15 March 2025: Clinical Research
Evaluating Cardiovascular Risk Factors Among Healthcare Professionals in Iran
Maryam Moshkani Farahani ADE 1, Seyyed Mohammad Saeed Ghiasi BE 1, Maziar Karamali DE 2, Reza Golchin Vafa ABCE 3*
DOI: 10.12659/MSM.947409
Med Sci Monit 2025; 31:e947409






Abstract
BACKGROUND: Cardiovascular disease is a leading cause of morbidity and mortality worldwide, necessitating accurate risk prediction models for effective prevention strategies. This study compares the predictive capabilities of 3 widely used 10-year cardiovascular risk assessment tools – Atherosclerotic Cardiovascular Disease (ASCVD) risk score, Framingham Risk Score (FRS), and Systematic Coronary Risk Evaluation 2 (SCORE2) – in healthcare professionals in Iran.
MATERIAL AND METHODS: This cross-sectional study analyzed data from 222 healthcare professionals at Jamaran Hospital in Tehran, assessing cardiovascular risk profiles using the ASCVD, FRS, and SCORE2 tools. Risk factors included age, sex, dyslipidemia, hypertension, diabetes, obesity, and smoking status. Risk scores were compared to evaluate concordance and classification accuracy across different risk levels.
RESULTS: The prevalence of cardiovascular risk factors was notable: hypertension (30.1%), dyslipidemia (65.7%), diabetes (7.2%), and obesity (24.3%). SCORE2 showed varied distributions of fatal and nonfatal cardiovascular events. ASCVD categorized most participants as low risk (85.6%), with smaller percentages in borderline (6.8%), intermediate (7.2%), and high-risk (0.5%) groups. FRS classified 97.7% as low risk and 2.3% as intermediate risk. Moderate agreement was observed between SCORE2 and ASCVD in moderate-risk (P<0.001, κ=0.43) and high-risk (P=0.007, κ=0.45) regions, with fair agreement between FRS and ASCVD (P<0.001, κ=0.435).
CONCLUSIONS: This study highlights the significant prevalence of cardiovascular risk factors among healthcare professionals in Iran. It emphasizes the need for recalibrating cardiovascular risk models to better reflect Iran’s unique population characteristics, ultimately improving risk prediction accuracy and preventive strategies.
Keywords: Cardiovascular Diseases, Public Health, Humans, Iran, Male, Female, Middle Aged, Cross-Sectional Studies, Health Personnel, adult, Heart Disease Risk Factors, Risk Assessment, Risk Factors, Prevalence, dyslipidemias, Hypertension
Introduction
Cardiovascular diseases (CVDs) are major health problems worldwide, causing a significant number of illnesses and deaths. Nevertheless, CVD fatalities are expected to increase once again because of a growing elderly population and hazardous behaviors [1]. CVDs pose a substantial public health issue in Iran, as well as in many other nations, and contribute to the increasing prevalence of noncommunicable diseases [2]. Examining cardiovascular risk factors is one of the most important steps for lowering the burden of CVD. This assessment is vital for providing information on preventive interventions and maximizing the efficient use of healthcare resources [3,4]. Risk stratification is a process that identifies people with a greater risk of developing certain conditions or diseases. Risk stratification allows for the implementation of personalized preventive measures and treatments [5].
Several cardiovascular risk prediction systems, including the pooled cohort equation and the Framingham risk score (FRS), offer distinct advantages and disadvantages for identifying and treating individuals at high risk [6,7]. The most frequently used risk scores in Iran include the Atherosclerotic Cardiovascular Disease 2013 Risk Calculator (ASCVD), created by the American College of Cardiology and the American Heart Association (AHA/ACC), FRS, and 2019 World Health Organization (WHO) CVD risk prediction charts [8–10]. Although these tools have been demonstrated to be beneficial in assessing CVD risk in Iranian populations, their suitability and precision can vary due to differences in demographic characteristics, frequency of risk factors, and underlying epidemiological patterns [11–13].
The latest European guidelines advise the use of recently revised Systematic Coronary Risk Evaluation (SCORE2) charts to identify apparently healthy people who have an increased risk of developing CVD over the next 10 years. The SCORE2 risk score has been designed to provide an estimation of the probability of experiencing cardiovascular events, including fatal and nonfatal incidents, during a 10-year period. The model takes into account variables, including age, sex, smoking history, cholesterol level, and systolic blood pressure [14–16]. The SCORE2 enhances accuracy by incorporating current data and accounting for variations in risk levels among different European countries while also considering variability within European populations [15].
The SCORE2 is currently receiving praise for its geographical calibration and methodology improvements, which have increased its prediction accuracy in terms of risk [17]. Recent studies have shown that the SCORE2 is more precise in assessing cardiovascular hazards in European populations than is the previous SCORE model. This leads to improved categorization and treatment of risk. The SCORE2 fills an important gap in the prior SCORE model by including nonfatal cardiovascular incidents alongside fatal events, resulting in a more thorough evaluation of risk [18–20]. The SCORE2 generally offers superior performance in assessing cardiovascular illness risk in Europe and helps physicians more precisely implement preventative treatments for patients at increased risk [15].
Despite the high prevalence of CVD in Iran, research on effective risk assessment tools remains limited. Prior studies have demonstrated differences in risk classification among various scoring systems, underscoring the importance of precise risk assessment instruments for successful preventative measures [21–23], especially the recently created SCORE2 model. Its applicability and accuracy in non-European settings, such as Iran, are not well documented. This study, with the goal of optimizing cardiovascular risk assessment in Iran, aims to assess cardiovascular risk among Jamaran Hospital staff via the use of the FRS, ASCVD, and SCORE2 risk scores in 222 healthcare professionals. By comparing these 3 risk assessment tools, we seek to determine the frequency of individuals classified as high risk and the concordance between different scoring systems.
Material and Methods
ETHICAL CONSIDERATIONS:
This study was approved by the Ethics Committee of Baqiyatallah University of Medical Sciences, under approval number IR.BMSU.BAQ.REC.1402.078. All participants provided written informed consent to participate in the study. The study adhered to the ethical guidelines outlined by the Declaration of Helsinki.
STUDY DESIGN:
We conducted this comparative cross-sectional study at Jamaran Hospital in Tehran, Iran. The study population consisted of hospital staff, including physicians, nurses, administrative personnel, and support staff. Individuals employed at Jamaran Hospital, aged between 40 and 75 years, who expressed a willingness to participate in the research met the inclusion criteria. To concentrate on primary prevention, we excluded people with a documented history of CVD. We included all eligible staff in the study to ensure comprehensive representation. This approach facilitated a thorough evaluation of cardiovascular risk across diverse occupational groups within the hospital.
DATA COLLECTION:
Data collection occurred over a 6-month period from January to June 2024. Each participant underwent a comprehensive cardiovascular risk assessment, which included a structured questionnaire and physical examination. To ensure the accuracy of the data, the questionnaires were completed by a general physician. The questionnaire collected detailed information on demographic data (age, sex), medical history (hyperlipidemia, hypertension, diabetes mellitus, lifestyle factors (smoking status), and family history of CVD. Physical examinations were used to measure blood pressure, height, weight, and body mass index (BMI). We collected blood samples to determine lipid profiles, which included triglycerides, low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein (HDL-C) cholesterol, and total cholesterol levels.
A medical doctor conducted blood pressure assessments on participants’ right arms while seated, preceded by a 5-min rest period, via an electronic blood pressure monitor. We obtained 2 successive readings, ensuring a 3-min gap between them. If there was a difference of more than 10 mmHg or 5 mmHg between the systolic and diastolic values, we conducted a third measurement and chose the 2 readings that were closest in value for further investigation. We subsequently computed the average systolic and diastolic blood pressures from the aforementioned pair of measurements. Furthermore, the doctor recorded the weight and height of each participant. We conducted cardiovascular risk assessment for each participant via 3 established methodologies: the FRS, ASCVD risk calculator, and SCORE2.
DEFINITIONS AND CRITERIA:
The 2023 European Society of Hypertension recommendations classifying hypertension into distinct stages. Grade 1 hypertension is characterized by a systolic blood pressure (SBP) ranging from 140 to 159 mmHg or a diastolic blood pressure (DBP) ranging from 90 to 99 mmHg. Grade 2 hypertension is defined as an SBP ranging from 160 to 179 mmHg or a DBP ranging from 100 to 109 mmHg. An SBP higher than 180 mmHg or a DBP higher than 110 mmHg indicates grade 3 hypertension. Hypertension in the third grade requires immediate medical intervention [24].
According to recent guidelines from the European Society of Cardiology, dyslipidemia is defined as an aberrant lipid profile characterized by decreased levels of HDL-C and/or increased levels of total cholesterol, LDL-C, and triglycerides [27]. We considered any total cholesterol level of 240 mg/dL or higher to be abnormal, in addition to triglyceride levels of 200 mg/dL or higher, LDL-C levels of 130 mg/dL or higher, and HDL-C values of 40 mg/dL or lower for men and 50 mg/dL or lower for women [25,26].
The American Diabetes Association guidelines classify diabetes as blood sugar levels of 126 mg/dL or greater when fasting, 200 mg/dL or higher during a 2-h oral glucose tolerance test, or 6.5% or higher when hemoglobin A1c is measured [27]. Smokers are defined as individuals who have smoked cigarettes, water pipes, or pipes within the previous 30 days at the time of evaluation [28]. According to the World Health Organization (WHO), weight categories are defined as follows: people with underweight have a BMI below 18.5 kg/m2, those with normal weight have a BMI in the range of 18.5 to 24.9 kg/m2, those with overweight have a BMI in the range of 25.0 to 29.9 kg/m2, and those with obesity have a BMI of 30 kg/m2 or higher [29]. A positive family history of CVD is defined as CVD occurring in first-degree relatives who develop CVD before the age of 55 years for men and 65 years for women [30].
RISK ASSESSMENT TOOLS:
For each participant, we estimated their 10-year risk of cardiovascular events via 3 different tools.
SCORE2: The SCORE2 program calculates the 10-year risk of cardiovascular events, including fatal and nonfatal events. We input data such as sex, age, SBP, smoking status, and total cholesterol and HDL-C levels into the model. We delineate risk categories in participants under 50 years of age as follows: we classify a risk of less than 2.5% as low to moderate, risk between 2.5% and 7.5% as high, and risk of 7.5% or higher as very high. For individuals aged 50 to 69 years, we classify a risk below 5% as low to moderate, risk between 5% and 10% as high, and risk of 10% or higher as very high [15]. Iran does not fall within the predefined risk regions of SCORE2; therefore, we applied each risk category (from low to very high) comprehensively to each individual to measure the cardiovascular risk profile of the study population.
ASCVD RISK CALCULATOR: We used the ASCVD risk calculator to calculate the risk of developing atherosclerotic cardiovascular events over a period of 10 years. The variables used as inputs in the model were age, race, sex, total cholesterol, HDL-C, SBP, hypertension treatment status, diabetes status, and smoking status. We categorized participants on the basis of their 10-year probability of cardiovascular events, classifying a probability below 5% as low risk and a probability between 5% and 7.4% as borderline. We classified individuals with a risk between 7.5% and 19.9% as having an intermediate level of risk. Finally, a risk exceeding 20% indicated a high-risk classification [31].
FRS: We used the FRS to compute the probability of experiencing cardiovascular events, specifically coronary heart disease, over a period of 10 years. The model incorporated sex, age, smoking status, SBP, HDL-C, and total cholesterol levels as input variables. This established risk assessment technique offers useful insights into predicting cardiovascular risk. Individuals classified as low risk have a 10-year probability of developing cardiovascular disease that is 10% or less. On the other hand, individuals labeled as intermediate risk have a 10-year probability ranging from 10% to 20%. Individuals classified as high risk have a 10-year probability of having a cardiovascular disease of 20% or greater [9].
STATISTICAL ANALYSIS:
We conducted the data analysis via SPSS software version 26.0. We summarized the demographic and clinical characteristics of the research population via descriptive statistics. The mean and standard deviation (SD) were used to describe continuous variables, whereas frequencies and percentages were used to describe categorical variables.
The primary outcome of the study centered on assessing the 10-year risk for CVDs predicted by the FRS, ASCVD, and SCORE2 tools. Comparative analysis encompassed 2 main aspects. First, we examined the categorization of risk levels according to the SCORE2, ASCVD, and FRS. Second, we conducted an evaluation of the concordance between the risk categories generated by these 3 tools via the Cohen kappa statistic. To compare risk scores, we categorized ASCVD risk as low (below 7.5%) or high (above 7.5%). Similarly, we classified SCORE2 risk as low (below 2.5%) or high (above 2.5%) for individuals under 50 years of age and low (below 5%) or high (above 5%) for those over 50 years of age. We also divided FRSs into low-risk (below 10%) and high-risk (above 10%) groups.
Results
DEMOGRAPHIC DATA:
The study involved a total of 222 healthcare practitioners. The study consisted of 162 male participants, accounting for 73% of the total, and 60 female participants, accounting for 27%. The average age of the participants was 46.51±8 years. The mean employment experience was 18.91±7 years.
CARDIOVASCULAR RISK FACTORS:
The average SBP and DBP of the participants were 123±12.2 and 78.1±9.4, respectively. The hypertension prevalence was 67 (30.1%), with 11 (4.9%) having known hypertension, 31 (13.9%) having newly elevated BP, 24 (10.8%) with newly diagnosed grade 1 hypertension, and 1 (0.4%) with recently diagnosed grade 2 hypertension. A total of 146 participants (65.7%) had dyslipidemia, with 1 prior diagnosis (0.4%), 127 new cases of abnormal HDL (57.2%), 37 new cases of abnormal LDL (16.6%), 14 new cases of abnormal triglycerides (6.3%), and 1 new case of abnormal total cholesterol (0.4%). Diabetes was present in 16 participants (7.2%), including 9 (4%) with previously diagnosed diabetes and 7 (3.1%) with newly diagnosed diabetes. Furthermore, the study identified 27 individuals (12.1%) as prediabetic. In this study, the prevalence of current smokers was 21 (9.4%). The prevalence of a positive CVD family history was 7 (3.1%). The BMI categories revealed that 0.9% of the participants had underweight, 25.2% had normal weight, 48.6% had overweight, and 24.3% had obesity (Table 1).
CARDIOVASCULAR RISK ASSESSMENT:
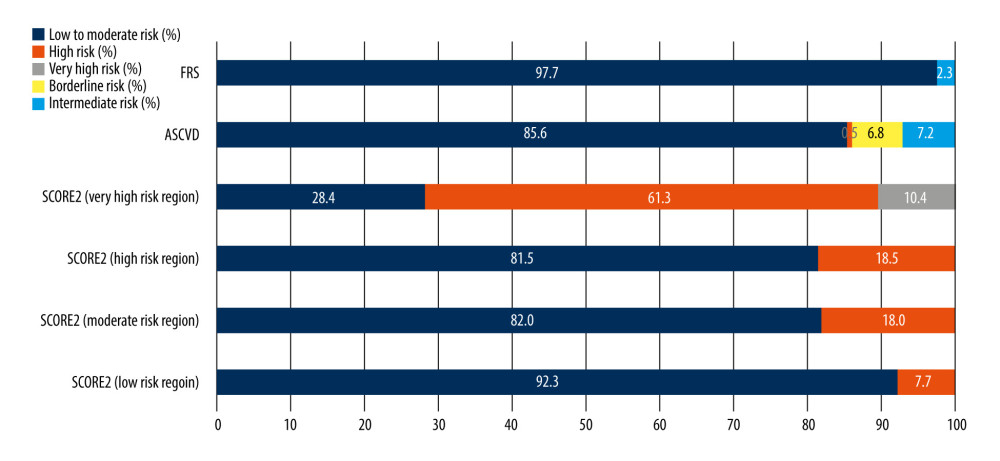
We used the SCORE2, ASCVD, and FRS tools to evaluate the probability of experiencing cardiovascular events during a 10-year period (Table 2, Figure 1). Each risk score was applied based on standard guidelines. We acknowledge the lack of recalibration, which can influence risk classification accuracy; however, this provides a baseline comparison for future recalibrated models.
The SCORE2 tool, modified for 4 risk regions, revealed participants’ different 10-year cardiovascular event distributions. The low-risk region chart classified participants into low- to moderate-risk (92.3%) and high-risk (7.7%) groups. The moderate-risk region chart classified 82% of the participants as low- to moderate-risk and 18% as high-risk. The high-risk region chart classified 81.5% of the participants as low- to moderate-risk and 18.5% as high-risk. Finally, in the very high-risk region chart, 28.4% of the regions were classified as low to moderate risk, 61.3% as high risk, and 10.4% as very high risk.
The ASCVD risk calculator classified the majority of participants, 190 (85.6%), as having low risk, followed by 15 (6.8%) as having borderline risk, 16 (7.2%) as having intermediate risk, and 1 (0.5%) as having high risk. Using the FRS, 217 participants (97.7%) were categorized as having low risk, whereas 2 (2.3%) were categorized as having intermediate risk.
CONCORDANCE ANALYSIS:
The results showed that the ASCVD and the SCORE2 moderate-risk region charts agreed at a moderate level (κ=0.43, 95% CI 0.29–0.59, P<0.001), suggesting a reasonable level of consistency in assessing cardiovascular risk. Moreover, there was moderate agreement between the ASCVD and SCORE2 high-risk region charts (κ=0.45, 95% CI 0.29, 0.61, P=0.007). However, the study revealed poor agreement between the SCORE2 very high-risk region and the ASCVD risk score, with a kappa coefficient of 0.06 (95% CI 0.03, 0.09, P=0.007). Additionally, there was only a slight improvement in agreement between the SCORE2 low-risk region and the ASCVD risk score, with a kappa coefficient of 0.236 (95% CI 0.02, 0.44, P<0.001). This finding indicated that there were still considerable discrepancies in the classification of low-risk individuals between the 2 scoring systems (Table 3).
Furthermore, the study revealed slight agreement between the FRS and SCORE2 risk regions. The kappa coefficients for the FRS and SCORE2 were as follows: low-risk region (κ=0.152, 95% CI −0.06, 0.36,
Discussion
LIMITATIONS:
Despite being the first study to assess the SCORE2 tool in Iran and providing comprehensive insights into cardiovascular risk among healthcare professionals, this study had some limitations. The use of a cross-sectional design limited our capacity to determine cause-and-effect linkages. To confirm these findings, longitudinal research is essential. In addition, the study was conducted exclusively at a solitary hospital in Tehran, Iran, which can restrict the applicability of the findings to more diverse populations. Finally, without recalibrating the SCORE2 tool to match Iran’s specific cardiovascular baseline, there may be an overestimation or underestimation of actual risk levels. Further studies with recalibrated models, larger sample sizes, and broader regional representation would strengthen the reliability of cardiovascular risk predictions for diverse populations across Iran.
Conclusions
In conclusion, this study highlights the significant burden of cardiovascular risk factors among healthcare professionals in Iran, with a notable prevalence of hypertension, dyslipidemia, and obesity. The use of 3 widely recognized cardiovascular risk assessment tools – SCORE2, ASCVD, and FRS – revealed varying levels of agreement in risk classification, emphasizing the need for population-specific recalibration. While the SCORE2 demonstrated better concordance in moderate- and high-risk regions, the differences in risk stratification underscore the importance of tailoring cardiovascular risk models to the unique risk profile of the Iranian population. The findings suggest that recalibration of these models could enhance the accuracy of cardiovascular risk prediction, ultimately improving preventive strategies and health outcomes. Future research should focus on optimizing these tools for Iran’s specific demographic and health characteristics to support more targeted interventions and effective risk management strategies.
Tables
Table 1. Baseline demographic data of the participants. Table 2. The 10-year risk of cardiovascular events using the Framingham Risk Score (FRS), Systematic Coronary Risk Evaluation 2 (SCORE2), and Atherosclerotic Cardiovascular Disease (ASCVD) tools.
Table 2. The 10-year risk of cardiovascular events using the Framingham Risk Score (FRS), Systematic Coronary Risk Evaluation 2 (SCORE2), and Atherosclerotic Cardiovascular Disease (ASCVD) tools. Table 3. Concordance analysis of cardiovascular risk assessment tools.
Table 3. Concordance analysis of cardiovascular risk assessment tools.
References
1. Roth GA, Mensah GA, Johnson COGBD-NHLBI-JACC Global Burden of Cardiovascular Diseases Writing Group, Global burden of cardiovascular diseases and risk factors, 1990–2019. Update from the GBD 2019 study: J Am Coll Cardiol, 2020; 76(25); 2982-3021 [Erratum in: J Am Coll Cardiol. 2021;77(15):1958–59]
2. GBD 2019 Iran Collaborators, Health system performance in Iran: A systematic analysis for the Global Burden of Disease Study 2019: Lancet, 2022; 399(10335); 1625-45
3. Rippe JM, Lifestyle strategies for risk factor reduction, prevention, and treatment of cardiovascular disease: Am J Lifestyle Med, 2018; 13(2); 204-12
4. Erhardt L, Moller R, Puig JG, Comprehensive cardiovascular risk management – what does it mean in practice?: Vasc Health Risk Manag, 2007; 3(5); 587-603 [Erratum in: Vasc Health Risk Manag. 2008;4(3):741]
5. Björnson E, Borén J, Mardinoglu A, Personalized cardiovascular disease prediction and treatment – a review of existing strategies and novel systems medicine tools: Front Physiol, 2016; 7; 2
6. Anderson KM, Odell PM, Wilson PW, Kannel WB, Cardiovascular disease risk profiles: Am Heart J, 1991; 121(1 Pt 2); 293-98
7. Sofogianni A, Stalikas N, Antza C, Tziomalos K, Cardiovascular risk prediction models and scores in the era of personalized medicine: J Pers Med, 2022; 12(7); 1180
8. Emamian MH, Hashemi H, Fotouhi A, Predicted 10-year risk of cardiovascular disease in the Islamic Republic of Iran and the body mass index paradox: East Mediterr Health J, 2020; 26(12); 1465-72
9. D’Agostino RB, Vasan RS, Pencina MJ, General cardiovascular risk profile for use in primary care: The Framingham Heart Study: Circulation, 2008; 117(6); 743-53
10. WHO CVD Risk Chart Working Group, World Health Organization cardiovascular disease risk charts: Revised models to estimate risk in 21 global regions: Lancet Glob Health, 2019; 7(10); e1332-e45 Erratum in: Lancet Glob Health. 2023;11(2):e196
11. Meysamie A, Salarvand F, Khorasanizadeh M, Cardiovascular risk assessment by FRS and SCORE in Iranian adult population: J Diabetes Metab Disord, 2017; 16; 35
12. Azizi F, Rahmani M, Emami H, Cardiovascular risk factors in an Iranian urban population: Tehran lipid and glucose study (phase 1): Soz Praventivmed, 2002; 47(6); 408-26
13. Hasani-Ranjbar S, Razmandeh R, Ghodssi-Ghassemabadi R, Comparison of Framingham Cardiovascular Risk Criteria and ASCVD Score in Iranian Obese Patients: Iran J Public Health, 2023; 52(2); 420-26
14. Visseren FLJ, Mach F, Smulders YMESC National Cardiac Societies; ESC Scientific Document Group, 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: Eur Heart J, 2021; 42(34); 3227-37 Erratum in: Eur Heart J. 2022;43(42):4468
15. SCORE2 working group and ESC Cardiovascular risk collaboration, SCORE2 risk prediction algorithms: New models to estimate 10-year risk of cardiovascular disease in Europe: Eur Heart J, 2021; 42(25); 2439-54
16. SCORE2-OP working group and ESC Cardiovascular risk collaboration, SCORE2-OP risk prediction algorithms: Estimating incident cardiovascular event risk in older persons in four geographical risk regions: Eur Heart J, 2021; 42(25); 2455-67
17. , SCORE2-Diabetes: 10-year cardiovascular risk estimation in type 2 diabetes in Europe: Eur Heart J, 2023; 44(28); 2544-56
18. Barkas F, Sakkou S, Styla C, Clinical application of the new cardiovascular risk prediction algorithms SCORE2 and SCORE2-OP in patients with dyslipidemia: Eur J Prevent Cardiol, 2022; 29(Suppl 1); zwac056.142
19. Popova K, Zhukov A, Troschanskiy D, NEWS2 score in the practice of infectious diseases hospital in COVID-19 patients: Implementation and results, 2021
20. Quevedo-Abeledo JC, González-Gay MÁ, Ferraz-Amaro I, SCORE2 versus SCORE in patients with systemic lupus erythematosus: Ther Adv Musculoskelet Dis, 2022; 14; 1759720X221092373
21. Zibaeenejad F, Mohammadi SS, Sayadi M, Ten-year atherosclerosis cardiovascular disease (ASCVD) risk score and its components among an Iranian population: A cohort-based cross-sectional study: BMC Cardiovasc Disord, 2022; 22(1); 162
22. Tolou H, Arsalan S, Salman N, Comparison between ASCVD versus WHO risk score in predicting of 10-year cardiovascular risk in an Iranian adult: A hospital-based cross-sectional study: Acta Medica Iranica, 2022; 60(1); 56-61
23. Jahangiry L, Dehghan A, Farjam M, Laboratory-based and office-based Globorisk scores to predict 10-year risk of cardiovascular diseases among Iranians: Results from the Fasa PERSIAN cohort: BMC Med Res Methodol, 2022; 22(1); 305 [Erratum in: BMC Med Res Methodol. 2022;22(1):315]
24. Mancia G, Kreutz R, Brunström M, 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension: Endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA): J Hypertens, 2023; 41(12); 1874-2071 [Erratum in: J Hypertens. 2024;42(1):194]
25. Jellinger PS, Handelsman Y, Rosenblit PD, American Association of Clinical Endocrinologists and American College of Endocrinology guidelines for management of dyslipidemia and prevention of cardiovascular disease: Endocr Pract, 2017; 23(Suppl 2); 1-87
26. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults, Executive summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III): JAMA, 2001; 285(19); 2486-97
27. Muntner P, Whelton PK, Woodward M, Carey RM, A Comparison of the 2017 American College of Cardiology/American Heart Association Blood Pressure Guideline and the 2017 American Diabetes Association Diabetes and Hypertension Position Statement for U.S. Adults with diabetes: Diabetes Care, 2018; 41(11); 2322-29
28. Solberg LI, Asche SE, Boyle R, Smoking and cessation behaviors among young adults of various educational backgrounds: Am J Public Health, 2007; 97(8); 1421-26
29. , Obesity: Preventing and managing the global epidemic. Report of a WHO consultation: World Health Organ Tech Rep Ser, 2000; 894; i-xii
30. Allport SA, Kikah N, Abu Saif N, Parental age of onset of cardiovascular disease as a predictor for offspring age of onset of cardiovascular disease: PLoS One, 2016; 11(12); e0163334
31. Goff DC, Lloyd-Jones DM, Bennett GAmerican College of Cardiology/American Heart Association Task Force on Practice Guidelines, 2013 ACC/AHA guideline on the assessment of cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines: Circulation, 2014; 129(25 Suppl 2); S49-73 [Erratum in: Circulation. 2014;129(25 Suppl. 2):S74–75]
32. Rezaei F, Seif M, Fattahi MR, Estimation of 10-year risk of cardiovascular diseases using WHO risk prediction charts: A population-based study in Southern Iran: Iran J Public Health, 2022; 51(7); 1667-76
33. Mirjalili SR, Marques-Vidal P, Kraemer A, Epidemiology of coronary heart disease risk factors in central Iran: A 10-year cohort study, 2023
34. Ostad AN, Dehnavi Z, Farshidi H, Food intake pattern and cardiovascular risk factors in patients with premature coronary artery disease in Iran: J Nutr Food Secur, 2022; 7(4); 525-35
35. Rezaianzadeh A, Moftakhar L, Seif M, Incidence and risk factors of cardiovascular disease among population aged 40–70 years: A population-based cohort study in the South of Iran: Trop Med Health, 2023; 51(1); 35
36. Saki N, Karandish M, Cheraghian B, Prevalence of cardiovascular diseases and associated factors among adults from southwest Iran: Baseline data from Hoveyzeh Cohort Study: BMC Cardiovasc Disord, 2022; 22(1); 309
37. Molani Gol R, Rafraf M, Asghari Jafarabadi M, Evaluation of cardiovascular risk factors in women referring to health centers in Tabriz, Iran, 2017: Health Promot Perspect, 2018; 8(4); 315-22
38. Rabani S, Sardarinia M, Akbarpour S, 12-year trends in cardiovascular risk factors (2002–2005 through 2011–2014) in patients with cardiovascular diseases: Tehran lipid and glucose study: PLoS One, 2018; 13(5); e0195543
39. Eslami A, Lotfaliany M, Akbarpour S, Trend of cardiovascular risk factors in the older Iranian population: 2002–2014: Geriatr Gerontol Int, 2018; 18(1); 130-37
40. Malekzadeh H, Lotfaliany M, Ostovar A, Trends in cardiovascular risk factors in diabetic patients in comparison to general population in Iran: Findings from National Surveys 2007–2016: Sci Rep, 2020; 10(1); 11724
41. Sadeghi T, Soltani N, Jamali Z, The prevalence and associated factors of overweight/obesity and abdominal obesity in South-Eastern of Iran: A cross-sectional study based on Rafsanjan cohort study: BMC Pub Health, 2023; 23(1); 861
42. Mokhtari M, Khalil D, Farzadfar F, The burden of cardiovascular disease attributable to modifiable risk factors and cost-effectiveness analysis of IraPEN Program in the General Population of Iran: Med J Islam Repub Iran, 2022; 36; 73
43. Ghorashi SM, Ahmadi P, Shahnazar Nezhad Khalesi R, Association between nontraditional risk factors and calculated 10-year risk of atherosclerotic cardiovascular disease in a large general population: Based on the Pars Cohort Study: J Tehran Heart Cent, 2023; 18(1); 24-32
44. Mirzaei M, Mirzaei M, Agreement between Framingham, IraPEN and non-laboratory WHO-EMR risk score calculators for cardiovascular risk prediction in a large Iranian population: J Cardiovasc Thorac Res, 2020; 12(1); 20-26
45. Rezaei F, Seif M, Gandomkar A, Agreement between laboratory-based and non-laboratory-based Framingham risk score in Southern Iran: Sci Rep, 2021; 11(1); 10767
46. Sepehrinia M, Pourmontaseri H, Sayadi M, Comparison of atherosclerotic cardiovascular disease (ASCVD) and Framingham risk scores (FRS) in an Iranian population: Int J Cardiol Cardiovasc Risk Prev, 2024; 21; 200287
47. Song Y, Skinner J, Bynum J, Regional variations in diagnostic practices: New Engl J Med, 2010; 363(1); 45-53
48. Nicolaides AN, Griffin M, Panayiotou AG, Performance of SCORE2 and SCORE2-OP risk algorithms in a Cypriot cohort: Int Angiol, 2022; 41(6); 492-99
49. van Trier TJ, Snaterse M, Boekholdt SM, Validation of Systematic Coronary Risk Evaluation 2 (SCORE2) and SCORE2-Older Persons in the EPIC-Norfolk prospective population cohort: Eur J Prev Cardiol, 2024; 31(2); 182-89
50. Quintal J, Candjondjo A, Rato Q, Differences in 10-year cardiovascular risk estimation using SCORE and SCORE2 risk prediction tools: a moderate risk country population analysis: Eur J Prevent Cardiol, 2023; 30(Suppl 1); zwad125.330
51. Van Trier T, Snaterse M, Boekholdt M, Performance of the Systematic COronary Risk Evaluation 2 (SCORE2) in the EPIC-Norfolk prospective population study: Eur J Prevent Cardiol, 2023; 30(Suppl 1); zwad125.325
Tables
Table 1. Baseline demographic data of the participants.Table 2. The 10-year risk of cardiovascular events using the Framingham Risk Score (FRS), Systematic Coronary Risk Evaluation 2 (SCORE2), and Atherosclerotic Cardiovascular Disease (ASCVD) tools.Table 3. Concordance analysis of cardiovascular risk assessment tools.Table 1. Baseline demographic data of the participants.Table 2. The 10-year risk of cardiovascular events using the Framingham Risk Score (FRS), Systematic Coronary Risk Evaluation 2 (SCORE2), and Atherosclerotic Cardiovascular Disease (ASCVD) tools.Table 3. Concordance analysis of cardiovascular risk assessment tools. In Press
Clinical Research
Association Between Total Cholesterol–to–High-Density Lipoprotein Ratio and Gestational Hypertension: A Cas...Med Sci Monit In Press; DOI: 10.12659/MSM.952395
Review article
Clinical Use of Endotracheal Intubation Without Neuromuscular Blockade: The Current Stage of KnowledgeMed Sci Monit In Press; DOI: 10.12659/MSM.951765
Clinical Research
Effect of Dexmedetomidine Hydrochloride Nasal Spray on Anxiety and Sleep in Patients Undergoing Gynecologic...Med Sci Monit In Press; DOI: 10.12659/MSM.952465
Clinical Research
Prognostic Value of Mortality Scoring Systems in Patients With Severe Burns: Identifying Key Predictors of ...Med Sci Monit In Press; DOI: 10.12659/MSM.951713
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,173
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,757,769
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,143
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,797
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387