23 February 2025: Clinical Research
Efficacy of King’s Combined Uterine Suture in Managing Placenta Accreta: A Retrospective Analysis
Wenqiang You ABCDEF 1, JinXiao Lin BCDF 1, LiPing Hu BCDFG 1*
DOI: 10.12659/MSM.945826
Med Sci Monit 2025; 31:e945826






Abstract
BACKGROUND: Placenta accreta is a spectrum disorder that can include an abnormally adherent placenta to placental tissue that invades the endometrium and myometrium and results in hemorrhage during or after delivery. King’s combined uterine suture is a combination of parauterine vascular ligation with longitudinal suturing of the lower uterine segment. This retrospective study aimed to evaluate outcomes from using King’s combined uterine suture for hemostasis in 49 parturient women with placenta accreta spectrum (PAS).
MATERIAL AND METHODS: Clinical data of parturient women with placenta accreta in Fujian Maternal and Child Health Hospital from January 2020 to January 2023 were retrospectively collected. King’s combined uterine suture ligation surgery was performed in these patients who had placenta accreta. Placenta accreta was diagnosed by the criteria for PAS. The outcomes of surgery and prognosis of newborns were analyzed.
RESULTS: A total of 49 parturient women were included and underwent successful intraoperative hemostasis without hysterectomy or ureteral injury. There were 4 cases of bladder rupture and 17 cases of uterine plastic surgery. The average intraoperative bleeding volume of the 49 patients was (507±162) mL. Patients had no long-term complications during postoperative follow-up. Apgar score of newborns was 9.67±0.77, and there was no asphyxia or neonatal death.
CONCLUSIONS: King’s combined uterine suture ligation surgery is applied to placenta accreta, which not only has a definite and fast hemostatic effect, but can also effectively preserve the uterus.
Keywords: Placenta Previa, Placenta Accreta, Hemorrhage, Hemostasis, Humans, Female, Pregnancy, Retrospective Studies, Placenta Accreta, adult, Ligation, Uterus, Suture Techniques, Treatment Outcome, Infant, Newborn, Sutures, Postpartum Hemorrhage
Introduction
In recent years, the prevalence of placenta accreta spectrum (PAS) has seen a substantial increase due to adjustments in fertility policies in China and a rise in cesarean delivery rates [1]. PAS includes placenta accreta, placenta increta, and placenta percreta [2]. Prenatal diagnosis of PAS is helps to provide optimal obstetric management and can significantly reduce the incidence of major bleeding and maternal mortality in pregnant women [3]. This surge in incidence poses significant challenges, given the associated risks of massive bleeding during prenatal, intraoperative, and postoperative stages [4]. The complications extend to potential hemorrhagic shock and disseminated intravascular coagulation, and, in severe cases, can necessitate a hysterectomy, highlighting the critical need for effective interventions to manage intraoperative bleeding in placenta previa [5,6].
Various surgical methods have been proposed by researchers worldwide to address this issue. Early techniques, such as continuous suture, interrupted suture, mattress suture, double suture, purse-string suture, figure-of-eight suture, the B-Lynch suture, square suturing, and uterine artery embolization, have been considered [7,8]. In recent years, a popular approach involves combining cesarean delivery with abdominal aortic balloon intervention to block uterine blood supply [9,10]. However, its use is declining in advanced centers due to its adverse effects and the development of surgical techniques.
In response to these challenges, our hospital has implemented King’s combined uterine suture ligation surgery (KCUSLS) as a novel approach to address PAS. KCUSLS involves a combination of parauterine vascular ligation with longitudinal suture of the lower uterine segment, which achieves effective hemostasis and has shown a promising application prospect in PAS [11].
Therefore, this retrospective study aimed to evaluate outcomes from using KCUSLS for hemostasis in 49 parturient women with PAS. We hope that this study will provide valuable insights to improve the surgical approach to PAS, ultimately improving patient outcomes and reducing the need for hysterectomy in patients with these high-risk pregnancies.
Material and Methods
ETHICAL APPROVAL OF THE RESEARCH PROTOCOL:
The study obtained ethical approval from the Institutional Review Committee of Fujian Maternal and Child Health Hospital. All participants and guardians of participants provided written informed consent.
SOURCE:
A total of 49 cases of postpartum women with placenta previa who were hospitalized and delivered in the Obstetrics Department of Fujian Maternal and Child Health Hospital from January 2020 to January 2023 were retrospectively collected. All of them were included in the study and underwent KCUSLS. The average age of these parturient women was 33.08±4.61 years, gestational week was 36.00±2.37 weeks, gestational frequency was 3.76±1.45, and delivery frequency was 1.16±0.71. Among them, 40 women (82.0%, 40/49) had a history of cesarean delivery, with a previous frequency of 1.16±0.71.
INCLUSION CRITERIA:
The inclusion criteria were as follows. (1) Placental adherence/invasion met the diagnostic criteria for PAS [12]: PAS is an abnormal adhesion or invasion of placental villi in the uterus and is categorized as placenta accreta, placenta increta, and placenta percreta, depending on the degree of invasion. Placenta accreta: the placental villi adhere only to the surface of the myometrium and do not invade the myometrium. Placenta increta: the placental villi invade the myometrium but do not penetrate the entire myometrium. Placenta percreta: the placental villi not only invade the myometrium, but also penetrate the myometrium and may enter paratesticular tissues, such as the bladder or rectum. (2) Secondary or higher color ultrasound indicated central placenta previa with placental implantation after 28 weeks of pregnancy. (3) Magnetic resonance imaging indicated placental implantation. (4) There was no coagulation dysfunction. (5) Placental implantation had been confirmed based on intraoperative conditions and/or postoperative pathology. (6) The cesarean delivery was performed by the same team, and KCUSLS was used. All patients were required to meet the above 5 criteria simultaneously.
PREOPERATIVE PREPARATION:
Two groups of venous channels were established by central venipuncture before surgery, and autologous blood transfusion equipment and insulation blankets were prepared. Excessive bleeding was evaluated, and 4 units of blood were collected before surgery. If there was excessive bleeding, timely blood transfusion could be performed. The patients and their family were fully communicated with, to emphasize the possibility of hysterectomy and bladder rupture, and an informed consent form was signed before surgery.
ANESTHESIA:
The recommended anesthesia method was general anesthesia. In fact, all 49 patients in this study were given general anesthesia.
INCISION SELECTION:
To facilitate exposure of the field of view, a lower abdominal incision was chosen.
SPECIFIC SURGICAL PROCEDURE:
After entering the abdomen, if there were adhesions, it was necessary to sufficiently separate the pelvic adhesions and free the uterus. The distended vessels on the surface of the uterus (see Figure 1) should be clamped and ligated in segments to achieve hemostasis. Ligation of these vessels takes anywhere from about 15 min to 30 min, and labor takes about 1 h. The peritoneum over the bladder was incised, and the bladder-uterus reflection was opened, and both sides were separated as much as possible to push the bladder to the level of the internal orifice of the cervix. Depending on the presentation of the fetus, an appropriate incision was chosen. Typically, a relatively high-positioned oblique incision was chosen, and the incision avoided the placenta and engorged blood vessels as much as possible.
Before the placenta was delivered, the uterus was directly pulled out of the abdominal cavity, and a large cotton pad was placed behind the uterus to push away the intestinal loops. The uterine incision and the placenta were clamped with 6 to 8 toothless oval forceps. Simultaneously, rapid ligation of bilateral uterine artery parametrial vessels was performed (the lowest ligation point should be below the bleeding point). The specific steps were as follows: the uterus was pulled out of the abdominal cavity, the bladder was pushed down and the peritoneum was folded to the internal orifice of the cervix; after feeling the pulsation of the uterine artery, the inner side of the uterine artery about 2 to 3 cm away from the uterine edge, No. 1 absorbable suture was used to suture the anterior and posterior walls of the uterus from front to back, and then from back to front through the avascular zone of the broad ligament, and the knot was tied. The same method was done on the other side.
If there was still excessive bleeding, rapid ligation of bilateral utero-ovarian artery anastomotic branches was performed. The specific steps were as follows: the needle was inserted 2 to 3 cm below the lateral edge of the uterine anterior wall under the round ligament. The other steps were the same as for the ligation of bilateral uterine artery parametrial vessels (see Figure 2).
Then, the placenta was manually detached, and complete removal of the placental tissue was attempted. If the placenta was deeply embedded in the anterior uterine wall or even penetrated, and the anterior wall of the uterus was thin and had lost its normal shape, the penetrated part of the uterine wall and placenta were excised (see Figures 3, 4).
With a No. 1 absorbable suture with a round needle, from front to back at a point 1 cm above the internal orifice of the cervix, 1 to 2 cm away from the right edge of the uterus, the anterior and posterior walls of the uterus were sutured. With the needle from back to front at a point 1cm below the upper edge of the uterine incision and 3 to 4 cm inside the right edge of the uterus, the anterior and posterior walls of the uterus were sutured, and the knot was tied on the anterior wall of the uterus. The left side was sutured in the same way (see Figure 5). In cases with significant loss of uterine anterior wall, uterine reconstruction was performed after hemostasis, and the abdomen was closed step by step.
INTRAOPERATIVE HEMOSTASIS SUPPLEMENT PROGRAM:
After the delivery of the fetal head, a routine intravenous injection of 100 μg of cabezine oxytocin was used during surgery. Additionally, 250 μg carboprost tromethamine was injected into the uterine body. If there was still a minor oozing of blood, uterine balloon compression was considered to stop the bleeding, including compressing the lower segment of the uterus and the inner opening of the cervix.
POSTOPERATIVE TREATMENT:
Postoperatively, patients were transferred to the Intensive Care Unit to prevent infection, and they were treated with oxytocin. Patients were given continuous component blood transfusion, if necessary, and were closely observed for vaginal bleeding and vital signs.
OBSERVATION TARGET:
Intraoperative bleeding volume, number of blood transfusions and transfusion volume (including autologous blood transfusions), surgical time, hysterectomy rate, bladder and ureteral injury rate, neonatal Apgar score, and asphyxia rate were observed in this study.
EVALUATION OF BLEEDING AMOUNT:
After blood was collected via suction, it was weighed and measured indirectly with a gauze pad.
STATISTICAL ANALYSIS:
Statistical analysis of the data was conducted using SPSS 24.0 software (IBM Corp, Armonk, NY, USA). Normally distributed data were represented as mean±SD. Non-normal distribution data were represented by the median quartile (M [P25–P75]).
Results
INTRAOPERATIVE SITUATION:
A total of 49 cases of puerperant women were confirmed, with varying degrees of PAS during the performed surgery, including 9 cases of placenta accreta (18.36%, 9/49), 23 cases of placenta increta (46.9%, 23/49), and 17 cases of placenta percreta (34.6%, 17/49). A total of 28 of 49 parturient women underwent pathological examination, and postoperative pathological diagnosis was confirmed as placental implantation. The average intraoperative bleeding volume of 49 patients was (507±162) mL. Fifteen patients (30.61%, 15/49) had intraoperative bleeding volume >500 mL, and 24 patients (48.9%, 24/49) received component transfusion. The median infusion of red blood cell suspension was 4.0 U. Eighteen patients underwent plasma transfusion, and the median was 400 mL (36.73%, 18/49). Nine patients (18.36%, 9/49) underwent autologous blood transfusion. Uterine balloon compression for hemostasis was used in 2 patients. Operative time was 107.51±532 min, and Apgar score of newborn was 9.67±0.77, with no asphyxia and no neonatal death. Some patients had part of the placenta penetrating the anterior wall of the uterus, which was thin and lost its normal shape. After excision, 17 patients underwent uterine plastic surgery. There was no hysterectomy or ureteral injury, but 4 patients showed bladder rupture during surgery (Table 1).
POSTOPERATIVE OBSERVATION AND FOLLOW-UP:
All patients recovered well and were discharged from the hospital 5 to 7 days after surgery. Complications, such as late postpartum hemorrhage, necrosis or infection of the lower segment of the uterus, or adhesions in the uterine cavity, were not found during maternal follow-up. However, 1 case of urinary tract infection occurred during the placement of a urinary catheter after bladder rupture repair surgery and recovered well after symptomatic treatment.
Discussion
The blood supply in the lower uterine segment during late pregnancy is significantly increased, compared with non-gestation [13]. When combined with placental implantation, the blood supply to the placental attachment in the lower segment of the uterus further increases, presenting vascular dilation [14]. Much neovascularization occurs between the surface of the lower segment of the uterus and the endometrium, as well as between the lower segment of the uterus and the bladder [15]. In addition, during pregnancy, the placenta continuously grows in the lower segment, causing the uterus to expand, and even erodes the uterine serosa, resulting in weak or even missing smooth muscle in the lower segment of the uterus [16]. Once this situation occurs, it is not possible to stop bleeding through effective muscle contraction and compression. After artificial placental dissection, the blood sinuses open, leading to massive bleeding, hypovolemic shock, disseminated intravascular coagulation, hysterectomy, and even death [17]. Therefore, it is essential to explore fast and effective hemostatic methods for reducing intraoperative bleeding during placental implantation, hysterectomy rates, and maternal mortality rates.
Currently, there are various surgical methods for hemostasis. The B-Lynch suture and Hayman’s suture are effective in treating postpartum hemorrhage caused by uterine atony, but the effect is not satisfactory in treating lower segment bleeding caused by placenta previa [18]. The placement of intrauterine balloons or gauze can be applied only as a supplementary hemostasis method after placenta previa delivery procedure [19]. With the development and collaboration of multiple disciplines in recent years, interventional therapy has been applied to patients with placental implantation. Many scholars have attempted to perform cesarean delivery while temporarily blocking the blood supply to the lower segment of the uterus with an abdominal aortic balloon, reducing intraoperative bleeding and hysterectomy rates [20]. However, there are some risks in abdominal aortic balloon occlusion surgery, such as abdominal aortic rupture, thrombosis, and failure of balloon catheter implantation. Moreover, many medical institutions lack intervention facilities or relevant experience, and the high cost has certain limitations in clinical work.
KCUSLS, proposed in this article, is a conservative surgical method for the treatment of placental implantation, which was applied to 49 patients with placenta accreta, and successful intraoperative hemostasis was achieved. There were no cases of uterine resection or ureteral injury, and maternal and neonatal outcomes were favorable. However, there were 4 cases of bladder rupture during the surgery, all of which occurred when the bladder was displaced upward and strongly adherent to the anterior wall of the uterus, with the placenta almost penetrating the thin anterior wall. Repair of the bladder rupture was performed by urological surgeons. To reduce the risk of bladder rupture, we are considering the involvement of urological surgeons in assisting with bladder displacement prior to the procedure, to observe whether it can reduce the incidence of bladder rupture [21].
KCUSLS has many advantages. First, the simple operation steps can quickly and effectively stop bleeding, making it simpler and easier to learn than other conservative surgical methods, such as iliac artery ligation. Second, all wound sutures are performed under direct visualization, allowing for intuitive observation of bleeding and a high success rate in hemostasis. Third, longitudinal suturing of the uterus keeps the lower segment of the uterus and cervical canal unobstructed, without forming a closed space inside the uterus, which is beneficial for blood discharge. Its hemostatic mechanism involves ligating the blood vessels adjacent to the bilateral uterine arteries to block blood supply to the lower segment. Ligating the uterine artery-ovarian collateral arteries obstructs blood flow to the upper segment of the uterus [22]. Longitudinal parallel compression, suturing, twisting, and closure of the uterine vascular bed and its branches from the lateral edge to the lower segment reduces blood supply [23]. Additionally, the close apposition and mechanical compression of the anterior and posterior walls of the uterus contribute to reducing bleeding [24]. Overall, the blood flow to the upper segment, lower segment, and lateral edges of the uterus is effectively obstructed, resulting in a reduction in intraoperative bleeding [25]. In the study by Xia et al [11], KCUSLS was revealed as an effective method for uterine hemostasis during cesarean delivery, which similar to our results.
The technique of KCUSLS is relatively simple to perform, but there are some important considerations in clinical practice. If there are adhesions in the abdominal cavity, it is necessary to separate the adhesions and completely free the uterus before proceeding to the next step. Before incising the uterine muscle layer, the bladder should be pushed down to the level of the cervical os or even lower and prepared for uterine artery ligation. This helps to minimize the time for hemostasis and reduces bleeding.
Performing uterine artery ligation before the delivery of the placenta is crucial. If the uterine artery ligation is performed after the delivery of the placenta, it can lead to significant intraoperative bleeding. In cases in which the placenta penetrates the anterior wall of the uterus and the bladder is adherent to the weakened anterior wall, there is a risk of bladder rupture during the process of pushing down the bladder. This can lead to continuous bleeding from placental abruption. In such cases, it may be advisable to wait until after the delivery of the fetus, when the uterus has contracted and the uterine wall is relatively thick, before pushing down the bladder.
In patients with endometriosis or pelvic adhesions due to multiple surgeries, it can be difficult to expose the posterior wall of the lower segment of the uterus, making it challenging to perform uterine artery ligation at the level of the cervical os. Hemostasis needs to be individualized in such cases. It is important to perform uterine artery ligation as low as possible, and during longitudinal suturing, puncture through the anterior wall and needle entry into the posterior wall should be guided by sensation and remain within the uterine muscle layer to avoid injury to other organs.
In addition, the sample size of this study was small, and the study population came from a single source, and more definitive conclusions are yet to be further confirmed by a large-sample, multicenter study.
Conclusions
The application of KCUSLS in placental implantation has a perfect hemostatic effect. It is fast and effective, which can lead to effectively preserving the uterus, and it is simple and easy to implement. It is worth promoting and applying, especially in specialized hospitals without vascular departments. However, more clinical practice is needed to avoid damaging adjacent organs, such as the bladder, during surgical procedures.
Figures
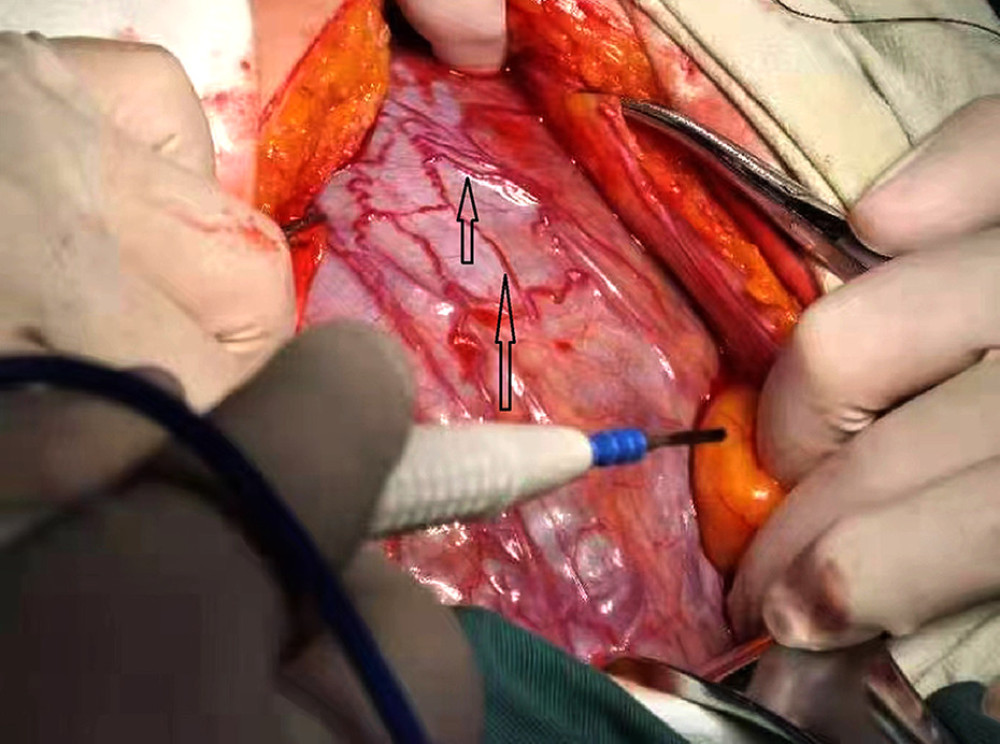 Figure 1. The distended vessels on the surface of the uterus for placental implantation. The arrow points to distended vessels. Production software: Adobe Photoshop21.1.0.106.
Figure 1. The distended vessels on the surface of the uterus for placental implantation. The arrow points to distended vessels. Production software: Adobe Photoshop21.1.0.106.  Figure 2. a) Ligation of parametrial blood vessels. b) Ligation of the communicating branch of the ovary. Production software: Adobe Photoshop21.1.0.106.
Figure 2. a) Ligation of parametrial blood vessels. b) Ligation of the communicating branch of the ovary. Production software: Adobe Photoshop21.1.0.106.  Figure 3. Placental implantation penetrating the anterior wall of the uterus. The arrow points to placenta previa. Production software: Adobe Photoshop21.1.0.106.
Figure 3. Placental implantation penetrating the anterior wall of the uterus. The arrow points to placenta previa. Production software: Adobe Photoshop21.1.0.106.  Figure 4. Uterine plastic surgery was performed to remove the penetrating part of the uterine wall and placenta, as the anterior wall of the uterus was weak and lost its normal shape. Production software: Adobe Photoshop21.1.0.106.
Figure 4. Uterine plastic surgery was performed to remove the penetrating part of the uterine wall and placenta, as the anterior wall of the uterus was weak and lost its normal shape. Production software: Adobe Photoshop21.1.0.106.  Figure 5. Front view of longitudinal parallel compression suture of the anterior and posterior walls of the lower segment of the uterus. Production software: Adobe Photoshop21.1.0.106.
Figure 5. Front view of longitudinal parallel compression suture of the anterior and posterior walls of the lower segment of the uterus. Production software: Adobe Photoshop21.1.0.106. 
References
1. Zhou C, Zhao Y, Li Y, Clinical analysis of factors influencing the development of placenta praevia and perinatal outcomes in first-time pregnant patients: Front Surg, 2022; 9; 862655
2. Hecht JL, Baergen R, Ernst LM, Classification and reporting guidelines for the pathology diagnosis of placenta accreta spectrum (PAS) disorders: Recommendations from an expert panel: Mod Pathol, 2020; 33(12); 2382-96
3. Rao J, Fan D, Zhou Z, Maternal and neonatal outcomes of placenta previa with and without coverage of a uterine scar: A retrospective cohort study in a tertiary hospital: Int J Womens Health, 2021; 13; 671-81
4. Wang Y, Jiang T, Huang G, Long-term follow-up of abdominal aortic balloon occlusion for the treatment of pernicious placenta previa with placenta accreta: J Interv Med, 2020; 3(1); 34-36
5. Jing L, Wei G, Mengfan S, Yanyan H, Effect of site of placentation on pregnancy outcomes in patients with placenta previa: PLoS One, 2018; 13(7); e0200252
6. Tsolakidis D, Zouzoulas D, Pados G, Pregnancy-related hysterectomy for peripartum hemorrhage: a literature narrative review of the diagnosis, management, and techniques: Biomed Res Int, 2021; 2021; 9958073
7. Kim ML, Hur YM, Ryu H, Clinical outcomes of prophylactic compression sutures for treatment of uterine atony during the cesarean delivery of twins: BMC Pregnancy Childbirth, 2020; 20(1); 40
8. Nalini N, Kumar A, Prasad MK, Obstetric and maternal outcomes after B-lynch compression sutures: A meta-analysis: Cureus, 2022; 14(11); e31306
9. Wu J, Guo R, Li L, Chu D, Wang X, Effectiveness and safety of prophylactic abdominal aortic balloon occlusion for patients with type III caesarean scar pregnancy: A prospective cohort study: BMC Pregnancy Childbirth, 2023; 23(1); 754
10. Zheng W, Dou R, Yan J, Intra-abdominal aortic balloon occlusion in the management of placenta percreta: Chin Med J (Engl), 2022; 135(4); 441-46
11. Xia L, Lin J, Dai Y, Wang X, Study on the application of King’s combined uterine suture for hemostasis during cesarean section: BMC Pregnancy Childbirth, 2021; 21(1); 762-68
12. American College of Obstetricians and Gynecologists; Society for Maternal-Fetal Medicine, Obstetric Care Consensus No. 7: Placenta Accreta Spectrum: Obstet Gynecol, 2018; 132(6); e259-e75
13. Wooldridge AL, Pasha M, Chitrakar P, Advanced maternal age impairs uterine artery adaptations to pregnancy in rats: Int J Mol Sci, 2022; 23(16); 9191-205
14. Pollheimer J, Vondra S, Baltayeva J, Regulation of placental extravillous trophoblasts by the maternal uterine environment: Front Immunol, 2018; 9; 2597
15. Morlando M, Collins S, Placenta accreta spectrum disorders: Challenges, risks, and management strategies: Int J Womens Health, 2020; 12; 1033-45
16. Arakaza A, Zou L, Zhu J, Placenta accreta spectrum diagnosis challenges and controversies in current obstetrics: A review: Int J Womens Health, 2023; 15; 635-54
17. Ananth CV, Lavery JA, Vintzileos AM, Severe placental abruption: Clinical definition and associations with maternal complications: Am J Obstet Gynecol, 2016; 214(2); 272e1-e9
18. Kuwabara M, Takahashi Y, Iwagaki S, Effectiveness of preventive B-lynch sutures in patients at a high risk of postpartum hemorrhage: J Obstet Gynaecol Res, 2022; 48(12); 3111-18
19. Wei J, Dai Y, Wang Z, Intrauterine double-balloon tamponade vs gauze packing in the management of placenta previa: A multicentre randomized controlled trial: Medicine (Baltimore), 2020; 99(7); e19221
20. Huo F, Liang H, Feng Y, Prophylactic temporary abdominal aortic balloon occlusion for patients with pernicious placenta previa: A retrospective study: BMC Anesthesiol, 2021; 21(1); 134
21. Yin H, Hu R, Outcomes of prophylactic abdominal aortic balloon occlusion in patients with placenta previa accreta: A propensity score matching analysis: BMC Pregnancy Childbirth, 2022; 22(1); 502
22. Chen WH, Huang KH, Kung FT, Effects of uterine artery occlusion during myomectomy on ovarian reserve: Serial follow-up of sex hormone levels, ultrasound parameters and Doppler characteristics: J Obstet Gynaecol Res, 2020; 46(5); 752-58
23. Fu M, Bu H, Fang Y, Parallel loop binding compression suture, a modified procedure for pernicious placenta previa complicated with placenta increta: Front Surg, 2021; 8; 786497
24. Mostfa AA, Zaitoun MM, Safety pin suture for management of atonic postpartum hemorrhage: ISRN Obstet Gynecol, 2012; 2012; 405795
25. Kwon YS, Cho YM, Im KS, Transient occlusion of uterine arteries in procedures with high risk of uterine bleeding: JSLS, 2019; 23(1); e201800072
Figures
Figure 1. The distended vessels on the surface of the uterus for placental implantation. The arrow points to distended vessels. Production software: Adobe Photoshop21.1.0.106.Figure 2. a) Ligation of parametrial blood vessels. b) Ligation of the communicating branch of the ovary. Production software: Adobe Photoshop21.1.0.106.Figure 3. Placental implantation penetrating the anterior wall of the uterus. The arrow points to placenta previa. Production software: Adobe Photoshop21.1.0.106.Figure 4. Uterine plastic surgery was performed to remove the penetrating part of the uterine wall and placenta, as the anterior wall of the uterus was weak and lost its normal shape. Production software: Adobe Photoshop21.1.0.106.Figure 5. Front view of longitudinal parallel compression suture of the anterior and posterior walls of the lower segment of the uterus. Production software: Adobe Photoshop21.1.0.106. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387