29 March 2025: Clinical Research
The Role of the Vojta Method in Diagnosing and Enhancing Motor Skills in Preterm Infants: A Prospective Open-Label Controlled Study
Agata Trafalska DOI: 10.12659/MSM.945495
Med Sci Monit 2025; 31:e945495






Abstract
BACKGROUND: The Vojta method is utilized for the early detection of abnormal psychomotor development in newborns and infants, particularly those born prematurely. This study aimed to evaluate the effects of the Vojta method in enhancing spontaneous motor skills and reducing abnormal responses in prematurely born children.
MATERIAL AND METHODS: This prospective, open-label controlled study included 200 children divided into 3 groups: extremely premature (≤29 weeks, n=49), very premature (30-33 weeks, n=51), and late preterm (34-37 weeks, n=50) infants. A control group consisted of 50 full-term children undergoing rehabilitation for central nervous system coordination disorders. Diagnoses were conducted using the Vojta method within the first 6 months of life, followed by reexaminations at 3 and 6 months post-diagnosis to assess rehabilitation progress.
RESULTS: Initial examinations revealed significant differences among groups in several reflex tests, with a higher number of abnormal reactions in infants born before 34 weeks of gestation. Follow-up examinations demonstrated statistically significant improvements in all groups, with the most notable progress observed in children born after 34 weeks. Specifically, the Vojta reflex, traction test, Peiper-Isbert vertical suspension, and Collis’ suspension tests all showed significant enhancements post-rehabilitation.
CONCLUSIONS: The Vojta method is a valuable tool for early diagnosis and intervention to address developmental delays among preterm and full-term infants. Tailoring interventions to individual needs and integrating advanced technologies can optimize its application, enhancing motor function maturation and improving the quality of life for at-risk infants.
Keywords: Child Development, Developmental Disabilities, Infant Care, Motor Skills, Pediatrics, Premature Birth, Psychomotor Disorders, Rehabilitation, Humans, Infant, Premature, Prospective Studies, Female, Male, Infant, Newborn, Infant, Gestational Age, Motor Skills Disorders
Introduction
Prematurely born children are at a significantly higher risk of developmental delays and neuromotor impairments due to the immaturity of their central nervous systems at birth. Studies report that “up to 50% of very preterm infants exhibit signs of motor developmental disorders in early childhood,” which can significantly affect their health, functional independence, and quality of life [1]. These motor deficits often persist into later stages of development, increasing the likelihood of conditions such as “cerebral palsy, coordination disorders, and learning disabilities” [2]. Early detection and intervention are critical for mitigating these effects, as “neuroplasticity in infancy provides a unique opportunity to improve motor function and developmental outcomes” [3].
The Vojta method, developed by Dr. Václav Vojta in the 1950s and 1960s, is a neurophysiological approach used for the diagnosis and treatment of motor disorders in infants and children [4]. It is based on the concept of reflex locomotion, which posits that specific patterns of movement are inherent within the central nervous system (CNS) and can be activated through targeted external stimuli [5]. Neuromodulation plays a crucial role in this process, as the method’s targeted stimulation influences neuronal circuits within the CNS, promoting neuroplasticity and facilitating the reorganization of neural pathways [6,7]. This activation can lead to improvements in muscle tone regulation, postural control, and coordinated movements, even in the presence of neurological impairments [8].
Prematurely born children face numerous neurodevelopmental challenges stemming from both anamnestic risks, such as prenatal and perinatal factors, and symptomatic risks observed during neurodevelopmental evaluations. Anamnestic risks, including maternal health complications, prematurity, and perinatal trauma, provide early indicators of potential developmental delays. Symptomatic risks, such as abnormal motor responses or primitive reflexes detected during neurodevelopmental assessments, often manifest in infancy and signal the need for early intervention. For this purpose, we take a detailed patient history and look for risk factors that have appeared during pregnancy, birth, and after the child is born [9].
The assessment of patient history is integral to identifying risk factors that influence neurodevelopmental outcomes in premature infants [10]. These risk factors can be categorized into prenatal, perinatal, and postnatal factors. Prenatal factors include maternal chronic illnesses, genetic predispositions, and intrauterine infections, while perinatal factors such as prematurity, hypoxia, and delivery complications play a critical role in shaping neurodevelopment. Postnatal risks include seizures, hypotonia, and CNS anomalies like myelomeningocele. These factors, collectively referred to as anamnestic risks, are crucial in predicting developmental trajectories [11]. They can be related to the period of pregnancy and originate from the mother (chronic diseases of the mother, genetic burdens, intrauterine dystrophy, intrauterine infections, risk of preterm labor) or from the baby (various congenital defects, especially of the CNS, and genetic and metabolic diseases) [12].
Additionally, perinatal risk factors – including the mode of delivery, prematurity, hypoxia, and perinatal trauma – significantly influence an infant’s neurodevelopmental outcomes [13]. Conversely, postnatal factors are conditions that arise after birth and include seizures, significant hypotonia (extremely low muscle tone), suckling disorders, prolonged jaundice, infectious diseases, and congenital heart or CNS defects such as myelomeningocele. These factors are collectively referred to as anamnestic risk, which encompasses risks identified from the patient’s medical history. The terms ‘at-risk child’ and ‘risk factors’ were introduced into the literature by Illingworth and Ingram in the 1960s [14,15]. They mainly included the infants expected to develop cerebral palsy. A list of risk factors has been compiled by many authors [16].
Symptomatic risks, on the other hand, are already symptoms, disorders that we find during a thorough neurodevelopmental examination [17,18]. One of the internationally recognized diagnostic methods is the Vojta method, the concept of which also includes therapeutic principles. The complete diagnostic method according to the Vojta method: I – assessment of the child’s spontaneous motor skills in pronated and supinated positions; II – assessment of postural reactivity, ie reaction to a shift in the body in space; and III – examination of selected primitive reflexes [19].
Relevant to this concept is the notion of ontogeny, which is a species-specific program of spontaneous emergence and improvement of individual functions in a child who is healthy and achieves normal patterns and skills, according to calendar age [20]. We can monitor this by observing the milestones described above. When observing a child’s spontaneous motor skills, we assess global patterns, ie, overall movement patterns (global assessment while lying on the stomach and back) and partial patterns (assessment of individual body parts, eg head position, hand function). The next diagnostic step is to assess postural reactivity, or positioning responses. Seven positioning responses are used in diagnosis, which we can evaluate from the neonatal period [21].
Further prognosis of the child’s development is possible only after the end of the period in which we observe physiological primary reflexes; we must take into account the dynamics of their appearance and extinction. A diagnosis of central nervous coordination disorder is not the same as cerebral palsy or the risk of cerebral palsy, and can also predict minor postural abnormalities, which will improve in the course of maturation of the CNS [22,23].
Several studies have demonstrated the effectiveness of the Vojta method in improving motor abilities in children with neurological disorders, such as cerebral palsy [24–26]. These findings suggest that early intervention using the Vojta method can positively influence motor development outcomes. However, there is limited research focusing on the application of the Vojta method specifically in prematurely born children. Premature infants are at a higher risk of developmental delays and neuromotor impairments due to the immaturity of their neurological systems at birth [26,27]. While early physiotherapy interventions are recommended for this population, the efficacy of the Vojta method in improving psychomotor development in preterm infants remains underexplored. Most existing studies have small sample sizes, lack control groups, or do not compare outcomes across different gestational ages.
Therefore, our study aims to fill these gaps in the literature by evaluating the effectiveness of the Vojta method as both a diagnostic and therapeutic tool in prematurely born children across various gestational ages. By conducting a prospective open-label controlled study with a substantial sample size, we seek to provide robust evidence on the utility of the Vojta method in early detection and enhancement of psychomotor development in this vulnerable population.
Material and Methods
STUDY DESIGN AND PARTICIPANTS:
This prospective, open-label, controlled study was conducted at the Provincial Specialist Hospital and Day Rehabilitation Centers in Wrocław. The study included 200 children: 150 prematurely born infants and 50 full-term infants as a control group. The participants were divided into 3 preterm groups based on gestational age: (i) extremely premature (≤29 weeks, n=49), (ii) very premature (30–33 weeks, n=51), and (iii) late preterm (34–37 weeks, n=50). The control group comprised full-term infants undergoing rehabilitation for CNS coordination disorders.
QUALIFICATION CRITERIA:
Inclusion criteria included gestational age ≤37 weeks for preterm groups, full-term infants diagnosed with CNS coordination disorders for the control group, age ≤6 months at the time of the initial assessment, and parental consent to participate in the study. Exclusion criteria included congenital malformations incompatible with life, severe genetic or metabolic syndromes unrelated to prematurity, and lack of parental consent. These criteria ensured a well-defined cohort for consistent analysis. The control group was selected to match the preterm groups in terms of age and gender distribution, ensuring demographic comparability across groups.
STUDY TIMELINE:
The study followed a structured timeline to evaluate therapeutic progress at 3 key time points. The baseline examination was conducted when infants were 0–6 months old, serving as the initial assessment using the Vojta method. The second examination occurred 3 months after the baseline to evaluate intermediate progress, and the third examination was conducted 6 months post-baseline to assess final therapeutic outcomes. Each examination adhered to a standardized protocol established for Vojta diagnostics. This protocol included the evaluation of reflex responses, spontaneous motor patterns, and postural reactivity. To ensure consistency and reliability, all assessments were performed by the same trained researcher using uniform methodologies.
ETHICAL CONSIDERATIONS:
The study protocol was approved by the local Bioethics Committee at the Wrocław Medical University (approval no. KB-677/2017). The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. Informed consent was obtained from parents or legal guardians of all participants, ensuring they were fully informed about the study’s objectives, procedures, risks, and benefits. Participants were free to withdraw at any time without consequences. Confidentiality and anonymity were strictly maintained. Data were anonymized and securely stored, accessible only to the research team. Results were reported in aggregate to prevent individual identification. The Vojta method was administered by trained professionals, ensuring minimal risk and discomfort to the children. The study adhered to ethical guidelines and regulatory requirements to ensure the integrity and ethical conduct of the research.
DIAGNOSIS AND INTERVENTION:
Children were included in the study during their first 6 months of life. Diagnosis was performed using the Vojta method, which assesses spontaneous motor skills, postural reactivity, and primitive reflexes to identify motor abnormalities. Based on the results of the initial examination (baseline), individualized rehabilitation needs and interdisciplinary therapy goals were established. Following the baseline assessment, rehabilitation began, and progress was monitored through follow-up examinations conducted approximately 3 months (second examination) and 6 months (third examination) after the baseline. During these assessments, the same diagnostic scheme was consistently applied to ensure reliable evaluation of therapeutic outcomes.
The Vojta method requires careful analysis of postural reactivity and motor skill alignment with the child’s corrected calendar age. If a match is observed, the child is deemed to follow normal developmental trajectories. However, deviations in postural reactions are identified by the number of disturbed partial patterns, starting from an analysis of global movement patterns. Even a single disturbed partial pattern qualifies the reaction as abnormal. A higher number of abnormalities indicates an increased likelihood of developmental disorders and further postural impairments. Rehabilitation progress was evaluated by analyzing changes in reflex responses and postural reactivity over the 6-month observation period. The Vojta method was applied exclusively by trained professionals certified in its use, following a standardized protocol. This protocol clearly defines which reactions are considered abnormal, ensuring precise and reproducible assessments. Therapeutic outcomes and differences in rehabilitation effectiveness were systematically analyzed across the study groups.
STATISTICAL ANALYSIS:
Statistical analysis was performed using Statistica 13.3 (TIBCO Software Inc.). The analysis aimed to evaluate the effectiveness of the Vojta method in diagnosing and improving psychomotor development in prematurely born children. Data from 200 children, divided into 4 groups based on gestational age, were collected. These included extremely premature (≤29 weeks), very premature (30–33 weeks), late preterm (34–37 weeks), and full-term (control) infants. Descriptive statistics, including mean, median, and standard deviation, were calculated to summarize the initial assessment scores and demographic characteristics of each group. Pearson’s chi-square test was used to compare the number of abnormal responses among the groups at each examination point (initial, 3 months, and 6 months). After conducting overall chi-square tests to compare the groups, post-hoc pairwise chi-square tests were performed to identify specific group differences. The Bonferroni correction was applied to adjust for multiple comparisons, resulting in an adjusted significance level of
Results
The baseline (initial) examination revealed significant differences among the gestational age groups in several reflex tests. Vojta reflex results showed that abnormal responses were most frequent in late preterm infants (66%) compared with extremely premature infants (40.8%) and very premature infants (54.9%). Axillary suspension tests exhibited fewer abnormalities in late preterm infants (34%) compared with extremely premature (59.2%) and very premature (54.9%) infants. Similar trends were observed across tests, including the Collis’ vertical suspension and Peiper-Isbert vertical suspension, where extremely premature infants demonstrated the highest percentage of abnormal responses (91.8% and 100%, respectively). These findings are summarized in Table 1.
In the second examination, statistically significant differences were found among the groups in all the analyzed reactions according to the Vojta method. Compared with Group 2 (very premature infants), Group 1 (extremely premature infants) performed worse in the axillary suspension reflex but better in the Vojta reflex. For other tests, there were minimal differences between these 2 groups.
Minimal differences were observed between Group 3 (late preterm infants) and the control group (Group 4) in most reactions during the second examination. However, in the axillary suspension reflex, more abnormalities were observed in Group 3 (44%) than in Group 4 (26%). This is likely related to a higher frequency of positional asymmetry in Group 3 (70%) compared with Group 4 (56%). Similar patterns were noted in the axillary suspension reflex across Groups 2 and 3. In the Vojta reflex, Groups 1 and 2 performed better than Groups 3 and 4. However, in all other responses, Groups 3 and 4 outperformed Groups 1 and 2. The results of these findings are summarized in Table 2.
In the third examination, the percentage of abnormalities between Group 3 and Group 4 showed minimal differences, except in the axillary suspension reflex. Here, Group 3 demonstrated a 44% abnormal response rate compared with 26% in Group 4. This finding aligns with the presence of positional asymmetry, the most common motor problem observed in Group 3 during the third examination. Notably, differences in abnormalities in the Vojta reflex were also observed. Group 1 had an abnormal response rate of 46.9%, Group 2 had 60.8%, Group 3 had 32%, and Group 4 had 36%. The data suggest that the Vojta reflex results may have a weaker correlation with global motor patterns. Table 3 presents these results.
A comprehensive analysis of Vojta reflex results across all examinations revealed statistically significant improvement (
In the traction test, statistically significant improvement (
For the Peiper-Isbert vertical suspension test, statistically significant improvement (
Statistically significant improvement (
Similar trends were noted in the Collis’ horizontal suspension test, where all groups demonstrated statistically significant improvement (
For the Landau reflex, statistically significant improvement (
In the axillary suspension reflex, statistically significant improvements (
Among infants born before 30 weeks of pregnancy, rehabilitation resulted in statistically significant improvements in several reflex tests, including the traction test (
Discussion
COMPARISON WITH PREVIOUS RESEARCH:
Previous studies have consistently corroborated the effectiveness of the Vojta method for early diagnosis and therapy in infants with motor disorders [5,28–30]. A systematic review and meta-analysis by Sánchez-González et al [28] highlighted the neurophysiological underpinnings of Vojta therapy, particularly its impact on cortical and muscle activity. While significant improvements were reported in balance and motor control in adults with neurological disorders, the analysis of pediatric populations revealed non-significant differences in gross motor function outcomes. This suggests that Vojta therapy may be most effective when integrated with complementary therapeutic approaches to enhance its rehabilitative impact. These findings align with our observation that late preterm and control groups benefited more significantly than extremely preterm groups, indicating the need for tailored strategies based on gestational age.
The significant improvements observed in this study, particularly in children born after 34 weeks of gestation, are consistent with findings from Stephens and Vohr [31], who reported better neurodevelopmental outcomes in late preterm infants than in extremely premature infants. These results reinforce the importance of considering gestational age as a key factor in designing rehabilitation programs.
DIAGNOSTIC ACCURACY AND NEUROMOTOR DEVELOPMENT:
Our analysis highlights the diagnostic utility of the Vojta method, particularly its comprehensive evaluation of reflex responses and spontaneous motor skills. This method provides a robust framework for identifying developmental delays early, as supported by Vojta and Peters [32]. Across the 3 examinations in this study, significant improvements were observed in all 7 reflex responses, with a progressive decrease in abnormal reactions. This underscores the importance of early intervention using the Vojta method to promote neuromotor development and reduce the risk of long-term motor deficits.
The reduction in psychomotor abnormalities across all groups indicates that the Vojta method facilitates maturation of motor patterns. In particular, the correlation between reduced abnormal positioning responses and improvements in psychomotor development highlights the method’s effectiveness in addressing underlying neuromotor dysfunctions. These findings are consistent with earlier studies demonstrating the Vojta method’s ability to enhance neuromuscular coordination and motor control [5,30].
LIMITATIONS AND METHODOLOGICAL REFINEMENTS:
One of the challenges in applying the Vojta method is its reliance on subjective assessments, which can vary based on the examiner’s expertise. This subjectivity could introduce variability into results, particularly in evaluations of spontaneous motor skills and reflex responses. To address this limitation, integrating objective assessment tools, such as wearable sensors and motion analysis systems, could enhance diagnostic accuracy. Recent studies have demonstrated the efficacy of these technologies in quantifying motor functions objectively, providing precise feedback on movement patterns and reducing examiner bias [33,34].
For example, wearable accelerometers have been successfully used to monitor motor behavior in infants with neurological impairments, offering valuable insights into movement quality and activity levels. Similarly, RGB-depth cameras and 2D video analysis have proven effective in tracking motor development, enabling clinicians to assess progress with greater consistency. Combining such technologies with the Vojta method could significantly improve the reliability of motor evaluations and provide a more comprehensive understanding of therapeutic outcomes.
PRACTICAL CHALLENGES AND RECOMMENDATIONS:
The adoption of the Vojta method in clinical practice often faces challenges related to parental apprehensions and therapist proficiency. Parents may express concerns about the therapy causing discomfort to their child, while therapists may feel uncertain about their ability to administer the method effectively due to its complexity. A study by Jung et al [29] found that providing thorough explanations of the therapy’s benefits and involving parents in the rehabilitation process significantly improved acceptance. Similarly, offering specialized training and ongoing support for therapists can enhance their confidence and competence, as noted by Sánchez-González et al [28].
Addressing these practical challenges through education and open communication is essential for the successful implementation of the Vojta method. For instance, structured training programs for therapists and informational sessions for parents could bridge gaps in understanding and foster greater trust in the method. Additionally, incorporating advanced technologies into the therapy process could alleviate some of these concerns by providing objective, real-time feedback on motor improvements.
FUTURE RESEARCH DIRECTIONS:
This study underscores the potential of the Vojta method in pediatric rehabilitation but also highlights areas for further exploration. Future research should focus on: (1) investigating the long-term outcomes of Vojta therapy to assess the sustainability of motor improvements; (2) exploring the integration of complementary therapies to enhance its efficacy, particularly in extremely preterm populations; (3) standardizing methodologies and incorporating objective assessment tools to minimize variability and improve diagnostic accuracy; and (4) examining the role of perinatal and environmental factors in shaping motor outcomes to better individualize therapy.
Conclusions
The Vojta method remains a valuable tool in early diagnosis and intervention for developmental delays in preterm and full-term infants. While its effectiveness is evident across gestational age groups, the findings of this study emphasize the importance of tailoring interventions to individual developmental needs. By integrating advanced technologies and addressing practical challenges, the Vojta method can be further optimized to enhance motor function maturation and improve quality of life for at-risk infants.
Figures
 Figure 1. Percentage of abnormal reflexes according to Vojta in 4 age groups during 3 examinations. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months).
Figure 1. Percentage of abnormal reflexes according to Vojta in 4 age groups during 3 examinations. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months).  Figure 2. Percentage of responses in the traction test in the 4 age groups during the 3 examinations. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months).
Figure 2. Percentage of responses in the traction test in the 4 age groups during the 3 examinations. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months).  Figure 3. Percentage of responses in the Peiper-Isbert vertical suspension reflex test in the 4 age groups during the 3 examinations. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months).
Figure 3. Percentage of responses in the Peiper-Isbert vertical suspension reflex test in the 4 age groups during the 3 examinations. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months).  Figure 4. Percentage of responses in the Collis’ vertical suspension reflex test in the 4 age groups during the 3 examinations. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months).
Figure 4. Percentage of responses in the Collis’ vertical suspension reflex test in the 4 age groups during the 3 examinations. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months). 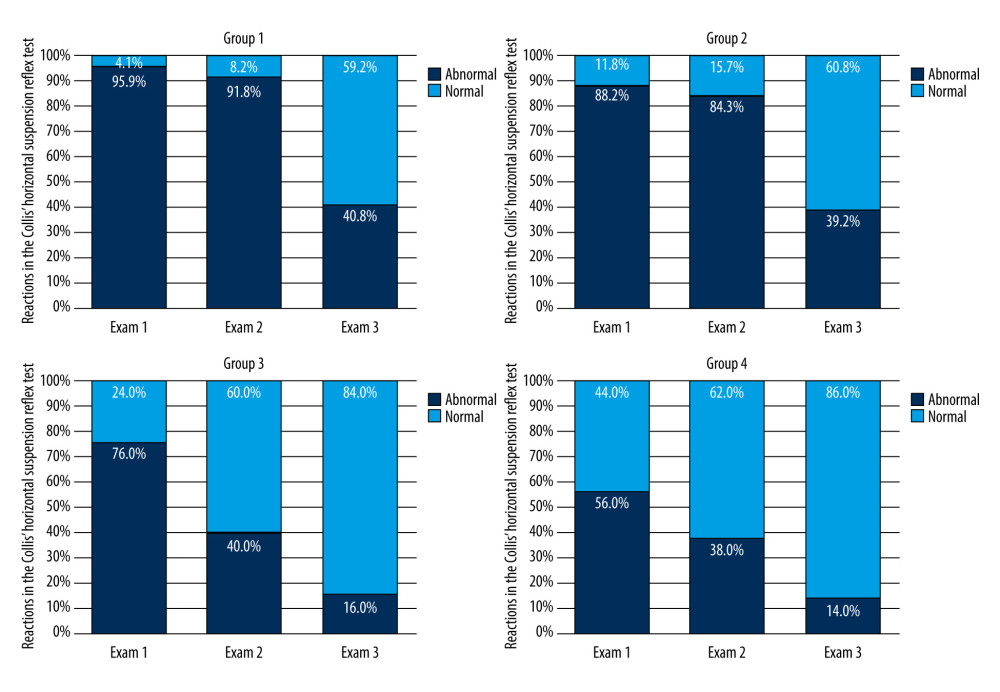 Figure 5. Percentage of responses in the Collis’ horizontal suspension reflex test in the 4 age groups during the 3 examinations. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months).
Figure 5. Percentage of responses in the Collis’ horizontal suspension reflex test in the 4 age groups during the 3 examinations. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months).  Figure 6. Percentage of Landau reflexes in 4 age groups during the 3 examinations. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months).
Figure 6. Percentage of Landau reflexes in 4 age groups during the 3 examinations. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months).  Figure 7. Percentage of axillary suspension reactions in 4 age groups during 3 examinations. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months).
Figure 7. Percentage of axillary suspension reactions in 4 age groups during 3 examinations. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months).  Figure 8. The number of abnormal responses in the Vojta test in groups of children in the respective examinations and the results of Kruskal-Wallis significance tests and multiple comparisons (post-hoc) with Dunn’s test. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months).
Figure 8. The number of abnormal responses in the Vojta test in groups of children in the respective examinations and the results of Kruskal-Wallis significance tests and multiple comparisons (post-hoc) with Dunn’s test. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months). Tables
Table 1. Evaluation of positioning responses by the Vojta method on the day of the initial examination (baseline) in groups of preterm infants differing in gestational age, and results of comparisons. Table 2. Evaluation of positioning responses by the Vojta method on the day of the second examination (after 3 months) in groups of preterm infants differing in gestational age, with results of comparisons.
Table 2. Evaluation of positioning responses by the Vojta method on the day of the second examination (after 3 months) in groups of preterm infants differing in gestational age, with results of comparisons. Table 3. Evaluation of positioning responses by the Vojta method on the day of the third examination (after 6 months) in groups of preterm infants differing in gestational age and results of comparisons.
Table 3. Evaluation of positioning responses by the Vojta method on the day of the third examination (after 6 months) in groups of preterm infants differing in gestational age and results of comparisons. Table 4. Number (percentage) of reflexes according to Vojta in groups of children differing in gestational age (Group) and examination time point, and results of Pearson’s chi-square independence test.
Table 4. Number (percentage) of reflexes according to Vojta in groups of children differing in gestational age (Group) and examination time point, and results of Pearson’s chi-square independence test. Table 5. Number (percentage) of reflexes in the traction test in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.
Table 5. Number (percentage) of reflexes in the traction test in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test. Table 6. Number (percentage) of reflexes in the Peiper-Isbert vertical suspension reflex test in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.
Table 6. Number (percentage) of reflexes in the Peiper-Isbert vertical suspension reflex test in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test. Table 7. Number (percentage) of reflexes in the Collis’ vertical suspension reflex test in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.
Table 7. Number (percentage) of reflexes in the Collis’ vertical suspension reflex test in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test. Table 8. Number (percentage) of reflexes in the Collis’ horizontal suspension reflex test in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.
Table 8. Number (percentage) of reflexes in the Collis’ horizontal suspension reflex test in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.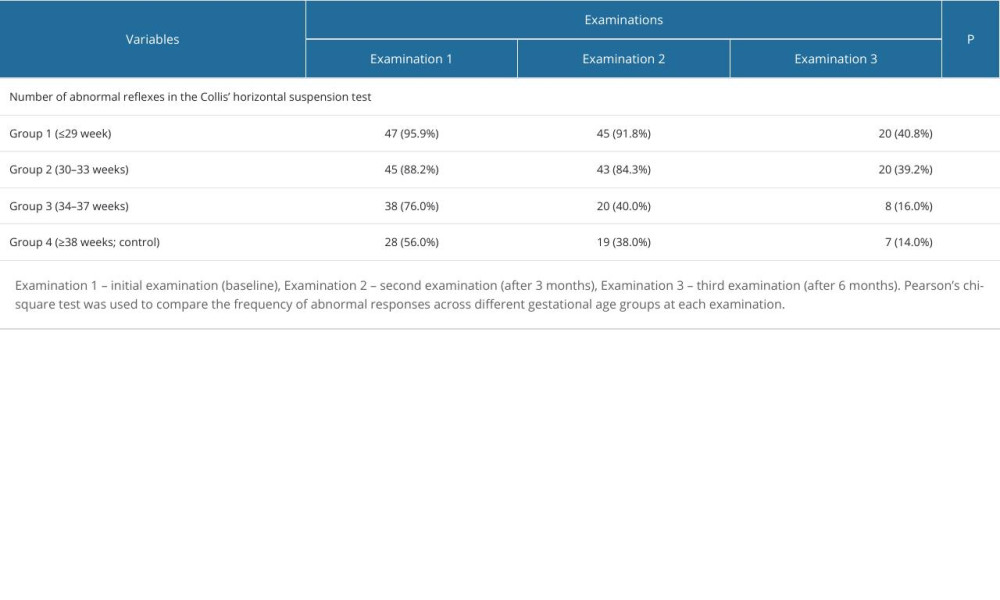 Table 9. Number (percentage) of Landau reflexes in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.
Table 9. Number (percentage) of Landau reflexes in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test. Table 10. Number (percentage) of axillary suspension reactions in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.
Table 10. Number (percentage) of axillary suspension reactions in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test. Table 11. Number of abnormal reactions in children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.
Table 11. Number of abnormal reactions in children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.
References
1. Prasad Gupta M, Gupta D, Usman A, Post-term birth and developmental coordination disorder: A narrative review of motor impairments in children: Cureus, 2024; 16; e63211
2. Moster D, Lie RT, Markestad T, Long-term medical and social consequences of preterm birth: N Engl J Med, 2008; 359; 262-73
3. Saigal S, Doyle LW, An overview of mortality and sequelae of preterm birth from infancy to adulthood: Lancet Lond Engl, 2008; 371; 261-69
4. Vojta VReflex rotation as a pathway to human locomotion: Z Orthop Ihre Grenzgeb, 1970; 108; 446-52 [in German]
5. Banaszek GVojta’s method as the early neurodevelopmental diagnosis and therapy koncept: Przegl Lek, 2010; 67; 67-76 [in Polish]
6. Kumar J, Patel T, Sugandh F, Innovative approaches and therapies to enhance neuroplasticity and promote recovery in patients with neurological disorders: A narrative review: Cureus, 2023; 15(7); e41914
7. Aderinto N, AbdulBasit MO, Olatunji G, Adejumo T, Exploring the transformative influence of neuroplasticity on stroke rehabilitation: A narrative review of current evidence: Ann Med Surg, 2023; 85; 4425-32
8. Evancho A, Tyler WJ, McGregor K, A review of combined neuromodulation and physical therapy interventions for enhanced neurorehabilitation: Front Hum Neurosci, 2023; 17; 1151218
9. Backes EP, Scrimshaw SCNational Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Division of Behavioral and Social Sciences and Education; Board on Children, Youth, and Families; Committee on Assessing Health Outcomes by Birth Settings: Birth Settings in America: Outcomes, Quality, Access, and Choice Feb 6, 2020; 3, Washington (DC), National Academies Press (US) Epidemiology of clinical risks in pregnancy and childbirth. Available from:https://www.ncbi.nlm.nih.gov/books/NBK555485/
10. Hyun SE, Kwon JY, Hong BY, Early neurodevelopmental assessments of neonates discharged from the Neonatal Intensive Care Unit: A physiatrist’s perspective: Ann Rehabil Med, 2023; 47(3); 147-61
11. Song IG, Neurodevelopmental outcomes of preterm infants: Clin Exp Pediatr, 2022; 66; 281-87
12. Menéndez-Pardiñas M, Alonso-Bidegaín M, Santonja-Medina F, Effects of Vojta therapy on the motor function of children with neuromotor disorders: Study protocol for a randomized controlled trial: J Clin Med, 2023; 12; 7373
13. Luca A, Vinturache A, Ilea C, Birth trauma in preterm spontaneous vaginal and cesarean section deliveries: A 10-years retrospective study: PLoS One, 2022; 17; e0275726
14. Illingworth RS, The child at risk of deafness: Clin Pediatr (Phila), 1964; 3; 510-11
15. Ingram TTS, The new approach to early diagnosis of handicaps in childhood: Dev Med Child Neurol, 1969; 11; 279-90
16. Sullivan MC, Msall ME, Functional performance of preterm children at age 4: J Pediatr Nurs, 2007; 22; 297-309
17. Cainelli E, Bisiacchi P, Neurodevelopmental disorders: Past, present, and future: Children, 2022; 10; 31
18. Carlsson T, Molander F, Taylor MJ, Early environmental risk factors for neurodevelopmental disorders – a systematic review of twin and sibling studies: Dev Psychopathol, 2021; 33(4); 1448-95
19. Andrzejewska M, Hap K, Biernat K, Factors affecting rehabilitation of infants with Central Coordination Disorders during a three-month-long observation: BMC Pediatr, 2021; 21; 579
20. Tomasello M, Gonzalez-Cabrera I, The role of ontogeny in the evolution of human cooperation: Hum Nat Hawthorne N, 2017; 28; 274-88
21. Costi GC, Radice C, Raggi AVojta’s seven postural reactions in the detection of neuromotor disorders in infants. Experience with 2382 subjects: Pediatr Medica E Chir Med Surg Pediatr, 1983; 5; 59-65 [In Italian]
22. Harris SR, Mickelson ECR, Zwicker JG, Diagnosis and management of developmental coordination disorder: Can Med Assoc J, 2015; 187; 659-65
23. Ip A, Mickelson ECR, Zwicker JG, Assessment, diagnosis, and management of developmental coordination disorder: Paediatr Child Health, 2021; 26; 375-78
24. Khanna S, Arunmozhi R, Goyal C, Neurodevelopmental treatment in children with cerebral palsy: A review of the literature: Cureus, 2023; 15(12); e50389
25. Ha S-Y, Sung Y-H, Stimulus zones of Vojta method and trunk control in children with spastic-type cerebral palsy: A quasi-experimental pilot study: J Bodyw Mov Ther, 2024; 38; 150-54
26. Spittle AJ, Orton J, Cerebral palsy and developmental coordination disorder in children born preterm: Semin Fetal Neonatal Med, 2014; 19; 84-89
27. de Kieviet JF, Piek JP, Aarnoudse-Moens CS, Oosterlaan J, Motor development in very preterm and very low-birth-weight children from birth to adolescence: A meta-analysis: JAMA, 2009; 302; 2235-42
28. Sánchez-González JL, Sanz-Esteban I, Menéndez-Pardiñas M, Critical review of the evidence for Vojta therapy: A systematic review and meta-analysis: Front Neurol, 2024; 15; 1391448
29. Jung MW, Landenberger M, Jung T, Vojta therapy and neurodevelopmental treatment in children with infantile postural asymmetry: A randomised controlled trial: J Phys Ther Sci, 2017; 29; 301-6
30. Parau D, Todoran AB, Barcutean L, The benefits of combining Bobath and Vojta therapies in infants with motor development impairment – a pilot study: Medicina (Mex), 2023; 59; 1883
31. Stephens BE, Vohr BR, Neurodevelopmental outcome of the premature infant: Pediatr Clin North Am, 2009; 56; 631-46
32. Vojta V, Peters A: The Vojta principle, 2007, Berlin, Germany, Springer International Publishing
33. Taylor E, Airaksinen M, Gallen A, Quantified assessment of infant’s gross motor abilities using a multisensor wearable: J Vis Exp, 2024; 207; 65949
34. Vaaras E, Airaksinen M, Vanhatalo S, Rasanen O, Evaluation of self-supervised pre-training for automatic infant movement classification using wearable movement sensors; 2023; 1-6
Figures
Figure 1. Percentage of abnormal reflexes according to Vojta in 4 age groups during 3 examinations. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months).Figure 2. Percentage of responses in the traction test in the 4 age groups during the 3 examinations. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months).Figure 3. Percentage of responses in the Peiper-Isbert vertical suspension reflex test in the 4 age groups during the 3 examinations. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months).Figure 4. Percentage of responses in the Collis’ vertical suspension reflex test in the 4 age groups during the 3 examinations. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months).Figure 5. Percentage of responses in the Collis’ horizontal suspension reflex test in the 4 age groups during the 3 examinations. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months).Figure 6. Percentage of Landau reflexes in 4 age groups during the 3 examinations. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months).Figure 7. Percentage of axillary suspension reactions in 4 age groups during 3 examinations. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months).Figure 8. The number of abnormal responses in the Vojta test in groups of children in the respective examinations and the results of Kruskal-Wallis significance tests and multiple comparisons (post-hoc) with Dunn’s test. Exam 1 – initial examination (baseline), Exam 2 – second examination (after 3 months), Exam 3 – third examination (after 6 months). Tables
Table 1. Evaluation of positioning responses by the Vojta method on the day of the initial examination (baseline) in groups of preterm infants differing in gestational age, and results of comparisons.Table 2. Evaluation of positioning responses by the Vojta method on the day of the second examination (after 3 months) in groups of preterm infants differing in gestational age, with results of comparisons.Table 3. Evaluation of positioning responses by the Vojta method on the day of the third examination (after 6 months) in groups of preterm infants differing in gestational age and results of comparisons.Table 4. Number (percentage) of reflexes according to Vojta in groups of children differing in gestational age (Group) and examination time point, and results of Pearson’s chi-square independence test.Table 5. Number (percentage) of reflexes in the traction test in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.Table 6. Number (percentage) of reflexes in the Peiper-Isbert vertical suspension reflex test in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.Table 7. Number (percentage) of reflexes in the Collis’ vertical suspension reflex test in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.Table 8. Number (percentage) of reflexes in the Collis’ horizontal suspension reflex test in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.Table 9. Number (percentage) of Landau reflexes in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.Table 10. Number (percentage) of axillary suspension reactions in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.Table 11. Number of abnormal reactions in children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.Table 1. Evaluation of positioning responses by the Vojta method on the day of the initial examination (baseline) in groups of preterm infants differing in gestational age, and results of comparisons.Table 2. Evaluation of positioning responses by the Vojta method on the day of the second examination (after 3 months) in groups of preterm infants differing in gestational age, with results of comparisons.Table 3. Evaluation of positioning responses by the Vojta method on the day of the third examination (after 6 months) in groups of preterm infants differing in gestational age and results of comparisons.Table 4. Number (percentage) of reflexes according to Vojta in groups of children differing in gestational age (Group) and examination time point, and results of Pearson’s chi-square independence test.Table 5. Number (percentage) of reflexes in the traction test in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.Table 6. Number (percentage) of reflexes in the Peiper-Isbert vertical suspension reflex test in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.Table 7. Number (percentage) of reflexes in the Collis’ vertical suspension reflex test in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.Table 8. Number (percentage) of reflexes in the Collis’ horizontal suspension reflex test in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.Table 9. Number (percentage) of Landau reflexes in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.Table 10. Number (percentage) of axillary suspension reactions in groups of children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test.Table 11. Number of abnormal reactions in children differing in gestational age (Group) and examination time point and results of Pearson’s chi-square independence test. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387