping and sham taping groups.
Table 1. Clinical characteristics of the stroke patients in the shoulder kinesiology taping and sham taping groups. Table 2. Comparison of physical findings between and within the shoulder kinesiology taping and sham taping groups.Table 1. Clinical characteristics of the stroke patients in the shoulder kinesiology taping and sham taping groups.Table 2. Comparison of physical findings between and within the shoulder kinesiology taping and sham taping groups.
Table 2. Comparison of physical findings between and within the shoulder kinesiology taping and sham taping groups.Table 1. Clinical characteristics of the stroke patients in the shoulder kinesiology taping and sham taping groups.Table 2. Comparison of physical findings between and within the shoulder kinesiology taping and sham taping groups. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387