29 July 2024: Review Articles
Jellyfish Stings: A Review of Skin Symptoms, Pathophysiology, and Management
Xiao Peng1CDEF, Ke-tong Liu1CEF, Jing-bo Chen123CDEF, Zi-hao Yan1CF, Blessing Danso1CD, Ming-ke WangDOI: 10.12659/MSM.944265
Med Sci Monit 2024; 30:e944265






Abstract
ABSTRACT: With the surge in the human coastal population and the increasing frequency of human activities along the coast, cases of marine envenomation, particularly jellyfish envenomation, have notably risen. Jellyfish stings can induce a spectrum of symptoms that vary in severity, encompassing skin injuries, acute systemic venom effects, delayed indirect sequelae, and even fatality, causing significant distress to patients. Among these manifestations, the occurrence of skin lesions following jellyfish stings is prevalent and substantial. These lesions are characterized by evident blister formation, development of bullae, subcutaneous hemorrhage, erythema, papules, wheal, ecchymosis, and ulceration or skin necrosis. Local cutaneous manifestations may persist for several weeks or even months after the initial sting. Despite aggressive treatment, many skin injuries still result in significant pigmentation or scarring after recovery. To address this issue effectively, it is imperative to conduct comprehensive evidence-based medical research, elucidate various components within jellyfish venom, and elucidate its pathogenic mechanism to develop targeted treatment programs. This article aims to review the skin symptoms, pathophysiology, and management of jellyfish stings. Such considerations can provide comprehensive guidance to medical professionals and the public and minimize the harm caused by jellyfish stings.
Keywords: Cnidarian Venoms, review, Marine Toxins, Emergency Treatment, Humans, Bites and Stings, Animals, Skin, Cnidaria, Skin Diseases, Scyphozoa
Introduction
The jellyfish, a marine invertebrate zooplankton distributed worldwide, belongs to the phylum Cnidaria, which encompasses various other organisms such as fire coral, stinging hydroids, sea wasps, sea nettle, and anemones [1]. The phylum Cnidaria is classified into 6 classes: Scyphozoa, Hydrozoa, Cubozoa, Anthozoa, Myxozoa, and Staurozoa [2]. Among these classes, only Scyphozoa, Hydrozoa, and Cubozoa contain animals referred to as jellyfish [3]. In recent years there has been an increase in recurrent jellyfish outbreaks observed in the oceans, including the Mediterranean Sea and the North Pacific Ocean, thereby increasing the potential risk of jellyfish stings and associated envenomation [3–5]. The estimated number of jellyfish sting incidents per year is approximately 150 million, with fatalities and hospitalizations occurring annually, particularly in the Indo-Pacific regions [6]. Beyond being a public health issue, jellyfish also pose obstacles to various human activities, including diving, fishing, aquaculture, and tourism [7–9]. However, the precise pathogenic mechanisms and constituents of jellyfish venom remain unclear, and the management of jellyfish stings continues to be an important medical topic [10–13]. This article aims to review the skin symptoms, pathophysiology, and management of jellyfish stings, which could provide comprehensive guidance for healthcare professionals and the general public.
Sting Process
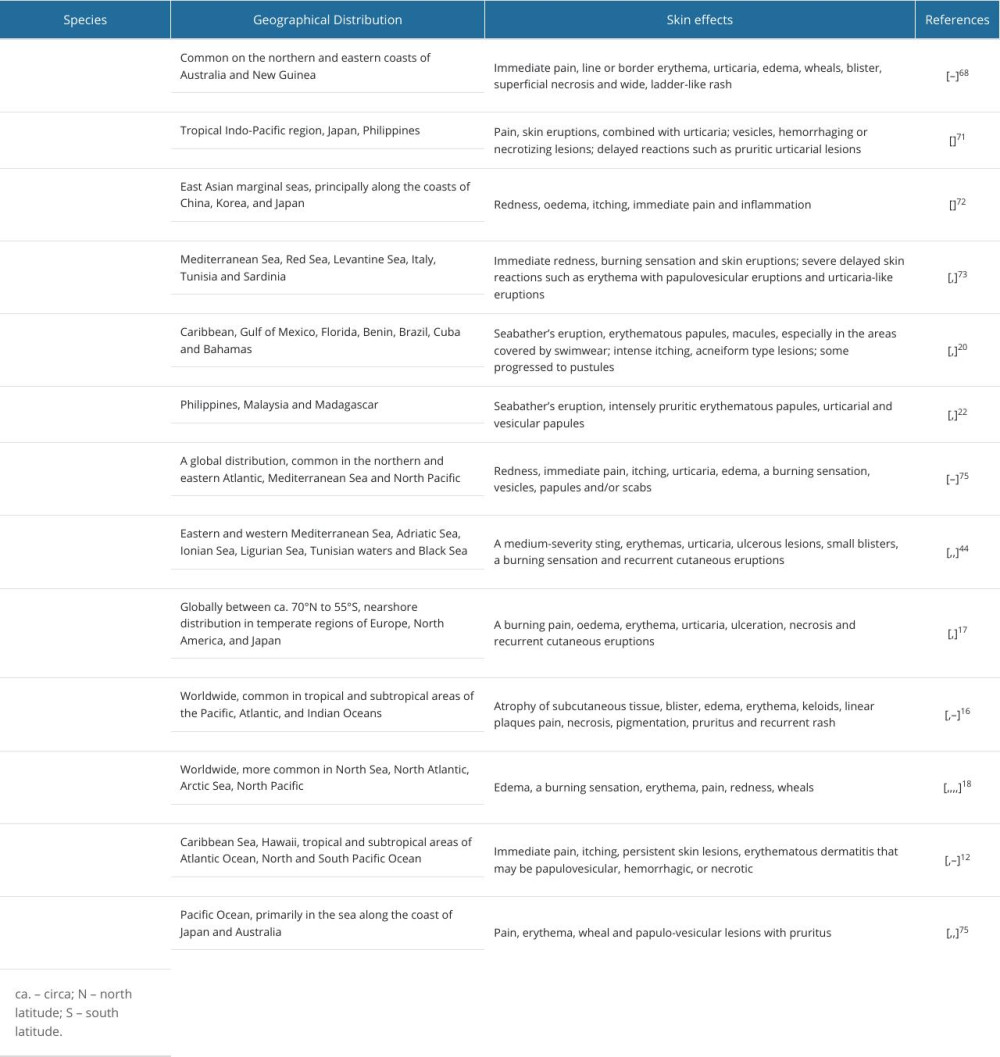
The geographical distribution and skin effects of stinging jellyfish are shown in Table 1. All geographic distribution maps of each jellyfish species are reproduced from the World Register of Marine Species (WoRMS) [2], with permission. However, these distributions may be deemed incomplete and should solely serve as a reference owing to the dynamic fluctuations in the global distribution of jellyfish and the limited data available on the WoRMS website.
The tentacles of jellyfish are densely covered with epidermal cells possessing specialized structures and functions, commonly referred to as cnidocytes [14]. Within the cnidocytes, there is a specialized organelle structure enclosed by a collagenous cystic shell known as the nematocyst [15]. Upon physical or chemical stimulation, the nematocysts undergo a rapid increase in static hydraulic pressure. The significant pressure disparity between the interior and exterior of the nematocysts ultimately propels the thread tube to function as a spring transmitter. Discharge of the tubule is one of nature’s most rapid mechanical events, which effectively penetrates human skin and delivers a substantial dose of jellyfish venom. The patient’s prognosis is contingent upon factors such as the jellyfish species, sting location, and individual characteristics [16,17].
Skin Symptoms
Most cutaneous manifestations and signs caused by jellyfish stings are nonspecific among the various classes. Generally, jellyfish stings start with feeling a prick, followed by subsequent swelling and burning or numbing sensations [16–18]. Subsequently, the sting rapidly induces erythema, papules, wheals, or jellyfish tentacle-like lesions characterized by linear, rope-like or whip-like marks accompanied by significant pain and itching. In severe cases, the skin develops obvious blisters, subcutaneous bleeding, and even ulcers or necrosis [6,16–18]. The local symptoms last 1–2 weeks or even several months. Despite proactive treatment, most stings leave noticeable skin pigmentation changes or scarring [19]. However, certain clinical characteristics of the lesion may raise suspicion regarding which Cnidaria class is responsible. For instance, Scyphozoan stings can cause jellyfish-shaped erythematous lesions, Hydrozoa stings can result in a linear rash with a “string of beads” appearance, and Cubozoan stings can leave whip-like marks that are relatively wide and cross-hatched, accompanied by a “frosted” appearance caused by superficial skin necrosis [3]. Seabather’s eruption (SBE), an acute dermatitis, is noteworthy, especially when caused by the thimble jellyfish
Immune Responses
The symptoms of jellyfish stings can arise indirectly from the body’s immune responses to toxin molecules and nematocysts, including skin lesions, inflammation, pyrexia, myoclonus, and paresthesia [24,25]. The proteins and polypeptides present in jellyfish venom, along with the collagen, glycoproteins, and polysaccharides found in the nematocysts, all can function as antigens or allergens within the human body, eliciting cellular or humoral immune responses [10,16]. Severe systemic allergic reactions sometimes occur, mainly due to prior exposure to antigenic toxins or similar biological components, and species-specific immunoglobulin antibodies in serum can remain high for several years [16,26]. Moreover, the multiple bioactive constituents within jellyfish venom can elicit immune responses via associated signaling pathways and cellular mechanisms [27,28]. For instance, Yap et al proposed that cnidarian pore-forming toxins (PFTs) exhibit similarities to bacterial PFTs, which can induce K+ efflux by penetrating the plasma membrane. Therefore, the reduction in intracellular K+ concentration activates NLRP3 inflammasome and p38 MAPK signaling pathways, regulating cytokine release and initiating immune responses [29]. Furthermore, mast cells, serving as potent promoters of inflammation, can be directly stimulated or their intrinsic or pattern recognition receptors can be activated by toxic components, resulting in degranulation and prompt release of cytokines such as histamine, prostaglandins, and leukotrienes, ultimately triggering accumulation or extravasation of immune cells at the sting site [30]. Additionally, chitin, collagen, polysaccharides, and other constituents within nematocysts can persistently activate proinflammatory innate immune cells such as Langerhans dendritic cells, macrophages, and mast cells, thereby resulting in persistent and recurrent symptoms of vesicular or pruritic dermatitis [10,16,29,31].
Toxins and Toxicity
Jellyfish toxins are mainly divided into 3 categories: Proteinoid toxins, non-protein toxins, and bioactive enzymes. These bioactive ingredients exhibit various biological toxicities including dermal necrosis, hemolysis, and adverse effects on cardiovascular, nervous, hepatic, and renal systems [11,32–34].
PFTs are a well-characterized group of toxin proteins that can be extracted from cnidarian venoms and are usually soluble in water at their very initial stage [35,36]. Most PFTs have potent cytotoxicity and lethality in mice, crayfish, sheep and humans. PFTs can interact with the cellular membrane, inducing structural and permeability alterations, which disrupts cells’ ion gradient, resulting in cellular infiltration, swelling, rupture, and cell death [29]. Additionally, 5 proteins belonging to the CaTX family of hemolysins, along with toxin components potentially involved in the formation of the membrane attack complex (MAC) such as perforin, have also been identified within the toxins derived from
Jellyfish venom can also contain histamine, 5-hydroxytryptamine, and kinin-like substances, which can induce local vasodilation in capillaries and venules [38,39]. Pain is a prevalent and distinctive symptom associated with stings, resulting from the contraction of smooth muscles other than vascular smooth muscles due to the biological impact of kinin and 5-hydroxytryptamines [16,40]. It has also been reported that moderate to severe pain is associated with a 200 μm-length piercing by the jellyfish tubule. In fact, deep penetration not only injects venom into dermal tissue, but also causes acute pain through physical stimulation of Aδ pain receptor fibers surrounding the plexus [41].
The enzymes in jellyfish venom can significantly upregulate the expression of inflammatory factors in dermal cells [42]. The suppressive effect of matrix metalloproteinase (MMP) inhibitors Batimastat, epigallocatechin gallate (EGCG), and ethylenediaminetetraacetic acid (EDTA) on toxic metalloproteinases-mediated skin damage suggested a pivotal role of metalloproteinases in the pathogenesis of jellyfish dermatitis [43]. Phospholipase, which is another prominent enzyme of jellyfish venom, has been identified in
Inhibiting Further Discharge of Tubules
Medical management of jellyfish stings is summarized in Figure 1. The primary concern is to promptly rescue the victim from potential drowning, followed by vigilant monitoring of vital signs, particularly for any indications of allergic reactions or systemic manifestations [16,18]. Simultaneously, prompt removal of any remaining tentacles and nematocysts from the skin is crucial to prevent further venom release [46].
Inhibiting further tubule discharge mitigates the influx of venom, but improper treatment can worsen the condition [17]. The recommended method is to delicately extract the tentacles using forceps or similar instruments, rather than the hands [10]. Some propose the application of sand or clothing to envelop the tentacles, followed by gentle wiping; however, this may induce pressure alterations that trigger tubule discharge [17]. Ballesteros et al identified ammonia, barium chloride, bleach, scented ammonia, carbonated cola, lemon juice, sodium chloride, and papain as substances capable of inducing nematocyst discharge, which should be avoided [47]. Rinsing with fresh water should also be avoided due to its lower osmotic pressure [16,48]. The ideal inhibition solution should be able to thoroughly eliminate the tentacles during rinsing and effectively impede or even deactivate the nematocysts [16–18].
The utilization of seawater for emergency treatment offers significant advantages owing to its inherent convenience. Experiments have substantiated that tubules of
Fenner et al reported that vinegar effectively inhibited tubule discharge, including
Saleratus solution has been proved to be effective in deactivating nematocysts of jellyfish, inhibiting the venom release and alleviating skin erythema [16,58,59]. However, Ballesteros et al observed that nematocysts will discharge in
An experimental study showed a 92% inhibitory efficacy of 50 mmol/L LaCl3 lotion on nematocyst discharge, and also demonstrated significant inhibition of tubule discharge by other metal cations, including K+, Ca2+, and Mg2+ [60]. Stingose, a commercial product containing 20% aluminum sulfate and 1.1% surfactant, is widely utilized for the treatment of marine life stings and has demonstrated effective relief for stings caused by
Urine, ammonia, 70% ethanol, isopropyl alcohol, and methylated alcohol have limited efficacy against most types of jellyfish stings and may even induce a vigorous discharge of nematocyst tubules [16–18,49]. However, there are exceptions. A 20% ammonia solution and a 70% ethanol solution have been reported to effectively reduce the chemosensory-induced tubule discharge of
In brief, there is still no universally applicable rinse solution available for an unidentified jellyfish sting. However, considering their widespread availability and effectiveness against a large number of jellyfish species, vinegar (5% acetic acid) and saleratus are recommended for immediate treatment in emergency situations. Furthermore, depending on the prevalent jellyfish species in specific regions, it is advisable for governmental authorities to proactively provide ready access to vinegar, saleratus, and certain types of metal cation solutions.
Reduction of Local Toxic Symptoms
In addition to removing the tentacles, appropriate measures should be taken to alleviate local pain and inflammation, as well as inactivate the toxin to limit further damage [16,18].
Hot compress or immersion in hot water is a commonly employed therapeutic approach for marine envenomation, but its underlying mechanism of action remains unclear [48]. Additionally, cold compress has demonstrated efficacy in pain reduction through restriction of inflammation and venom dissemination [17,62]. However, Li et al conducted a comprehensive review involving a total of 435 participants to compare the efficacy of hot and cold compresses after stings of
The study conducted by Burnett et al concluded that the sole use of lidocaine as the externally applied agent did not yield sufficient efficacy in pain management [64]. However, Birsa et al demonstrated that solutions containing 10% and 15% lidocaine hydrochloride could promptly alleviate pain induced by
Future Directions
Currently, researchers possess a limited comprehension of the clinical effects and mechanisms associated with jellyfish stings, primarily due to their reliance on a small number of cases. Given the extensive biological diversity exhibited by toxic jellyfish species, it is imperative to develop individualized treatment protocols due to the significant variation in symptoms resulting from jellyfish stings. Furthermore, despite the diverse range of symptoms caused by jellyfish stings, there remains insufficient empirical evidence to substantiate the presence of active venom components directly accountable for these clinical manifestations. Therefore, comprehensive analyses of venom components from each jellyfish species are required in the future. In addition, the mechanism of action and cytotoxic signaling pathways of bioactive toxin molecules should be further investigated and elucidated to establish a theoretical foundation for the development of targeted drugs against jellyfish stings. The optimal and effective emergency management of jellyfish stings lacks consensus, highlighting the need for standardized diagnostic criteria and treatment protocols in the near future to reduce mortality rates and improve prognosis.
Conclusions
Jellyfish stings can cause a variety of clinical manifestations, most notably skin lesions, and there is no specific treatment. In this article, we review the skin symptoms, pathophysiology, and management of jellyfish stings to provide guidance to healthcare professionals and the public. Further investigations should be conducted, with a focus on elucidating the pathogenic mechanisms of bioactive components in jellyfish venoms and developing effective control strategies. Additionally, standardized diagnostic criteria and treatment protocols should be established for different species of jellyfish to facilitate the comprehensive management of jellyfish stings.

References
1. Staggs R, Pay JL: Cnidaria toxicity, Treasure Island (FL), StatPearls Publishing https://www.ncbi.nlm.nih.gov/books/NBK538170/
2. : WoRMS – World Register of Marine Species https://www.marinespecies.org/index.php
3. Cunha SA, Dinis-Oliveira RJ, Raising awareness on the clinical and forensic aspects of jellyfish stings: A worldwide increasing threat: Int J Environ Res Public Health, 2022; 19(14); 8430
4. Gravili C, Jelly surge in the Mediterranean Sea: Threat or opportunity?: Mediterr Mar Sci, 2020; 21(1); 11-21
5. Schmitt C, De Haro L, Clinical marine toxicology: A European perspective for clinical toxicologists and poison centers: Toxins, 2013; 5(8); 1343-52
6. Boulware DR, A randomized, controlled field trial for the prevention of jellyfish stings with a topical sting inhibitor: J Travel Med, 2006; 13(3); 166-71
7. Bosch-Belmar M, Giomi F, Rinaldi A: Sci Rep, 2016; 6; 27929
8. Bosch-Belmar M, Milisenda G, Basso L, Jellyfish impacts on marine aquaculture and fisheries: Rev Fish Sci Aquac, 2020; 29(2); 242-59
9. Krzyżak J, Korzeniewski K, Marine creatures dangerous for divers in tropical waters: Int Marit Health, 2021; 72(4); 283-92
10. Tibballs J, Yanagihara AA, Turner HC, Immunological and toxinological responses to jellyfish stings: Inflamm Allergy Drug Targets, 2011; 10(5); 438-46
11. Jouiaei M, Yanagihara A, Madio B, Ancient venom systems: A review on cnidaria toxins: Toxins, 2015; 7(6); 2251-71
12. McGee RG, Webster AC, Lewis SR, Interventions for the symptoms and signs resulting from jellyfish stings: Cochrane Database Syst Rev, 2023; 6(6); CD009688
13. Warrell DA, Venomous bites, stings, and poisoning: An update: Infect Dis Clin North Am, 2019; 33(1); 17-38
14. DeLoughery EP, There’s something in the water: An overview of jellyfish, their stings, and treatment: Int Marit Health, 2022; 73(4); 199-202
15. Amreen Nisa S, Vinu D, Krupakar P, Jellyfish venom proteins and their pharmacological potentials: A review: Int J Biol Macromol, 2021; 176; 424-36
16. Montgomery L, Seys J, Mees J, To pee, or not to pee: A review on envenomation and treatment in European jellyfish species: Mar Drugs, 2016; 14(7); 127
17. Remigante A, Costa R, Morabito R, Impact of scyphozoan venoms on human health and current first aid options for stings: Toxins, 2018; 10(4); 133
18. Cegolon L, Heymann W, Lange J, Jellyfish stings and their management: A review: Mar Drugs, 2013; 11(12); 523-50
19. Tønseth KAHealth damage after jellyfish stings: Tidsskr Nor Laegeforen, 2007; 127(13); 1777-78 [in Norwegian]
20. Rossetto AL, Proença LA, de O, Seabather’s eruption: Report of case in northeast region of Brazil: An Bras Dermatol, 2012; 87; 472-74
21. de Arauyo Eyer-Silva W, Pitombo FB, Rosa da Silva GA, Seabather’s eruption in Ipanema Beach, Rio de Janeiro, Brazil: Rev Soc Bras Med Trop, 2018; 51; 119
22. Guevara BEK, Dayrit JF, Haddad V: Clin Exp Dermatol, 2017; 42(7); 808-10
23. Chuan CH, Venmathi Maran BA, Yap TK, New records of cubozoan and scyphozoan jellyfish from Sabah Waters, Malaysia: Diversity, 2021; 13(9); 420
24. Bordehore C, Nogué S, Gili J: J Travel Med, 2015; 22(1); 61-63
25. Glatstein M, Adir D, Galil B, Pediatric jellyfish envenomation in the Mediterranean Sea: Eur J Emerg Med, 2018; 25(6); 434-39
26. Amato G, Vita F, Gemelli F, Jellyfish anaphylaxis: A wide spectrum of sensitization routes: Allergy Asthma Proc, 2020; 41(3); 158-66
27. Yu C, Yin X, Li A, Toxin metalloproteinases exert a dominant influence on pro-inflammatory response and anti-inflammatory regulation in jellyfish sting dermatitis: J Proteomics, 2024; 292; 105048
28. Choudhary I, Hwang D, Chae J, Proteomic changes during the dermal toxicity induced by nemopilema nomurai jellyfish venom in HaCaT human keratinocyte: Toxins (Basel), 2021; 13(5); 311
29. Yap W, Hwang J, Response of cellular innate immunity to cnidarian pore-forming toxins: Molecules, 2018; 23(10); 2537
30. Prasad P, Yanagihara AA, Small-Howard AL, Secretogranin III directs secretory vesicle biogenesis in mast cells in a manner dependent upon interaction with chromogranin A: J Immunol, 2008; 181(7); 5024-34
31. Yanagihara AA, Wilcox C, Smith J, Cubozoan envenomations: Clinical features, pathophysiology and management: The cnidaria, past, present and future: The world of medusa and her sisters, 2016; 637-52, Springer International Publishing
32. D’Ambra I, Lauritano C, A review of toxins from cnidaria: Mar Drugs, 2020; 18(10); 507
33. Yang F, Yang K, Wang Y, Insights into the discovery and intervention of metalloproteinase in marine hazardous jellyfish: J Hazard Mater, 2024; 472; 134526
34. Frazão B, Vasconcelos V, Antunes A, Sea anemone (Cnidaria, Anthozoa, Actiniaria) toxins: An overview: Mar Drugs, 2012; 10(12); 1812-51
35. Klompen AML, Kayal E, Collins AG, Cartwright P, Phylogenetic and selection analysis of an expanded family of putatively pore-forming jellyfish toxins (Cnidaria: Medusozoa): Genome Biol Evol, 2021; 13(6); evab081
36. Gupta LK, Molla J, Prabhu AA, Story of pore-forming proteins from deadly disease-causing agents to modern applications with evolutionary significance: Mol Biotechnol, 2024; 66(6); 1327-56
37. Rachamim T, Morgenstern D, Aharonovich D, The dynamically evolving nematocyst content of an anthozoan, a scyphozoan, and a hydrozoan: Mol Biol Evol, 2015; 32(3); 740-53
38. Badré S, Bioactive toxins from stinging jellyfish: Toxicon, 2014; 91; 114-25
39. Shuhua Huo, Shuguang Xu, Xiaoyun SuResearch progress on jellyfish stings: Chin J Emerg Med, 2017; 26(2); 249-50 [in Chinese]
40. Chongyang Z, Qingyi M, Zewu Q2014 Expert Consensus on the Treatment of Jellyfish Stings in China: Clin Misdiagnosis Mistreatment, 2014(10); 1-5 [in Chinese]
41. Kitatani R, Yamada M, Kamio M, Length is associated with pain: Jellyfish with painful sting have longer nematocyst tubules than harmless jellyfish: PLoS One, 2015; 10(8); e0135015
42. Li A, Yu H, Li R: Toxins, 2019; 11(3); 156
43. Hwang DH, Lee H, Choudhary I, Protective effect of epigallocatechin-3-gallate (EGCG) on toxic metalloproteinases-mediated skin damage induced by Scyphozoan jellyfish envenomation: Sci Rep, 2020; 10(1); 18644
44. Mariottini GL, Pane L, Mediterranean jellyfish venoms: A review on scyphomedusae: Mar Drugs, 2010; 8(4); 1122-52
45. Yue Y, Yu H, Li R: Toxins, 2017; 9(2); 47
46. Yanagihara AA, Wilcox CL, Cubozoan sting-site seawater rinse, scraping, and ice can increase venom load: Upending current first aid recommendations: Toxins (Basel), 2017; 9(3); 105
47. Ballesteros A, Trullas C, Jourdan E: Mar Drugs, 2022; 20(9); 571
48. Ward NT, Darracq MA, Tomaszewski C, Evidence-based treatment of jellyfish stings in North America and Hawaii: Ann Emerg Med, 2012; 60(4); 399-414
49. Birsa LM, Verity PG, Lee RF, Evaluation of the effects of various chemicals on discharge of and pain caused by jellyfish nematocysts: Comp Biochem Physiol Part C Toxicol Pharmacol, 2010; 151(4); 426-30
50. Pyo MJ, Lee H, Bae SK: Toxicon, 2016; 109; 26-32
51. Burnett JW, Rubinstein H, Calton GJ, First aid for jellyfish envenomation: South Med J, 1983; 76(7); 870-72
52. Doyle T, Headlam J, Wilcox C: Toxins, 2017; 9(7); 215
53. Fenner PJ, Williamson J, Callanan VI: Med J Aust, 1986; 145(11–12); 569-74
54. Mianzan HW, Fenner PJ, Cornelius PF: Cutis, 2001; 68(1); 45-48
55. Yanagihara A, Wilcox C, King R: Toxins, 2016; 8(1); 19
56. Wilcox C, Headlam J, Doyle T: Toxins, 2017; 9(5); 149
57. Edelist D, Angel DL, Barkan N: Regional Environ Change, 2023; 23(3); 114
58. Fenner PJ, Williamson J: Med J Aust, 1987; 147(5); 258-59
59. DeClerck MP, Bailey Y, Craig D: Wilderness Environ Med, 2016; 27(1); 25-38
60. Ling Han, Ying Lu, Jiaxin LiResearch progress on multi-effect protective agents for the navy: China Surfactant Deterg Cosmet, 2018; 48(11); 656-660 [in Chinese]
61. Morabito R, Marino A, Dossena S: Toxicon, 2014; 83; 52-58
62. Exton DR, Fenner PJ, Williamson JA, Cold packs: Effective topical analgesia in the treatment of painful stings by Physalia and other jellyfish (for editorial comment, see page 610; see also pages 621, 626 and 708): Med J Aust, 1989; 151(11–12); 625-26
63. Wilcox C, Yanagihara A, Heated debates: Hot-water immersion or ice packs as first aid for cnidarian envenomations?: Toxins, 2016; 8(4); 97
64. Burnett JW, Treatment of Atlantic cnidarian envenomations: Toxicon, 2009; 54(8); 1201-5
65. Lubbock R, Amos WB, Removal of bound calcium from nematocyst contents causes discharge: Nature, 1981; 290(5806); 500-1
66. Yanagihara AA, Shohet RV, Cubozoan venom-induced cardiovascular collapse is caused by hyperkalemia and prevented by zinc gluconate in mice: PLoS One, 2012; 7(12); e51368
67. Yanagihara AA, Methods and compositions for treating and/or inhibiting toxins using copper-containing compounds: Google Patents, 2019 https://patents.google.com/patent/US10172883B2/en
68. Mebs D, Durch Quallen verursachte Verletzungen: Hautarzt, 2014; 65(10); 873-78
69. Winter KL, Isbister GK, McGowan S: Toxicol Lett, 2010; 192(3); 419-24
70. Auerbach PS, Gupta D, Van Hoesen K, Dermatological progression of a probable box jellyfish sting: Wilderness Environ Med, 2019; 30(3); 310-20
71. Horiike T, Nagai H, Kitani S: Int Arch Allergy Immunol, 2015; 167(2); 73-82
72. Hwang DH, Koh PO, Mohan Prakash RL: Toxins, 2022; 14(12); 831
73. Uri S, Marina G, Liubov G: Contact Dermatitis, 2005; 52(5); 282-83
74. Giallongo G, Douek J, Harbuzov Z, Long-term changes in population genetic features of a rapidly expanding marine invader: Implication for invasion success: Biol Invasions, 2021; 23(8); 2541-52
75. Tibballs J, Australian venomous jellyfish, envenomation syndromes, toxins and therapy: Toxicon, 2006; 48(7); 830-59
76. Miller B, von der Heyden S, Gibbons M: Afr J Mar Sci, 2012; 34(3); 425-30
77. Ballesteros A, Marambio M, Fuentes V: Toxins, 2021; 13(8); 509
78. Leoni V, Bonnet D, Ramírez-Romero E: Glob Ecol Biogeogr, 2021; 30(3); 622-39
79. Ballesteros A, Marambio M, Trullas C: Int J Environ Res Public Health, 2023; 20(3); 2344
80. Hamner WM, Dawson MN, A review and synthesis on the systematics and evolution of jellyfish blooms: Advantageous aggregations and adaptive assemblages: Hydrobiologia, 2009; 616(1); 161-91
81. Yang K, Klausner JD: Am J Trop Med Hyg, 2023; 109(1); 201-4
82. Labadie M, Aldabe B, Ong N: Clin Toxicol, 2012; 50(7); 567-70
83. Haddad V, da Silveira FL, Cardoso JLC, A report of 49 cases of cnidarian envenoming from southeastern Brazilian coastal waters: Toxicon, 2002; 40(10); 1445-50
84. Reese E, Depenbrock P, Water envenomations and stings: Curr Sports Med Rep, 2014; 13(2); 126-31
85. Helmholz H, Ruhnau C, Schütt C: Toxicon, 2007; 50(1); 53-64
86. Hoffmann FR, Jungblut S, Holst S, Therapieoptionen bei Vernesselungen durch Quallen an deutschen Küstengewässern: Notf Rettungsmedizin, 2017; 20(5); 403-9
87. Tamanaha RH, Izumi AK: J Am Acad Dermatol, 1996; 35(6); 991-93
88. Lewis C, Bentlage B, Yanagihara A: Zootaxa, 2013; 3737(4); 473
89. Lawley JW, Ames CL, Bentlage B: Biol Bull, 2016; 231(2); 152-69
90. Hammill E, Johnson E, Atwood TB, Ocean acidification alters zooplankton communities and increases top-down pressure of a cubozoan predator: Glob Change Biol, 2018; 24(1); e128-e38
91. Ohtaki N, Oka K, Sugimoto A: J Dermatol, 1990; 17(2); 108-14
In Press
Clinical Research
Comparative Effectiveness of a Nurse-Led Care Model vs Usual Care in Rheumatoid Arthritis: A Longitudinal C...Med Sci Monit In Press; DOI: 10.12659/MSM.953211
Clinical Research
Impact of Treatment Modality on Pain, Sexual Function, and Psychological Well-Being in Patients With Bartho...Med Sci Monit In Press; DOI: 10.12659/MSM.952422
Clinical Research
Association Between Radiographic Knee Osteoarthritis, Pre-Fracture Mobility, and Hip Fracture Patterns in O...Med Sci Monit In Press; DOI: 10.12659/MSM.952678
Clinical Research
Association Between Total Cholesterol–to–High-Density Lipoprotein Ratio and Gestational Hypertension: A Cas...Med Sci Monit In Press; DOI: 10.12659/MSM.952395
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,084
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,757,530
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,116
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,768
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387