24 March 2025: Clinical Research
Impact of Cholecalciferol Supplementation on Radiotherapy Outcomes in Advanced Cervical Cancer
Dodi Suardi ABE 1, Raden Tina Dewi Judistiani AE 2*, Muhamad Rinaldi E 1, Nurvita Trianasari CD 3, Basuki Hidayat AC 4, Ronny Lesmana AE 5, Rudi Supriyadi AE 6, Syahrul Rauf ABE 7, Budi Setiabudiawan AE 8, Yudi Mulyana Hidayat AE 1, Aisyah Shofiatun Nisa AE 1
DOI: 10.12659/MSM.945964
Med Sci Monit 2025; 31:e945964






Abstract
BACKGROUND: Cervical cancer is the fourth most common cancer among women. The case fatality rate of advanced-stage cervical cancer was approximately 50% in 2020 worldwide. A new approach to finding a better treatment outcome for advanced-stage cervical cancer is needed. Research findings showed that cholecalciferol may benefit cancer cell control. This study aimed to understand the impact of cholecalciferol supplementation on advanced-stage cervical cancer treatment by radiotherapy.
MATERIAL AND METHODS: A randomized controlled trial with a pretest-posttest control group design was conducted between 2021 and 2023 at Dr. Hasan Sadikin Hospital, Bandung, Indonesia. Eligible consecutive patients were recruited and randomly assigned to either the Treatment or Control group using a simple randomization method. The Treatment group received 10 000 IU of cholecalciferol daily for 7 weeks during radiotherapy and for 12 weeks after treatment, while the Control group received a placebo in addition to the same radiotherapy protocol. Clinical outcomes were assessed 3 months after treatment completion.
RESULTS: We recruited 123 subjects in this study. The complete response rate was 82.61% in the Treatment group and 64.8% in the Control group. The Treatment group had a higher average serum cholecalciferol level after completion of the protocol.
CONCLUSIONS: Supplementation with 10 000 IU of cholecalciferol among advanced-stage cervical cancer patients undergoing radiotherapy treatment resulted in improved therapeutic response and maintaining serum cholecalciferol levels, which may further benefit cancer-free survival.
Keywords: Cervix Uteri, Cholecalciferol, Radiotherapy, Humans, Female, Uterine Cervical Neoplasms, Middle Aged, Dietary Supplements, Treatment Outcome, adult, Aged, Indonesia, Neoplasm Staging
Introduction
Cervical cancer is the fourth most frequent cancer among women worldwide. There were 604 127 cervical cancer cases and 341 831 deaths worldwide, and in Indonesia there were 36 633 new cases and 21 003 deaths [1]. Cervical cancer was the second most frequent cancer among females aged 15–44 in Indonesia. The 5-year incidence of cervical cancer in Indonesia was approximately at 92 930 cases, and the incidence rate was 68.43 per 100 000 [1]. There were 27 837 suspected cases and 3894 confirmed cases detected by cervical cancer screening from 2021 to 2023 in Indonesia [1].
Early-stage cervical cancer is preferably treated surgically, with advancing-stage radiation becoming the leading choice of treatment. Tissues that quickly grow are more susceptible to immediate radiation damage. Postoperative radiation can reduce local recurrence. Damage to adjacent healthy tissue depends on several factors [2,3].
Radiation induces cell death by causing DNA and cell membrane damage. Radiation energy is stored within the nucleus; free radicals break DNA chains, causing cells to lose their ability to reproduce. The damage caused by radiation may not be morphologically evident until several days or months later. In some cases, damaged cells can still divide to a limited extent [3].
Cholecalciferol in its active form, 1,25(OH)2D3, can increase the effectiveness of several conventional anti-cancer drugs, such as anti-metabolites and platinum-based drugs, and it can be used in combination. Cholecalciferol regulates the expression of molecules that inhibit proliferation, such as p21 and p27, and reduces the expression of hypoxia-induced oncogenic factor 1a (HIF1a) and c-Myc. Cholecalciferol influences tumor suppressor gene p53, decreasing the regulation of anti-apoptotic proteins (eg, Bcl-2 and Bcl-XL), enhancing the regulation of pro-apoptotic proteins (eg, BAX, BAK, and BAD), and recruiting Ca2+/calpain-dependent caspase and caspase 12 to regulate cancer cell growth [4].
Cholecalciferol also modulates the cancer microenvironment through molecular pathways for inflammatory signals and non-coding microRNA expression. Cholecalciferol supplementation not only enhances the effects of traditional cancer therapy but also confers resistance by regulating cancer stem cell growth and microRNA gene expression [5]. Cholecalciferol is involved in tumor metabolism, and it also has a primary role in regulating cell survival pathways like c-Myc, HIF1a, and p53.
Cholecalciferol enhances radiation sensitivity by inducing cell death via an autophagy process. Adjuvant cholecalciferol therapy elevates autophagy levels, decreasing cell reproduction capacity and promoting cell death. This transforms autophagy from cytoprotective to cytotoxic mode, enhancing radiation efficacy [2].
Various diagnostic methods can be utilized in the clinical setting to monitor clinical response regarding tumor size and expansion. Ultrasonography has gained significant attention as it does not require patient preparation, but compared to other techniques it is quicker, more cost-effective, and more widely available. Recent studies have demonstrated the high accuracy of ultrasonography in detecting tumors and assessing their size, stromal involvement, and parametrial infiltration. Transvaginal and transrectal ultrasonography has high sensitivity and specificity in stromal invasion depth evaluation, along with high specificity and moderate sensitivity for assessing involvement of the parametrium [6].
Animal studies show that cholecalciferol has a significant role in preventing breast cancer. Jacobson et al showed that a higher incidence of breast tumors occurred in mice with low cholecalciferol and calcium diet after exposure to carcinogen 7,12-dimethylbenzanthracene (DMBA). In organ culture of rat mammary glands, it reduced preneoplastic lesions induced by DMBA in initiation and promotion stages. This research suggests that cholecalciferol has a direct antineoplastic effect on mammary glands and that cholecalciferol signaling can prevent early and late tumorigenesis [7].
The active form of cholecalciferol, calcitriol, has extracellular functions, including anti-cancer activity. Supplementation with cholecalciferol is thought to enhance tumor suppressor genes and mechanisms of cancer cell death, potentially altering the outcomes of radiation therapy. The present study was based on findings of unpublished reports in our center, which observed changes in autophagy and mitochondrial biomarkers in patients with cervical cancer who received cholecalciferol while undergoing radiation therapy. Cholecalciferol increases radiation sensitivity through autophagy processes, inhibits cell proliferation, and promotes cell death.
This study aimed to determine whether vitamin D supplementation can improve therapeutic response in cervical cancer patients undergoing radiotherapy. To the best of our knowledge, this is one of the first studies to investigate this specific combination of high-dose cholecalciferol and radiotherapy in advanced-stage cervical cancer patients.
Material and Methods
STUDY DESIGN:
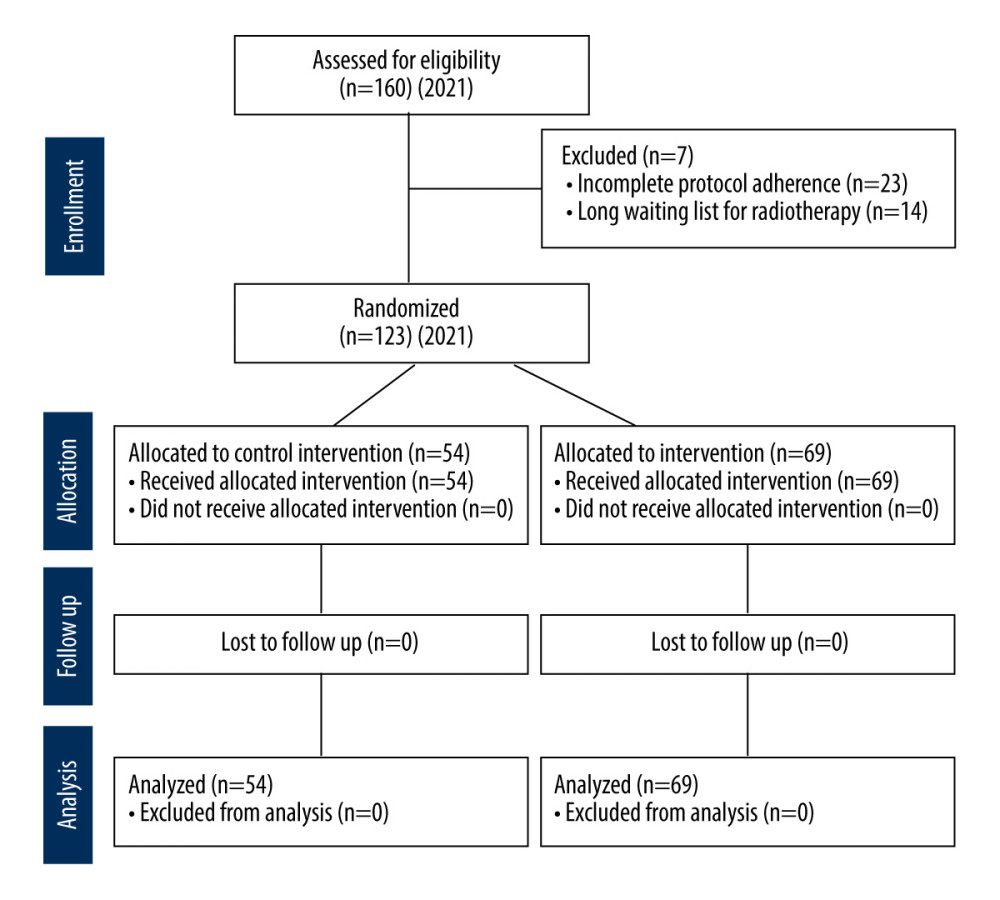
A randomized controlled trial with a pretest-posttest control group design was conducted between 2021 and 2023 at Dr. Hasan Sadikin Hospital in Bandung, Indonesia. Consecutive sampling was used to recruit eligible participants, who were then randomized into Intervention and Control groups to ensure balanced allocation. The study focused on advanced-stage cervical cancer patients (FIGO stages IIB–IVA) (Figure 1).
An oncologist performed a complete clinical examination, ultrasonography for staging, and histopathological assessment for a conclusive cervical cancer diagnosis. These evaluations were conducted before treatment and at follow-up.
The Treatment group received supplementation with 10 000 IU cholecalciferol daily for 7 weeks during radiotherapy and for 12 weeks during the post-treatment follow-up period. The Control group received a placebo in addition to the same radiotherapy protocol. Radiotherapy followed the hospital’s standardized treatment guidelines. Clinical outcomes were assessed 3 months after treatment completion.
PARTICIPANTS:
The target population was patients with confirmed advanced-stage cervical cancer who were eligible for radiotherapy. All subjects gave written consent to receive a complete internal and external radiotherapy course. Laboratory assessments included measurement of blood cholecalciferol level, and other parameters were assessed to ensure eligibility for the standard radiotherapy treatment protocol.
Sample calculation for the minimum required sample for multiple logistic regression was calculated, setting type I error of 5% (Zα=1.96) and type II error of 10% (Zβ=1.28). Odds ratio (OR) was set at 3.25. The minimum required sample size was 122 subjects. We recruited a minimum sample of 61 samples in both groups. To minimize potential bias and account for dropouts, an additional 20% was added to the calculated sample size.
VARIABLES, MEASUREMENTS, AND TREATMENT:
The independent variable was serum cholecalciferol level. The dependent variable was the clinical response of patients based on the RECIST criteria, which include complete and partial response and stable and progressive disease. The confounding factors were the subjects’ characteristics and the histopathological profiles of the cancer (squamous cell carcinoma, adenosquamous carcinoma, and other types).
Combined clinical and paraclinical assessments were used in diagnosing cervical cancer. Physical examinations included visual inspection of the cervix, vaginal walls, secretions, fornices, and bimanual examination to evaluate the uterine size, consistency, and position, as well as cervical consistency, parametrium condition, and adnexa status. Transrectal ultrasonography was performed to evaluate tumor size and extension. A tissue biopsy of the cervix was collected to determine the histopathological subtype of cervical cancer by pathologists. Serum cholecalciferol level was assessed using a competitive enzyme-linked immunosorbent assay (CLIA) kit for 25(OH)D (Euroimmune®).
After consecutive recruitment, the subjects were allocated to receive randomized envelopes containing either cholecalciferol or placebo. The pharmacist kept random allocations. The clinical responses were recorded by oncologists who were blinded to the allocation. Internal and external radiotherapy was conducted by a radiologist at the hospital. Cervical cancer radiotherapy was performed with 20–30 Gy internal radiation followed by external radiation of 40–50 Gy [8,9]. Therapeutic response monitoring was performed using transrectal ultrasonography and categorized based on RECIST criteria. After completion of follow-up, the randomization treatment and other follow-up data were revealed to the principal investigator.
VITAMIN D CATEGORIZATION:
Vitamin D levels were categorized as follows:
The categorization was based on established guidelines from the literature and was used to assess baseline vitamin D status [10].
STATISTICAL ANALYSIS:
Numerical data were assessed for normality before conducting statistical tests. The Shapiro-Wilk test was used for datasets with fewer than 50 observations, while the Kolmogorov-Smirnov test was applied for larger datasets. If the data were normally distributed, an independent t-test was used to compare the characteristics of the 2 study groups. If the data were not normally distributed, the Mann-Whitney U test was performed. Categorical data were analyzed using the chi-square test, provided no more than 20% of expected cell counts were below 5. For 2×2 tables, Fisher’s exact test was used, and for larger tables, the Kolmogorov-Smirnov test was applied.
To evaluate differences between the 2 groups before and after treatment, paired t-tests were used for normally distributed numerical data, and the Wilcoxon signed-rank test was used otherwise. For categorical data, McNemar’s test was employed for paired 2×2 tables, while the marginal homogeneity test was used for categories with more than 2 levels.
The obtained data were recorded in case report file forms. Data entry and analysis were processed using SPSS version 24.0 software for Windows. Data analysis was first conducted descriptively for dependent and independent variables. Then, serum cholesterol levels and clinical responses based on RECIST criteria in both groups were compared before and after completion of protocols. The results and the tests are displayed in Tables 1 and 2, and the following discussion.
ETHICS APPROVAL:
The research protocol subjects were presented in a full board meeting of the Research Ethics Committee of Universitas Padjajdjaran in accordance with International Conference on Harmonisation – Good Clinical Practice (ICH-GCP) guidelines (984/UN6.KEP/EC/2021).
Results
A total of 160 subjects were screened and recruited. However, 14 subjects were excluded prior to treatment due to the long waiting list for radiotherapy, and 23 subjects dropped out due to incomplete protocol adherence, leaving a total of 123 subjects for complete follow-up. The final sample included 69 subjects in the Treatment group and 54 in the Control group. The recruitment process was initiated at the onset of the COVID-19 pandemic in 2020, which introduced significant logistical and technical challenges. Further recruitment was not feasible due to time and financial constraints.
Statistical analysis showed that the subjects in both groups were comparable at baseline, with no significant differences in mean or median values of age, parity, initial tumor size, or histological type of cancer cells (Table 1). The average age was 49.93±8.66 years in the Control group and 50.38±9.18 years in the Treatment group. The parity was 3.07±1.34 versus 2.93±1.27, respectively. Most subjects in the Control group (81.5%) and Treatment group (79.7%) had squamous cell carcinoma (SCC), while 18.5% and 20.3% had adenosquamous carcinoma. The mean initial tumor size was 86.58±76.50 cm3 in the Control group and 109.19±106.62 cm3 in the Treatment group. These baseline characteristics are summarized in Table 1.
Significant differences were observed in serum cholecalciferol levels at the end of radiation treatment (Table 2). The Treatment group exhibited a post-radiation median cholecalciferol level of 38.09 ng/mL, compared to 6.86 ng/mL in the Control group (p<0.01). The change in cholecalciferol levels (delta) was also significantly higher in the Treatment group (24.51 ng/mL) compared to the Control group (−8.29 ng/mL, p<0.01).
Therapeutic response, based on RECIST criteria, showed a statistically significant difference between the 2 groups. The Treatment group had a complete response rate of 82.61% versus 64.81% in the Control group (p=0.021), with partial response rates of 17.39% and 35.19%, respectively (Table 2). No cases of stable or progressive disease were observed.
Tumor size reduction (delta) after radiotherapy was greater in the Treatment group (−60.96 cm3) compared to the Control group (−51.35 cm3), although the difference was not statistically significant (p=0.405, Table 2).
Discussion
This study demonstrated that high-dose vitamin D supplementation alongside radiotherapy significantly improved complete response rates in advanced cervical cancer patients, with 82.61% in the Treatment group compared to 64.81% in the Control group. The Treatment group also showed a substantial post-radiotherapy increase in serum cholecalciferol levels (median 38.09 ng/mL) compared to the Control group (median 6.86 ng/mL,
The study subjects’ average age was 49.93±8.7 years in the Control group and 50.38±9.2 years in the Treatment group, aligning with the reported age range for cervical cancer (from 44 years in Vanuatu to 68 years in Singapore), while the global average age at first diagnosis is 53 years [10]. In low human development index (HDI) countries, cervical cancer incidence rates can reach 100 per 100 000 women, rising from age 25, compared to approximately 20 per 100 000 in high HDI countries, where rates peak at age 40 [12]. Multiparity was common among the study subjects, and while research shows a correlation between high parity and cervical cancer, the mechanisms remain unclear, with hypotheses including cervical trauma from childbirth and hormonal changes during pregnancy [8,9]. The high burden of cervical cancer in developing countries stems from late-stage diagnosis, inadequate treatment, and socio-cultural barriers, contrasting with high-resource countries that demonstrate the effectiveness of early detection and screening programs, which remain underutilized in low HDI countries, reaching only 7% of the targeted 70% of at-risk women in 2023 [12].
The IVA test program in Indonesia continues to progress in expanding early detection of cervical cancer through community health centers, private clinics, and Posyandu, a community-based health program in Indonesia that provides services for mothers, infants, and toddlers. Despite these advancements, challenges persist, including unequal distribution of health workers, limiting access in certain areas, low public awareness coupled with stigma following test results, and insufficient continuous annual funding to increase coverage. Nonetheless, the government plays a crucial role in combating cervical cancer by integrating IVA testing into primary health services, training health workers, conducting educational campaigns, and enhancing access and affordability. Similarly, cholecalciferol deficiency remains a global health issue, affecting approximately 1 billion people worldwide. Defined as a serum 25-hydroxy cholecalciferol level below 20 ng/mL (<50 nmol/L) and insufficiency as 21–29 ng/mL (52–72 nmol/L), its prevalence varies across regions, influenced by factors such as sun exposure, weather, clothing habits, skin pigmentation, geography, altitude, supplementation, obesity, and air pollution. Although prevalent in both developing and developed nations, industrialization, lifestyle, and nutritional shifts have exacerbated this issue even in tropical countries [9].
A study by Emre et al showed that HPV-positive women had significantly lower cholecalciferol levels (8.29 IU/mL) compared to HPV-negative women (11.43 IU/mL), supported by findings that cervical cancer patients generally have lower cholecalciferol levels [6]. Cholecalciferol deficiency is associated with an increased risk of cervical intraepithelial neoplasia (CIN) and worse cancer outcomes [13]. Histologically, in the present study squamous cell carcinoma (SCC) was most common in the Control group (81.5%), while adenosquamous carcinoma (ASC) dominated the Treatment group (79.7%), with HPV16 primarily linked to SCC and HPV18 to ASC. Clear cell cervical carcinoma, with lower immune checkpoint protein expression, has worse survival rates and higher resistance to radiotherapy compared to HPV-related adenocarcinoma [8,14,15]. Given its role in modulating processes like cell proliferation, apoptosis, and immune response, addressing cholecalciferol deficiency is essential for improving cervical cancer outcomes [8,15].
The response to therapy in this study, based on RECIST criteria, showed that the Treatment group achieved 57 complete responses and 12 partial responses (a total of 82.61% complete responses). In comparison, the Control group had 36 complete responses and 19 partial responses (64.81% complete responses). The number of complete responses in the Control group is aligned with 2017 research by Winarto et al [16], which found a 68.29% complete response rate to radiotherapy in cervical cancer patients with stage IIA–IIIB. This indicates an increase in complete response among patients receiving radiotherapy with supplementation of cholecalciferol compared to those without supplementation of cholecalciferol, by 14.32% [8].
The research findings demonstrate that the initial tumor dimensions in the Control and Treatment group were 86.58±76.500 mm and 109.19±106.617 mm, respectively. Data sourced from the Cancer Registry by the Indonesian Society of Gynecology Oncology (INASGO) show the occurrence of cervical cancer prevalence cases at advanced stages, particularly in stages III and IV. The tumor measurements observed in this investigation are consistent with the FIGO 2018 classification for cervical cancer, indicating an advanced disease stage[13,17].
High-dose cholecalciferol (10 000 IU/day, totaling approximately 300 000 IU monthly) was well tolerated in our study, with no adverse effects observed. The literature supports this dosage’s safety in cancer settings and suggests that it can enhance treatment response by stabilizing serum levels within a safe range [17]. The total monthly dose of 300 000 IU of vitamin D was administered based on prior evidence supporting its safety and efficacy in clinical settings, with no significant adverse effects observed in this study cohort. High-dose vitamin D regimens have been shown to be generally well tolerated, although monitoring for potential hypercalcemia or kidney-related complications is recommended, as discussed in recent studies [18,19].
The analysis results indicate no significant age, parity, or tumor size differences between the Control and Treatment groups. This suggests that both groups had similar tumor sizes and patient profiles. The analysis revealed no significant differences in anatomical pathology results between the Control and Treatment groups.
Pre-radiation cholecalciferol levels in the 2 groups were 18.11±11.255 ng/mL and 16.31±8.127 ng/mL, indicating similar concentrations within the deficiency or insufficiency categories, as classified by Shim et al (<12 ng/mL for severe deficiency, 12–19 ng/mL for deficiency, 20–29 ng/mL for insufficiency, and ≥30 ng/mL for sufficiency) [10]. Research suggests cervical cancer patients tend to have lower cholecalciferol levels, and supplementation may reduce cancer-related mortality, although outcomes remain inconclusive. A study by Hosono (2010) indicated a potential reduced risk of cervical cancer with increased cholecalciferol intake, while phase II trials combining cholecalciferol with other anti-cancer agents, such as cyclophosphamide and curcumin, have shown efficacy in cervical and endometrial cancers, with manageable toxicity [16]. Vahedpoor et al demonstrated that long-term cholecalciferol supplementation significantly improved CIN1 regression rates (84.6% vs 53.8%, p=0.01), potentially through HPV clearance, but benefits were not observed in more advanced lesions like CIN2/3 [16,20].
Cholecalciferol supplementation helps mitigate radiotherapy-induced adverse effects, including vaginal toxicity symptoms such as lubrication loss, dyspareunia, and discharge, while enhancing epidermal cell differentiation and pro-inflammatory responses to reduce infection risks. Compared to the Control cohort, patients receiving cholecalciferol experienced fewer post-radiotherapy symptoms, such as uncontrollable bleeding (2.9% vs 35.2%) and discharge (36.2% vs 55.6%), with fewer other problems (4.4% vs 35.2%). Tumor size reduction was also greater in the treatment group (92.91 mm vs 71.99 mm). These findings highlight cholecalciferol’s role in improving radiotherapy outcomes and reducing related symptoms in cervical cancer patients [11,21].
Conclusions
This study showed that supplementation with 10 000 IU daily cholecalciferol in patients with advanced cervical cancer subjects’ stages IIB–IVA during a 7-week radiotherapy course, followed by 12 weeks after completion, resulted in better complete response. We suggest that the administration of 10 000 IU of cholecalciferol should be established as a daily treatment for cervical cancer patients undergoing radiotherapy.
Data Availability
The dataset used and/or analyzed during the current study is available from the corresponding author on reasonable request.
References
1. Seiwert TY, Salama JK, Vokes EE, The concurrent chemoradiation paradigm – general principles: Nat Clin Pract Oncol, 2007; 4(2); 86-100
2. Bhatla N, Aoki D, Sharma DN, Sankaranarayanan R, Cancer of the cervix uteri: 2021 update: Int J Gynaecol Obstet, 2021; 155(Suppl 1); 28-44
3. Chi D: Principles and practice of gynecologic oncology, 2024, Lippincott Williams & Wilkins
4. Jeon SM, Shin EA, Exploring vitamin D metabolism and function in cancer: Exp Mol Med, 2018; 50(4); 1-14
5. Negri M, Gentile A, de Angelis C, Vitamin D-induced molecular mechanisms to potentiate cancer therapy and to reverse drug-resistance in cancer cells: Nutrients, 2020; 12(6); 1798
6. Suardi D, The Comparison of 25-hydroxyvitamin D3 between patients with and without cervical cancer: Open Access Macedonian Journal of Medical Sciences, 2021; 9(B); 564-68
7. Welsh J, Vitamin D and breast cancer: Insights from animal models: Am J Clin Nutr, 2004; 80(6 Suppl); 1721S-24S
8. Bogdanova A, Andrawos C, Constantinou C, Cervical cancer, geographical inequalities, prevention and barriers in resource depleted countries: Oncol Lett, 2022; 23(4); 113
9. Tekalegn TY, Sahiledengle B, Woldeyohannes D, High parity is associated with increased risk of cervical cancer: Systematic review and meta-analysis of case-control studies: Womens Health (Lond), 2022; 18; 17455065221075904
10. Shim J, Pérez A, Symanski E, Nyitray AG, Association between serum 25-hydroxyvitamin D level and human papillomavirus cervicovaginal infection in women in the United States: J Infect Dis, 2016; 213(12); 1886-92
11. Vahedpoor Z, Mahmoodi S, Samimi M, Long-term vitamin D supplementation and the effects on recurrence and metabolic status of cervical intraepithelial neoplasia grade 2 or 3: A randomized, double-blind, placebo-controlled trial: Ann Nutr Metab, 2018; 72(2); 151-60
12. Arbyn M, Weiderpass E, Bruni L, Estimates of incidence and mortality of cervical cancer in 2018: A worldwide analysis: Lancet Glob Health, 2020; 8(2); e191-e203 [Erratum in: Lancet Glob Health. 2022;10(1):e41]
13. Hilger J, Friedel A, Herr R, A systematic review of vitamin D status in populations worldwide: Br J Nutr, 2014; 111(1); 23-45
14. Feldman D, Krishnan AV, Swami S, The role of vitamin D in reducing cancer risk and progression: Nat Rev Cancer, 2014; 14(5); 342-57
15. Burger EA, de Kok IMCM, Groene E, Estimating the natural history of cervical carcinogenesis using simulation models: A CISNET comparative analysis: J Natl Cancer Inst, 2020; 112(9); 955-63
16. Winarto H, Rahakbauw E, Supriana N, Radiotherapy response of cervical cancer patients at a tertiary referral hospital in Indonesia: Indonesian Journal of Obstetrics and Gynecology, 2017; 230-35
17. Stolnicu S, Karpathiou G, Guerra E, Clear Cell Carcinoma (CCC) of the cervix is a Human Papillomavirus (HPV)-independent tumor associated with poor outcome: A comprehensive analysis of 58 cases: Am J Surg Pathol, 2022; 46(6); 765-73
18. Yilmaz R, Efficacy and safety of single or consecutive double high-dose oral cholecalciferol supplementation in adult patients with vitamin D deficiency: Steroids, 2023; 194; 109308
19. Scragg R, Khaw KT, Toop L, Monthly high-dose vitamin D supplementation and cancer risk: A post hoc analysis of the vitamin D assessment randomized clinical trial: JAMA Oncol, 2018; 4(11); e182178
20. Hosono S, Matsuo K, Kajiyama H, Association between dietary calcium and vitamin D intake and cervical carcinogenesis among Japanese women: Eur J Clin Nutr, 2010; 64(4); 400-9
21. Momenimovahed Z, Tiznobaik A, Taheri S, Salehiniya H, Ovarian cancer in the world: epidemiology and risk factors: Int J Womens Health, 2019; 11; 287-99
Tables
 Table 1. Study patient characteristics.
Table 1. Study patient characteristics. Table 2. Comparison of tumor size and response to pre- and post-radiation therapy in the Control and Treatment groups.Table 1. Study patient characteristics.Table 2. Comparison of tumor size and response to pre- and post-radiation therapy in the Control and Treatment groups.
Table 2. Comparison of tumor size and response to pre- and post-radiation therapy in the Control and Treatment groups.Table 1. Study patient characteristics.Table 2. Comparison of tumor size and response to pre- and post-radiation therapy in the Control and Treatment groups. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387