09 February 2025: Clinical Researc
Inflammatory Biomarkers from Blood Counts as Prognostic Tools in Metastatic Esophageal Cancer
Yonca Yılmaz Ürün DOI: 10.12659/MSM.947202
Med Sci Monit 2025; 31:e947202






Abstract
BACKGROUND: Globally, esophageal cancer ranks as the sixth leading cause of cancer-related mortality. This retrospective study from a single center in Turkey aimed to evaluate hematological inflammatory biomarkers in complete blood count (CBC) data and outcomes in 113 patients with advanced esophageal carcinomas.
MATERIAL AND METHODS: We conducted a retrospective analysis of 113 patients with metastatic esophageal cancer composed of squamous (92), adenocarcinoma (18), and small cell (3) histology. We investigated neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio (LMR), platelet-to-lymphocyte ratio (PLR), neutrophil-to-platelet lymphocyte ratio (NLPR), neutrophile-to-monocyte ratio (NMR), systemic inflammation index (SII), systemic inflammatory response index (SIRI), and aggregate index of systemic inflammation (AISI) in terms of prognosis.
RESULTS: The initial treatment for 25.7% of patients consisted of a carboplatin-paclitaxel combination. In response to the initial round of chemotherapy, 52.2% of patients showed improvement (15% complete, 37.2% partial), while 18.6% experienced disease progression. Neutropenia was observed as the most prevalent severe (grades 3-4) adverse reaction, affecting 19.8% of patients. Higher NLR, PLR, SII, NLPR, SIRI, and AISI values were associated with worse survival (P=0.016, P=0.008, P=0.011, P=0.028, P=0.014, P=0.001, respectively), whereas higher LMR was correlated with better survival (P=0.001). The NMR analysis showed no significant association (P=0.46). Multivariate analysis identified independent prognostic factors except histology, PLR, and NLPR.
CONCLUSIONS: Research indicates that inflammatory indicators obtained from complete blood count analyses possess prognostic significance for individuals with metastatic esophageal cancer. These biomarkers demonstrate diverse capacities in forecasting the course of the disease. These simple and inexpensive markers need further confirmation to guide individualized treatment planning.
Keywords: Blood Cell Count, Esophagus, inflammation, Prognosis, Humans, Esophageal Neoplasms, Male, Female, Middle Aged, Aged, Retrospective Studies, Biomarkers, Tumor, Neutrophils, adult, Lymphocytes, Neoplasm Metastasis, Turkey, Monocytes, Aged, 80 and over, Adenocarcinoma
Introduction
Globally, esophageal cancer ranks as the seventh most prevalent cancer and the sixth leading cause of cancer-related mortality, resulting in over 500 000 deaths annually [1]. Projections indicate it will claim 880 000 lives by 2040 [2]. In the United States, 2024 estimates predict 22 370 new diagnoses and 16 130 fatalities [3]. The predominant subtype, squamous cell carcinoma (SCC), comprises about 85% of cases. However, cases of adenocarcinoma are increasing [4].
Esophageal cancers are often not diagnosed at an early stage and are associated with high mortality, with more than one-third of patients diagnosed at the metastatic stage [5]. The 5-year survival rate of patients with metastatic disease is approximately 5% [6]. Unfortunately, many patients are diagnosed with locally advanced-stage relapse despite multimodal treatment [7,8]. Most esophageal cancers are classified as either squamous cell carcinoma (ESCC) or adenocarcinoma. While squamous cell carcinoma remains the most prevalent form, the landscape of esophageal cancer is undergoing a significant shift. Over the past 4 decades, there has been a remarkable surge in the occurrence of esophageal adenocarcinoma (EAC), indicating a notable epidemiological transition in this disease [9]. Several factors contribute to the development of ESCC, including socioeconomic disadvantage, use of tobacco products, and alcohol intake (with the latter 2 having a multiplicative effect on risk when combined). Dietary habits also significantly influence ESCC occurrence. Specifically, the consumption of high-temperature beverages, nitrosamine-containing foods (such as processed meats), and red meat has been associated with an elevated ESCC risk. Additionally, deficiencies in micronutrients such as beta-carotene, folate, vitamin C, vitamin E, and riboflavin have been linked to an increased likelihood of developing ESCC [10]. Over the last 4 decades, advances in cancer treatment have led to a reduction in mortality rates, despite the generally poor prognosis. Comparing the 2 types of esophageal cancer, EAC shows a more favorable prognosis than ESCC. Research conducted in 2003 examined the survival trends of EAC and ESCC from the mid-1970s to the late 1990s, showing an increase in the relative 5-year survival rate for EAC from 5.7 to 13.6 throughout the study period. Likewise, ESCC saw an improvement in its 5-year relative survival rate, rising from 4.5 to 11.8 [11].
Cancer progression and management are significantly influenced by inflammation, which Hanahan et al recognized as a hallmark of cancer [12]. As an essential and inherent immune response, inflammation occurs when tissue homeostasis is disrupted. Patients with chronic inflammatory conditions are predisposed to cancer development at all stages [13]. The activation of tissue repair mechanisms by inflammation promotes the proliferation and survival of premalignant cells. Additionally, inflammation induces immunosuppression and fosters a microenvironment conducive to malignant cell survival [14]. Various cancer types are associated with inflammation, which contributes to their progression and metastasis [15,16].
Research has demonstrated that neutrophils significantly contribute to the growth and advancement of tumors. They accomplish this by releasing factors that promote proliferation, inhibiting T-lymphocyte function, and encouraging tumor angiogenesis [17,18]. Lymphocytes, crucial elements of the immune system, can impede tumor growth and spread, while halting its progression through cytotoxic actions [19]. Monocytes also play a vital role in immune responses, capable of modifying the tumor microenvironment by inducing local immunosuppression and supporting angiogenesis [20]. As a rich source of cytokines, platelets can enhance tumor development by promoting blood vessel formation [21,22]. The systemic inflammatory response can be assessed through various blood parameters, including C-reactive protein, cytokines, leukocytes and their subsets, and platelets [23].
Research has shown that various inflammatory markers correlate with esophageal cancer patient survival. Elevated neutrophil-lymphocyte ratio (NLR) and platelet-lymphocyte ratio (PLR) are notable indicators of reduced overall survival (OS) [24]. A large-scale retrospective analysis of 1883 esophageal SCC patients who underwent radical esophagectomy revealed that decreased perioperative lymphocyte-monocyte ratio (LMR) and increased NLR were linked to poorer survival outcomes. However, neutrophil-monocyte ratio (NMR) showed no association with survival [25]. Another retrospective study involving 655 esophagectomy patients demonstrated that high preoperative systemic inflammatory index (SII) and low prognostic nutritional index (PNI) strongly indicated unfavorable prognosis [26]. In an evaluation of 916 esophageal SCC patients who had radical esophagectomy, the systemic inflammatory response index (SIRI) emerged as an independent prognostic factor. Additionally, the aggregate index of systemic inflammation (AISI) was identified as a crucial determinant of prognosis [27]. Most of the current literature is based on early disease onset such as neoadjuvant and surgical treatment, and there are few studies evaluating these inflammatory markers in advanced stages. In a recent study evaluating the prognostic factors of advanced squamous cell esophageal cancer and gastric adenocarcinoma in both cancers, high hemoglobin, eosinophil, and CD4+ lymphocytes were independent predictive factors for PFS. Also, these parameters had prognostic effects [28]. In a different study investigating the gastric adenocarcinomas in terms of inflammatory biomarkers at the time of diagnosis, the modified Glascow prognostic score was found to be prognostic, but NLR, PLR, and SIRI were not independently related to OS in patients with metastasis [29]. In contrast to this research, our aim is to assess markers in esophageal cancer patients at the stage when metastasis has occurred. Also, there is a need for investigation due to rarity of the disease in Western countries [30].
Accumulating evidence from recent studies suggests that various inflammatory markers have a predictive value for survival in patients with cancer. Compared to other prognostic factors, inflammation-based prognostic indices are easy and feasible to obtain from routine blood tests before treatment. Some studies suggested treatment changes according to inflammatory clinical markers [31,32]. However, previous studies have provided limited information, mostly on non-metastatic patients, and have investigated the effect of single inflammatory markers on prognosis. A complete blood count (CBC) is an inexpensive, easy-to-administer laboratory test that is available in almost every healthcare facility and provides a wealth of information about blood cells and the immune system by evaluating different parameters. In this study, we aimed to investigate the association of 8 different biomarkers (NLR, PLR, LMR, NMR, SIRI, NLPR, SIRI, and AISI), which can only be obtained using complete counts, with survival in patients with metastatic esophageal cancer. Also, we assessed which of these factors is valuable and feasible for predicting the prognosis of metastatic esophageal cancer. Therefore, this retrospective study from a single center in Turkey aimed to evaluate hematological and inflammatory biomarkers in complete blood count data and outcomes in 113 patients with advanced esophageal carcinomas.
Material and Methods
ETHICS STATEMENT:
The research was conducted in line with the principles outlined in the Declaration of Helsinki. Additionally, the Ethics Committee at Van Yüzüncü Yıl University provided local approval for the study (16.02.2024 dated and 2024-02/14 numbered decision). Informed consent was not obtained from patients because of the retrospective design of the study. The Ethics Committee did not require informed consent.
PATIENT SELECTION:
Our research involved a retrospective analysis of esophageal carcinoma patients treated and monitored at the Van Yüzüncü Yıl University Faculty of Medicine Hospital from January 2012 to December 2023. The study included individuals over 18 years old diagnosed with stage 4 esophageal carcinoma who had not received prior systemic treatment for metastatic disease. We excluded patients under 18 years of age, those with multiple cancers, individuals without metastatic disease, and cases with incomplete data.
The time from initiation of first-line therapy to disease advancement, death, or final check-up in non-progressing individuals was used to determine progression-free survival (PFS). Overall survival (OS) was measured from the beginning of first-line treatment until death or the last follow-up date.
Patients were categorized based on 3 factors: tumor differentiation (good-moderate-poor), tumor location (proximal-middle-distal), and Eastern Cooperative Oncology Group (ECOG) Performance score (0–1 versus 2). For all patients, we gathered the following clinical information: age, gender, coexisting medical conditions, types of histology, histological grading, TNM staging, tumor site, and pretreatment blood cell counts including white blood cells, neutrophils, monocytes, lymphocytes, and platelets. The blood samples were analyzed before the first cycle of chemotherapy in metastatic stage to prevent differences in patients.
Blood samples for analysis were collected routinely prior to treatment initiation and/or at the time of diagnosis and were retrospectively evaluated through a structured electronic chart review. Laboratory measurements were categorized as being performed at initial diagnosis if the blood draw occurred at the time of histopathological cancer confirmation or within a 1-month window before or after this date. Blood samples taken within this 1-month period were only included in the analysis if no cancer-specific treatments (such as surgery, systemic therapy, or radiation) had been administered during that time frame. In cases where multiple laboratory analyses were available, the one closest to the histopathological first diagnosis date was selected for this study. The classification of laboratory parameters as being conducted at first diagnosis was contingent upon the blood draw taking place at the time of histopathological initial cancer diagnosis or within the specified 1-month window.
A Sysmex XN-1000 automated hematology analyzer (Sysmex, Japan) was used for blood cell counting and leukocyte differentiation. This system utilizes flowcytometry fluorescence technology to obtain data on cell membrane composition and cytoplasmic activity [33]. Normal limits for laboratory values were PLT 150–350 G/l, WBC 4.0–10.0 G/l, neutrophils 2.0–7.5 G/l, lymphocytes 1.0–4.0 G/l, and monocytes 0.0–1.2 G/l. Other units were recalculated and converted to the appropriate units. We computed various inflammatory markers using the following formulas: NLR was calculated as neutrophil divided by lymphocyte (N/L); PLR as platelet divided by neutrophil (P/L); NMR as neutrophil divided by monocyte (N/M); LMR as lymphocyte divided by monocyte (L/M); SII as platelet multiplied by neutrophil, then divided by lymphocyte (PxN/L); NLPR as neutrophil divided by the product of lymphocyte and platelet (N/LxP); SIRI as the product of neutrophil and monocyte, divided by lymphocyte (NxM/L); and AISI as the product of neutrophil, platelet, and monocyte, divided by lymphocyte (NxPxM/L). Blood parameters were determined based on pretreatment blood counts.
STATISTICAL ANALYSIS:
Statistical analysis of all data was conducted using SPSS software (version 26.0; IBS SPSS, Armonk, NY, USA). Frequencies are used to present categorical data, while numerical data are expressed as medians or means based on their distribution. The Shapiro-Wilk and Kolmogorov-Smirnov methods were employed to determine data distribution. ROC analysis was utilized to identify the optimal predictive values for NLR, PLR, SII, PNI, and SIRI (Figure 1). For data without an optimal value, the median value of the relevant data in the study population was used for prediction. The chi-squared test was applied to examine associations between categorical data. The Kaplan-Meier method and log-rank test were used to evaluate overall survival stratified by multiple inflammatory biomarkers. Cox regression was employed for multivariate analyses. A P value less than 0.05 was considered statistically significant.
Results
PATIENT CHARACTERISTICS:
The study encompassed 113 participants (47 male, 66 female) with a mean age of 66 years. Hypertension and Diabetes Mellitus was observed in 19.5% and 8% of the subjects, respectively. Dysphagia was the most common presenting symptom, affecting 94.2% of patients.
In response to the initial round of chemotherapy, 52.2% of patients showed improvement (15% complete, 37.2% partial), while 18.6% experienced disease progression. Most patients (81.4%) were diagnosed with the SCC subtype, and 49.3% had tumors located in the middle esophagus. Metastases to distant lymph nodes were the most prevalent (53.2%). Additional demographic and clinicopathological features of the study population are detailed in Table 1.
The initial treatment for 25.7% of patients consisted of a carboplatin-paclitaxel combination. Neutropenia was observed as the most prevalent severe (grade 3–4) adverse reaction, affecting 19.8% of patients. Table 2 provides a comprehensive overview of the various chemotherapy protocols employed and their corresponding adverse effects.
The mean neutrophil and lymphocyte counts were 5000 n/ul and 2040 n/ul, respectively, and monocyte and platelet values were 580 n/ul and 274 000 n/ul, respectively. The pretreatment blood and inflammatory parameters of the patients are summarized in Table 3.
SURVIVAL ANALYSIS:
The study revealed significant differences in median survival times based on various biomarkers. Subjects with low NLR had a median survival of 25 months, compared to 12 months for those with high NLR, which is a statistically significant difference (P=0.016). This finding was consistent across 2 separate analyses. For NMR, patients with low rates demonstrated a median survival of 20 months, while those with high rates exhibited a median survival of 15 months, although this difference was not statistically significant (P=0.40). Conversely, high LMR rates were associated with significantly longer median survival (32 months) compared to low LMR rates (11 months) (P=0.002). Low SII rates were correlated with a median survival of 25 months, significantly higher than the 11 months observed in patients with high SII rates (P=0.011). Patients with low NLPR rates had a median survival of 23 months, significantly longer than the 15 months for those with high NLPR rates (P=0.028). Low PLR was associated with significantly better survival compared to higher values (P=0.008). The median OS were 32 and 14 months, respectively. SIRI rates demonstrated a marked difference, with low rates associated with 42 months median survival compared to 12 months for high rates (P=0.014). Finally, low AISI rates corresponded to a median survival of 32 months, significantly higher than the 12 months observed in patients with high AISI rates (P=0.007) (Figures 2, 3).
In multivariate analysis, in terms of OS the prognostic effect of histology, NLPR and PLR were not observed (
Discussion
This study demonstrated that NLR, PLR, LMR, SII, NLPR, SIRI, and AISI were associated with survival, whereas NMR did not exhibit an association with survival in patients with metastatic esophageal cancer. Elevated NLR, PLR, SII, NLPR, SIRI, and AISI values were correlated with decreased survival, while higher LMR values were associated with improved survival outcomes. Despite the limitations inherent in this study, it possesses several distinctive characteristics. Primarily, while most of the existing research has focused on local or locally advanced disease, our patient cohort comprised exclusively individuals with metastatic disease. Furthermore, the evaluation of multiple parameters enhances the significance of our investigation.
Inflammation plays a significant role in the tumor microenvironment, influencing cancer development, immune evasion, and metastasis. The correlation between elevated NLR and PLR values and poorer survival outcomes observed in this study aligns with the hypothesis that increased neutrophils and platelets contribute to tumor progression by promoting angiogenesis and suppressing anti-tumor immunity. The association between high NLR and PLR and unfavorable survival outcomes in metastatic esophageal cancer is well substantiated by the extant literature.
A meta-analysis of 20 studies involving 6457 patients found that a higher preoperative NLR was associated with worse survival in patients with esophageal cancer [34]. In a retrospective study of 168 patients who underwent curative surgery followed by chemotherapy for esophageal cancer, longer survival and lower anastomotic leakage were observed in the low PLR group [35]. In a study in which 1883 patients with esophageal SCC who underwent radical esophagectomy were evaluated retrospectively, low perioperative LMR and high NLR values were associated with worse survival, but NMR was not associated with survival [25]. Some studies have found the morphology of erythrocytes and platelets has utility in predicting prognosis of esophageal cancer patients who underwent surgery [36]. In a study evaluating 204 patients with advanced esophageal cancer who underwent concurrent chemoradiotherapy, NLR and LMR were shown to predict survival [37]. In a study of 370 esophageal SCC patients undergoing curative surgery, a low LMR was found to be an independent predictor of poor prognosis [38]. Puhr et al investigated the effect of inflammatory markers in early stages of esophageal adenocarcinomas who underwent surgery. Although NLR, PLR and SIRI had prognostic effect in univariate analysis, they lost their effect in multivariate analysis, and only modified Glascow prognostic score predicted prognosis in early stages of esophageal adenocarcinoma [29]. In our study, low NLR, PLR, and NLPR were associated with better survival, whereas low LMR was associated with worse survival. NMR is not associated with survival. High NLR and PLR reflect a pro-inflammatory state in which neutrophils and platelets help tumor growth, while reduced lymphocytes weaken the immune system against cancer.
In our study, higher LMR was associated with better survival outcomes. This finding emphasizes the critical role of lymphocytes in generating an effective immune response against cancer. A higher LMR probably reflects a more favorable immune profile in which increased lymphocyte activity suppresses tumor proliferation and metastasis, while a lower monocyte count limits the tumor-promoting effects of chronic inflammation.
In a retrospective study of 298 esophageal SCC patients, patients with low SII had significantly better 5-year survival than patients with high SII (51.9% vs 24.0%,
We also found that the comprehensive indices SII, SIRI, and AISI, which include neutrophils, lymphocytes, and platelets, have strong prognostic value. These indices provide a more integrated reflection of inflammatory and immune responses in cancer patients. Previous studies have been conducted in limited and locally advanced disease, and our study confirmed the negative impact of higher values on patient outcomes in stage 4 disease, which was significantly associated with worse survival.
The availability of these prognostic markers from simple, inexpensive blood tests has important clinical implications. These biomarkers could be easily integrated into routine clinical practice, allowing patients to be stratified according to their risk profile. Patients with high inflammatory markers may require more aggressive treatment strategies or closer monitoring, while those with more favorable markers may be candidates for less intensive treatments.
However, it is important to note that these markers should be interpreted in combination with other clinical factors such as tumor stage, histology, and patient performance status. Blood-based biomarkers provide a useful tool but are not a substitute for comprehensive clinical assessment.
This study has several limitations. First, this was a single-center retrospective study with a relatively small sample size. Second, whole-blood parameters may be affected by factors such as anti-inflammatory drug use. Third, the adenocarcinoma and small cell cancer subtype was smaller than squamous cell subtype, which decreased the comparative power of analysis in these groups.
Conclusions
In conclusion, in our study, higher NLR, PLR, SII, NLPR, SIRI, and AISI values were associated with worse survival, whereas higher LMR values were associated with better survival. We did not find any association between NMR and survival, which is consistent with the existing literature. Complete blood count-derived inflammatory markers demonstrate prognostic significance for patients with metastatic esophageal cancer. Studies reveal that these biomarkers possess varying capabilities in predicting the course of the disease. These simple and inexpensive markers may need further confirmation to guide individualized treatment planning.
Figures
 Figure 1. ROC curve analysis of the optimal cut-off values of neutrophil to lymphocyte (NLR), lymphocyte to monocyte (LMR), platelet to lymphocyte (PLR), neutrophil platelet lymphocyte (NLPR), neutrophile to monocyte ratio (NMR), systemic inflammation index (SII), systemic inflammatory response index (SIRI), and aggregate index of systemic inflammation (AISI).
Figure 1. ROC curve analysis of the optimal cut-off values of neutrophil to lymphocyte (NLR), lymphocyte to monocyte (LMR), platelet to lymphocyte (PLR), neutrophil platelet lymphocyte (NLPR), neutrophile to monocyte ratio (NMR), systemic inflammation index (SII), systemic inflammatory response index (SIRI), and aggregate index of systemic inflammation (AISI).  Figure 2. (A) The Kaplan-Meier curves in terms of overall survival for platelet-lymphocyte ratio. (B) The Kaplan-Meier curves in terms of overall survival for lymphocyte-monocyte ratio. (C) The Kaplan-Meier curves in terms of overall survival for neutrophil-lymphocyte ratio. (D) The Kaplan-Meier curves in terms of overall survival for neutrophil-monocyte ratio.
Figure 2. (A) The Kaplan-Meier curves in terms of overall survival for platelet-lymphocyte ratio. (B) The Kaplan-Meier curves in terms of overall survival for lymphocyte-monocyte ratio. (C) The Kaplan-Meier curves in terms of overall survival for neutrophil-lymphocyte ratio. (D) The Kaplan-Meier curves in terms of overall survival for neutrophil-monocyte ratio. 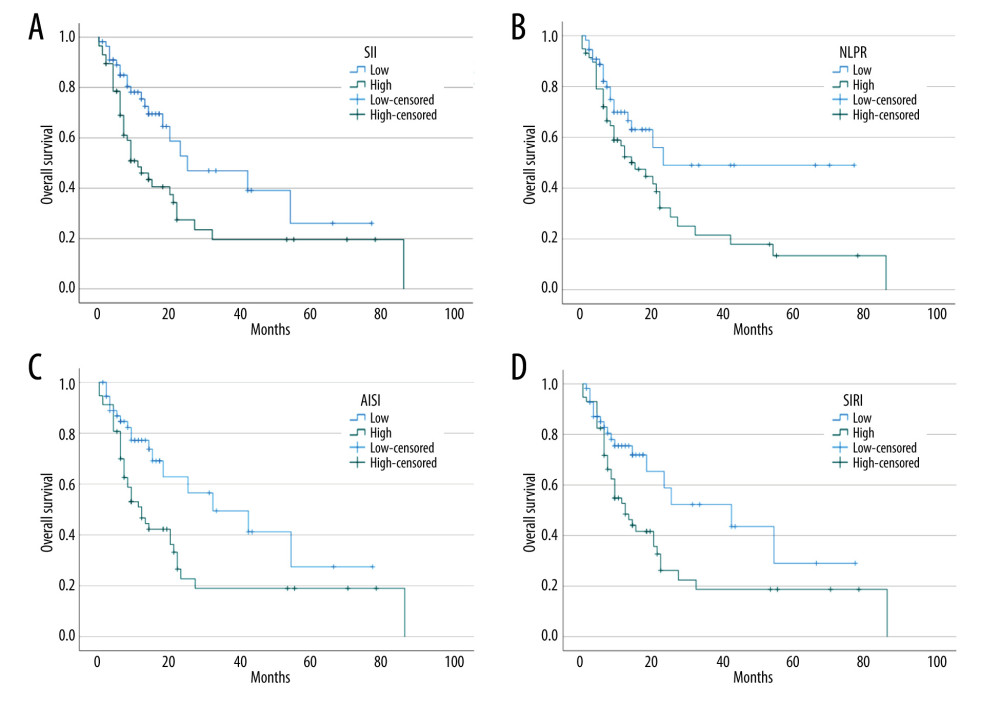 Figure 3. (A) The Kaplan-Meier curves in terms of overall survival for systemic inflammatory index. (B) The Kaplan-Meier curves in terms of overall survival for neutrophil-lymphocyte-platelet ratio. (C) The Kaplan-Meier curves in terms of overall survival for aggregate index of systemic inflammation. (D) The Kaplan-Meier curves in terms of overall survival for systematic inflammation response index.
Figure 3. (A) The Kaplan-Meier curves in terms of overall survival for systemic inflammatory index. (B) The Kaplan-Meier curves in terms of overall survival for neutrophil-lymphocyte-platelet ratio. (C) The Kaplan-Meier curves in terms of overall survival for aggregate index of systemic inflammation. (D) The Kaplan-Meier curves in terms of overall survival for systematic inflammation response index. References
1. Sung H, Ferlay J, Siegel RL, Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries: Cancer J Clin, 2021; 71(3); 209-49
2. Morgan E, Soerjomataram I, Rumgay H, The global landscape of esophageal squamous cell carcinoma and esophageal adenocarcinoma incidence and mortality in 2020 and projections to 2040: New estimates from GLOBOCAN 2020: Gastroenterology, 2022; 163(3); 649-58e2
3. Siegel RL, Giaquinto AN, Jemal A, Cancer statistics, 2024: Cancer J Clin, 2024; 74(1); 12-49
4. Arnold M, Ferlay J, van Berge Henegouwen MI, Soerjomataram I, Global burden of oesophageal and gastric cancer by histology and subsite in 2018: Gut, 2020; 69(9); 1564-71
5. Chen Z, Ren Y, Du XL, Incidence and survival differences in esophageal cancer among ethnic groups in the United States: Oncotarget, 2017; 8(29); 47037-51
6. Siegel RL, Miller KD, Jemal A, Cancer statistics, 2019: Cancer J Clin, 2019; 69(1); 7-34
7. Smyth EC, Lagergren J, Fitzgerald RC, Oesophageal cancer: Nat Rev Dis Primer, 2017; 3; 17048
8. Patel N, Benipal B, Incidence of esophageal cancer in the United States from 2001–2015: A United States cancer statistics analysis of 50 states: Cureus, 2018; 10(12); e3709
9. Napier KJ, Scheerer M, Misra S, Esophageal cancer: A Review of epidemiology, pathogenesis, staging workup and treatment modalities: World J Gastrointest Oncol, 2014; 6(5); 112-20
10. Liang H, Fan JH, Qiao YL, Epidemiology, etiology, and prevention of esophageal squamous cell carcinoma in China: Cancer Biol Med, 2017; 14(1); 33-41
11. Polednak AP, Trends in survival for both histologic types of esophageal cancer in US surveillance, epidemiology and end results areas: Int J Cancer, 2003; 105(1); 98-100
12. Hanahan D, Hallmarks of cancer: New dimensions: Cancer Discov, 2022; 12(1); 31-46
13. Elinav E, Nowarski R, Thaiss CA, Inflammation-induced cancer: Crosstalk between tumours, immune cells and microorganisms: Nat Rev Cancer, 2013; 13(11); 759-71
14. Grivennikov SI, Greten FR, Karin M, Immunity, inflammation, and cancer: Cell, 2010; 140(6); 883-99
15. Demir H, Katırcılar Y, Beypınar İ, Prognostic value of systemic immune index in patients with metastatic gastric cancer: Eur Arch Med Res, 2021; 37(2); 95-100
16. Sozel H, Prognostic impact of prognostic nutritional index and neutrophil/lymphocyte ratio in patients with small-cell lung cancer: Eurasian J Med Investig, 2021; 5(2); 207-12
17. Uribe-Querol E, Rosales C, Neutrophils in cancer: Two sides of the same coin: J Immunol Res, 2015; 2015; 983698
18. Xiong S, Dong L, Cheng L, Neutrophils in cancer carcinogenesis and metastasis: J Hematol OncolJ Hematol Oncol, 2021; 14(1); 173
19. Mantovani A, Allavena P, Sica A, Balkwill F, Cancer-related inflammation: Nature, 2008; 454(7203); 436-44
20. Chanmee T, Ontong P, Konno K, Itano N, Tumor-associated macrophages as major players in the tumor microenvironment: Cancers, 2014; 6(3); 1670-90
21. Balkwill F, Mantovani A, Inflammation and cancer: Back to Virchow?: Lancet, 2001; 357(9255); 539-45
22. Bambace NM, Holmes CE, The platelet contribution to cancer progression: J Thromb Haemost, 2011; 9(2); 237-49
23. McCormick Matthews LH, Noble F, Tod J, Systematic review and meta-analysis of immunohistochemical prognostic biomarkers in resected oesophageal adenocarcinoma: Br J Cancer, 2015; 113(1); 107-18
24. Yodying H, Matsuda A, Miyashita M, Prognostic significance of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in oncologic outcomes of esophageal cancer: A systematic review and meta-analysis: Ann Surg Oncol, 2016; 23(2); 646-54
25. Shang QX, Yang YS, Hu WP, Clinical and prognostic significance of preoperative lymphocyte-monocyte ratio, neutrophil-lymphocyte ratio and neutrophil-monocyte ratio on esophageal squamous cell carcinoma patients: Transl Cancer Res, 2020; 9(6); 3903-14
26. Zhang H, Shang X, Ren P, The predictive value of a preoperative systemic immune-inflammation index and prognostic nutritional index in patients with esophageal squamous cell carcinoma: J Cell Physiol, 2019; 234(2); 1794-802
27. Geng Y, Zhu D, Wu C, A novel systemic inflammation response index (SIRI) for predicting postoperative survival of patients with esophageal squamous cell carcinoma: Int Immunopharmacol, 2018; 65; 503-10
28. Li N, Gao L, Ge Y, Prognostic and predictive significance of circulating biomarkers in patients with advanced upper gastrointestinal cancer undergoing systemic chemotherapy: Front Oncol, 2023; 13; 1195848
29. Puhr HC, Weirauch CC, Selimi F, Systemic inflammatory biomarkers as prognostic tools in patients with gastroesophageal adenocarcinoma: J Cancer Res Clin Oncol, 2023; 149(19); 17081-91
30. Liu CQ, Ma YL, Qin Q, Epidemiology of esophageal cancer in 2020 and projections to 2030 and 2040: Thorac Cancer, 2023; 14(1); 3-11
31. Motzer RJ, Penkov K, Haanen J, Avelumab plus axitinib versus sunitinib for advanced renal-cell carcinoma: N Engl J Med, 2019; 380(12); 1103-15
32. Beypınar I, Sözel Y, Önder AH, Assessing the prognostic value of IMDC risk score for nivolumab-treated patients with renal cancer and malignant melanoma: Cancer Biomark, 2023; 38(3); 367-77
33. Lapić I, Brenčić T, Rogić D, The value of extended inflammatory parameters obtained on Sysmex XN-1000 haematology analyser as early laboratory indicators of COVID-19: Scand J Clin Lab Invest, 2022; 82(3); 257-59
34. Pirozzolo G, Gisbertz SS, Castoro C, Neutrophil-to-lymphocyte ratio as prognostic marker in esophageal cancer: A systematic review and meta-analysis: J Thorac Dis, 2019; 11(7); 3136-45
35. Aoyama T, Ju M, Komori K, The platelet-to-lymphocyte ratio is an independent prognostic factor for patients with esophageal cancer who receive curative treatment: In Vivo, 2022; 36(4); 1916-22
36. Hirahara N, Matsubara T, Kawahara D, Prognostic value of hematological parameters in patients undergoing esophagectomy for esophageal squamous cell carcinoma: Int J Clin Oncol, 2016; 21(5); 909-19
37. Li KJ, Xia XF, Su M, Predictive value of lymphocyte-to-monocyte ratio (LMR) and neutrophil-to-lymphocyte ratio (NLR) in patients with oesophageal cancer undergoing concurrent chemoradiotherapy: BMC Cancer, 2019; 19(1); 1004
38. Xu X, Jing J, Inflammation-related parameter serve as prognostic biomarker in esophageal squamous cell carcinoma: Front Oncol, 2022; 12; 900305
39. Feng JF, Chen S, Yang X, Systemic immune-inflammation index (SII) is a useful prognostic indicator for patients with squamous cell carcinoma of the esophagus: Medicine (Baltimore), 2017; 96(4); e5886
40. Wang HK, Wei Q, Yang YL, Clinical usefulness of the lymphocyte-to-monocyte ratio and aggregate index of systemic inflammation in patients with esophageal cancer: A retrospective cohort study: Cancer Cell Int, 2023; 23(1); 13
41. Yan K, Wei W, Shen W, Combining the systemic inflammation response index and prognostic nutritional index to predict the prognosis of locally advanced elderly esophageal squamous cell carcinoma patients undergoing definitive radiotherapy: J Gastrointest Oncol, 2022; 13(1); 13-25
Figures
Figure 1. ROC curve analysis of the optimal cut-off values of neutrophil to lymphocyte (NLR), lymphocyte to monocyte (LMR), platelet to lymphocyte (PLR), neutrophil platelet lymphocyte (NLPR), neutrophile to monocyte ratio (NMR), systemic inflammation index (SII), systemic inflammatory response index (SIRI), and aggregate index of systemic inflammation (AISI).Figure 2. (A) The Kaplan-Meier curves in terms of overall survival for platelet-lymphocyte ratio. (B) The Kaplan-Meier curves in terms of overall survival for lymphocyte-monocyte ratio. (C) The Kaplan-Meier curves in terms of overall survival for neutrophil-lymphocyte ratio. (D) The Kaplan-Meier curves in terms of overall survival for neutrophil-monocyte ratio.Figure 3. (A) The Kaplan-Meier curves in terms of overall survival for systemic inflammatory index. (B) The Kaplan-Meier curves in terms of overall survival for neutrophil-lymphocyte-platelet ratio. (C) The Kaplan-Meier curves in terms of overall survival for aggregate index of systemic inflammation. (D) The Kaplan-Meier curves in terms of overall survival for systematic inflammation response index. Tables
 Table 1. Demographic, clinical and pathologic findings of the patients.
Table 1. Demographic, clinical and pathologic findings of the patients. Table 2. Chemotherapy regimens and chemotherapy adverse effects.
Table 2. Chemotherapy regimens and chemotherapy adverse effects. Table 3. Pretreatment blood and inflammatory parameters.Table 1. Demographic, clinical and pathologic findings of the patients.Table 2. Chemotherapy regimens and chemotherapy adverse effects.Table 3. Pretreatment blood and inflammatory parameters.
Table 3. Pretreatment blood and inflammatory parameters.Table 1. Demographic, clinical and pathologic findings of the patients.Table 2. Chemotherapy regimens and chemotherapy adverse effects.Table 3. Pretreatment blood and inflammatory parameters. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387