13 April 2025: Review Articles
Inclisiran in Cardiovascular Health: A Review of Mechanisms, Efficacy, and Future Prospects
Fanke Huang ABCDEFG 1, Qiuting Dai FG 1, Yilu Zhou F 1, Jing Guan F 1, Jingjing Wu F 1, Yanyan Dong F 1, Jianfeng Lv AG 1*
DOI: 10.12659/MSM.946439
Med Sci Monit 2025; 31:e946439






Abstract
ABSTRACT: Dyslipidemia is a significant risk factor for cardiovascular disease, and managing low-density lipoprotein cholesterol levels is a crucial strategy for both the prevention and treatment of cardiovascular disease. The active ingredient in the novel lipid-lowering drug, inclisiran, is a new type of small interfering RNA that primarily regulates blood lipid levels by inhibiting the synthesis of proprotein convertase subtilisin type 9 (PCSK9). Enhanced lipid-lowering effects can be achieved following 3 administrations. This article summarizes inclisiran’s mechanism of action, efficacy, safety, current research hotspots, clinical applications, and future development prospects, based on the latest literature and research advancements. Through comparative analysis with traditional lipid-lowering drugs, we conclude that inclisiran has promising application prospects and market potential, as it can complement traditional statin therapies to enhance lipid-lowering efficiency. This not only provides convenience to patients but also improves treatment compliance. Its safety profile alleviates patients’ concerns and mitigates the impact of negative emotions on their condition. Additionally, the potential applications of inclisiran in oncology have been identified. However, inclisiran also presents certain limitations and challenges. For instance, its long-term safety and efficacy require further investigation in future studies, and its high cost can restrict its widespread adoption and promotion. Furthermore, additional clinical evidence is needed to evaluate its synergistic or antagonistic effects when used in conjunction with other medications.
Keywords: PCSK9 Inhibitors, Hyperlipidemia, Familial Combined, Clinical Trial, Humans, Cardiovascular Diseases, RNA, Small Interfering, Proprotein Convertase 9, dyslipidemias, Cholesterol, LDL, Hypolipidemic Agents
Introduction
Data from the Global Burden of Disease Database (GBD) in 2019 indicate that 61% of cardiovascular disease (CVD) is attributable to atherosclerotic cardiovascular disease (ASCVD), with dyslipidemia identified as the second leading risk factor for ASCVD [1]. From a large number of clinical studies, genetic tests, and epidemiological investigations, it has been concluded that the main factor contributing to these risks is elevated levels of cholesterol in the body. Hypercholesterolemia induces alterations in arterial endothelial permeability, facilitating the migration of low-density lipoprotein cholesterol (LDL-C) into the arterial wall. Within the arterial wall, LDL-C binds to the low-density lipoprotein receptor (LDLR), resulting in its absorption and retention. Subsequently, LDL-C undergoes oxidation and is modified into apolipoprotein B, which is then recognized by scavenger receptors on macrophages. This recognition prompts endocytosis, leading to the transformation of macrophages into foam cells. Foam cells initiate inflammatory responses through the secretion of various cytokines. In response, smooth muscle cells in the arterial intima proliferate and produce collagen, contributing to coronary arteriosclerosis and cardiovascular disease [2]. As LDL-C is the primary target for blood lipid intervention, further research and discussion are needed to determine how to effectively control blood lipids within a specified target range based on ASCVD risk stratification. How to keep cholesterol in the required range is particularly important for the primary and secondary prevention of cardiovascular events in patients with dyslipidemia, especially hypercholesterolemia [3,4].
Currently, statins, the most commonly used medications for lowering cholesterol, have been shown to significantly reduce the risk of ASCVD events and reduce LDL-C levels by an average of 27% in studies [5]. Numerous meta-analyses of clinical studies have shown that in order to reduce the risk of CVD, LDL-C levels should be controlled as low as possible and that there is no lower limit to this level [6]. Other adjunctive therapeutic options are needed for patients who cannot achieve LDL-C control or who cannot tolerate statins. As an effective target for reducing LDL-C, protein convertase subtilisin/kexin type 9 (PCSK9) indirectly influences plasma LDL levels primarily by regulating the expression of LDLR on the cytoplasmic membrane [7,8]. Consequently, blocking the binding of PCSK9 to LDLR is crucial for controlling LDL-C levels. Current research and development of therapeutic agents primarily focus on small interfering RNA (siRNA) and monoclonal antibodies. Monoclonal antibodies are proteins that bind to PCSK9, thereby reducing serum LDL levels by inhibiting the interaction between PCSK9 and LDLR [9]. A notable example of this class of drugs is evolocumab, which has been shown to significantly decrease LDL-C levels and the incidence of adverse cardiovascular events in patients with dyslipidemia [10,11]. However, the requirement for frequent administration poses challenges to patient treatment compliance. Moreover, its suboptimal performance, high cost, and limited applicability in certain patient populations have restricted its use in clinical lipid-lowering treatment. In contrast, siRNA targets the expression of the PCSK9 gene in liver cells, inhibiting the secretion of PCSK9 and thereby reducing LDL-C levels [12,13]. Nevertheless, as an emerging lipid-lowering therapy, siRNA treatment requires further clinical trial data to establish its long-term safety, efficacy, applicability, and potential adverse reactions.
Inclisiran represents a pioneering siRNA-based therapy primarily used for the adjuvant treatment of individuals with primary hypercholesterolemia or mixed dyslipidemia. Currently, the ORION clinical trial, which is being conducted across multiple countries, is assessing the long-term safety and efficacy of inclisiran, including its use in adolescent patients with familial hypercholesterolemia (FH) and other special populations. In this article, we aim to review inclisiran with respect to its mechanism of action, safety profile, adverse reactions, applicability, and long-term efficacy. This article analyzes the advantages and disadvantages of inclisiran over conventional lipid-lowering therapies, and describes its clinical pharmacodynamics and benefit-risk assessment based on evidence-based evidence in order to provide guidance to clinicians and clinical pharmacists in formulating an optimal lipid-lowering regimen. A comprehensive summary of the research on inclisiran is presented, identifying future potential and current constraints that need to be overcome.
Inclisiran Mechanism of Action
siRNA interferes with the expression of specific genes that possess complementary nucleotide sequences by promoting the degradation of post-transcriptional mRNA, thereby preventing translation [14]. Research indicates that inclisiran, a long-acting synthetic siRNA, selectively targets PCSK9. Upon entering the bloodstream, it first binds specifically to N-acetylgalactosamine and the asialoglycoprotein receptor on the liver cell membrane, facilitating its entry into liver cells. Subsequently, inclisiran associates with the RNA-induced silencing complex and binds to the mRNA encoding the PCSK9 protein, mediated by the antisense strand, thus inhibiting the production of PCSK9 protein. PCSK9 is a protein that regulates the expression of LDLR on the surface of hepatocytes [15–18]. Consequently, inclisiran’s inhibition of PCSK9 indirectly enhances the expression of LDLR, resulting in a hypolipidemic effect. The current proposed mechanism of action of inclisiran in treating hyperlipidemia is illustrated in Figure 1.
Analysis of Current Hot Keywords Related to Inclisiran
Keyword co-occurrence analysis, after consolidating synonyms, used the VOSviewer tool to summarize 1,194 key terms. Subsequently, a statistical analysis of the frequency of these key terms was conducted, and a keyword co-occurrence network was constructed based on VOSviewer. From the high-frequency keywords ranked in the top 22 (Table 1) and the keyword co-occurrence network (Figure 2), it is evident that besides the search term, efficacy, PCSK9, safety, and risk are the most frequently occurring keywords. The efficacy, safety, and risk of inclisiran in patients with hypercholesterolemia are currently the most prominent topics within this domain. This suggests that ongoing research related to inclisiran primarily focuses on clinical trials, with FH and ASCVD patients being the primary beneficiaries of inclisiran studies. Controlling lipid levels is a fundamental objective of inclisiran research. Double-blind clinical trials remain the most widely used research method in this field, and comparative studies between inclisiran and the traditional lipid-lowering therapy, evolocumab, also garner significant attention.
Summary of Clinical Studies of Inclisiran
EFFICACY:
Dose-response effects were evaluated in multiple phase I/II clinical studies, demonstrating that PCSK9 and LDL-C levels improved in patients treated with inclisiran at various doses. In the multi-ascending dose clinical study ORION-1, it was observed that patients receiving 300 mg of inclisiran sodium at baseline and again at 90 days, followed by injections every 180 days, achieved the most significant LDL-C reduction, with a decrease of 48% to 51% [19,20].
SAFETY AND TOLERABILITY:
Inclisiran is a highly specific protein that effectively targets the reduction of LDL-C, significantly minimizing off-target effects and not producing any obvious adverse reactions [21]. In an analysis of 3 clinical studies, 77.3% of patients in the control group and 78.0% of patients in the inclisiran treatment group experienced at least 1 treatment-related adverse event. Serious adverse events occurred in 23% of patients in the control group and 20.4% of patients in the inclisiran treatment group. The adverse events more commonly observed in the inclisiran group included nasopharyngitis, arthralgia, back pain, urinary tract infection, diarrhea, bronchitis, and injection site reactions. The incidence rates of injection site reactions were 1.8% in the control group and 8.2% in the inclisiran treatment group. Local injection site reactions were the predominant type, all of which were mild to moderate and had no lasting effects [22]. There was no significant difference in the incidence of adverse events between the inclisiran and control groups across all age categories. However, the elderly population constituted the majority of adverse events in both groups. The recent ORION-13 and ORION-16 studies included 162 adolescent patients with FH (12 heterozygous FH [HeFH] patients in the ORION-13 study and 150 HoFH patients in the ORION-16 study). The results of these relevant studies have not yet been published. Should these results demonstrate good safety and tolerability, they may further support the safety profile of inclisiran in the adolescent population, addressing existing research gaps [23].
LONG-TERM SAFETY:
The ORION-8 study serves as a continuation of the long-term efficacy and tolerability follow-up for patients involved in the phase II (ORION-3) and phase III (ORION-9, ORION-10, and ORION-11) inclisiran lipid-lowering trials. Among these patients, the mean exposure to inclisiran, including the parent trials, was 3.7 years, with a maximum exposure of 6.8 years. The mean percentage change in LDL-C levels was −49.4% (95% CI: −50.4, −48.3). The incidence of injection site adverse events during treatment was reported at 5.9%, all classified as mild to moderate, and the proportion of patients with inclisiran-related anti-drug antibodies was 5.5% [24]. These results indicate that inclisiran can maintain good efficacy, tolerability, and safety during long-term lipid-lowering treatment in patients.
SAFETY IN PATIENTS WITH COMORBIDITIES:
The lipid-lowering effect of inclisiran is also applicable to patients with diabetes with poor blood lipid control, with the incidence of adverse events being generally similar between diabetic and non-diabetic groups [25]. The ORION-6 trial evaluated the safety of inclisiran in patients with hyperlipidemia across varying degrees of liver impairment (Child-Pugh grades). This study recruited 28 patients, of whom 12 (42.9%) experienced a total of 36 adverse events: 1 patient with normal liver function (8.3%); 8 patients with mild liver function impairment (80.0%); and 3 patients with moderate liver function impairment (50.0%). The primary adverse event reported was cough. Inclisiran was found to be safe and tolerable in patients with mild to moderate hepatic impairment. This study indicates that the lipid-lowering efficacy of inclisiran is not adversely affected by liver function impairment, and there is no need for dosage adjustment in patients with mild or moderate liver damage [26]. This finding provides valuable guidance for formulating inclisiran treatment dosages in patients with liver function impairment. However, data on patients with severe liver function impairment are lacking, suggesting that future studies may address this gap. The ORION-7 phase I and ORION-1 phase II studies assessed the pharmacodynamic properties of inclisiran in patients with renal impairment. In the ORION-7 study, inclisiran demonstrated similar lipid-lowering effects across patients with mild, moderate, and severe renal impairment, with drug concentrations completely eliminated 48 h after administration in all groups. In the ORION-1 study, the efficacy of inclisiran on blood lipids and PCSK9 was found to be independent of renal function impairment. The incidence of adverse events among patients with mild to moderate renal impairment in the 2 studies was generally comparable, and the occurrence of injection site adverse reactions was low. These studies confirmed that the efficacy of inclisiran remains unaffected by renal function impairment, demonstrating strong safety and tolerability in patients with mild to moderate renal impairment [27]. However, for patients with severe renal impairment, the limited sample size precludes drawing any definitive conclusions.
SAFETY IN SWITCHING THERAPY:
ORION-3 is a 4-year open-label extension study based on the phase II ORION-1 trial. The inclisiran group will continue to receive 2 injections (284 mg inclisiran subcutaneous injection) annually. The switching treatment group will receive treatment every 2 months during the first year, followed by 2 injections (284 mg inclisiran subcutaneous injection) annually for the subsequent 3 years. Among the participants, 233 patients (80%) in the inclisiran-only group and 80 patients (87%) in the switch group completed the full 4-year observation period. During long-term treatment, the reduction rates of LDL-C concentration and PCSK9 levels in both patient groups were generally similar, with a relatively stable maintenance status. Regarding the incidence of adverse events, the rate of serious adverse events in the inclisiran treatment group was 37%, primarily due to nasopharyngitis, while the conversion group reported a rate of 34%, mainly associated with hypertension [28]. This study demonstrates that patients switching to inclisiran and continuing treatment in clinical practice have not experienced any negative effects on drug efficacy or safety.
In comparison to traditional lipid-lowering medications, inclisiran demonstrates superior safety and tolerability, eliminating the necessity for dose adjustments in patients with specific complications, such as those with liver and kidney impairments. Furthermore, during the clinical treatment process, adjusting the treatment plan to include inclisiran does not exacerbate the patient’s disease burden.
DRUG COMBINATION APPLICATION:
The 2023 version of the Chinese blood lipid management guidelines emphasizes that the decision to initiate drug combination therapy in clinical practice generally depends on the type of dyslipidemia, as well as the baseline levels and target values to be achieved. Statins remain a primary class of lipid-lowering medications. For patients whose lipid levels do not reach the target despite the use of moderate-intensity statins, the addition of cholesterol absorption inhibitors or PCSK9 inhibitors can be considered [29]. Furthermore, the 2023 American Heart Association/American College of Cardiology guidelines for chronic coronary artery disease have classified inclisiran as a level 2b recommendation for use alongside statins when ezetimibe and PCSK9 monoclonal antibodies are not tolerated as complementary treatments [30]. The recent ORION-10 and ORION-11 studies recruited 1561 and 1617 patients with ASCVD or ASCVD risk equivalents, respectively. All patients were treated with the maximum tolerated doses of statins and cholesterol absorption inhibitors. Despite these treatments, LDL-C levels remained challenging to control. Following grouping, patients received either inclisiran (284 mg) or a placebo. In the ORION-10 study, inclisiran resulted in a 52.3% reduction in LDL-C levels by day 510, while in ORION-11, a 49.9% reduction was observed. The adverse event profile for patients treated with inclisiran was comparable to that of the placebo group, with between-group differences of 1.7% in the ORION-10 trial and 4.2% in the ORION-11 trial. Although injection site reactions were more prevalent in the inclisiran group than in the placebo group, these reactions were generally mild to moderate and did not necessitate intervention. Importantly, both trials reported no significant differences in the occurrence of serious adverse events between the treatment groups [31]. These 2 studies demonstrate that patients receiving adjuvant treatment with inclisiran, in conjunction with statin therapy and a cholesterol absorption inhibitor, can achieve greater lipid-lowering efficacy without increasing the risk of adverse events. Consequently, when a patient’s blood lipid levels do not reach the target after using the maximum tolerated dose of statin therapy, or when treatment outcomes are suboptimal due to poor compliance or other factors, inclisiran can serve as an effective adjunct for enhanced lipid lowering [32].
ADVERSE CARDIOVASCULAR EVENTS:
Based on 3 phase III clinical trials (ORION-9, ORION-10, and ORION-11), a total of 3655 individual participants (inclisiran [n=1833]; placebo [n=1822]) at high risk for cardiovascular events were included. The data were analyzed to assess the relationship between inclisiran and the risk of adverse cardiovascular events. The occurrence of major adverse cardiovascular events (MACE), as well as fatal and nonfatal myocardial infarction and fatal and nonfatal stroke, was reported. The results indicated that the inclisiran group experienced significantly fewer MACEs than the placebo group (131 cases vs 172 cases) [33]. At Day 540, Kaplan-Meier estimates indicated the rates of MACEs, fatal and nonfatal myocardial infarction, and fatal and nonfatal stroke were 7.4% vs 9.5% and 1.9% vs 2% for the inclisiran and placebo treatment groups, respectively. The rates for fatal and nonfatal stroke were 3% and 0.7% vs 0.9%. Cox proportional hazards regression analysis revealed that inclisiran, compared with placebo, had hazard ratios of 0.75 (95% CI: 0.60, 0.94) for MACEs, 0.81 (95% CI: 0.51, 1.29) for fatal and nonfatal myocardial infarction, and 0.81 (95% CI: 0.51, 1.29) for death. The hazard ratio for fatal and nonfatal stroke was 0.80 (95% CI: 0.39, 1.67). These findings confirm that early treatment with inclisiran can significantly reduce the incidence of MACE in patients at high risk for cardiovascular events, thereby enhancing patient prognosis and quality of life. However, the duration of outcome observation is limited, and further long-term clinical observational research is necessary for supplementary verification of MACE outcomes.
POPULATION STUDIES IN INCLISIRAN:
According to the high-frequency keyword table and keyword time series analysis chart, prior to 2020 (Figures 2, 3), research on inclisiran predominantly focused on verifying its efficacy and safety. After 2020, the research objectives have gradually become more refined, indicating that the overall effectiveness and safety of the drug have been largely established. The current and future trend is expected to involve more personalized group studies on patients, including evaluations of inclisiran across different races or demographic groups. The ORION-15 study specifically assessed the efficacy, safety, and pharmacokinetics of inclisiran in Japanese patients with high-risk cardiovascular disease and elevated LDL-C levels. The results indicated that over 86% of patients treated with inclisiran achieved the lipid management goals established by the Japanese Atherosclerosis Society in 2017 [34]. In terms of pharmacokinetics, inclisiran was undetectable in plasma after 48 h across all doses. Its safety profile aligns with findings from long-term global studies of inclisiran [19]. Additionally, ORION-18 represents the first phase III double-blind trial conducted in China, primarily evaluating the efficacy and safety of inclisiran in patients with ASCVD or those at high risk for ASCVD. Therefore, inclisiran is demonstrated to be safe and effective in Asian patients with ASCVD or high-risk ASCVD [35]. Future research will further validate the conclusions drawn from studies involving diverse patient groups.
Evidence from epidemiological, genetic, and clinical studies indicates that LDL-C is a significant risk factor for ASCVD. Specifically, for every 1 mmol/L decrease in LDL-C, the incidence of ASCVD events is reduced by 20% to 23%. Furthermore, data indicate that since the 20th century, the overall mortality rate from coronary heart disease in the United States has exhibited a downward trend, with risk factor control contributing 44% and reductions in total cholesterol accounting for 24% of this decline. Consequently, most countries and regions consider patients with hypercholesterolemia as the primary treatment target among those with dyslipidemia [29]. The study of inclisiran in patients with homozygous familial hypercholesterolemia (HoFH), known as the ORION-2 study, demonstrated that when combined with statins and ezetimibe, inclisiran effectively reduces LDL-C levels in HoFH patients [36]. The ORION-9 study involved 482 adults with HeFH and found that inclisiran significantly reduced LDL-C levels in patients across all HeFH genotypes. The incidence of adverse events was comparable between the 2 groups, suggesting that inclisiran offers a safe and effective treatment option for patients with hypercholesterolemia [37].
APPLICATION IN THE ONCOLOGY FIELD:
PCSK9 inhibitors and PCSK9 siRNA have been extensively investigated in the context of cancer research. Several studies indicate that PCSK9 is highly expressed in various tumor tissues [38]. The overexpression of PCSK9 can influence epithelial-mesenchymal transition and phosphatidylinositol 3-kinase signaling in tumor cells [39]. The kinase/protein kinase B signaling pathway is known to enhance the proliferation, migration, and invasion of tumor cells [40]. Additionally, PCSK9 siRNA has been shown to promote apoptosis in tumor cells via mitochondrial and endoplasmic reticulum pathways. In vitro experiments further demonstrate that PCSK9 siRNA can protect prostate cancer cells from radiation-induced damage by inhibiting apoptosis, suggesting that inclisiran has potential applications in cancer treatment [41].
Discussion
Inclisiran is a promising siRNA that inhibits the production of PCSK9 in liver cells, resulting in reduced degradation of low-density LDLR and thereby lowering LDL-C levels. It requires only 2 to 3 injections per year [42]. In the United States, inclisiran is FDA-approved as an adjunct to the highest tolerated statin therapy, with or without additional lipid-lowering treatments, for patients who are statin intolerant or contraindicated for statin use. When combined with lipid-lowering therapy, LDL-C levels can be reduced by 44% to 54% in patients with ASCVD or those at high risk of developing hypercholesterolemia [43–45]. Inclisiran is recommended for secondary prevention in patients with ACVD who are statin intolerant or require additional LDL-C lowering [46]. However, ezetimibe remains a more suitable option for primary prevention of ASCVD and for patients needing to reduce residual LDL-C levels, due to its lower cost and potential to improve cardiovascular outcomes [47]. Inclisiran has demonstrated efficacy in treating individuals at high risk for ASCVD as well as those with HeFH [48]. Strict management of patients’ blood lipid levels has significantly decreased the risk of cardiovascular events, alleviated economic burdens, and improved the overall quality of life for patients [49]. For patients with diabetes and mild hepatic hyperlipidemia who also present with renal impairment, the treatment dose and individualized regimen for inclisiran do not require modification. While the reduction in PCSK9 and LDL-C levels in patients with moderate liver damage is somewhat less pronounced than in those with normal or mild liver damage, this variance does not necessitate an adjustment in the treatment dosage. Some studies indicate that the long-term use of statin lipid-lowering agents can pose potential risks for liver function impairment and can lead to negative emotional outcomes, such as anxiety and depression, which significantly reduce treatment compliance [50]. In severe cases, sleep quality can also be adversely affected. Furthermore, chronic mood disorders and lifestyle disturbances can negatively impact the recovery of patients from physical ailments [51]. In contrast to traditional statin lipid-lowering drugs, inclisiran exerts a reduced burden on liver and kidney function [52]. However, research has yet to confirm whether it can indirectly enhance treatment outcomes by alleviating patients’ concerns and mitigating negative emotions. Although inclisiran demonstrates a weaker capacity to lower LDL-C than do PCSK9 monoclonal antibodies, its biannual dosing schedule is significantly less frequent than the bi-monthly regimen of monoclonal antibodies, making it more acceptable to patients [53]. Frequent administration of monoclonal antibodies and the prevalence of injection site adverse reactions have imposed a significant psychological burden on patients undergoing long-term treatment. A survey on the use of PCSK9 monoclonal antibodies indicated that 33.7% of patients discontinue treatment due to its high cost [54]. In contrast, the targeted specificity of inclisiran results in minimal efficacy variation among individuals, while its lipid-lowering effect is long-lasting and stable. Additionally, its method of administration is more convenient, mitigating fluctuations in patients’ blood lipid levels caused by various factors. This reduction in fluctuations lowers the risk of ASCVD and enhances patients’ prognosis and quality of life. Inclisiran is also characterized by good safety and tolerability [55]. Multiple clinical trials have established that inclisiran presents a low risk of adverse events, primarily limited to injection site reactions. To date, no serious adverse events have been reported [56,57].
Regarding the long-term effectiveness, safety, and cardiovascular outcomes of inclisiran, the earliest cohort of subjects has been monitored for approximately 8 years. Further and longer-term follow-up studies are necessary to evaluate its impact on the prevention and treatment of cardiovascular diseases. Additionally, the molecular mechanisms and pathways through which inclisiran-mediated reduction of LDL-C exerts cardiovascular protective effects remain to be elucidated. The development of new siRNA drugs targeting other lipid metabolism or cardiovascular disease-related genes may offer opportunities for personalized and precision medicine. The highly controlled nature of clinical trials often fails to reflect the complexities and diversity present in clinical practice. For instance, the populations included in current clinical trials predominantly consist of white males, highlighting the need for more comprehensive research to confirm the long-term efficacy and safety of inclisiran across various racial, ethnic, and social groups. Previous studies have demonstrated that lower LDL-C levels can significantly reduce the risk of cardiovascular events and mortality in patients with dyslipidemia [58,59]. The latest blood lipid management guidelines propose more stringent requirements for blood lipid control. While it is essential to maintain low blood lipid levels, it is equally important to avoid significant fluctuations in these levels. This indicates that the advantages of long-term, stable blood lipid control far outweigh those of short-term, fluctuating control [6]. Consequently, future research should prioritize the long-term efficacy, safety, and cardiovascular outcomes associated with inclisiran. Ongoing studies such as ORION-4, ORION-1, and ORION-2 aim to establish the long-term safety of inclisiran in patients who are at high cardiovascular risk and have elevated LDL-C. The results of the ORION-4 study are not anticipated to be announced until 2026, and its primary endpoint is the incidence of MACEs. In the ORION 9, 10, and 11 clinical studies, research conducted by Ray et al indicated that inclisiran significantly reduced the prevalence of MACEs; however, the effect of inclisiran on MACE reduction remains uncertain [60].
According to a survey report on dyslipidemia in Chinese adults, the overall prevalence of dyslipidemia among adults is as high as 35.6%, while the lipid-lowering treatment coverage rate for patients at high-risk for ASCVD is only 5.5%, and the LDL-C target achievement rate stands at just 25.5%. Dyslipidemia has become a significant threat to public health [61]. The low treatment coverage can be attributed primarily to issues related to treatment cost, convenience, and efficacy, which directly impact patient compliance. Addressing these concerns by providing cost-effective solutions, enhancing treatment accessibility, and reducing economic burdens can significantly improve patient adherence. The development of inclisiran aims to address the limitations of traditional lipid-lowering drugs. However, reducing production costs and improving manufacturing efficiency remain key challenges for developers. Currently, the price of inclisiran in the United States (2023) is $3,290.63 per dose, with actual patient expenses varying based on insurance type and coverage. Notably, inclisiran is not covered by insurance in China, further exacerbating the financial burden on patients. Despite its potential for improved therapeutic benefits and prognostic outcomes, the high cost of treatment remains a deterrent. If production costs can be reduced, inclisiran may gain wider acceptance and potentially become a first-line lipid-lowering therapy [62], offering promising prospects for effective management of dyslipidemia [63].
Angiopoietin-like 3 (ANGPTL3) and PCSK9 are prominent targets in contemporary lipid-lowering research. Zodasiran (Levodasilan), a novel drug with significant potential for targeting ANGPTL3, represents the siRNA lipid-lowering therapeutic drug, following inclisiran, specifically targeting ANGPTL3 in the liver. The clinical development of zodasiran has advanced to phase II trials, focusing on mixed hyperlipidemia and exploring its effects on ANGPTL3 deficiency and the risk of hepatic steatosis [64]. The emergence of siRNA-based lipid-lowering drugs signifies a new era in lipid management, transitioning therapy into the realm of RNA therapeutics. Additionally, this approach holds untapped potential in other fields, such as cancer therapy, which is anticipated to be further validated through ongoing and future studies.
Conclusions
In conclusion, inclisiran, as a promising new lipid-lowering agent, will provide a new optimal therapeutic strategy for patients with hyperlipidemia, as the lipid-lowering study of inclisiran continues to improve.
Figures
 Figure 1. Inclisiran mechanism of action within hepatocytes (BioRender, version 2024, Science Suite Inc).
Figure 1. Inclisiran mechanism of action within hepatocytes (BioRender, version 2024, Science Suite Inc).  Figure 2. Inclisiran co-occurrence diagram of keywords in the Web of Science coreconcentr (VOSviewer, version 1.6.20, The Centre for Science and Technology Studies, CWTS).
Figure 2. Inclisiran co-occurrence diagram of keywords in the Web of Science coreconcentr (VOSviewer, version 1.6.20, The Centre for Science and Technology Studies, CWTS).  Figure 3. Inclisiran time sequence map of keywords in the research field (CiteSpace, version 6.2.4, University of Redsell University, USA).
Figure 3. Inclisiran time sequence map of keywords in the research field (CiteSpace, version 6.2.4, University of Redsell University, USA). References
1. , China Cardiovascular Health and Disease Report 2022%J: Chinese Journal of Cardiovascular Medicine, 2023; 28(04); 297-312
2. Goldstein JL, Brown MS, A century of cholesterol and coronaries: From plaques to genes to statins: Cell, 2015; 161(1); 161-72
3. Wang Z, Guo Y, Chinese guidelines for blood lipid management (basic edition 2024): Chinese Circulation Journal, 2024; 39(04); 313-21
4. Ikezaki H, Lim E, Cupples LA, Small dense low-density lipoprotein cholesterol is the most atherogenic lipoprotein parameter in the prospective Framingham offspring study: J Am Heart Assoc, 2021; 10(5); e019140
5. Abul-Husn NS, Manickam K, Jones LK, Genetic identification of familial hypercholesterolemia within a single U.S. health care system: Science, 2016; 354(6319); aaf7000
6. Mach F, Baigent C, Catapano ALESC Scientific Document Group, 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk: Eur Heart J, 2020; 41(1); 111-88 Erratum in: Eur Heart J. 2020;41(44):4255
7. Scherer DJ, Nelson AJ, Psaltis PJ, Nicholls SJ, Targeting low-density lipoprotein cholesterol with PCSK9 inhibitors: Intern Med J, 2017; 47(8); 856-65
8. Pirillo A, Catapano AL, Proprotein convertase subtilisin Kexin 9 inhibitors: Cardiol Clin, 2018; 36(2); 241-56
9. Hess CN, Low Wang CC, Hiatt WR, PCSK9 inhibitors: Mechanisms of action, metabolic effects, and clinical outcomes: Annu Rev Med, 2018; 69; 133-45
10. Robinson JG, Farnier M, Krempf MODYSSEY LONG TERM Investigators, Efficacy and safety of alirocumab in reducing lipids and cardiovascular events: N Engl J Med, 2015; 372(16); 1489-99
11. Sabatine MS, Giugliano RP, Wiviott SDOpen-Label Study of Long-Term Evaluation against LDL Cholesterol (OSLER) Investigators, Efficacy and safety of evolocumab in reducing lipids and cardiovascular events: N Engl J Med, 2015; 372(16); 1500-9
12. Gareri C, Polimeni A, Giordano S, Antisense oligonucleotides and small interfering RNA for the treatment of dyslipidemias: J Clin Med, 2022; 11(13); 3884
13. Ickenstein LM, Garidel P, Lipid-based nanoparticle formulations for small molecules and RNA drugs: Expert Opin Drug Deliv, 2019; 16(11); 1205-26
14. Jadhav V, Vaishnaw A, Fitzgerald K, Maier MA, RNA interference in the era of nucleic acid therapeutics: Nat Biotechnol, 2024; 42(3); 394-405
15. Kosmas CE, Muñoz Estrella A, Sourlas A, Inclisiran: A new promising agent in the management of hypercholesterolemia: Diseases, 2018; 6(3); 63
16. Zhang Y, Chen H, Hong L, Inclisiran: A new generation of lipid-lowering siRNA therapeutic: Front Pharmacol, 2023; 14; 1260921
17. Shadid M, Badawi M, Abulrob A, Antisense oligonucleotides: Absorption, distribution, metabolism, and excretion: Expert Opin Drug Metab Toxicol, 2021; 17(11); 1281-92
18. Shen X, Corey DR, Chemistry, mechanism and clinical status of antisense oligonucleotides and duplex RNAs: Nucleic Acids Res, 2018; 46(4); 1584-600
19. Ray KK, Landmesser U, Leiter LA, Inclisiran in patients at high cardiovascular risk with elevated LDL cholesterol: N Engl J Med, 2017; 376(15); 1430-40
20. Ray KK, Stoekenbroek RM, Kallend D, Effect of 1 or 2 doses of inclisiran on low-density lipoprotein cholesterol levels: One-year follow-up of the ORION-1 randomized clinical trial: JAMA Cardiol, 2019; 4(11); 1067-75
21. Katzmann JL, Packard CJ, Chapman MJ, Targeting RNA with antisense oligonucleotides and small interfering RNA: JACC State-of-the-art review: J Am Coll Cardiol, 2020; 76(5); 563-79
22. Wright RS, Ray KK, Raal FJORION Phase III Investigators, Pooled patient-level analysis of inclisiran trials in patients with familial hypercholesterolemia or atherosclerosis: J Am Coll Cardiol, 2021; 77(9); 1182-93
23. Reijman MD, Schweizer A, Peterson ALH, Rationale and design of two trials assessing the efficacy, safety, and tolerability of inclisiran in adolescents with homozygous and heterozygous familial hypercholesterolaemia: Eur J Prev Cardiol, 2022; 29(9); 1361-68
24. Wright RS, Raal FJ, Koenig W, Inclisiran administration potently and durably lowers LDL-C over an extended-term follow-up: The ORION-8 trial: Cardiovasc Res, 2024; 120(12); 1400-10
25. Leiter LA, Teoh H, Kallend D, Inclisiran lowers LDL-C and PCSK9 irrespective of diabetes status: The ORION-1 randomized clinical trial: Diabetes Care, 2019; 42(1); 173-76
26. Kallend D, Stoekenbroek R, He Y, Pharmacokinetics and pharmacodynamics of inclisiran, a small interfering RNA therapy, in patients with hepatic impairment: J Clin Lipidol, 2022; 16(2); 208-19
27. Wright RS, Collins MG, Stoekenbroek RM, Effects of renal impairment on the pharmacokinetics, efficacy, and safety of inclisiran: An analysis of the ORION-7 and ORION-1 Studies: Mayo Clin Proc, 2020; 95(1); 77-89
28. Ray KK, Troquay RPT, Visseren FLJ, Long-term efficacy and safety of inclisiran in patients with high cardiovascular risk and elevated LDL cholesterol (ORION-3): Results from the 4-year open-label extension of the ORION-1 trial: Lancet Diabetes Endocrinol, 2023; 11(2); 109-19
29. Li JJ, Zhao SP, Zhao D, 2023 Chinese guideline for lipid management: Front Pharmacol, 2023; 14; 1190934
30. Virani SS, Newby LK, Arnold SVPeer Review Committee Members, 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline for the management of patients with chronic coronary disease: A report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines: Circulation, 2023; 148(9); e9-e119 [Erratum in: Circulation. 2023;148(13):e148; Erratum in: Circulation. 2023;148(23):e186]
31. Ray KK, Wright RS, Kallend DORION-10 and ORION-11 Investigators, Two phase 3 trials of inclisiran in patients with elevated LDL cholesterol: N Engl J Med, 2020; 382(16); 1507-19
32. Ray KK, Kallend D, Leiter LAORION-11 Investigators, Effect of inclisiran on lipids in primary prevention: The ORION-11 trial: Eur Heart J, 2022; 43(48); 5047-57
33. Ray KK, Raal FJ, Kallend DGORION Phase III investigators, Inclisiran and cardiovascular events: A patient-level analysis of phase III trials: Eur Heart J, 2023; 44(2); 129-38
34. Yamashita S, Kiyosue A, Maheux P, Efficacy, safety, and pharmacokinetics of inclisiran in Japanese patients: Results from ORION-15: J Atheroscler Thromb, 2024; 31(6); 876-903
35. Huo Y, Lesogor A, Lee CW, Efficacy and safety of inclisiran in Asian patients: Results from ORION-18: JACC Asia, 2023; 4(2); 123-34
36. Hovingh GK, Lepor NE, Kallend D, Inclisiran durably lowers low-density lipoprotein cholesterol and proprotein convertase Subtilisin/Kexin Type 9 expression in homozygous familial hypercholesterolemia: The ORION-2 pilot study: Circulation, 2020; 141(22); 1829-31
37. Raal FJ, Kallend D, Ray KKORION-9 Investigators, Inclisiran for the treatment of heterozygous familial hypercholesterolemia: N Engl J Med, 2020; 382(16); 1520-30
38. Yuan J, Cai T, Zheng X, Potentiating CD8+ T cell antitumor activity by inhibiting PCSK9 to promote LDLR-mediated TCR recycling and signaling: Protein Cell, 2021; 12(4); 240-60 [Erratum in: Protein Cell. 2022;13(9):694–700]
39. Wang L, Li S, Luo H, PCSK9 promotes the progression and metastasis of colon cancer cells through regulation of EMT and PI3K/AKT signaling in tumor cells and phenotypic polarization of macrophages: J Exp Clin Cancer Res, 2022; 41(1); 303
40. Xu X, Cui Y, Cao L, PCSK9 regulates apoptosis in human lung adenocarcinoma A549 cells via endoplasmic reticulum stress and mitochondrial signaling pathways: Exp Ther Med, 2017; 13(5); 1993-99
41. Gan SS, Ye JQ, Wang L, Inhibition of PCSK9 protects against radiation-induced damage of prostate cancer cells: Onco Targets Ther, 2017; 10; 2139-46
42. Mohamed AA, Ray KK, Inclisiran and cardiovascular events: A comprehensive review of efficacy, safety, and future perspectives: Curr Opin Cardiol, 2023; 38(6); 527-32
43. Mulder JWCM, Galema-Boers AMH, Roeters van Lennep JE, First clinical experiences with inclisiran in a real-world setting: J Clin Lipidol, 2023; 17(6); 818-27
44. Marrs JC, Anderson SL, Inclisiran for the treatment of hypercholesterolaemia: Drugs Context, 2024; 13; 2023-12–3
45. Frampton JE, Inclisiran: A review in hypercholesterolemia: Am J Cardiovasc Drugs, 2023; 23(2); 219-30
46. Lloyd-Jones DM, Morris PB, Ballantyne CMWriting Committee, 2022 ACC Expert consensus decision pathway on the role of nonstatin therapies for LDL-cholesterol lowering in the management of atherosclerotic cardiovascular disease risk: A report of the American College of Cardiology Solution Set Oversight Committee: J Am Coll Cardiol, 2022; 80(14); 1366-418 [Erratum in: J Am Coll Cardiol. 2023;81(1):104]
47. Nissen SE, Lincoff AM, Brennan DCLEAR Outcomes Investigators, Bempedoic acid and cardiovascular outcomes in statin-intolerant patients: N Engl J Med, 2023; 388(15); 1353-64
48. Dyrbuś K, Gąsior M, Penson P, Inclisiran-new hope in the management of lipid disorders?: J Clin Lipidol, 2020; 14(1); 16-27
49. Katsiki N, Vrablik M, Banach M, Gouni-Berthold I, Inclisiran, low-density lipoprotein cholesterol and lipoprotein (a): Pharmaceuticals (Basel), 2023; 16(4); 577
50. Chantzaras A, Yfantopoulos J, Association between medication adherence and health-related quality of life of patients with hypertension and dyslipidemia: Hormones (Athens), 2023; 22(4); 665-76
51. Yin H, Zhang Q, Li Y, Ma J, Prevalence and correlates of severe anxiety in patients with first hospitalization for major depressive disorder combined with dyslipidemia: A large sample cross-sectional study: Front Psychiatry, 2024; 14; 1289614
52. Lumen A, Zhang X, Dutta S, Upreti VV, Predicting clinical pharmacokinetics/pharmacodynamics and impact of organ impairment on siRNA-based therapeutics using a mechanistic physiologically-based pharmacokinetic-pharmacodynamic model: Clin Pharmacol Ther, 2024; 115(5); 1054-64
53. André E, De Pauw A, Verdoy R, Changes of metabolic phenotype of cardiac progenitor cells during differentiation: Neutral effect of stimulation of AMP-activated protein kinase: Stem Cells Dev, 2019; 28(22); 1498-513
54. Bradley CK, Shrader P, Sanchez RJ, The patient journey with proprotein convertase subtilisin/kexin type 9 inhibitors in community practice: J Clin Lipidol, 2019; 13(5); 725-34
55. Burnett H, Fahrbach K, Cichewicz A, Comparative efficacy of non-statin lipid-lowering therapies in patients with hypercholesterolemia at increased cardiovascular risk: A network meta-analysis: Curr Med Res Opin, 2022; 38(5); 777-84
56. Banerjee Y, Pantea Stoian A, Cicero AFG, Inclisiran: A small interfering RNA strategy targeting PCSK9 to treat hypercholesterolemia: Expert Opin Drug Saf, 2022; 21(1); 9-20
57. Samuel E, Watford M, Egolum UO, Inclisiran: A first-in-class siRNA therapy for lowering low-density lipoprotein cholesterol: Ann Pharmacother, 2023; 57(3); 317-24
58. Silverman MG, Ference BA, Im K, Association between lowering LDL-C and cardiovascular risk reduction among different therapeutic interventions: A systematic review and meta-analysis: JAMA, 2016; 316(12); 1289-97
59. Baigent C, Blackwell L, Emberson JCholesterol Treatment Trialists’ (CTT) Collaboration, Efficacy and safety of more intensive lowering of LDL cholesterol: A meta-analysis of data from 170,000 participants in 26 randomised trials: Lancet, 2010; 376(9753); 1670-81
60. Stoekenbroek RM, Kallend D, Wijngaard PL, Kastelein JJ, Inclisiran for the treatment of cardiovascular disease: The ORION clinical development program: Future Cardiol, 2018; 14(6); 433-42
61. Zhang M, Deng Q, Wang L, Prevalence of dyslipidemia and achievement of low-density lipoprotein cholesterol targets in Chinese adults: A nationally representative survey of 163,641 adults: Int J Cardiol, 2018; 260; 196-203 [Erratum in: Int J Cardiol. 2018;267:218]
62. Kam N, Perera K, Zomer E, Inclisiran as adjunct lipid-lowering therapy for patients with cardiovascular disease: A cost-effectiveness analysis: Pharmacoeconomics, 2020; 38(9); 1007-20
63. Galactionova K, Salari P, Mattli R, Cost-effectiveness, burden of disease and budget impact of inclisiran: Dynamic cohort modelling of a real-world population with cardiovascular disease: Pharmacoeconomics, 2022; 40(8); 791-806 [Erratum in: Pharmacoeconomics. 2022;40(8):835]
64. Rosenson RS, Gaudet D, Hegele RAARCHES-2 Trial Team, Zodasiran, an RNAi therapeutic targeting ANGPTL3, for mixed hyperlipidemia: N Engl J Med, 2024; 391(10); 913-25
Figures
Figure 1. Inclisiran mechanism of action within hepatocytes (BioRender, version 2024, Science Suite Inc).Figure 2. Inclisiran co-occurrence diagram of keywords in the Web of Science coreconcentr (VOSviewer, version 1.6.20, The Centre for Science and Technology Studies, CWTS).Figure 3. Inclisiran time sequence map of keywords in the research field (CiteSpace, version 6.2.4, University of Redsell University, USA). Tables
 Table 1. High-frequency keywords of inclisiran (top 18).
Table 1. High-frequency keywords of inclisiran (top 18).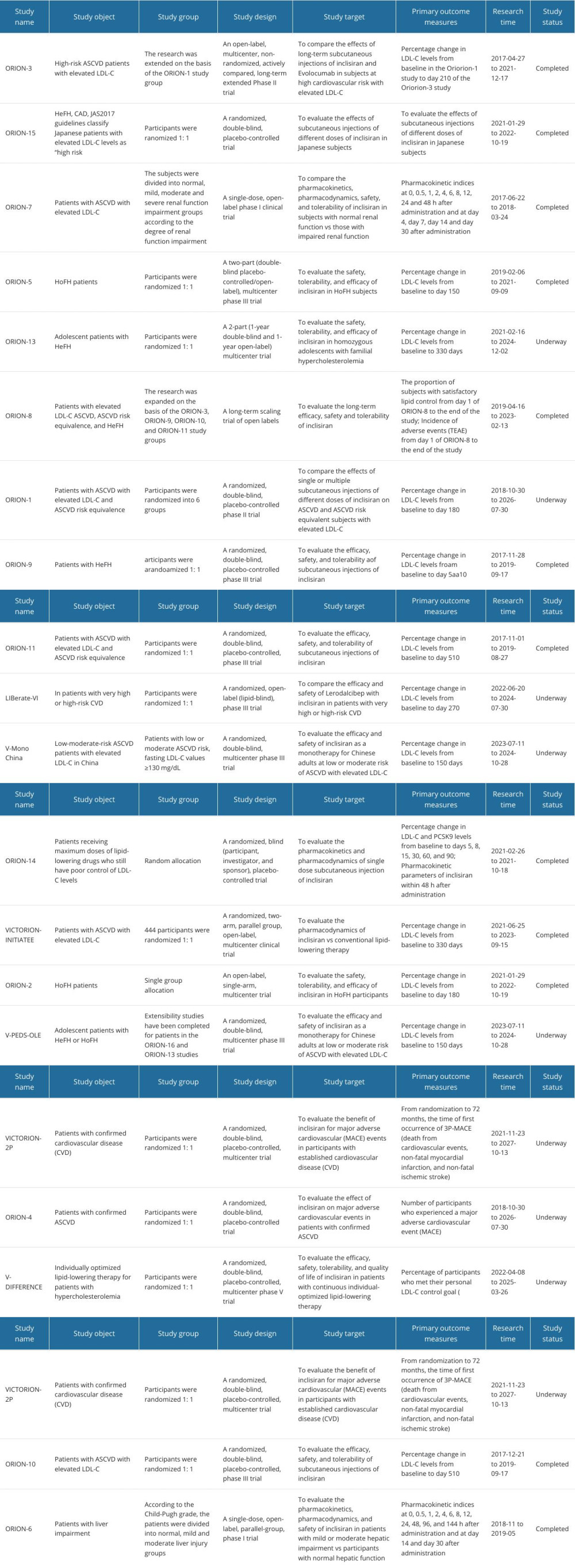 Table 2. Features and results of clinical trials of inclisiran in the treatment of hyperlipidemia.Table 1. High-frequency keywords of inclisiran (top 18).Table 2. Features and results of clinical trials of inclisiran in the treatment of hyperlipidemia.
Table 2. Features and results of clinical trials of inclisiran in the treatment of hyperlipidemia.Table 1. High-frequency keywords of inclisiran (top 18).Table 2. Features and results of clinical trials of inclisiran in the treatment of hyperlipidemia. In Press
Clinical Research
Association Between Total Cholesterol–to–High-Density Lipoprotein Ratio and Gestational Hypertension: A Cas...Med Sci Monit In Press; DOI: 10.12659/MSM.952395
Review article
Clinical Use of Endotracheal Intubation Without Neuromuscular Blockade: The Current Stage of KnowledgeMed Sci Monit In Press; DOI: 10.12659/MSM.951765
Clinical Research
Effect of Dexmedetomidine Hydrochloride Nasal Spray on Anxiety and Sleep in Patients Undergoing Gynecologic...Med Sci Monit In Press; DOI: 10.12659/MSM.952465
Clinical Research
Prognostic Value of Mortality Scoring Systems in Patients With Severe Burns: Identifying Key Predictors of ...Med Sci Monit In Press; DOI: 10.12659/MSM.951713
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,173
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,757,769
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,143
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,797
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387