18 March 2025: Clinical Research
Impact of Nurse-Led Versus Surgeon-Led Preoperative Counseling and Follow-Up on Postoperative Outcomes in Pediatric Tonsillectomy: A Longitudinal Observational Study
Mengting Fan DOI: 10.12659/MSM.945597
Med Sci Monit 2025; 31:e945597






Abstract
BACKGROUND: Pre-tonsillectomy complex challenges in explaining surgeries requirements and preparing children for curative surgeries. In addition, post-tonsillectomy pain and complications are reported in children with tonsillitis. The objective of the study was to compare the intensities of postoperative pain and frequencies of postoperative complications among children undergoing elective tonsillectomy who received different types of counseling and follow-up care.
MATERIAL AND METHODS: Children received pre-tonsillectomy nurse-led counseling and post-tonsillectomy nurse-led follow-up care for 6 months (NCC cohort, n=29), pre-tonsillectomy surgeon-led counseling and post-tonsillectomy surgeon-led follow-up care for 6 moths (FSS cohort, n=35), or did not receive counseling and received everyday surgeons’ visits during hospital stays only (UUS cohort, n=38).
RESULTS: Post-tonsillectomy pain was 4 (IQ range, 5-4) per child at discharge from the hospital. The children reported mild pain during the 1-month follow-up. Children in the NCC cohort had fever, post-tonsillectomy pain at discharge and 1 months after surgeries, needed less tramadol, had fewer hospital stays, had fewer immediate and late post-tonsillectomy complications (especially anxiety and vomiting), and had higher personal satisfaction and higher clinical benefits than children in the FSS and UUS cohorts (P<0.05). Nausea was reported in all children. A total of 56 (55%) children had a decrease in oral intake during the follow-up period.
CONCLUSIONS: Children may experience more post-tonsillectomy pain than expected at discharge and during follow-up. After tonsillectomy, children had a decrease in oral intake. Nurse-led counseling and follow-up care have favorable post-tonsillectomy outcomes and high personal satisfaction of children undergoing curative tonsillectomies.
Keywords: Aftercare, Counseling, Nurses, Pediatric, Pain, Postoperative, Postoperative Care, Tonsillectomy, Humans, Female, Child, Male, Longitudinal Studies, Child, Preschool, Postoperative Complications, Surgeons, Treatment Outcome, Preoperative Care, Follow-Up Studies, Nurses
Introduction
Tonsillectomy is a minor and common surgical procedure in children [1]. Caregivers experience complex preoperative challenges in explaining and preparing children for tonsillectomy [2]. Parents face problems while providing preoperative care for children undergoing tonsillectomy [3]. Tonsillectomy causes postoperative pain as well as early and late postoperative complications [4]. Because of high postoperative pain, children have problems with behavior, oral intake, and sleep after tonsillectomy [5]. The quality of life of children after tonsillectomy is often unsatisfactory [6]. These confounding effects increase the risk of secondary hemorrhage, inadequate rest periods, and suboptimal pain management after tonsillectomy in children [7]. Most parents have inadequate knowledge of how to manage their children’s post-tonsillectomy pain and complications [1] and pre-tonsillectomies counseling of children regarding postoperative pain and complications [3].
Because of parents’ inadequate knowledge, they provide improper medication for post-tonsillectomy pain and complications or they would misguide in the follow-up period [8]. Many interventions and techniques are adopted by parents after tonsillectomy for pain and complication management, but these are not sufficient [1]. Postoperative outcomes are influenced by pain management interventions and the context in which these are provided [9]. Nurse-led telephonic aftercare has been reported to be beneficial for partial postoperative pain management and complications among children aged 4–12 years who underwent tonsillectomy in Canada [1]. However, nurse-led telephonic aftercare has been reported to be partially effective for postoperative pain management and complications among children undergoing tonsillectomy in western Hubei Province, China [10]. In addition, preoperative nursing counseling could be useful in identifying and defining risk factors for elective surgery patients and preoperative care policies [11]. Nurses have an important role in the early postoperative phase and post-discharge follow-up because they have the most contact with patients throughout the perioperative pathways [12]. There is the lack of consensus on the most effective strategies for preoperative counseling and postoperative follow-up care for children undergoing tonsillectomy. Therefore, there is need for pre-tonsillectomy counseling on children’s well-being and post-tonsillectomies care and to address caregivers’ challenges for better pain management and prevention of complications in children with tonsillitis.
The objectives of the current retrospective study of electronic medical records were to compare the intensities of postoperative pain and frequencies of postoperative complications among children undergoing elective tonsillectomy who receive different types of counseling and follow-up care (nurse-led pre-tonsillectomy counseling and nurse-led post-tonsillectomy follow-up, or surgeon-led pre-tonsillectomy counseling, and surgeon-led post-tonsillectomy follow-up care, or children and their parents who did not receive pre-tonsillectomy counseling and received only post-tonsillectomy surgeon visits during hospital stays) in western Jiangsu Province, China.
Material and Methods
ETHICS APPROVAL AND CONSENT TO PARTICIPATE:
The designed protocols were prepared by the authors themselves and approved by the Human Ethics Committee of the First Affiliated Hospital of Soochow University ((2024) Lunyan Approval No. 755ehT, September 14, 2020). The study followed the laws of China and the v2008 Helinski Declaration. The requirement for informed consent was waived by the Human Ethics Committee of the First Affiliated Hospital of Soochow University because of the retrospective nature of the study.
INCLUSION CRITERIA:
We included children aged 4–12 years undergoing elective tonsillectomy for tonsillitis with an American Society of Anesthesiologists (ASA) physical status of 1 (a normal healthy patient) or 2 (a patient with mild systemic disease).
EXCLUSION CRITERIA:
We excluded children with neurocognitive deficits (cognitive impairment, especially in complex attention) and/or chronic pain (persistent ongoing and recurrent episodic pain), as well as children with recurrent tonsillitis, as these can affect the post-tonsillectomy clinical course.
SAMPLE SIZE CALCULATION:
We used OpenEpi software (version 3.0, Epidemiologic Statistics for Public Health, Version. www.OpenEpi.com). We assumed that professional-led counseling and professional-led follow-up care would decrease intensities of postoperative pain by 15% and result in a 10% reduction in postoperative complications (hypothesized% frequency of outcome factor in the population) of children undergoing elective tonsillectomy compared to children and their parents who did not receive preoperative professional-led counseling and received only postoperative surgeons’ visits during hospital stays (effect size). In addition, α was 0.05, β was 0.1, at a 95% confidence interval (CI), and a standard deviation (SD) of 5%. The required sample size (minimum children required in the cohort) was calculated to be 27 [1,13].
COHORTS:
In the NCC cohort, a total of 29 children undergoing elective tonsillectomy received preoperative nurse-led counseling and nurse-led postoperative follow-up care for 6 months (a nurse visit every month at the institute, a surgeon visit every day until discharge, and a postoperative surgeon visit when required for complications). In the FSS cohort, a total of 35 children undergoing elective tonsillectomy received preoperative surgeon-led counseling and postoperative surgeon-led follow-up care for 6 months (a surgeon visit every month at the institute, a surgeon visit every day until discharge, and a postoperative surgeon visit when required for complications). In the UUS cohort (usual care), 38 children undergoing elective tonsillectomy did not receive professional-led preoperative healthcare counseling and received only daily postoperative surgeon visits during hospital stays and postoperative surgeon-led follow-up visits when required. The selection of professionals for counseling and follow-up care was based on the availability of professionals in the institute. Children and their parents who did not receive preoperative healthcare professional-led counseling were included in the UUS cohort. In addition to professional-led counseling and professional-led follow-up care, children also received treatment directed by surgeons during the study period.
NURSE-LED PREOPERATIVE COUNSELING AND NURSE-LED POSTOPERATIVE FOLLOW-UP CARE: One day before the operation in the ward or operating room, nurses educated the children and their parents (including caregivers) regarding surgeries, their necessities, and postoperative complications, including average hospital stays with or without the help of verbal or visual aids. After the operation in the postoperative anesthesia care unit and ward, nurses provided verbal education regarding average hospital stays, postoperative complications including pain and swallowing disorders, and measures to overcome postoperative complications [13,14].
SURGEON-LED PREOPERATIVE COUNSELING AND SURGEON-LED POSTOPERATIVE FOLLOW-UP CARE: One day before the operation in the ward or operating room, surgeons educated children and their parents (including caregivers) regarding surgeries, their necessities, postoperative complications including average hospital stays, and surgical charges with or without the help of verbal or visual aids. After the operation in the postoperative anesthesia care unit and ward, surgeons provided verbal education regarding average hospital stays, postoperative complications including pain and swallowing disorders, and treatments to overcome postoperative complications (during patients’ visits to surgeons in the hospital) [13].
USUAL CARE:
In usual care for children undergoing elective tonsillectomy, children and their parents did not receive preoperative healthcare professional-led counseling at the hospital and received only daily postoperative surgeon visits during hospital stays and surgeon-led postoperative follow-up visits when required (for postoperative complications such as swallowing disorders and bleeding.
POSTOPERATIVE PAIN INTENSITY: When children regained consciousness after anesthetization, postoperative pain was evaluated by nurses using the Faces Pain Scale-Revised, with scores from 0 to 10. A score of 0 indicates no pain, and 10 indicates the maximum possible pain. Children were asked to choose a face that corresponded to their pain, and each face was associated with a number [15]. Postoperative pain was evaluated after tonsillectomies, at discharge, and -month after surgery. Pain scores of 3 or less were considered mild [1].
POSTOPERATIVE ANALGESIC DOSAGE:
For postoperative pain, children received 25 mg of mouth-dissolving tramadol tablets (available brands in the Chinese market) twice a day during hospital stays. In follow-up, children received 25 mg of mouth-dissolving tramadol tablet when they indicated they were feeling pain. During the hospital stay after surgery and at 6-month follow-up, the total consumption of tramadol (mg) was calculated for each patient.
HOSPITAL STAYS:
Length of hospital stay was the time from admission to the hospital to discharge.
FREQUENCIES OF POSTOPERATIVE COMPLICATIONS:
Data on immediate (during hospital stays) and late (after discharge of patients at 6-month follow-up) postoperative complications in children were collected and analyzed.
During hospital stays, data were collected by nurses, and at the end of 6-month follow-up data were collected by caregivers with or without the help of healthcare professionals (nurses or surgeons) who were engaged in aftercare. In the case of missing data, hospital records of patient visits and pharmacy records of purchases were collected. Caregivers were asked to provide information on any further purchases of medication(s) in the follow-up period.
CLINICAL BENEFITS OF HEALTH PROFESSIONAL-LED COUNSELING AND PROFESSIONAL-LED AFTERCARE: The clinical benefits of health professional-led counseling and aftercare of children who underwent elective tonsillectomy for tonsillitis were evaluated. Scores for health professional-led counseling and health professional-led aftercare were calculated from the risk of undercare, as expressed in equation 1. The risk of undercare was defined by a calculation that involved the intensities of post-tonsillectomy pain above which the children was received post-tonsillectomy analgesic medications (equation 2). The differences in postoperative pain intensities ranged from 0% to 100%. The beneficial score of the health professional-led counseling and health professional-led aftercare is the area above the curve of the counseling and care method, and the working area is the area under the curve of the adopted counseling and care methods. For all counseling and care, the reference standard used was 15% or more difference in postoperative pain and 10% or more difference in incidence of postoperative immediate and late complications in children regarding the negative control group (children and their parents who did not receive preoperative professional-led counseling and received only postoperative surgeons’ visits during hospital stays) [16].
PERSONAL SATISFACTION:
Our institute has its own personal satisfaction form for the parents or guardians of the enrolled children. It includes 3 items: prehospital service, hospital stay, and posthospital service. Personal satisfaction was assessed at the 6-months of follow-up. The grading of personal satisfaction (for prehospital service, hospital stay, and posthospital service) was 0=completely dissatisfied; 0.25=dissatisfied; 0.5=partially satisfied; 0.75=satisfied; and 1=extremely satisfied. The total score was 3, and the higher the score, the higher the satisfaction level.
STATISTICAL ANALYSES:
GraphPad 3.01 Software (San Diego, CA, USA) was used for statistical analysis. Categorial, continuous normal, and continuous non-normal variables are depicted as frequencies with percentages in parenthesis, mean±SD, and median with Q3-Q1 in parenthesis. Soup calculator® was used to calculate quartile values. The chi-square test (χ2 test) with Yate’s corrections (2×2 tables) of independence (large numbers of tables) or Fisher’s exact test (2×2 tables) was used for categorical variables for statistical analysis. Kolmogorov and Smirnov methods are used to check the normality of data distribution. For normal continuous variables, one-way analysis of variance (ANOVA) was used for statistical analysis. Kruskal-Wallis’ test (nonparametric ANOVA) and Mann-Whitney test (between cohorts) or Friedman’s test (within cohort) were used for statistical analysis of non-normal continuous variables. Tukey’s (for normal) and Dunn’s (for non-normal) multiple comparisons tests were used for post hoc analysis of continuous variables. A
Results
STUDY POPULATION:
From September 20, 2020, to October 1, 2023, 114 children who underwent elective tonsillectomies were reported at the First Affiliated Hospital of Soochow University, Suzhou, Jiangsu, China, and the referring institute for tonsillitis. Among these 114 children, 5 had neurocognitive deficits and 7 had chronic pain. Therefore, the data from these (5+7=12 children) were excluded from analyses. Intensities of postoperative pain (Faces Pain Scale-Revised scale) at discharge and at 6-month follow-up, frequencies of postoperative complications in 102 children undergoing elective tonsillectomy, postoperative analgesic dosage (during 6 months after surgery), and hospital stay were collected from electronic records of institutes and evaluated. A flow diagram of this retrospective study is shown in Figure 1.
DEMOGRAPHIC AND CLINICAL CONDITIONS:
The sex ratio was almost 1: 1. The children were 7.78±2.25 years of age (minimum: 4 years, maximum: 12 years), ethnically Han Chinese, and caregivers were mostly their mothers. The demographic and clinical conditions of the children are presented in Table 1 and there were no significant differences among the 3 groups.
POSTOPERATIVE PAIN INTENSITY:
All the children experienced postoperative pain at discharge. Postoperative pain was 4 (IQ range, 5–4) per child at discharge from the hospital. At 1-month follow-up, postoperative pain was reported to be 2 (3–1) per child, 1 (1–0) per child, and 0 (0–0) for the USS, FSS, and NCC cohorts, respectively. At 1-month follow-up, postoperative pain was reported to be decreased in all children of all cohorts as compared to at the discharge conditions. Children in the NCC cohort had less postoperative pain at discharge and at 1 month after surgeries than those in the FSS and UUS cohorts. The children in the FSS cohort had less postoperative pain at discharge and 1 month after surgeries than those in the UUS cohort.
POSTOPERATIVE ANALGESIC DOSAGE:
Children in the NCC cohort consumed less tramadol during hospital stays after surgery and 6 months of follow-up than those in the FSS and UUS cohorts. The children in the FSS cohort consumed less tramadol during hospital stays after surgery and 6 months of follow-up than those in the UUS cohort.
HOSPITAL STAYS:
Hospital stays were longer for children in the UUS cohort than in the NCC cohort. Hospital stays were equal for children in the FSS and UUS cohorts, and between the NCC and FSS cohorts.
PERSONAL SATISFACTION: Personal satisfaction for parents or guardians of patients was higher for children in the NCC cohort than for children in the FSS and UUS cohorts. Personal satisfaction for parents or guardians of patients was higher for children in the FSS cohort than for children in the USS cohort. The details of outcome measures are presented in Table 2.
POST-TONSILLECTOMIES COMPLICATIONS:
Incidences of immediate and late postoperative complications, especially anxiety and vomiting, were higher among children in the UUS cohort, followed by those of children in the FSS and NCC cohorts. Nausea was reported in all the children who underwent tonsillectomies. Dysphagia was reported only in children in the UUS cohort. Half of children across all cohorts who underwent tonsillectomy had fever and vomiting, and one-third experienced dizziness. A total of 56 (55%) children had a decrease in oral intake during the follow-up period. The details of immediate (during hospital stays of patients) and late (after discharge of patients at 6 months of follow-up) postoperative complications are reported in Table 3.
CLINICAL BENEFITS FOR HEALTH PROFESSIONAL-LED COUNSELING AND PROFESSIONAL-LED AFTERCARE: A total of 26 and 8 children from the NCC and FSS cohorts, respectively, had 15% or more differences in postoperative pain and 10% or more in the differences in the incidence of postoperative immediate and late complications in the UUS cohort. Children in the NCC, FSS, and UUS cohorts had 0–0.9 beneficial scores of 0–0.1 beneficial scores, and no beneficial scores, respectively. Above 0.9, 0.1, and 0 beneficial scores, the children of the NCC, FSS, and UUS cohorts were at risk of under-treatment, respectively. If there were more than the 88% and more than the 24% differences in the incidence of post-tonsillectomies pain and immediate and late complications in children regarding the USS cohort, the children were at risk of under-treatment for the NCC and the FSS cohorts, respectively. The details of the clinical benefits of health professional-led counseling and professional-led aftercare are shown in Figure 2 and Table 4. Results of the assumption tests are presented in Table 5.
Discussion
Postoperative pain was higher at discharge and mild at 1-month follow-up visit. The results of postoperative pain in the current study are consistent with those of a randomized clinical trial [1], a prospective study on adult patients [17], and observational, longitudinal study [4], a randomized controlled trial [9], a prospective study [10], a qualitative interview study [18], a prospective quasi-experimental pilot study [2], and a randomized trial [19]. The higher incidence of postoperative pain at discharge and at 1-month follow-up could be attributed to specific factors such as surgical technique, children characteristics, for example, female gender. The enrolled children had more postoperative pain than expected at discharge and at 1-month follow-up after tonsillectomy.
Immediate and late postoperative complications, especially anxiety and vomiting, were higher among children in the UUS cohort, followed by those of children in the FSS and NCC cohorts. The results of postoperative complications are consistent with those of randomized controlled trials [9], prospective studies [10], qualitative interview studies [18], and randomized clinical trials [1]. Follow-up care does not affect postoperative events [10]. The significant differences in anxiety and vomiting in the study populations from the available studies [1, 10] could be due to the small sample size or the use of analgesic medicine itself (more analgesic use among children in the UUS cohort). Critical assessments are required for the potential reasons for the observed differences between cohorts, such as the impact of sample size or analgesic use. Professional-led counseling and follow-up care did not have a significant effect on postoperative complications in children after tonsillectomy.
More than 50% of children had a decrease in oral intake, consistent with results of a randomized clinical trial [1], but differing from a prospective study [10]. Pain intensity after surgery in the 1-month follow-up was higher in the current study, and children with pain often have decreased oral intake [10]. In addition, early discharge of children after tonsillectomy is associated with more complications during follow-up [1]. After tonsillectomy, children generally have a decrease in oral intake because of poor pain control and nausea.
Personal satisfaction for children and their caregivers was highest among children and caregivers of the NCC cohort, followed by those of children and caregivers of the UUS and FSS cohorts. Greater frequency and availability of nurses at institutes may increase personal satisfaction among children and their caregivers. The details of the comparative studies on children and adults undergoing tonsillectomy in different settings are presented in Table 6.
The risk of under-treatment was lower for children in the NCC cohort than in the FSS cohort. Nurse-led counseling and postoperative care can provide good pain control and patient satisfaction, which can help to decrease pain intensity in children. Nurse-led counseling and postoperative care are more helpful for children after tonsillectomy than other professional-led counseling and postoperative care.
This study has several limitations. The small sample size may have led to type I errors. The measurement of pain intensity, which was the primary objective of the study, was subjective but not objective. The study explained the reason for good personal satisfaction as frequencies and availabilities of nurses at institutes than those of surgeons. However, the statement about intervention of NCC and FSS were similarly that a nurse or surgeon visit every month. The possible justification for this is that a nurse or surgeon visit every month this is protocol but surgeons visit during their outpatient department (OPD), however, nurse were not engaged in the OPD. The study has avoided reporting of postoperative pain and frequencies of postoperative complications according to the matter of surgical technique for the procedure itself, which as previous studies showed patients who undergo intracapsular tonsillectomy particularly using coblation have a shorter recovery period and require less analgesia. This is a limitation of our study. Types of surgical technique and anesthesia methods were not evaluated because these were accessible to anesthesiologists and surgeons. However, the authors are nursing staff from the pediatric surgery department.
Conclusions
Children may have more post-tonsillectomy pain than expected at discharge and follow-up for tonsillitis due to specific factors of children themselves. Professional-led counseling and follow-up care did not have a significant effect on post-tonsillectomy complications. After tonsillectomy, children generally had a decrease in oral intake attributed to post-tonsillectomy complications, especially nausea. Professional-led counseling, especially nurse-led counseling and professional-led follow-up care, can improve personal satisfaction for children and their caregivers for curative tonsillectomy surgeries due more frequent nurse visits and greater availability of nurses.
Availability of Data and Materials
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Figures
 Figure 1. The flow diagram of the retrospective study. Red color indicates poor outcomes. Green color indicates good outcomes. Black color indicates not worse but not good outcomes.
Figure 1. The flow diagram of the retrospective study. Red color indicates poor outcomes. Green color indicates good outcomes. Black color indicates not worse but not good outcomes.  Figure 2. The schematic presentation of the clinical benefits of health professional-led counseling and professional-led aftercare.
Figure 2. The schematic presentation of the clinical benefits of health professional-led counseling and professional-led aftercare. Tables
Table 1. Demographical and clinical conditions of the enrolled children who underwent curative surgeries for tonsillitis. Table 2. Outcome measures of the enrolled children after curative surgeries for tonsillitis.
Table 2. Outcome measures of the enrolled children after curative surgeries for tonsillitis. Table 3. Immediate (during hospital stays of patients) and late (after discharge of patients in 6-months of follow-up) postoperative complications of the enrolled children after tonsillitis.
Table 3. Immediate (during hospital stays of patients) and late (after discharge of patients in 6-months of follow-up) postoperative complications of the enrolled children after tonsillitis.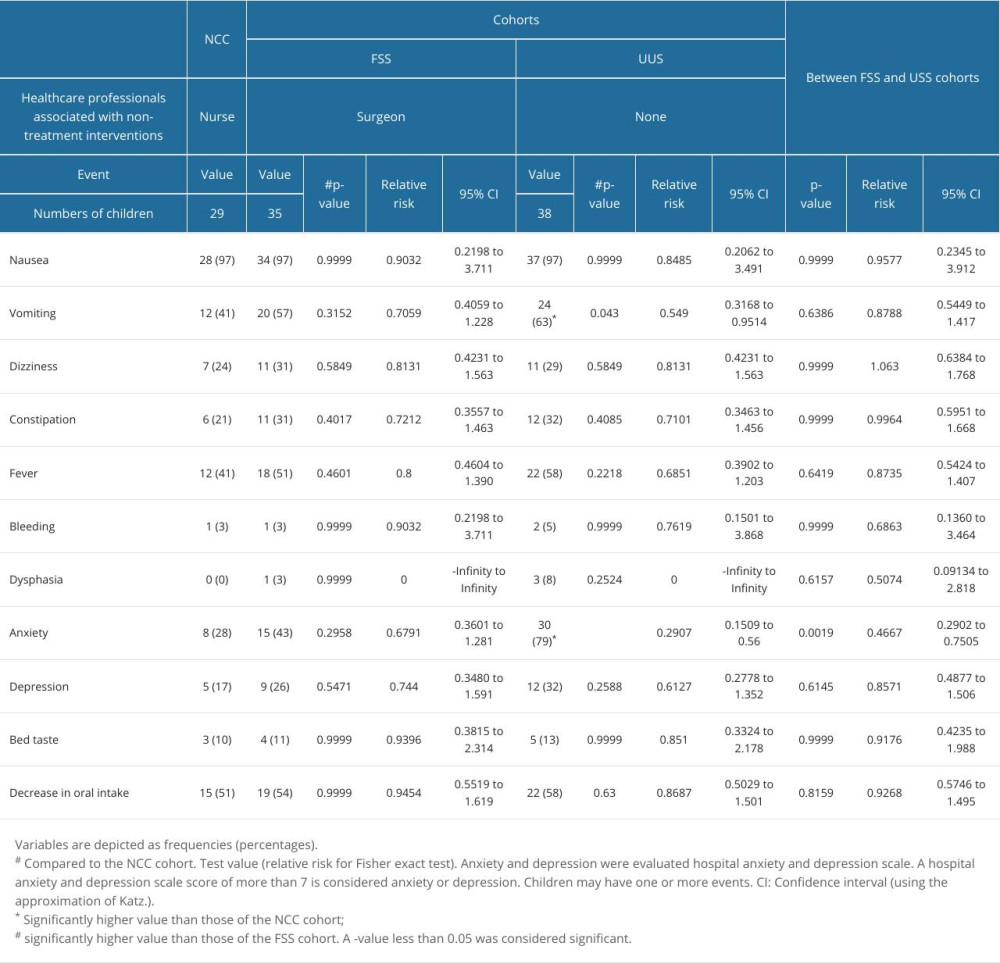 Table 4. Values of the clinical benefits of health professional-led counseling and professional-led aftercare for curative tonsillitis in children.
Table 4. Values of the clinical benefits of health professional-led counseling and professional-led aftercare for curative tonsillitis in children. Table 5. Results of assumption tests.
Table 5. Results of assumption tests. Table 6. Comparative studies on children/adults undergoing tonsillectomy in different settings for tonsillitis.
Table 6. Comparative studies on children/adults undergoing tonsillectomy in different settings for tonsillitis.
References
1. Paquette J, le May S, Lachance FJ, A randomized clinical trial of a nurse telephone follow-up on paediatric tonsillectomy pain management and complications: J Adv Nurs, 2013; 69(9); 2054-65
2. Wozney L, Vakili N, Chorney J, The impact of a text messaging service (tonsil-text-to-me) on pediatric perioperative tonsillectomy outcomes: Cohort study with a historical control group: JMIR Perioper Med, 2022; 5(1); e39617
3. Song JSA, Wozney L, Chorney J, Design and validation of key text messages (Tonsil-Text-To-Me) to improve parent and child perioperative tonsillectomy experience: A modified Delphi study: Int J Pediatr Otorhinolaryngol, 2017; 102; 32-37
4. Lao BK, Kain ZN, Khoury D, A comprehensive examination of the immediate recovery of children following tonsillectomy and adenoidectomy: Int J Pediatr Otorhinolaryngol, 2020; 135; 110106
5. Dorkham MC, Chalkiadis GA, von Ungern Sternberg BS, Davidson AJ, Effective postoperative pain management in children after ambulatory surgery, with a focus on tonsillectomy: Barriers and possible solutions: Paediatr Anaesth, 2014; 24(3); 239-48
6. Zhou Y, Peng M, Zhou J, Quality of life in children undergoing tonsillectomy: A cross-sectional survey: Ital J Pediatr, 2023; 49(1); 52
7. Lancer HR, Beech T, Weller M, Secondary post-tonsillectomy haemorrhage: Is there evidence of diurnal and monthly variation in haemorrhage rates?: J Laryngol Otol, 2023; 137(9); 1017-21
8. Kaminsky O, Fortier MA, Jenkins BN, Children and their parents’ assessment of postoperative surgical pain: Agree or disagree?: Int J Pediatr Otorhinolaryngol, 2019; 123; 84-92
9. van Vliet LM, Godfried MB, van Deelen GW, Placebo effects of nurses’ communication alongside standard medical care on pain and other outcomes: A randomized controlled trial in clinical tonsillectomy care: Psychother Psychosom, 2020; 89(1); 56-58
10. Xin Y, Li X, Du J, Efficacy of telephone follow-up in children tonsillectomy with day surgery: Indian J Pediatr, 2019; 86(3); 263-66
11. Malley A, Kenner C, Kim T, Blakeney B, The role of the nurse and the preoperative assessment in patient transitions: AORN J, 2015; 102(2); 181e1-e9
12. Wainwright TW, Jakobsen DH, Kehlet H, The current and future role of nurses within enhanced recovery after surgery pathways: Br J Nurs, 2022; 31(12); 656-59
13. van Vliet LM, van Dulmen S, Thiel B, Examining the effects of enhanced provider-patient communication on postoperative tonsillectomy pain: Protocol of a randomised controlled trial performed by nurses in daily clinical care: BMJ Open, 2017; 7(11); e015505
14. Soleymanifard F, Khademolhoseyni SM, Nouri JM, Nursing process in post tonsillectomy pain diagnosis: A systematic review: Glob J Health Sci, 2014; 7(1); 180-87
15. Atisook R, Euasobhon P, Saengsanon A, Jensen MP, Validity and utility of four pain intensity measures for use in international research: J Pain Res, 2021; 14; 1129-39
16. Zhang Y, Yu D, Yang Q, Li W, Diagnostic efficacy of physical examination, preoperative ultrasound, and/or computed tomography in detecting lymph node metastasis: A single-center retrospective analysis of patients with squamous cell carcinoma of the head and neck: Oral Surg Oral Med Oral Pathol Oral Radiol, 2022; 134(3); 386-96
17. Zagólski O, Gajda M, Stręk P, Adult tonsillectomy: Postoperative pain depends on indications: Braz J Otorhinolaryngol, 2016; 82(5); 589-95
18. Idvall E, Holm C, Runeson I, Pain experiences and non-pharmacological strategies for pain management after tonsillectomy: A qualitative interview study of children and parents: J Child Health Care, 2005; 9(3); 196-207
19. Sutters KA, Savedra MC, Miaskowski C, Children’s expectations of pain, perceptions of analgesic efficacy, and experiences with nonpharmacologic pain management strategies at home following tonsillectomy: J Spec Pediatr Nurs, 2007; 12(3); 139-48
Figures
Figure 1. The flow diagram of the retrospective study. Red color indicates poor outcomes. Green color indicates good outcomes. Black color indicates not worse but not good outcomes.Figure 2. The schematic presentation of the clinical benefits of health professional-led counseling and professional-led aftercare. Tables
Table 1. Demographical and clinical conditions of the enrolled children who underwent curative surgeries for tonsillitis.Table 2. Outcome measures of the enrolled children after curative surgeries for tonsillitis.Table 3. Immediate (during hospital stays of patients) and late (after discharge of patients in 6-months of follow-up) postoperative complications of the enrolled children after tonsillitis.Table 4. Values of the clinical benefits of health professional-led counseling and professional-led aftercare for curative tonsillitis in children.Table 5. Results of assumption tests.Table 6. Comparative studies on children/adults undergoing tonsillectomy in different settings for tonsillitis.Table 1. Demographical and clinical conditions of the enrolled children who underwent curative surgeries for tonsillitis.Table 2. Outcome measures of the enrolled children after curative surgeries for tonsillitis.Table 3. Immediate (during hospital stays of patients) and late (after discharge of patients in 6-months of follow-up) postoperative complications of the enrolled children after tonsillitis.Table 4. Values of the clinical benefits of health professional-led counseling and professional-led aftercare for curative tonsillitis in children.Table 5. Results of assumption tests.Table 6. Comparative studies on children/adults undergoing tonsillectomy in different settings for tonsillitis. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387