05 July 2025: Clinical Research
Relationship Between CRP/ALB Ratio and Severity of Coronary Artery Lesions in Hypertensive Patients with Acute Myocardial Infarction
Xiuping Lou ABCDE 1, Nonghao Wen BDE 1, Yan Wang BCD 1, Ling Fang ABCDEFG 2,3*
DOI: 10.12659/MSM.946897
Med Sci Monit 2025; 31:e946897






Abstract
BACKGROUND: Hypertension is a significant risk factor for acute myocardial infarction (AMI), exacerbating myocardial ischemia and associated complications. This study explored the relationship between the C-reactive protein (CRP)-to-albumin (ALB) ratio (CRP/ALB) levels and the severity of coronary artery lesions and prognosis in 100 hypertensive patients with acute myocardial infarction.
MATERIAL AND METHODS: We enrolled 100 hypertensive patients with acute myocardial infarction and categorized them into different severity groups of coronary artery lesions based on coronary angiography results. Clinical data, including CRP and ALB levels, were collected, and the CRP/ALB ratio was calculated. Statistical methods were used to analyze the association between CRP/ALB ratio and the severity of coronary artery lesions. Patients were further divided into high and low CRP/ALB expression groups based on the median ratio value, and prognoses were compared. Kaplan-Meier survival curves and the log-rank test were used to assess adverse outcomes.
RESULTS: The CRP/ALB ratio significantly increased with the severity of coronary artery disease. Pearson correlation coefficient analysis demonstrated a significant positive correlation between the CRP/ALB ratio and the severity of coronary artery disease (P<0.05). Patients in the high CRP/ALB expression group had a significantly higher rate of unfavorable prognosis (40.00%) compared to those in the low expression group (16.00%) (P=0.008). The Kaplan-Meier (KM) survival curves for patients with high serum CRP/ALB expression shifted to the left compared to those with low expression, indicating poorer outcomes.
CONCLUSIONS: The CRP/ALB ratio is positively correlated with the severity of coronary artery disease. Higher serum CRP/ALB levels increase the risk of poor outcomes in hypertensive patients with AMI.
Keywords: biomarkers, Hypertension, Humans, C-Reactive Protein, Male, Female, Middle Aged, Myocardial Infarction, Prognosis, Coronary Artery Disease, Aged, Severity of Illness Index, Risk Factors, Coronary Angiography, Coronary Vessels, Kaplan-Meier Estimate, Serum Albumin
Introduction
Hypertension significantly increases the risk of acute myocardial infarction (AMI). Studies have shown that elevated blood pressure not only exacerbates the degree of myocardial ischemia but is also closely associated with multiple severe complications, including heart failure, arrhythmias, and increased risk of death [1–3]. Coronary angiography (CAG) is considered the criterion standard for diagnosing AMI; however, it is an invasive procedure that carries certain risks and potential complications [4,5]. Cardiac-specific biomarkers such as troponin (cTn) and creatine kinase MB (CK-MB) play a crucial role in the diagnosis of AMI, particularly troponin, which is currently regarded as the most sensitive and specific marker [6,7]. However, elevations in these biomarkers are not exclusive to AMI; other conditions like liver disease and end-stage renal disease can also cause false-positive results [8]. Therefore, developing more sensitive and specific biomarkers and optimizing treatment strategies remain critical challenges in current clinical practice.
In recent years, an increasing number of studies have shown that inflammatory responses play a critical role in the development and progression of cardiovascular diseases [9]. C-reactive protein (CRP) is an important inflammatory marker for cardiovascular diseases. It has been reported that elevated CRP levels are closely associated with the severity of coronary artery lesions. However, using CRP alone may not be sufficient to comprehensively assess a patient’s inflammatory status, as it can be influenced by various factors such as infections and inflammatory diseases [10]. ALB is an indicator of nutritional status and inflammation degree [11]. Low ALB levels have become an independent predictor of coronary artery disease and other cardiovascular diseases [12]. In patients with ST-elevation myocardial infarction (STEMI) who underwent direct percutaneous coronary intervention (PCI), the uric acid/albumin ratio was a predictor of intracoronal thrombotic severity [13]. The CRP/ALB ratio combines the effects of inflammatory response and nutritional status, providing a more comprehensive reflection of the patient’s overall condition [14,15]. Multiple studies have shown that the CRP/ALB ratio holds significant importance in prognostic assessments across various diseases, particularly in cancer and acute pancreatitis [16–18]. It has been reported that the combination of CRP and albumin has high predictive value for in-hospital mortality and out-of-hospital major adverse cardiac events (MACE) after percutaneous coronary intervention (PCI) in AMI patients (AUC of 0.850, sensitivity of 87.5%, and specificity of 70.6%) [19]. However, there is a lack of research assessing the severity of AMI in hypertensive patients using the CRP/ALB ratio. In this study, we investigated the correlation between the CRP/ALB ratio and the severity of coronary artery lesions and prognosis. By monitoring changes in the CRP/ALB ratio, doctors can promptly adjust treatment strategies during disease progression, thereby improving treatment outcomes.
Material and Methods
STUDY DESIGN AND PARTICIPANTS:
This single-center, hospital-based, cross-sectional observational study evaluated the severity of coronary artery disease in patients with acute myocardial infarction (AMI) and a history of hypertension. We included a consecutive sample of 100 patients admitted for AMI treatment who also had a history of hypertension. All patients underwent coronary angiography within 48 hours of symptom onset to assess the extent of coronary artery lesions.
INCLUSION AND EXCLUSION CRITERIA:
Inclusion criteria: (1) Hypertensive patients aged 30–70 years. (2) Hypertension diagnosed using a calibrated electronic sphygmomanometer to measure systolic and diastolic blood pressure while resting, measured at least twice, with a 5-minute interval between measurements. If both measurements met the diagnostic criteria for hypertension (systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg), then hypertension was confirmed. Alternatively, a history of hypertension could be confirmed if the patient was currently undergoing antihypertensive drug therapy. (3) Clinically diagnosed acute myocardial infarction (AMI) confirmed by electrocardiogram (ECG) showing ST-segment elevation or new left bundle branch block. (4) Elevated blood markers (eg, high troponin levels). (5) Completed coronary angiography within 48 hours of the onset of the disease. (6) Able to provide complete clinical data and serum samples. (7) Signed informed consent and agreed to participate in the study.
Exclusion criteria: (1) Younger than 30 or older than 70 years. (2) Had undergone cardiac surgery or interventional treatment. (3) Had other significant cardiovascular diseases such as severe heart failure or arrhythmias. (4) Had severe liver or kidney dysfunction or inflammatory diseases. (5) Pregnant or breastfeeding women. (6) Unable to comply with study requirements.
DATA COLLECTION:
This study systematically extracted the detailed medical history of patients through the electronic medical record system of the hospital, and collected clinical data, including age, sex, smoking history, and diabetes. Venous blood samples were collected from all patients on an empty stomach in the early morning, and serum was separated and stored at −80°C for subsequent testing. The serum CRP level was measured by high-sensitivity enzyme-linked immunosorbent assay (ELISA) and the serum ALB level was measured by biochemical methods. Among them, CRP ELISA kit (JL13865-96T, detection range: 31.25–2000 pg/mL; Sensitivity: 15.9 pg/mL) was purchased from Jianglai Biological. The CRP/ALB ratio was calculated as the CRP level divided by the ALB level.
:
The Gensini score is the sum of the scores for the degree of coronary artery stenosis and the location of lesions. The scoring for the degree of stenosis was as follows: the stenosis degree 1–25% was recorded as 1 point; 26–50% as 2 points; 51–75% as 4 points; 76–90% as 8 points; 91–99% as 16 points; and 100% as 32 points. The lesion score is the product of the individual lesion score and a coefficient, which indicates the importance of stenosis at different locations in the coronary artery system. The coefficients for each location are as follows: left main stem is 5; proximal left anterior descending (LAD) is 2.5; mid-LAD is 1.5; aorta and first diagonal branch is 1; second diagonal branch is 0.5; distal LAD is 1; proximal left circumflex (LCX) is 2.5; mid-LCX is 2.5; distal LCX is 1; obtuse marginal branch is 0.5; proximal right coronary artery (RCA) segment is 1; mid-RCA is 1; distal RCA is 1; posterior descending artery is 1; and left ventricular posterior branch is 0.5. A Gensini score of 1–30 is considered mild, 31–60 is moderate, and >60 is severe.
FOLLOW-UP AND PROGNOSTIC ASSESSMENT:
Patients were followed up for 2 years after discharge via outpatient visits or telephone calls, with evaluations conducted every 3 months. The follow-up period aimed to document poor prognosis, including heart failure, recurrent acute myocardial infarction (AMI), cardiogenic shock, and death from cardiovascular events (MACE).
STATISTICAL ANALYSIS:
GraphPad Prism 9.50 software (GraphPad Software, Inc., San Diego, CA, USA) was used for statistical analysis and graphing of data. Measurement data with a normal distribution are expressed as the mean±standard deviation and analyzed by
Results
A total of 100 cases of acute myocardial infarction (AMI) in hypertensive patients were included in the study. The patients ranged in age from 32 to 68 years old, with an average age of 52.7±15.2 years old, including 56 men and 44 women. There were 50 (50%) who had a smoking history, and 35 (35%) had diabetes.
According to the results of Gensini scores, the patients were divided into a mild lesions group (n=35), a moderate lesions group (n=45), and a severe lesions group (n=20). The mean Gensini score was 18.5±5.5 in the mild lesions group, 48.6±8.0 in the moderate lesions group, and 85.2±6.9 in the severe lesions group.
The CRP/ALB ratio was 0.14±0.03for the mild lesions group, 0.25±0.05 for moderate lesions group, and 0.40±0.06 for the severe lesions group (Figure 1).
Pearson correlation coefficient analysis showed a striking positive correlation between CRP/ALB ratio and Gensini score in coronary artery disease. The strength of this association is reflected by a Pearson correlation coefficient (r) value of 0.630, which has a significance level (
Based on the median value of the CRP/ALB level, hypertensive patients with AMI were divided into a low-expression group and a high-expression group. The 2-year poor prognosis conditions of the 2 groups were compared. The results showed that the poor prognosis rate of patients in the high CRP/ALB group (40.00%) was significantly higher than that in the low CRP/ALB group (16.00%) (
Discussion
s study explored the relationship between the CRP/ALB ratio and the severity of coronary artery lesions in hypertensive patients with acute myocardial infarction. The results revealed a significant positive correlation between the CRP/ALB ratio and the severity of coronary artery lesions. As the severity of lesions increased, the CRP/ALB ratio also increased. This suggests that the CRP/ALB ratio might serve as a potential biomarker for evaluating the extent of coronary artery lesions in hypertensive patients with acute myocardial infarction.
Inflammation plays a crucial role in the occurrence and development of acute myocardial infarction [13,21]. CRP is an acute-phase protein that reflects the inflammatory state of the body [22]. Elevated levels of CRP can be used to identify patients at risk of cardiovascular disease and certain cancers, and guide treatment in an environment-dependent manner [23]; ALB levels are typically influenced by nutritional status and the degree of inflammation [11]. In an inflammatory state, liver cells may be damaged or dysfunctional, decreasing in their ability to synthesize proteins [24,25], and their ratio can reflect the comprehensive impact of inflammation and body nutrition on coronary artery disease. The change of this ratio may indicate that there is a close relationship between inflammation and the progression of coronary atherosclerosis in patients with hypertension and AMI. Inflammation can promote the instability and rupture of atherosclerotic plaque through a variety of ways, thus leading to the occurrence of AMI and the aggravation of coronary artery disease [10,26,27].
The CRP/ALB ratio not only considers the impact of inflammation, but also incorporates the assessment of nutritional status, thus providing a more comprehensive reflection of the patient’s overall condition [28]. The CRP/ALB ratio is more closely associated with the severity of coronary artery disease than the use of CRP and ALB alone [29]. The CRP/ALB ratio is an new independent predictor of long-term adverse outcomes in coronary heart disease patients undergoing percutaneous coronary intervention (PCI) [30]. In this study, there was a significant positive correlation between the CRP/ALB ratio and the severity of coronary artery disease, indicating that as the severity of coronary artery disease increased, the CRP/ALB ratio significantly increased. In addition, higher serum CRP/ALB levels increase the risk of poor outcomes in hypertensive patients with AMI. CRP/ALB can be used to assess the severity of coronary artery lesions and also to predict the long-term prognosis of patients. This has important guiding significance for clinicians to formulate personalized treatment plans and follow-up programs. For example, a higher CRP/ALB ratio indicates strong inflammatory responses and poor nutritional status. Clinicians can use this information to increase the frequency of patient monitoring, such as by increasing the frequency of follow-up blood tests and echocardiograms to promptly identify potential risks. Additionally, in terms of treatment, they can consider intensifying anti-inflammatory therapy, providing appropriate nutritional supplementation, and adjusting medication regimens to improve patient outcomes and actively prevent adverse cardiovascular events.
This study has some limitations: the sample size was small and limited to a specific patient population, which may affect the external validity of the results. There are confounding factors that are not fully controlled (eg, age, sex, comorbidities, medication use), which may affect the expression of CRP/ALB ratio. In addition, the molecular and cellular mechanisms involved in the association of CRP/ALB ratio with coronary artery disease, as well as their specific roles in pathological and physiological processes, have not been thoroughly explored. Therefore, the present study needs to be validated in larger and more diverse cohorts, exploring the molecular and cellular mechanisms involved in the association between the CRP/ALB ratio and coronary artery disease, exploring its role in pathological and physiological processes, and further evaluating its practical utility.
Conclusions
The study showed that in hypertensive patients with acute myocardial infarction, there was a positive correlation between the CRP/ALB ratio and the severity of coronary artery lesions. The higher the ratio was, the more severe the lesions were, and higher serum CRP/ALB levels increased the risk of poor prognosis. Therefore, the CRP/ALB ratio could serve as a potential indicator for evaluating the degree of coronary artery lesions and the prognosis of patients, providing guidance for clinical treatment.
Figures
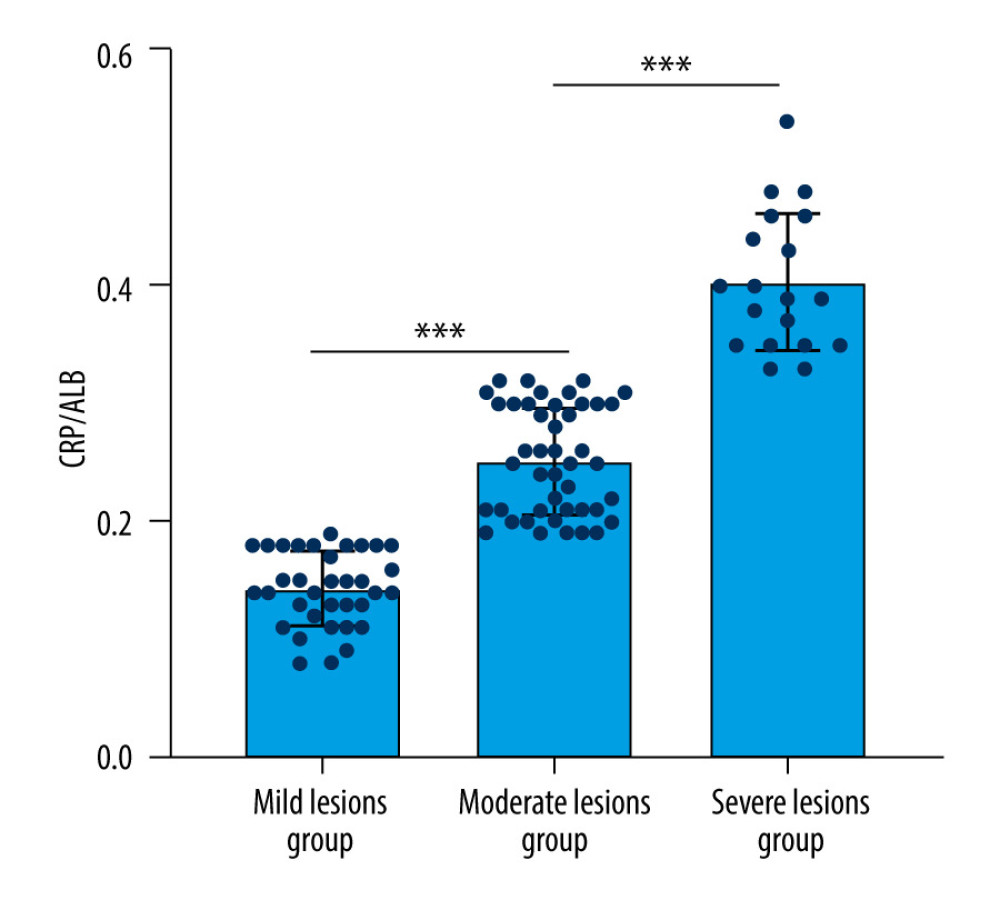 Figure 1. CRP/ALB ratio of different severity of coronary artery lesions. CRP – C-reactive protein; ALB – albumin. *** P<0.001. (GraphPad Prism, version 9.50 GraphPad Software, Inc.).
Figure 1. CRP/ALB ratio of different severity of coronary artery lesions. CRP – C-reactive protein; ALB – albumin. *** P<0.001. (GraphPad Prism, version 9.50 GraphPad Software, Inc.). 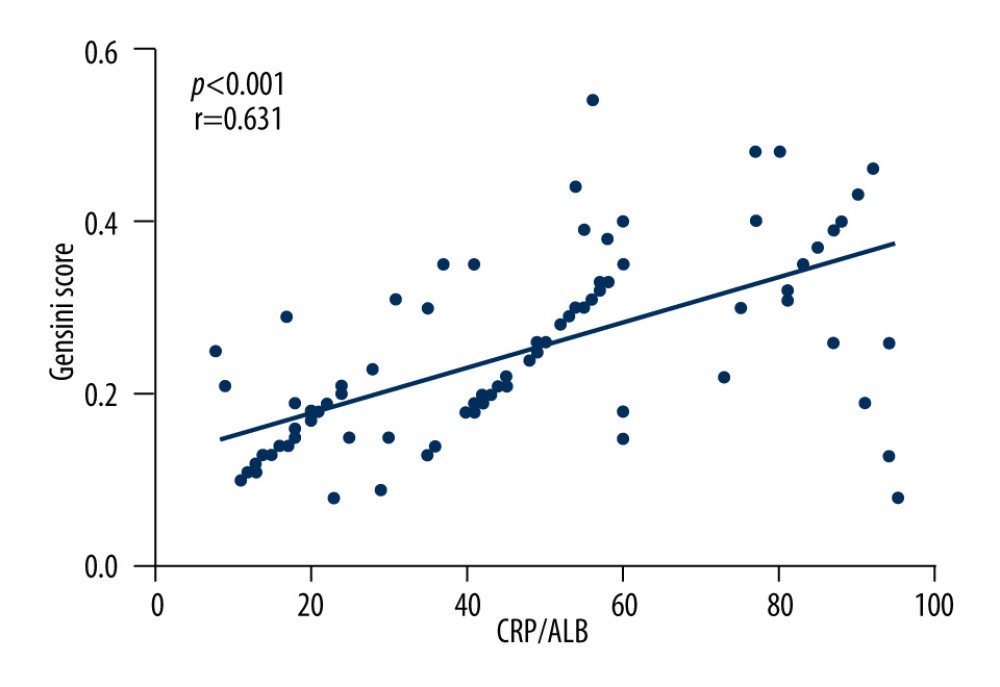 Figure 2. Correlation between CRP/ALB ratio and Gensini score. CRP – C-reactive protein; ALB – albumin; r – correlation coefficient. (GraphPad Prism, version 9.50 GraphPad Software, Inc.).
Figure 2. Correlation between CRP/ALB ratio and Gensini score. CRP – C-reactive protein; ALB – albumin; r – correlation coefficient. (GraphPad Prism, version 9.50 GraphPad Software, Inc.). 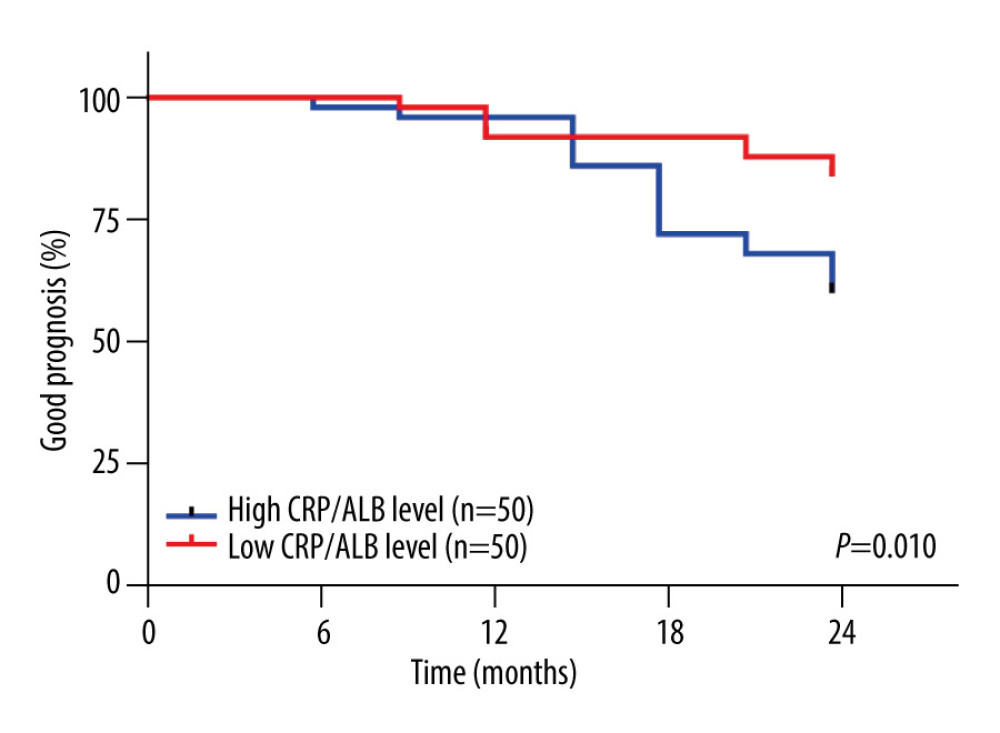 Figure 3. Kaplan-Meier curves of prognosis by serum CRP/ALB levels. CRP – C-reactive protein; ALB – albumin; The survival curve of the high CRP/ALB group shifted to the left compared to the low CRP/ALB group, indicating a longer survival period for patients in the low CRP/ALB group. (GraphPad Prism, version 9.50 GraphPad Software, Inc.).
Figure 3. Kaplan-Meier curves of prognosis by serum CRP/ALB levels. CRP – C-reactive protein; ALB – albumin; The survival curve of the high CRP/ALB group shifted to the left compared to the low CRP/ALB group, indicating a longer survival period for patients in the low CRP/ALB group. (GraphPad Prism, version 9.50 GraphPad Software, Inc.). 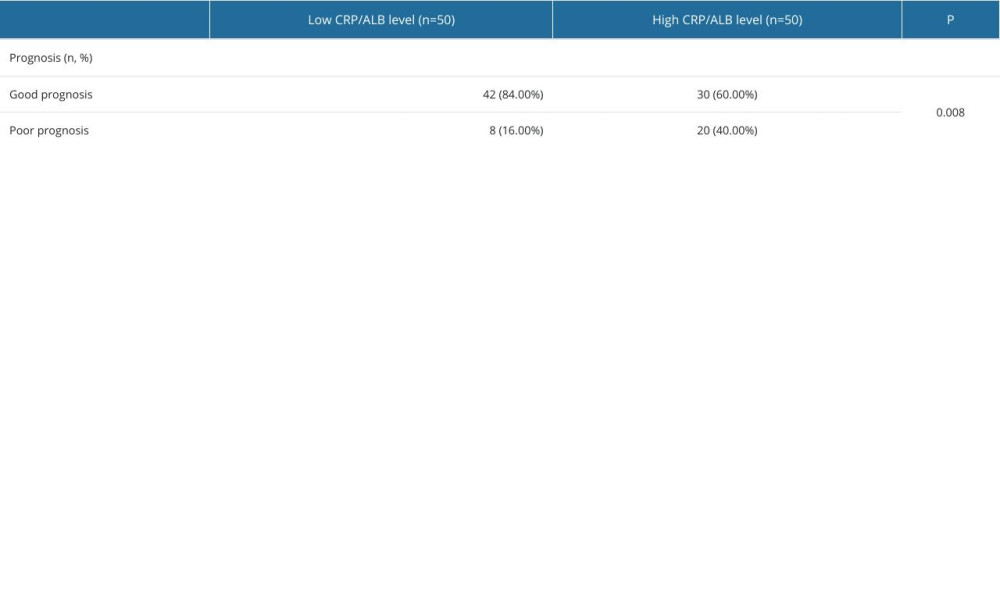
References
1. Pedrinelli R, Ballo P, Fiorentini C, Hypertension and acute myocardial infarction: An overview: J Cardiovasc Med (Hagerstown), 2012; 13(3); 194-202
2. Yusuf S, Hawken S, Ounpuu S, Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study: Lancet, 2004; 364(9438); 937-52
3. Sun X, Feng Y, Gong C, Hypertension-driven regulatory T-cell perturbations accelerate myocardial ischemia-reperfusion injury: Hypertension, 2023; 80(10); 2046-58
4. Wang Y, Yang R, Zhang Y, Prognostic value of serum 1,5-anhydroglucitol levels in patients with acute myocardial infarction: Rev Cardiovasc Med, 2022; 23(12); 394
5. Gao Y, Guo Y, Hao W, Correlation analysis and diagnostic value of serum homocysteine, cystatin C and uric acid levels with the severity of coronary artery stenosis in patients with coronary heart disease: Int J Gen Med, 2023; 16; 2719-31
6. Gupta S, Singh KN, Bapat V, Diagnosis of acute myocardial infarction: CK-MB versus cTn-T in Indian patients: Indian J Clin Biochem, 2008; 23(1); 89-91
7. Lee H, Kang H, Chae H, Oh EJ, Limited contribution of creatine kinase-myocardial band alongside high-sensitivity cardiac troponin in diagnosing acute myocardial infarction in an emergency department: Ann Lab Med, 2024; 44(6); 586-90
8. Mansouri F, Seyed Mohammadzad MH, Molecular miR-19a in acute myocardial infarction: Novel potential indicators of prognosis and early diagnosis: Asian Pac J Cancer Prev, 2020; 21(4); 975-82
9. Li C, Zong W, Zhang M, Increased ratio of circulating T-helper 1 to T-helper 2 cells and severity of coronary artery disease in patients with acute myocardial infarction: A prospective observational study: Med Sci Monit, 2019; 25; 6034-42
10. Attiq A, Afzal S, Ahmad W, Kandeel M, Hegemony of inflammation in atherosclerosis and coronary artery disease: Eur J Pharmacol, 2024; 966; 176338
11. Eckart A, Struja T, Kutz A, Relationship of nutritional status, inflammation, and serum albumin levels during acute illness: A prospective study: Am J Med, 2020; 133(6); 713-722e7
12. Arques S, Human serum albumin in cardiovascular diseases: Eur J Intern Med, 2018; 52; 8-12
13. Duman H, İpek E, Durak H, Uric acid to albumin ratio as a predictive marker for intracoronary thrombus severity in ST-segment elevation myocardial infarction (STEMI) patients undergoing primary percutaneous coronary intervention (PCI): Med Sci Monit, 2024; 30; e945832
14. Gomes de Lima KV, Maio R, Nutritional status, systemic inflammation and prognosis of patients with gastrointestinal cancer: Nutr Hosp, 2012; 27(3); 707-14
15. Glapa-Nowak A, Szczepanik M, Banaszkiewicz A, C-reactive protein/albumin ratio at diagnosis of pediatric inflammatory bowel disease: A retrospective multi-center study: Med Sci Monit, 2022; 28; e937842
16. Lu J, Xu BB, Zheng ZF, CRP/prealbumin, a novel inflammatory index for predicting recurrence after radical resection in gastric cancer patients: post hoc analysis of a randomized phase III trial: Gastric Cancer, 2019; 22(3); 536-45
17. Tominaga T, Nonaka T, Sumida Y, The C-reactive protein to albumin ratio as a predictor of severe side effects of adjuvant chemotherapy in stage III colorectal cancer patients: PLoS One, 2016; 11(12); e0167967
18. Kaplan M, Ates I, Akpinar MY, Predictive value of C-reactive protein/albumin ratio in acute pancreatitis: Hepatobiliary Pancreat Dis Int, 2017; 16(4); 424-30
19. Shan J, Zhao Q, Liu F, Analysis of clinical outcome and prognosis of C-reactive protein combined with albumin in patients with acute myocardial infarction: Altern Ther Health Med, 2024 [Online ahead of print]
20. Wang N, Liang C, Relationship of Gensini score with retinal vessel diameter and arteriovenous ratio in senile CHD: Open Life Sci, 2021; 16(1); 737-45
21. Matter MA, Paneni F, Libby P, Inflammation in acute myocardial infarction: The good, the bad and the ugly: Eur Heart J, 2024; 45(2); 89-103
22. Olson ME, Hornick MG, Stefanski A, A biofunctional review of C-reactive protein (CRP) as a mediator of inflammatory and immune responses: Differentiating pentameric and modified CRP isoform effects: Front Immunol, 2023; 14; 1264383
23. Rizo-Téllez SA, Sekheri M, Filep JG, C-reactive protein: A target for therapy to reduce inflammation: Front Immunol, 2023; 14; 1237729
24. Chen N, Yu Y, Shen W, Nutritional status as prognostic factor of advanced oesophageal cancer patients treated with immune checkpoint inhibitors: Clin Nutr, 2024; 43(1); 142-53
25. Kaysen GA, Albumin turnover in renal disease: Miner Electrolyte Metab, 1998; 24(1); 55-63
26. Klingenberg R, Luscher TF, Inflammation in coronary artery disease and acute myocardial infarction – is the stage set for novel therapies?: Curr Pharm Des, 2012; 18(28); 4358-69
27. Moreira DM, da Silva RL, Vieira JL, Role of vascular inflammation in coronary artery disease: Potential of anti-inflammatory drugs in the prevention of atherothrombosis. Inflammation and anti-inflammatory drugs in coronary artery disease: Am J Cardiovasc Drugs, 2015; 15(1); 1-11
28. Li Y, Li H, Song C, Early prediction of disease progression in patients with severe COVID-19 using C-reactive protein to albumin ratio: Dis Markers, 2021; 2021; 6304189
29. Karabağ Y, Çağdaş M, Rencuzogullari I, Relationship between C-reactive protein/albumin ratio and coronary artery disease severity in patients with stable angina pectoris: J Clin Lab Anal, 2018; 32(7); e22457
30. Liu ZY, Tang JN, Cheng MD, C-reactive protein-to-serum albumin ratio as a novel predictor of long-term outcomes in coronary artery disease patients who have undergone percutaneous coronary intervention: analysis of a real-world retrospective cohort study: Coron Artery Dis, 2021; 32(3); 191-96
Figures
Figure 1. CRP/ALB ratio of different severity of coronary artery lesions. CRP – C-reactive protein; ALB – albumin. *** P<0.001. (GraphPad Prism, version 9.50 GraphPad Software, Inc.).Figure 2. Correlation between CRP/ALB ratio and Gensini score. CRP – C-reactive protein; ALB – albumin; r – correlation coefficient. (GraphPad Prism, version 9.50 GraphPad Software, Inc.).Figure 3. Kaplan-Meier curves of prognosis by serum CRP/ALB levels. CRP – C-reactive protein; ALB – albumin; The survival curve of the high CRP/ALB group shifted to the left compared to the low CRP/ALB group, indicating a longer survival period for patients in the low CRP/ALB group. (GraphPad Prism, version 9.50 GraphPad Software, Inc.). In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387