21 September 2024: Clinical Research
Comparison of Remimazolam and Dexmedetomidine for Sedation in Awake Endotracheal Intubation in Scoliosis Surgery: A Retrospective Analysis
Lei Zhou1ABDEF*, Yu Huang2ABDEF, Rui Zhou3CDE, Siyuan Liu1ADEFDOI: 10.12659/MSM.944632
Med Sci Monit 2024; 30:e944632






Abstract
BACKGROUND: Awake endotracheal intubation (AEI) involves the placement of an endotracheal tube in patients who can maintain spontaneous respirations. This retrospective study aimed to compare sedation with remimazolam during AEI with that of dexmedetomidine in patients who underwent scoliosis correction surgery.
MATERIAL AND METHODS: This is a retrospective study based on data from 98 patients who had AEI procedures between January and December 2023. The remimazolam group included 55 patients, and the dexmedetomidine group included 43 patients. Remimazolam 0.05 mg/kg was injected 1 min before intubation, while dexmedetomidine 1 ug/kg was pumped 10 min before intubation. Evaluations of AEI, hemodynamics, and respiratory adverse events were then compared between the 2 groups.
RESULTS: There was no significant difference in demographic data between the groups. After administrating sedation, dexmedetomidine led to a larger reduction of mean arterial pressure (MAP) and heart rate (HR) than did remimazolam (11.30±1.86 vs 8.33±2.28 mmHg, P<0.001; 12.28±2.50 vs 2.85±1.82 beats/min, P<0.001). When conducting intubation, the increase of MAP in the remimazolam group was lower than that in the dexmedetomidine group (7.40±2.81 vs 9.26±5.08 mmHg, P=0.024), while the difference in HR change was not significant (7.53±5.41 vs 8.37±5.31 beats/min, P=0.441). When combined with local anesthesia, the success rate of AEI, time of AEI procedure, attempt times, increase of MAP during intubation, depth of sedation, and respiratory adverse events were comparable between the groups (P>0.05).
CONCLUSIONS: With local anesthesia, remimazolam and dexmedetomidine sedation can facilitate AEI for patients with scoliosis. However, remimazolam is associated with more stable hemodynamics.
Keywords: Intubation, Intratracheal, airway management, Scoliosis, Dexmedetomidine, Remimazolam, Humans, Retrospective Studies, Female, Male, Hypnotics and Sedatives, Wakefulness, Adolescent, Benzodiazepines, Hemodynamics, Heart Rate, adult, Conscious Sedation
Introduction
Scoliosis is described as aberrant curvature and rotation of the spine. Scoliosis can be idiopathic or caused by other diseases and is usually diagnosed when patients are at a young age [1]. Patients with scoliosis often have varying degrees of cardiopulmonary dysfunction, pain, and low quality of life. Surgical correction is an effective way to improve a patient’s condition. In particular, patients with a large Cobb angle (≥50°) and rapid progress (≥10° per year) should consider surgery [2]. Awake endotracheal intubation (AEI), also known as awake tracheal intubation [3], is often required during surgical anesthesia in patients with scoliosis, due to abnormal head and neck motion or postoperative placement of external stents that restrict head and neck motion [4].
AEI is still the most widely accepted strategy for an expected difficult airway, owing to the high security and success rate [5]. Although AEI can be conducted with only local anesthesia, sedation is commonly applied during the procedure to alleviate stress and improve patients’ cooperation. Remifentanil and dexmedetomidine are highly recommended sedatives [5,6]. However, there are some concerns about the 2 drugs. Remifentanil, one kind of opioid, significantly depresses the respiratory system [7,8], which is extremely risky for patients with scoliosis. Dexmedetomidine invariably leads to bradycardia by inhibiting norepinephrine release and sympathetic nervous system activity [9,10]. Moreover, dexmedetomidine-induced bradycardia can even cause cardiac arrest in high-risk patients [11]. Thus, a novel strategy for AEI is needed.
Remimazolam, a benzodiazepine, has been widely recognized by anesthesiologists for its effectiveness and safety [12,13]. More importantly, it has little effect on the cardiovascular system and spontaneous respiration [14,15]. In addition, Murata et al reported a case in which the patient completed awake craniotomy and showed good tolerance after discontinuation of remimazolam [16]. Therefore, remimazolam is an ideal candidate for AEI sedation. However, studies on AEI sedation with remimazolam for scoliosis surgery are still lacking. Therefore, this retrospective study aimed to compare sedation with remimazolam during AEI with dexmedetomidine in 98 patients undergoing surgery for scoliosis between January and December 2023.
Material and Methods
ETHICS STATEMENT:
This study was designed as a retrospective study, since rectifying surgery for scoliosis has been suspended in our institution for various reasons. Ethics issue for this was approved by the Ethics Committee of the Second Affiliated Hospital of Chengdu Medical College (China National Nuclear Corporation 416 Hospital). The approval number is YJ-2024-020. Written informed consent was not required.
RETROSPECTIVE DATA SOURCE:
Adult patients who underwent scheduled correction surgery for scoliosis with AEI were considered eligible. Medical records for these patients from January 1, 2023, to December 31, 2023, at our hospital were extracted to establish the database. The reason for the timespan is that remimazolam was first used in AEI after January 1, 2023, and the surgery was suspended on January 1, 2024. According to the records and our habit of AEI sedation, 2 groups were established: remimazolam group (AEI with remimazolam) and dexmedetomidine group (AEI with dexmedetomidine). Cases of patients with incomplete data reports or pre-administration of other sedatives and those with preoperative hypoxia or hypertension were excluded.
DESCRIPTION OF AEI:
After entering the operation room, patients were routinely monitored with electrocardiograph, SpO2, invasive blood pressure (IBP), and bispectral index (BIS). Dexmedetomidine or remimazolam was the sedative for patients. Accordingly, patients were divided into the dexmedetomidine group and remimazolam group when we retrospectively screened the medical records. Ten minutes before intubation, dexmedetomidine (Yangtze River Pharmaceutical Group, Jiangsu, China) was continuously pumped with a dosage of 1 ug/kg (ie, the rate for a patient of 50 kg is 300 ug/h), and methylprednisolone (Pfizer Manufacturing Belgium NV, Belgium) 40 mg, penehyclidine (Nhwa Pharmaceutical Cooperation, Jiangsu, China) 0.01 mg/kg, and ramosetron (Lummy Pharmaceutical Cooperation, Chongqing, China) 0.3 mg were injected via peripheral venous administration. Tetracaine mucilage (Lijun Pharmaceutical Cooperation, Xi’an, China) 5 mL was then applied to perform the surface anesthesia of the mouth and throat. Five minutes before intubation, sufentanil (Humanwell Healthcare, Yichang, China) 0.01 ug/kg was administered intravenously. One minute after performing cricothyroid membrane puncture and rapid endotracheal injection of 1% lidocaine (Harvest Pharmaceutical Cooperation, Shanghai, China) 2 mL, endotracheal intubation was conducted with the guidance of a fiber bronchoscope. Remimazolam (Hengrui Medicine, Jiangsu, China) 0.05 mg/kg was injected when performing cricothyroid membrane puncture and injection of lidocaine 1 min before intubation. For unsuccessfully intubated cases, intubation was performed again upon SpO2 rising to baseline. The patients were sent back to the ward after 3 failed attempts, and the surgery was delayed.
OUTCOMES:
The primary outcome was successful AEI rate of the first attempt. The secondary outcomes were as follows: (1) time to successful AEI (from AEI procedure initiation to successful intubation), (2) number of attempts to AEI, (3) mean arterial pressure (MAP) change (from sedative administration to intubation, and before and after intubation), (4) heart rate (HR) change (from sedative to the moment before intubation, and from the moment before intubation to intubation procedure), (5) BIS value before and during intubation, (6) successful rate of AEI, (7) incidence of hypoxia before intubation initiation, and (8) the first value of end-tidal CO2 (EtCO2) after intubation. These data were collected from electronic records of the Anesthesia Information Management System.
DATA EXTRACTION:
Two investigators blinded to the group assignments screened each case separately to determine the eligibility of the records, and subsequently, extracted the related data. Disagreements between the investigators were settled by discussion or by consulting an attending expert. All investigators were well trained. A senior investigator did a spot check to verify the reliability of the data.
STATISTICAL ANALYSIS:
EpiData 3.1 was used to input the extracted data, and the data were imported into SPSS 26.0 for storage and analysis. Categorical variables, such as successful rate of AEI and incidence of hypoxia before intubation initiation, were expressed as the number of cases (percentage) and analyzed by the chi-square test. The measurement data were first tested for normality (Kolmogorov-Smirnov test). The variables with a normal distribution, such as MAP, HR, BIS, and EtCO2, were expressed as mean ± standard deviation (SD) and analyzed by independent-sample
Results
COMPARISON OF BASELINE:
The demographic data were comparable between the remimazolam group and dexmedetomidine group, including sex, age, height, body mass index (BMI), and Mallampati classification, although the weight of the remimazolam group was higher than that of the dexmedetomidine group (44.22±5.42 vs 42.05±4.04 kg, P=0.031) (Table 1).
COMPARISON OF AEI-RELATED INDICATORS:
The successful AEI rate of the first attempt was 70.91% (39/55) in the remimazolam group and 65.12% (28/43) in the dexmedetomidine group, with no significant difference between the 2 groups (P=0.541, Figure 3A). There were 3 cases of failure to conduct AEI, with 1 in the remimazolam group and 2 in the dexmedetomidine group (Figure 3B). The reason in the medical records was described as difficult glottis exposure. The overall success rate of AEI had no significant difference between the groups (98.18% vs 95.35%, P=0.580, Figure 3B). According to the practice guideline in our department, endotracheal intubation should not be conducted more than 3 times; therefore, the 3 patients had failed attempts in AEI. They were sent back to the ward, as the medical records documented, and their surgeries were delayed. The attempt times to successful AEI were similar in both groups (1(1,2) vs 1(1,2), P=0.487). Figure 3C shows the cases of different attempts. Also, there was no significant difference in the total time taken by anesthesiologists to conduct AEI between the groups (11(11,14) vs 11(11,15) min, P=0.535, Figure 3D).
COMPARISON OF HEMODYNAMICS:
After administration of remimazolam or dexmedetomidine, the blood pressure (BP) of the patients was significantly decreased. In comparison with that in the dexmedetomidine group, the decrease of MAP in the remimazolam group was significantly less during sedation and the moment before intubation (8.33±2.28 vs 11.30±1.86 mmHg, P<0.001, Figure 4A). Moreover, when conducting intubation, the increase of MAP in the remimazolam group was lower than that of the dexmedetomidine group (7.40±2.81 vs 9.26±5.08 mmHg, P=0.024, Figure 4B). In comparison with that of dexmedetomidine, the decrease of HR caused by remimazolam was significantly lower before intubation (2.85±1.82 vs 12.28±2.50 beats/min, P<0.001, Figure 4C). However, the increase of HR induced by remimazolam was similar to that of dexmedetomidine (7.53±5.41 vs 8.37±5.31 beats/min, P=0.441, Figure 4D).
COMPARISON OF DEGREE OF SEDATION AND RESPIRATORY EVENTS:
The BIS value was equivalent between the remimazolam and dexmedetomidine groups, whether before intubation or during intubation (82.65±1.89 vs 82.33±1.82, P=0.387; 90.75±3.03 vs 91.05±3.17, P=0.634, respectively, Figure 5). Although some patients had hypoxia after the sedative, the difference was not significant (9.09% vs 18.60%, P=0.168, Figure 6A). In addition, there was no significant difference in the first EtCO2 after successful intubation (41.78±2.89 vs 41.49±3.40 mmHg, P=0.654, Figure 6B).
Discussion
We conducted a retrospective study on the comparison of remimazolam and dexmedetomidine in AEI. The results indicated that AEI could be successfully performed under remimazolam or dexmedetomidine sedation, but remimazolam was associated with more stable hemodynamics.
AEI is still regarded as the foremost choice for a difficult airway [17]. Successful AEI is determined by the airway anatomy of patients, dexterity of operators, operating apparatus, and well-controlled stimulation. It has been reported that over 90% of patients with an anticipated difficult airway can undergo successful AEI with proper methods [18,19]. The result of this study is consistent with these reports. Under the procedure of our institution, overall success rate of the first attempt was comparable in the remimazolam group and the dexmedetomidine group. We gave up trying a fourth time, as repeated intubation increases the likelihood of injury, bleeding, and edema [20,21].
Nevertheless, patients are commonly distressed due to the intensive stimulation induced by AEI. In spite of propofol and local anesthesia, patients can still experience nausea or bucking [22]. Sedation can make it a more tolerable and comfortable process for the patients, especially for those who are particularly anxious or sensitive. Moreover, the stimulation can lead to huge hemodynamic fluctuation, such as a sudden increase of BP and tachycardia. It is reported that AEI under local anesthesia and sedation with midazolam and fentanyl can lead to significant hemodynamic changes (HR increase >20 beats/min, systolic BP increase >20 mmHg), and the changes last for more than 5 min [23]. In our study, sedation under either remimazolam or dexmedetomidine combined with local anesthesia effectively suppressed intubation-induced stress, as the increase of HR and MAP was less than 10 beats/min and 10 mmHg, respectively. However, the dexmedetomidine-induced decrease of MAP after sedation and intubation-induced increase of MAP were significantly larger than that of remimazolam, which means remimazolam performed better in minimizing BP fluctuation. Also, remimazolam had little effect on HR, while dexmedetomidine caused significant decreases in HR. Recently, the continuous administration of remimazolam for AEI was successfully performed in maxillofacial surgery; however, the results indicated no significant differences in hemodynamic parameters between dexmedetomidine and remimazolam [24]. The different effects may be attributed to the cardiopulmonary dysfunction of patients with scoliosis [25].
Sedatives can result in hypoventilation, and some vulnerable patient’s conditions even deteriorate into resultant hypoxia and hypercarbia [26,27]. According to the records, 5 patients in the remimazolam group and 8 in the dexmedetomidine group had hypoxia that could be rectified by reminding the patients to breathe deeply. The first value of EtCO2 after intubation was far lower than the upper limit of the normal range, which further proves the steerable and safe sedation induced by remimazolam or dexmedetomidine.
The primary limitation of this study is the study design. The optimal design to compare remimazolam with dexmedetomidine in AEI is a prospective randomized trial. In this way, the tolerance degree can be directly reflected by evaluating patient responses, such as patient discomfort scores and post-intubation scores [28,29]. The present study was designed as a retrospective study because scoliosis correction was suspended this year in our hospital. Another limitation is that the relatively low prevalence of scoliosis and limited timespan lead to the small sample size. Even so, the present study can provide preliminary results, and further studies should be conducted.
Conclusions
This retrospective study indicates that both remimazolam and dexmedetomidine sedation combined with local anesthesia can facilitate AEI for patients with scoliosis. However, remimazolam is associated with more stable hemodynamics. Prospective randomized trials are needed to verify our findings.
Figures
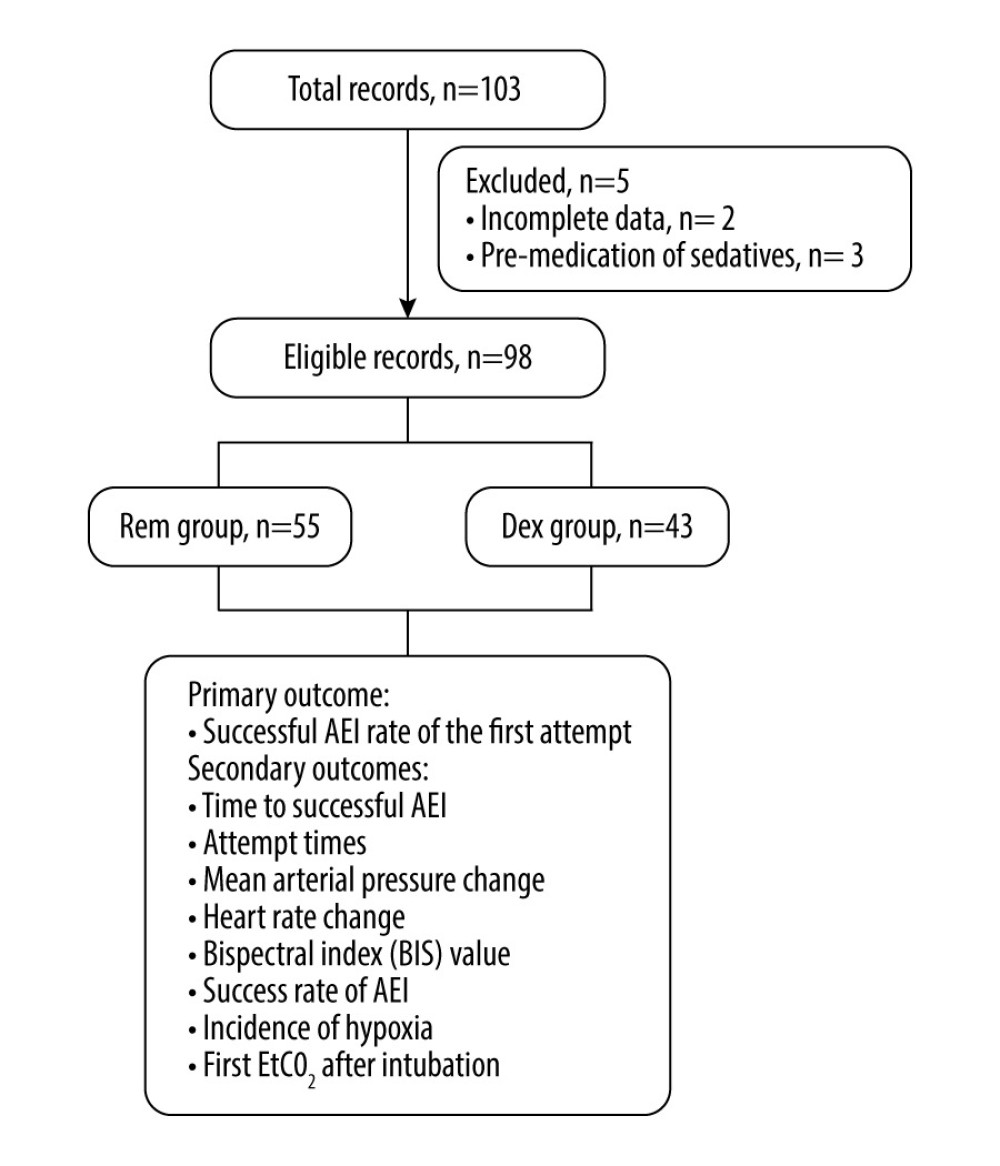 Figure 1. Study flowchart. Rem – remimazolam; Dex – dexmedetomidine; AEI – awake endotracheal intubation; EtCO2 – end-tidal carbon dioxide.
Figure 1. Study flowchart. Rem – remimazolam; Dex – dexmedetomidine; AEI – awake endotracheal intubation; EtCO2 – end-tidal carbon dioxide.  Figure 2. X-ray (A) and computed tomography (B, C) images of scoliosis in our study.
Figure 2. X-ray (A) and computed tomography (B, C) images of scoliosis in our study.  Figure 3. Intubation-related parameters. (A) Success rate for the first attempt. (B) Overall success rate. (C) Comparison of attempt times. (D) Time of awake intubation procedure. Rem – remimazolam; Dex – dexmedetomidine
Figure 3. Intubation-related parameters. (A) Success rate for the first attempt. (B) Overall success rate. (C) Comparison of attempt times. (D) Time of awake intubation procedure. Rem – remimazolam; Dex – dexmedetomidine  Figure 4. Hemodynamic changes. (A) Decrease of mean arterial pressure (MAP) after administrating remimazolam or dexmedetomidine. (B) Increase of MAP when intubating. (C) Decrease of heart rate (HR) after administrating remimazolam or dexmedetomidine. (D) Increase of HR when intubating. Rem – remimazolam; Dex – dexmedetomidine. * P<0.05; ** P<0.001.
Figure 4. Hemodynamic changes. (A) Decrease of mean arterial pressure (MAP) after administrating remimazolam or dexmedetomidine. (B) Increase of MAP when intubating. (C) Decrease of heart rate (HR) after administrating remimazolam or dexmedetomidine. (D) Increase of HR when intubating. Rem – remimazolam; Dex – dexmedetomidine. * P<0.05; ** P<0.001.  Figure 5. Comparison of bispectral index (BIS) value. Rem – remimazolam; Dex – dexmedetomidine.
Figure 5. Comparison of bispectral index (BIS) value. Rem – remimazolam; Dex – dexmedetomidine.  Figure 6. Comparison of respiratory adverse events. (A) The number of patients with and without hypoxia. (B) The first end-tidal carbon dioxide (EtCO2) value after intubation. Rem – remimazolam; Dex – dexmedetomidine.
Figure 6. Comparison of respiratory adverse events. (A) The number of patients with and without hypoxia. (B) The first end-tidal carbon dioxide (EtCO2) value after intubation. Rem – remimazolam; Dex – dexmedetomidine. 
References
1. Mesiti BL, Scoliosis: An overview: Radiol Technol, 2021; 93(1); 55-72
2. Boulay C, Peltier E, Jouve JL, Pesenti S, Functional and surgical treatments in patients with spinal muscular atrophy (SMA): Arch Pediatr, 2020; 27(7S); 7S35-7S39
3. Chen Q, Qin B, Zhang M, The safety and efficacy of remimazolam compared to dexmedetomidine for awake tracheal intubation by flexible bronchoscopy: A randomized, double-blind, controlled trial: Drug Des Devel Ther, 2024; 18; 967-78
4. Hudec J, Prokopová T, Kosinová M, Gál R, Anesthesia and perioperative management for surgical correction of neuromuscular scoliosis in children: A narrative review: J Clin Med, 2023; 12(11); 3651
5. Vora J, Leslie D, Stacey M, Awake tracheal intubation: BJA Educ, 2022; 22(8); 298-305
6. Ahmad I, El-Boghdadly K, Bhagrath R, Difficult Airway Society guidelines for awake tracheal intubation (ATI) in adults: Anaesthesia, 2020; 75(4); 509-28
7. Baldo BA, Toxicities of opioid analgesics: Respiratory depression, histamine release, hemodynamic changes, hypersensitivity, serotonin toxicity: Arch Toxicol, 2021; 95(8); 2627-42
8. Nie J, Chen W, Jia Y, Comparison of remifentanil and esketamine in combination with propofol for patient sedation during fiberoptic bronchoscopy: BMC Pulm Med, 2023; 23(1); 254
9. Zhong Q, Kumar A, Deshmukh A, Bennett C, Dexmedetomidine reduces incidences of ventricular arrhythmias in adult patients: a meta-analysis: Cardiol Res Pract, 2022; 2022; 5158362
10. Gavino L, Willaredt M, Chiche JD, Ben-Hamouda NAlpha-2 adrenoreceptor agonists for the intensive care physician: Rev Med Suisse, 2023; 19(825); 872-877 [in French]
11. Bahraini A, Banerjee O, Ra J, Bradycardia resulting in cardiac arrest in a critically ill patient receiving dexmedetomidine: Trauma Case Rep, 2021; 36; 100548
12. Rex DK, Bhandari R, Lorch DG, Safety and efficacy of remimazolam in high risk colonoscopy: A randomized trial: Dig Liver Dis, 2021; 53(1); 94-101
13. Hu Q, Liu X, Wen C, Remimazolam: An updated review of a new sedative and anaesthetic: Drug Des Devel Ther, 2022; 16; 3957-74
14. Huang Y, Zheng D, Xu K, Randomized, single-blind, comparative study of remimazolam besylate vs propofol for facial plastic surgery: Aesthet Surg J, 2024; 44(6); NP357-NP364 [Erratum in: Aesthet Surg J. 2024;44(6):NP443]
15. Zhu X, Wang H, Yuan S, Efficacy and safety of remimazolam in endoscopic sedation – a systematic review and meta-analysis: Front Med (Lausanne), 2021; 8; 655042
16. Murata H, Yokoyama A, Hara T, Remimazolam and low-dose flumazenil for awake craniotomy: J Anesth, 2022; 36(6); 789-90
17. Apfelbaum JL, Hagberg CA, Connis RT, 2022 American Society of Anesthesiologists practice guidelines for management of the difficult airway: Anesthesiology, 2022; 136(1); 31-81
18. Sidhu VS, Whitehead EM, Ainsworth QP, A technique of awake fibreoptic intubation. Experience in patients with cervical spine disease: Anaesthesia, 1993; 48(10); 910-13
19. Rai MR, Parry TM, Dombrovskis A, Warner OJ, Remifentanil target-controlled infusion vs propofol target-controlled infusion for conscious sedation for awake fibreoptic intubation: A double-blinded randomized controlled trial: Br J Anaesth, 2008; 100(1); 125-30
20. Butler KH, Clyne B, Management of the difficult airway: Alternative airway techniques and adjuncts: Emerg Med Clin North Am, 2003; 21(2); 259-89
21. Saeg AAA, Alnori H, Laryngeal injury and dysphonia after endotracheal intubation: J Med Life, 2021; 14(3); 355-60
22. Hamard F, Ferrandiere M, Sauvagnac XPropofol sedation allows awake intubation of the difficult airway with the Fastrach LMA: Can J Anaesth, 2005; 52(4); 421-27 [in French]
23. Shyam R, Chaudhary AK, Sachan P, Evaluation of fastrach laryngeal mask airway as an alternative to fiberoptic bronchoscope to manage difficult airway: A comparative study: J Clin Diagn Res, 2017; 11(1); UC09-UC12
24. Chen Q, Qin B, Zhang M, The safety and efficacy of remimazolam compared to dexmedetomidine for awake tracheal intubation by flexible bronchoscopy: A randomized, double-blind, controlled trial: Drug Des Devel Ther, 2024; 18; 967-78
25. Li Q, Zeng F, Chen T, Anesthetic management of patients after scoliosis surgery: A single-center retrospective study: Orthop Surg, 2020; 12(6); 1753-59
26. Wang Y, Liu F, Zhang Y, The effect of capnography on the incidence of hypoxia during sedation for EGD and colonoscopy in mildly obese patients: A randomized, controlled study: BMC Anesthesiol, 2023; 23(1); 188
27. Mayr NP, Michel J, Bleiziffer S, Sedation or general anesthesia for transcatheter aortic valve implantation (TAVI): J Thorac Dis, 2015; 7(9); 1518-26
28. Sachan M, Singh NK, Naithani B, Comparative study of intubating conditions and hemodynamic changes during awake fiber-optic intubation using midazolam with fentanyl versus dexmedetomidine in cases of difficult airway: Natl J Maxillofac Surg, 2022; 13(2); 201-7
29. Verma AK, Verma S, Barik AK, Intubating conditions and hemodynamic changes during awake fiberoptic intubation using fentanyl with ketamine versus dexmedetomidine for anticipated difficult airway: A randomized clinical trial: Braz J Anesthesiol, 2021; 71(3); 259-64
Figures
Figure 1. Study flowchart. Rem – remimazolam; Dex – dexmedetomidine; AEI – awake endotracheal intubation; EtCO2 – end-tidal carbon dioxide.Figure 2. X-ray (A) and computed tomography (B, C) images of scoliosis in our study.Figure 3. Intubation-related parameters. (A) Success rate for the first attempt. (B) Overall success rate. (C) Comparison of attempt times. (D) Time of awake intubation procedure. Rem – remimazolam; Dex – dexmedetomidineFigure 4. Hemodynamic changes. (A) Decrease of mean arterial pressure (MAP) after administrating remimazolam or dexmedetomidine. (B) Increase of MAP when intubating. (C) Decrease of heart rate (HR) after administrating remimazolam or dexmedetomidine. (D) Increase of HR when intubating. Rem – remimazolam; Dex – dexmedetomidine. * P<0.05; ** P<0.001.Figure 5. Comparison of bispectral index (BIS) value. Rem – remimazolam; Dex – dexmedetomidine.Figure 6. Comparison of respiratory adverse events. (A) The number of patients with and without hypoxia. (B) The first end-tidal carbon dioxide (EtCO2) value after intubation. Rem – remimazolam; Dex – dexmedetomidine. In Press
Clinical Research
Body Weight and Insulin Resistance Indicators Among ChildrenMed Sci Monit In Press; DOI: 10.12659/MSM.951434
Clinical Research
Comparison of Radiographic Cervical Sagittal Alignment Parameters in Patients With Nonspecific Neck Pain, D...Med Sci Monit In Press; DOI: 10.12659/MSM.952950
Clinical Research
Combined Fibrinogen and Urinary α1-Microglobulin as Predictors of Respiratory Tract Infection in Children w...Med Sci Monit In Press; DOI: 10.12659/MSM.951066
Database Analysis
Evaluation of Salivary Total Oxidant Status (TOS) and Total Antioxidant Status (TAS) in Orthodontic Patient...Med Sci Monit In Press; DOI: 10.12659/MSM.952052
Most Viewed Current Articles
17 Jan 2024 : Review article 14,175,576
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,756,620
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,465,966
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,651
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387