07 July 2025: Clinical Research
Evaluating Postoperative Hidden Blood Loss in Proximal Femoral Nail Anti-Rotation Fixation: The Role of Greater Trochanter Fracture Comminution
Zahra Al Timimi DOI: 10.12659/MSM.947226
Med Sci Monit 2025; 31:e947226






Abstract
BACKGROUND: Intertrochanteric fractures can be managed using insertion of a proximal femoral nail anti-rotation (PFNA) intramedullary nail inserted into the femur. The helical blade used with the PFNA technique has the advantage of less bone removal and good biomechanical properties, but significant hidden blood loss (HBL) can occur. This study compared postoperative HBL in 219 elderly patients with intertrochanteric fractures using PFNA fixation, stratified by greater trochanter comminution status (comminuted vs non-comminuted).
MATERIAL AND METHODS: We retrospectively analyzed data on 219 elderly patients who underwent PFNA for intertrochanteric fractures between March 2019 and June 2024. The patients were divided into 2 groups: Group A (n=68) with comminuted fractures of the greater trochanter and Group B (n=151) with non-comminuted fractures. Demographic and clinical characteristics of patients were compared. Blood loss was calculated using established formulas. Intraoperative blood loss, postoperative HBL, postoperative complications, and length of hospital stay were statistically analyzed.
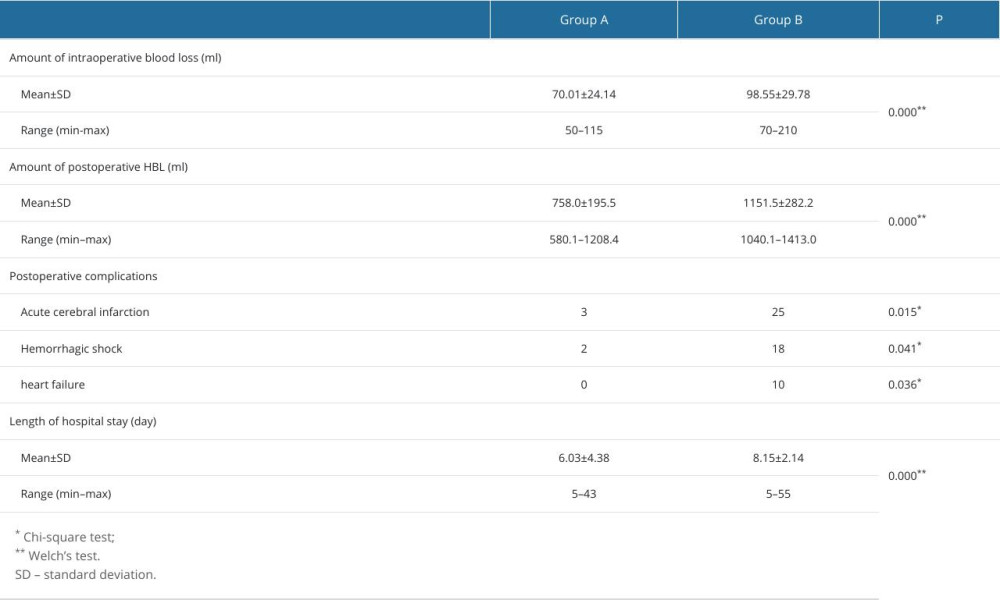
RESULTS: No significant differences were observed in demographic and clinical characteristics between the groups (P>0.05). However, Group A had significantly more intraoperative blood loss (70.0±24.1 ml vs 98.6±29.8 ml, P=0.000) and postoperative HBL (758.0±195.5 ml vs 1151.5±282.2 ml, P=0.000), and longer hospital stays (P=0.000), as well as higher rates of complications, including acute cerebral infarction, hemorrhagic shock, and heart failure (P values 0.015, 0.041, and 0.036, respectively).
CONCLUSIONS: Greater trochanter comminution is associated with significantly elevated HBL in intertrochanteric fractures treated with PFNA fixation. Orthopedic surgeons must recognize this risk factor in perioperative management.
Keywords: Fractures, Comminuted, Blood Loss, Surgical, Fracture Fixation, Intramedullary, proximal femoral fractures, Humans, Female, Male, Retrospective Studies, Hip Fractures, Aged, Bone Nails, Aged, 80 and over, Postoperative Hemorrhage, Postoperative Complications, Femur, Length of Stay, Femoral Fractures
Introduction
Intertrochanteric fracture is a severe and common injury that occurs predominantly in the elderly [1]. Fracture fixation with PFNA is a minimally invasive surgery with a small incision (Figure 1) and minimal intraoperative blood loss [2,3]. However, overall blood loss can be substantially greater than that observed intraoperatively [4]. One study showed that overall blood loss was 1473 mL more than that observed intraoperatively in patients undergoing PFNA for intertrochanteric fractures [5]. There are some reports of significant HBL following the operation [5–7]. The HBL refers to unobserved blood loss occurring during surgical procedures and in the postoperative period, which, although not easily detected, can lead to serious complications. Unfortunately, the HBL is often ignored in patients treated with intramedullary fixations because it is a relatively simple surgical procedure, with short duration of surgery and minimal intraoperative blood loss [8]. Larger amounts of HBL can lead to anemia, hypoproteinemia, and severe complications such as cerebral infarction, delirium, shock, and heart failure, endangering the lives of the elderly [9–13].
In our clinical practice, we have observed that that patients with comminuted fractures of the greater trochanter often have significantly increased postoperative HBL (Figures 2, 3). We hypothesized that a comminuted fracture in the greater trochanter is a major cause of massive postoperative HBL when PFNA is used to treat the femoral intertrochanteric fracture. To test this hypothesis, we retrospectively assessed data on postoperative complications, length of hospital stay, and postoperative HBL of patients undergoing PFNA for intertrochanteric fractures in our hospital over the past 5 years. This study compared postoperative HBL in 219 elderly patients with intertrochanteric fractures using PFNA fixation, stratified by greater trochanter comminution status (comminuted vs non-comminuted).
Material and Methods
ETHICS APPROVAL AND STUDY SUBJECTS:
This study was approved by the Medical Ethics Committee of Lianshui People’s Hospital Affiliated to Kangda College (approval no: 2019–014). All methods were performed in accordance with the Declaration of Helsinki. We retrospectively analyzed date on 219 patients who underwent PFNA for intertrochanteric fractures of the femur between March 2019 and June 2024. Inclusion criteria were: (1) 65< age <89 years, (2) injury caused by low-energy trauma, (3) duration of surgery <60 min, and (5) time between surgery and injury <2 days. Exclusion criteria were: (1) patients with coagulation disorder, and (2) patients who received a blood transfusion due to severe anemia.
STUDY DESIGN:
According to whether there was a comminuted fracture in the greater trochanter of the femur, 219 patients were divided into Group A and Group B. The patients with an intact greater trochanter or those with fractures divided into 2 fragments were assigned to Group A (n=68), while the patients with 3 or more fragments were assigned to Group B (n=151). The height and weight of all patients were recorded preoperatively. Since the patients could not be weighted on a conventional scale, their weight was estimated by the orthopedic surgeon supported by the patients’ own information. Upon admission, all patients received anticoagulant treatment with subcutaneous injections of low-molecular-weight heparin calcium every 12 hours. Anticoagulation treatment was suspended 12 h before surgery.
SURGICAL PROCEDURE:
During the surgery, the patients received intraspinal anesthesia, were placed on a traction operating table, and underwent closed reduction of the fracture under fluoroscopic guidance using a C-arm X-ray machine. The incision was made above the apex of the greater trochanter, approximately 3 cm in length. With the apex of the greater trochanter as the entry point, a guide needle was inserted into the femoral bone marrow cavity. The intramedullary nail was inserted into the medullary cavity along the guidance needle after creating a proximal femoral channel using an electric drill. Under fluoroscopic guidance, a Kirschner wire was drilled below the central axis of the femoral neck. Then, a spiral blade with appropriate length was hammered into the femoral neck along the Kirschner wire. A screw was inserted into the tail of the intramedullary nail to firmly attach the spiral blade to the intramedullary nail. After a screw was drilled into the bilateral cortical bone of the proximal femur through the distal hole of the intramedullary nail, the fracture was fixed with PFNA. No drainage tube was placed in the incision.
HBL MEASURES:
HBL was calculated as follows [10,14]:
Overt blood loss was defined as the intraoperative blood loss (calculated as the liquid in the suction bottle minus the irrigation fluid used during the operation, plus the net weight increase from weighing gauze dressings, etc.) combined with postoperative visible blood loss (wound drainage).
The estimated total blood volume (TBV) was calculated as follows:
Hct0h was the hematocrit (Hct) level at the beginning of the operation, and Hct48h was the patient’s Hct 48 hours after the operation.
OTHER OUTCOME MEASURES:
Various complications were prevented and treated, and anticoagulant treatment resumed 12 hours after surgery. The surgery duration was recorded. Postoperative patients were closely monitored for complications such as shock, acute cerebral infarction, and heart failure. A head CT scan was performed again 24 hours after surgery to compare with preoperative results for acute cerebral infarction.
STATISTICAL ANALYSIS:
Statistical analysis was performed using SPSS version 24.0 software (SPSS, Inc., Chicago, IL, USA). Descriptive data are expressed as mean±standard deviation (SD), median (min-max), or number. The chi-square test was used to compare categorical variables between the groups, while Welch’s
Results
Patients who received blood transfusions after surgery were excluded from the study due to significant impacts on their hemoglobin level results. In Group A, 3 patients were excluded, and in Group B, 12 patients were excluded.
Group A comprised 16 males and 52 females (mean age 76.45±9.77 years; range 63–89), while Group B included 43 males and 108 females (mean age 78.27±11.02 years; range 66–87). No significant intergroup differences were observed in sex distribution (
Hypertension (55.88% vs 50.99%), diabetes mellitus (30.88% vs 32.45%), and old cerebral infarction (26.47% vs 24.50%) were the predominant comorbidities, with no significant intergroup differences observed in hypertension (
The mean operative duration was similar between the 2 groups – 39.91±8.09 minutes (range 23–55) in Group A and 40.24±7.89 minutes (range 20–54) in Group B (
The mean intraoperative blood loss was significantly lower in Group A (70.01±24.14 ml; range 50–115 ml) compared to Group B (98.55±29.78 ml; range 70–210 ml) (
Discussion
The clinical research results showed that the patients with comminuted fractures of the greater trochanter had significantly greater postoperative HBL than those with non-comminuted fractures. Patients with comminuted fractures had significantly higher risks of postoperative acute cerebral infarction, hemorrhagic shock, and heart failure, and a significantly longer average hospital stay, compared to patients with non-comminuted fractures.
Our findings agree with those of Yu et al, who found that PFNA and dynamic hip screw (DHS) techniques result in considerable postoperative HBL when treating geriatric intertrochanteric fractures, with PFNA showing significantly greater HBL compared to DHS [8]. Studies by other scholars have also confirmed that substantial hidden blood loss is frequently associated with PFNA internal fixation following intertrochanteric femoral fractures [4–7]. The primary contributors to high HBL after PFNA fixation of femoral intertrochanteric fractures in elderly patients include: (1) inadequate interstitial fluid return, (2) hemolysis, (3) damage to red blood cells, and (4) ongoing blood loss before and after surgery [15]. Other factors also played significant roles, including the use of anticoagulants, osteoporosis, fracture reduction, and intramedullary penetration, including use of anticoagulant, osteoporosis, fracture reduction, and intramedullary penetration [5,16–19]. However, their analysis did not account for the potential impact of greater trochanter comminution status (whether the fracture was comminuted or not) on the volume of HBL. The present retrospective analysis of 219 cases over the past 5 years found a significant association between comminuted fractures of the greater trochanter and large volumes of postoperative HBL.
Several studies have revealed a close relationship between HBL following intramedullary nailing fixation and the classification of intertrochanteric fractures. The main classification systems for such fractures include the AO and Evans classifications. The results indicate that unstable or advanced types of intertrochanteric fractures are associated with increased HBL [20]. However, our study did not use the aforementioned traditional classification systems but instead focused on the severity of greater trochanteric fractures. Patients with an intact greater trochanter or those with fractures divided into 2 fragments were included in Group A, while patients with 3 or more fragments were included in Group B. According to the Evans classification, Group A included Type I, Type IIB, and reverse intertrochanteric fractures, while Group B included Type IIA and Type III. According to the AO classification, Group A included Types A1, A21, A22, and A3, while Group B included Type A23.
Postoperative acute cerebral infarction is closely related to hypoperfusion of cerebral tissue, often secondary to acute excessive blood loss [21–23]. Hemorrhagic shock and heart failure result directly from acute excessive blood loss [24,25]. Excessive blood loss and acute anemia increase the risk of cardio-cerebrovascular events, which are associated with high mortality rates [26]. The increased average length of hospital stay results from various complications [27]. All of these complications can be caused by massive postoperative HBL. The above results confirmed our hypothesis.
To understand this study’s hypothesis, the local anatomical structure of the femoral trochanter and its pathological manifestations after injury and surgery must be carefully analyzed. The greater trochanter is mainly composed of cancellous bone, which contains a many of tiny blood vessels [28]. Intertrochanteric fractures are a type of metaphyseal fracture with rich blood supply [19]. When a femoral intertrochanteric fracture occurs, the small blood vessels in the cancellous bone are also destroyed [29]. Additionally, the integrity of the cortical bone and surrounding periosteum is damaged, reducing the ability to restrict expansion of the hematoma [30]. During the surgery, the processes of fracture reduction and intramedullary penetration destroy the small blood vessels temporarily blocked by clots, resulting to persistent bleeding [31–33]. The displacement of bone fragments in comminuted fractures is much greater than in non-comminuted fractures [34]. Subsequently, the degree of small-vessel damage inevitably increases with the degree of comminution of the fracture [35]. The blood is more likely to seep into the tissue compartments through the severely injured cortical bone and periosteum, and the pressure inside the hematoma is reduced, making it difficult to stop bleeding. Therefore, the amount of HBL after surgery will naturally increase. A large amount of blood diffuses under the deep fascia and/or within the superficial fascia, leading to the formation of large areas of cyan-purple ecchymosis [36]. The aforementioned are the pathologic basis of massive HBL after PFNA internal fixation for comminuted fracture of the greater trochanter of the femur.
Our study has some limitations to consider. First, the sample size was not large, potentially leading to small deviations in the study results. Second, the degree of osteoporosis in patients was inconsistent, slightly affecting the study results. Third, differences in coagulation function among patients would affect the amount of blood lost after surgery. Fourth, due to concerns about the large impact on the hemoglobin results, the patients receiving blood transfusions due to massive HBL were excluded from the study—3 patients in Group A and 12 patients in Group B were excluded, and their data were not analyzed and compared, resulting in a smaller difference in postoperative HBL between the groups, but this did not affect our conclusion, and in fact supported it. Fifth, the conclusion of this study lacked significant innovation and did not present technical methods for mitigating bleeding. We will conduct further research in the future, enlarge the sample size, and stratify patients based on degree of osteoporosis and coagulation function to narrow the differences between groups and obtain more precise results. Particularly, we will focus on minimizing HBL and addressing complications arising from it. Sixth, due to the inability to accurately measure patients’ height and weight, these values could only be estimated based on the orthopedic surgeon’s clinical experience. This approximation might have introduced variability in the calculated TBV, thereby ultimately affecting the accuracy of HBL determination. Finally, no standard method has been established for measuring intraoperative and postoperative blood loss. Consequently, our evaluation relied on comparison with an established technique rather than against the actual quantity. The assessment of so-called ‘true’ blood loss was limited by methodological constraints.
Conclusions
When PFNA is used for internal fixation of intertrochanteric fractures of the femur, although there are many factors that can lead to massive postoperative HBL, comminuted fractures of the greater trochanter are also a significant factor that cannot be ignored, and the orthopedic team members need to be aware of the risk. Corresponding measures should be taken to decrease blood loss, thereby ensuring perioperative safety of patients.
Figures
 Figure 1. The anterolateral thigh incision for PFNA internal fixation of an intertrochanteric femoral fracture. The incision at the apex of the femoral greater trochanter measures approximately 3 cm in length, while the incision for spiral blade insertion is approximately 1.5 cm long, and the incision for distal locking screw placement is about 1 cm in length.
Figure 1. The anterolateral thigh incision for PFNA internal fixation of an intertrochanteric femoral fracture. The incision at the apex of the femoral greater trochanter measures approximately 3 cm in length, while the incision for spiral blade insertion is approximately 1.5 cm long, and the incision for distal locking screw placement is about 1 cm in length. 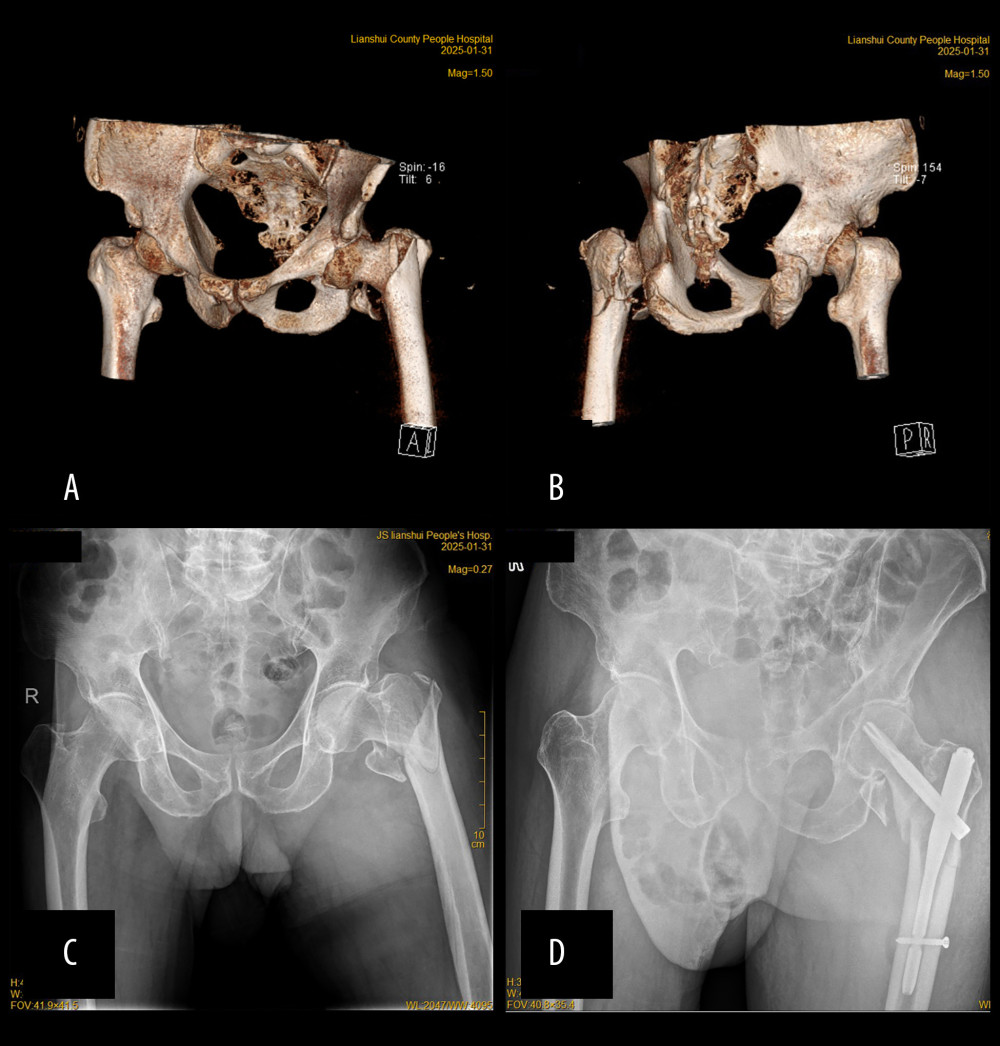 Figure 2. Preoperative and postoperative figure images of an intertrochanteric femoral fracture with comminuted greater trochanter treated with PFNA fixation. (A, B) Preoperative three-dimensional CT imaging; (C) Preoperative X-ray imaging; (D) Postoperative X-ray imaging.
Figure 2. Preoperative and postoperative figure images of an intertrochanteric femoral fracture with comminuted greater trochanter treated with PFNA fixation. (A, B) Preoperative three-dimensional CT imaging; (C) Preoperative X-ray imaging; (D) Postoperative X-ray imaging. 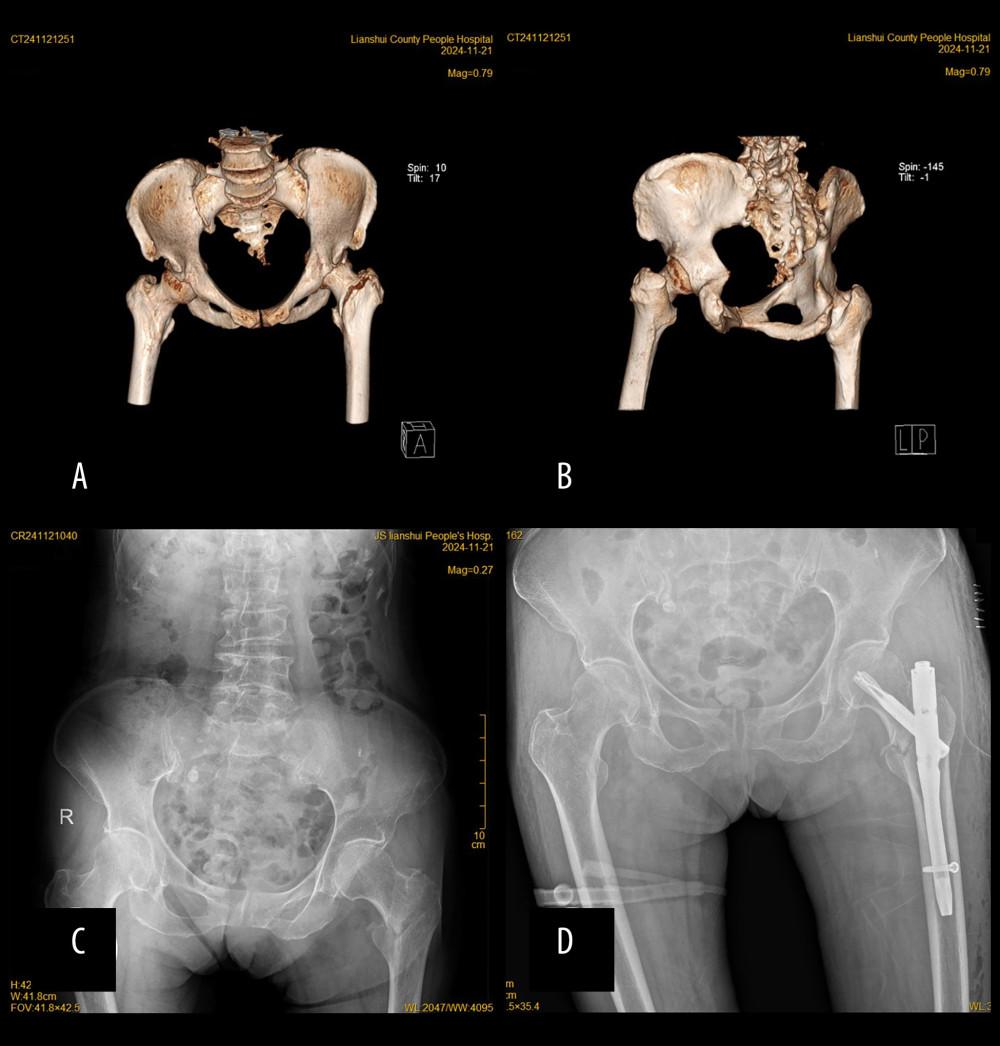 Figure 3. Preoperative and postoperative figure images of an intertrochanteric femoral fracture with non-comminuted greater trochanter treated with PFNA fixation. (A, B) Preoperative three-dimensional CT imaging; (C) Preoperative X-ray imaging; (D) Postoperative X-ray imaging.
Figure 3. Preoperative and postoperative figure images of an intertrochanteric femoral fracture with non-comminuted greater trochanter treated with PFNA fixation. (A, B) Preoperative three-dimensional CT imaging; (C) Preoperative X-ray imaging; (D) Postoperative X-ray imaging. 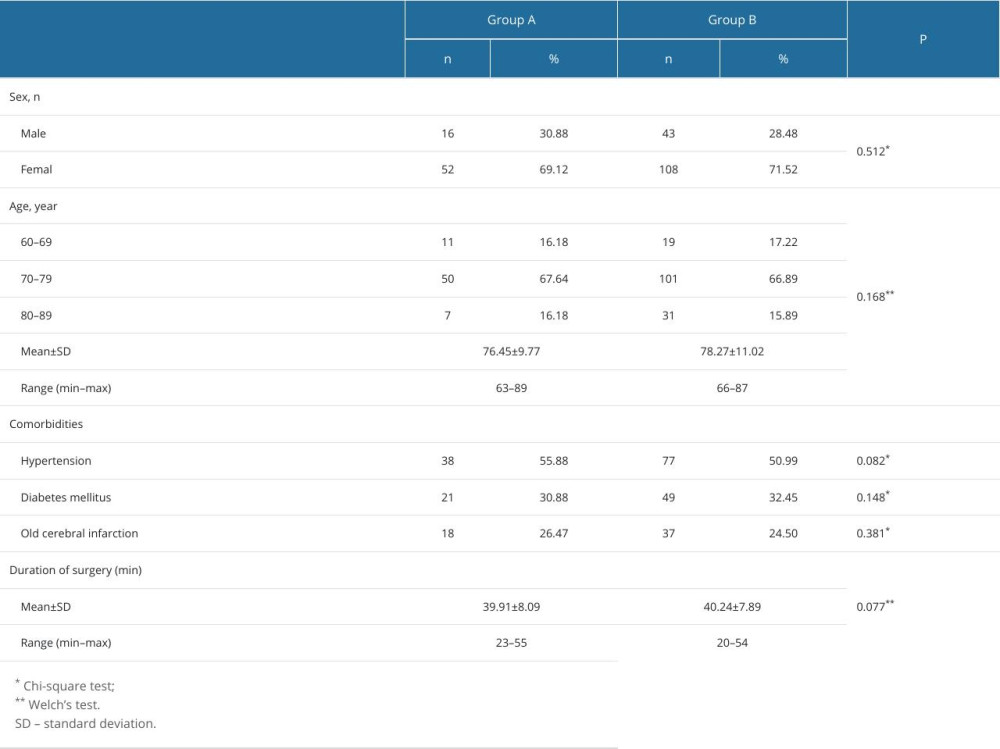
References
1. Polat G, Bayram S, Gökçeoğlu YS, The effect of bone morphology on fracture type and treatment result in patients with intertrochanteric femur fracture aged over 65 years: Ulus Travma Acil Cerrahi Derg, 2022; 28(12); 1731-38
2. Mu W, Zhou J, PFNA-II internal fixation helps hip joint recovery and improves quality of life of patients with lateral-wall dangerous type of intertrochanteric fracture: Biomed Res Int, 2021; 2021; 5911868
3. Hao Z, Wang X, Zhang X, Comparing surgical interventions for intertrochanteric hip fracture by blood loss and operation time: A network meta-analysis: J Orthop Surg Res, 2018; 13(1); 157
4. Lei J, Zhang B, Cong Y, Tranexamic acid reduces hidden blood loss in the treatment of intertrochanteric fractures with PFNA: A single-center randomized controlled trial: J Orthop Surg Res, 2017; 12(1); 124
5. Foss NB, Hidden blood loss after surgery for hip fracture: J Bone Joint Surg Br, 2006; 88(8); 1053-59
6. Zhang C, Chen Z, Wang M, Comparison of clinical outcomes with proximal femoral nail anti-rotation versus dynamic hip screw for unstable intertrochanteric femoral fractures: A meta-analysis: Medicine (Baltimore), 2023; 102(6); e32920
7. Liu Y, Sun Y, Fan L, Perioperative factors associated with hidden blood loss in intertrochanteric fracture patients: Musculoskelet Surg, 2017; 101(2); 139-44
8. Yu W, Zhang X, Wu R, The visible and hidden blood loss of Asia proximal femoral nail anti-rotation and dynamic hip screw in the treatment of intertrochanteric fractures of elderly high- risk patients: A retrospective comparative study with a minimum 3 years of follow-up: BMC Musculoskelet Disord, 2016; 17; 269
9. Yang X, Wu Q, Wang X, Investigation of perioperative hidden blood loss of unstable intertrochanteric fracture in the elderly treated with different intramedullary fixations: Injury, 2017; 48(8); 1848-52
10. Cai L, Wang T, Di L, Comparison of intramedullary and extramedullary fixation of stable intertrochanteric fractures in the elderly: A prospective randomised controlled trial exploring hidden perioperative blood loss: BMC Musculoskelet Disord, 2016; 17(1); 475
11. Tsai CF, Yip PK, Chen CC, Cerebral infarction in acute anemia: J Neurol, 2010; 257(12); 2044-51
12. Xu X, Zhu Q, Yang Y, Investigation of perioperative blood loss of femoral shaft fractures treated with intramedullary nail or locking compression plate: Injury, 2021; 52(7); 1891-96
13. Lu C, Wei X, Li L, Robot-assisted PFNA surgery improves clinical outcomes in the treatment of unstable femoral intertrochanteric fractures in elderly patients compared with traditional PFNA surgery: Sci Rep, 2025; 15(1); 3836
14. Luo XP, Peng J, Zhou L, Intramedullary administration of tranexamic acid reduces bleeding in proximal femoral nail antirotation surgery for intertrochanteric fractures in elderly individuals: A randomized controlled trial: Chin J Traumatol, 2024 [Online ahead of print]
15. Luo G, Liu J, Ni W, The role of post-traumatic antifibrinolysis in the perioperative blood management of elderly patients with intertrochanteric fractures treated with PFNA: A randomised controlled trial: Injury, 2024; 55(12); 111877
16. Jiang W, Shang L, Tranexamic acid can reduce blood loss in patients undergoing intertrochanteric fracture surgery: A meta-analysis: Medicine (Baltimore), 2019; 98(11); e14564
17. Morritt DG, Morritt AN, Kelley SP, Blood ordering protocol based on proposed surgical implant in fractured neck of femur patients: Ann R Coll Surg Engl, 2005; 87(6); 445-48
18. Yu X, Zhang H, Zhang X, Effects of the ratios of marrow cavity diameter to intramedullary nail diameter from different layers on blood loss during perioperative period for femoral intertrochanteric fractures: Medicine (Baltimore), 2019; 98(37); e16936
19. Lou L, Xu L, Wang X, Comprehensive assessment of risk factors and development of novel predictive tools for perioperative hidden blood loss in intertrochanteric femoral fractures: A multivariate retrospective analysis: Eur J Med Res, 2024; 29(1); 626
20. Castaneda-Vega S, Beer-Hammer S, Leiss V: Mol Imaging Biol, 2023; 25(2); 363-74
21. Simonato D, Gaugain S, Le Dorze M, Early cerebral infarction after aneurysmal subarachnoid hemorrhage is associated with prior global cerebral hypoperfusion: World Neurosurg, 2022; 168; e546-e54
22. van Veelen MJ, Brodmann Maeder M, Hypothermia in trauma: Int J Environ Res Public Health, 2021; 18(16); 8719
23. Yu LQ, Meng CC, Jin XS, Clinical study of sodium bicarbonated Ringer’s solution on fluid resuscitation of patients with hemorrhagic shock: Eur Rev Med Pharmacol Sci, 2022; 26(5); 1535-42
24. O’Meara E, Murphy C, McMurray JJ, Anemia and heart failure: Curr Heart Fail Rep, 2004; 1(4); 176-82
25. Wei H, Xiao Q, He J, Effect and safety of topical application of tranexamic acid to reduce perioperative blood loss in elderly patients with intertrochanteric fracture undergoing PFNA: Medicine (Baltimore), 2021; 100(34); e27123
26. Kang Y, Liu J, Chen H, Enhanced recovery after surgery (ERAS) in elective intertrochanteric fracture patients result in reduced length of hospital stay (LOS) without compromising functional outcome: J Orthop Surg Res, 2019; 14(1); 209
27. Cristofolini L, In vitro evidence of the structural optimization of the human skeletal bones: J Biomech, 2015; 48(5); 787-96
28. Cui H, Chen K, Lv S, An analysis of perioperative hidden blood loss in femoral intertrochanteric fractures: Bone density is an important influencing factor: BMC Musculoskelet Disord, 2021; 22(1); 6
29. Rayatdoost F, Grottke O, The use of large animal models in trauma and bleeding studies: Hamostaseologie, 2023; 43(5); 360-73
30. DuBose JJ, Burlew CC, Joseph B, Pelvic fracture-related hypotension: A review of contemporary adjuncts for hemorrhage control: J Trauma Acute Care Surg, 2021; 91(4); e93-e103
31. Cullinane DC, Schiller HJ, Zielinski MD, Eastern Association for the Surgery of Trauma practice management guidelines for hemorrhage in pelvic fracture – update and systematic review: J Trauma, 2011; 71(6); 1850-68
32. Millar NL, Deakin AH, Millar LL, Blood loss following total knee replacement in the morbidly obese: Effects of computer navigation: Knee, 2011; 18(2); 108-12
33. Bulstra AEJ, Al-Dirini RMA, Turow A, The influence of fracture location and comminution on acute scaphoid fracture displacement: Three-dimensional CT analysis: J Hand Surg Eur Vol, 2021; 46(10); 1072-80
34. Dresing KMinimally invasive osteosynthesis of pilon fractures: Oper Orthop Traumatol, 2012; 24(4–5); 368-82 [in German]
35. Heffernan MJ, Lucak T, Igbokwe L, The reverse oblique supracondylar humerus fracture: Description of a novel fracture pattern: J Pediatr Orthop, 2020; 40(2); e131-e37
Figures
Figure 1. The anterolateral thigh incision for PFNA internal fixation of an intertrochanteric femoral fracture. The incision at the apex of the femoral greater trochanter measures approximately 3 cm in length, while the incision for spiral blade insertion is approximately 1.5 cm long, and the incision for distal locking screw placement is about 1 cm in length.Figure 2. Preoperative and postoperative figure images of an intertrochanteric femoral fracture with comminuted greater trochanter treated with PFNA fixation. (A, B) Preoperative three-dimensional CT imaging; (C) Preoperative X-ray imaging; (D) Postoperative X-ray imaging.Figure 3. Preoperative and postoperative figure images of an intertrochanteric femoral fracture with non-comminuted greater trochanter treated with PFNA fixation. (A, B) Preoperative three-dimensional CT imaging; (C) Preoperative X-ray imaging; (D) Postoperative X-ray imaging. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387