08 July 2025: Clinical Research
Evaluation of Knee Anatomical Parameters in Posterior Horn Medial Meniscus Injuries Using MRI
Gengshuang Tian ABCDEF 1*, Jiasu Wang ABCDEF 1, Menghao Wu ABE 2, Yubo Liu ABCDF 1
DOI: 10.12659/MSM.948366
Med Sci Monit 2025; 31:e948366






Abstract
BACKGROUND: Meniscus injuries, particularly posterior horn injuries of the medial meniscus are common. This study compared the anatomical parameters on magnetic resonance imaging (MRI) of the posterior horn of the medial meniscus of the knee joint in 43 patients with medial meniscus injury with 54 uninjured knee joints.
MATERIAL AND METHODS: We retrospectively analyzed data from 97 patients (43 with medial meniscus injury and 54 controls) who presented with knee pain without a history of trauma from 2021 to 2022. We assessed and compared various knee anatomical parameters through quantitative measurements on MRI images, including the posterior condylar angle (PCA), the angle between the posterior tangent of the distal femoral shaft and the transepicondylar axis (PTFS-TEA), the ratio of medial femoral condyle length to medial tibial plateau length at knee extension (MFL/MTL), medial and lateral tibial slopes (MTS and LTS), the difference between MTS and LTS (MTS-LTS), the anatomical medial proximal tibia angle (aMPTA), the anatomical lateral distal femoral angle (aLDFA), and the distal condylar angle (DCA).
RESULTS: Our analysis revealed no statistically significant differences in the knee anatomical parameters assessed between the study group and the control group (P>0.05), including PCA, PTFS-TEA, MFL/MTL, MTS, LTS, MTS-LTS, aMPTA, aLDFA, and DCA. Further analysis by sex also showed no significant differences (P>0.05).
CONCLUSIONS: The assessed knee geometric parameters do not appear to be risk factors for non-traumatic posterior horn injuries of the medial meniscus.
Keywords: Knee, meniscus, Anatomists, Humans, Male, Magnetic Resonance Imaging, Female, adult, Tibial Meniscus Injuries, Retrospective Studies, Knee Joint, Middle Aged, Menisci, Tibial, Femur, Knee Injuries, Tibia, young adult
Introduction
The meniscus provides load distribution and shock absorption in the knee joint and can withstand up to 45% of the knee joint load [1,2]. In the medial compartment of the knee joint, the posterior horn of the medial meniscus bears most of the stress [3]. The meniscus also lubricates and protects articular cartilage [2]. However, meniscal tears are common, with an incidence of 61 per 100 000 in the United States general population and 8.7 per 1000 in active-duty military personnel. Medial meniscus tears are more common than lateral ones, especially in the posterior horn, which accounts for 27.8% of medial meniscus injuries. Diagnosis relies on history, physical exam, and MRI. Treatment includes conservative management with RICE and medications for mild cases, and surgery for severe or persistent cases [4–6]. There was no clear history of trauma or other knee disorders in these patients, many of whom were young. This suggests that there may be other factors that cause meniscus injuries that remain to be found.
Previous studies have identified age, sex, body mass index, and exercise style as significant risk factors for posterior horn tears of the medial meniscus [5,7]. While one study proposed that common Asian postures, such as the lotus position or squatting, might contribute to these tears, subsequent research has not supported this hypothesis [7,8]. In recent years, the role of anatomical parameters in knee biomechanics has been a focus of attention. The slope of the tibial plateau in particular has been shown to significantly affect knee joint rotation, femur and tibia motion, and anterior cruciate ligament (ACL) injury [1,9,10]. However, the relationship between tibial plateau slope and meniscus injury remains a matter of debate. Lee et al [11] found a significantly higher incidence of medial meniscus injury in patients with posterior tibial slope (PTS) ≥13° and in patients with ACL dysfunction. In contrast, ElMansori et al [12,13] observed that patients with meniscus injuries had a higher lateral tibial slope compared to those without meniscus injuries among the ACL-injured population, but they did not find a correlation between medial tibial slope (MTS) and medial meniscal injury. Additionally, other studies have indicated that MRI and arthroscopy have only minimal to moderate utility in detecting and diagnosing the location, region, and morphology of meniscal injuries in patients with ACL tears, suggesting caution when using MRI alone for diagnosis [14]. Most relevant studies have involved patients with ACL injuries, with fewer studies focusing exclusively on meniscal injuries [1,15].
PTS is one of the frequently mentioned anatomical structures that can lead to ACL injury or meniscus injury, and the geometry of the distal femur, such as its distal rotation, is often measured to guide prosthetic installation in total knee replacement [16], but the association between the distal rotation of the femur and meniscus injury is rarely mentioned. To the best of our knowledge, this study is the first to investigate the relationship between distal femoral rotation and non-traumatic posterior horn injuries of the medial meniscus.
Therefore, this study compared the anatomical parameters on magnetic resonance imaging (MRI) of the posterior horn of the medial meniscus of the knee joint in 43 patients with medial meniscus injury with 54 uninjured knee joints. The parameters assessed included the posterior condylar angle (PCA), the angle between the posterior tangent of the distal femoral shaft and the transepicondylar axis (PTFS-TEA), the ratio of medial femoral condyle length to medial tibial plateau length at knee extension (MFL/MTL), medial and lateral tibial slopes (MTS and LTS), the difference between MTS and LTS (MTS-LTS), the anatomical medial proximal tibia angle (aMPTA), the anatomical lateral distal femoral angle (aLDFA), and the distal condylar angle (DCA).
Material and Methods
MRI MEASUREMENTS:
The American College of Radiology provides guidelines for knee MRI, specifying a maximum field-of-view of 16 cm, a maximum slice thickness of 4 mm, a maximum interslice gap of 50%, and a minimum phase-frequency matrix of 192×256. These parameters are essential for ensuring high-quality imaging and accurate measurement of knee anatomical parameters [17].
MEASUREMENT OF POSTERIOR TIBIAL SLOPE (PTS, MTS AND LTS):
PTS, MTS, and LTS were measured on transverse and sagittal MRI images, as described by Lee et al [10,11]. First, the longitudinal axis of the tibia needs to be determined. The longitudinal axis of the tibia is determined by the center of the 2 circles. The first circle should be tangent to the proximal tibia, anterior and posterior tibia cortex, and the second circle should also be tangent to the anterior and posterior tibia cortex. The center of the second circle needs to be on the circumference of the first circle. The line connecting the center of the 2 circles is defined as the longitudinal axis of the tibia. Second, the midline of the tibial plateau and the medial or lateral tibial plateau need to be identified on the axial image to determine the corresponding central image on the sagittal image. Finally, the peak anterior and most posterior points of the proximal tibial cartilage were connected on different sagittal planes. The tibia slope is defined as the angle between the reference line of the proximal tibia and the vertical line of the longitudinal axis of the tibia (Figure 1). If the tibia slope is positive, it means that the anterior peak of the proximal tibia is higher than the highest point of the posterior.
MEASUREMENT OF PCA:
PCA is defined as the angle between 2 marked lines on the axial MRI image, one of which is the transepicondylar axis (TEA) connecting the most prominent position of the lateral epicondyle and the groove of the medial epicondyle, and the other was the posterior condyle line connecting the most posterior point of on the medial and lateral condyles (Figure 2). The PCA was defined as positive when the distal femur was externally rotated.
MEASUREMENT OF PTFS-TEA:
PTFS-TEA was measured according to the measurement introduced by Yang et al [18]. The position of the tangent behind the distal femoral shaft was marked at the upper popliteal level. PTFS-TEA was defined as the angle between the posterior tangent of the distal femoral shaft and the line of the most posterior points on the medial and lateral condyles (Figure 3).
MEASUREMENT OF AMPTA AND ALDFA:
aMPTA was measured on magnetic resonance coronal images, defined as the angle between the anatomical axis of the tibia (as described by Lee et al [11]) and the tangent line of the cartilage margin of the proximal tibia. Similarly, aLDFA was defined as the angle between the anatomical axis of the femur and the tangent line of the cartilage margin of the lateral femur (Figure 4).
MEASUREMENT OF DCA AND MFL/MTL:
DCA was defined as the angle between the distal tangent of the femoral condyle and the transepicondylar axis on the MRI coronal plane (Figure 5). According to the measurement method described by Kwak et al [19], MFL/MTL was defined as the ratio of the length of the medial femoral condyle to the length of the medial tibial plateau on the medial MRI coronal plane image (Figure 6).
STATISTICAL ANALYSIS:
All data were analyzed using the SPSS 24.0 statistical package (IBM, Armonk, New York, USA). Normality and homogeneity of variance were initially tested for all parameters to determine the data distribution. Normally distributed data are described as mean±SD and compared between the 2 groups using the independent-samples
Results
BASELINE CHARACTERISTICS AND STATISTICAL ANALYSIS:
The t test was used to analyze differences in age, rotation angle, and posterior angle of medial tibial plateau. Other data were analyzed using the Mann-Whitney U test. The correlation coefficients of the 2 authors were good (0.804 to 0.978). There were no statistically significant differences between the study group and the control group in demographic characteristics including age, sex and leg side (Table 1).
COMPARISON OF KNEE ANATOMICAL PARAMETERS:
For PCA, PTFS-AFE, MTS, LTS, MTS-LTS, and aLDFA, t test results showed no significant difference between the control and study groups. Detailed statistical results are shown in Table 2. For DCA, MFL/MTL, and aMPTA, the Wilcoxon rank-sum test showed no significant difference between the 2 groups (Table 3).
SEX-SPECIFIC ANALYSIS RESULTS:
In both female and male patients, the observed parameters were not significantly different between the control and study groups (Table 4).
Discussion
The aim of this study was to explore the risk factors for meniscus injury by comparing knee anatomical parameters in the normal population with the non-traumatic posterior horn of the medial meniscus on MRI images. The main finding of this study was that knee anatomical parameters was not associated with the posterior horn of the medial meniscus, including PCA, PTFS-AFE, MTS, LTS, MTS-LTS, DCA, MFL/MTL, aLDFA, and aMPTA in both women and men.
ElMansori et al [13] measured MTS and LTS on CT scans in 362 patients with ACL injury and found that MTS had no effect on the incidence of meniscus injury compared with patients without meniscus injury. Markl et al [20] measured MTS and LTS on MRI scans of patients with acute ACL injury and found that posterior meniscus injury was more common, but was not associated with higher PTS. This conclusion is similar to our study’s findings. However, there are also some studies that differ from our conclusions. For instance, in a study of 174 patients diagnosed with ACL injury, Lee et al [11] found that patients with PTS ≥13° had a significantly higher incidence of medial meniscus injury (90% vs 58%) than patients with PTS <13°. This suggests that medial meniscus injuries occur more frequently in knees with loss of ACL function and larger PTS. High PTS (MPTS and LPTS) seems to predispose patients to meniscal lesion in an acute ACL-insufficient knee. It has also been suggested that smaller MTS can lead to impact injury in the posterior corner of the medial meniscus [12]. We believe that the primary cause of these inconsistencies is the difference in study populations. The subjects in the studies by Lee et al and others were all patients with ACL injuries. Given that there is only a minimal to moderate correlation between MRI and arthroscopy in detecting and diagnosing the location, region, and morphology of meniscal injuries in patients with ACL tears [14], this could be the main reason for the discrepancies.
However, most patients with meniscus injuries in our clinical work do not have a history of ACL injury or trauma. We reviewed previous studies and found that there are few studies on the relationship between PTS and meniscal injury in patients with only meniscal injury, and the conclusions are conflicting. Alici et al [1] compared PTS in patients with and without meniscus injury and found that MTS was not associated with medial meniscus injury (MTS: 3.18±3.19 vs 3.27±1.12; LTS: 2.88±0.89 vs 2.91±1.01). Khan et al [12] suggested that shallower MTS was associated with posterior horn injury of medial meniscus (3.8±2.5 vs 2.4±2.3). Our results suggest that PTS is not associated with the posterior horn injury of medial meniscus (MTS: 12.42±4.46 vs 12.03±4.16; LTS: 10.46±4.59 vs 9.50±4.53). Additionally, Hashemi et al [10] reported that the average medial and lateral tibial slopes of females were greater than those of males, but there was no significant difference in medial tibial slope between the male or female groups in our study (Table 4). The controversy about PTS and meniscus injury may be due to different measurement methods selection, ethnic differences, poor matching between groups in sample selection, and MRI measurement.
Acute meniscus injuries often occur in knee joints with multiple ligament injuries or excessive flexion or squatting [3,21]. When the knee is flexed at 90°, the posterior angle of the meniscus transfers more load than the anterior angle [22, 23]. Three-dimensional MRI analysis and cadaver biomechanical studies found that the medial compartment femur-tibial contact area of the intact knee was greater at low flexion (0° and 30°) than at high flexion (60° and 90°) [24,25]. We hypothesized that greater contact area is conducive to intraarticular stability and may explain the lack of difference in MFL/MTL measured in knee extension between the 2 groups.
In our study, DCA and PCA were measured in the coronal and cross-sectional planes to analyze the relationship between the anatomical parameters of the distal femur and the medial meniscus injury. The DCA is the angle between the TEA and the tangent line of the distal femoral articular surface on the coronal plane, which reflects the tilt of the distal femoral condyle relative to the TEA in the extended position of the knee joint. When the distal femoral condyle has dysplasia or a bone defect, the angle increases, and the knee joint valgus deformity is more obvious in the extended position. PCA is the angle between TEA and the tangent line of the posterior articular surface of the posterior femoral condyle on the cross-sectional plane, which reflects the tilt of the posterior femoral condyle relative to the TEA in the flexion position of the knee. When the posterior of the lateral femoral condyle has dysplasia or a bone defect, the angle will increase, and the knee flexion valgus deformity will be more obvious. In theory, valgus deformity changes the stress on the meniscus and causes injury in either the extension or flexion position of the knee. However, our study showed no correlation between medial meniscus injury and measured parameters. The main role of the meniscus is to redistribute the contact force through the tibiofemoral joint, which is the result of the combined action of femoral-side, tibial-side, and soft-tissue factors, rather than a single factor playing a decisive role. We believe that it is insufficient to analyze the geometric characteristics of any side to summarize the stress characteristics of the meniscus, and it is difficult to analyze the factors influencing meniscus injury.
For PTFS-AFE, Yang et al [18] showed that it was associated with patellofemoral joint stability, and we suspected that there might be a link with tibiofemoral joint movement, but the results refuted our speculation.
The present study has several limitations. Heavy body weight is a known risk factor for meniscus injury due to the increased load on the knee joint. However, body mass index (BMI) was not included in this study, which may have led to differences in the characteristics of the included groups. Additionally, the degree of knee joint degeneration in the study population was not graded, and severe bone hyperplasia may have affected the measurement of local knee parameters. Furthermore, there is a certain degree of subjectivity in the selection of MR images and the choice of reference points when measuring knee joint parameters, which may also lead to errors in the results. Given these factors, the sample size of this study was relatively small, and additional studies are needed to verify these results.
Conclusions
The evaluated knee geometric parameters were not associated with non-traumatic posterior horn tears of the medial meniscus.
Figures
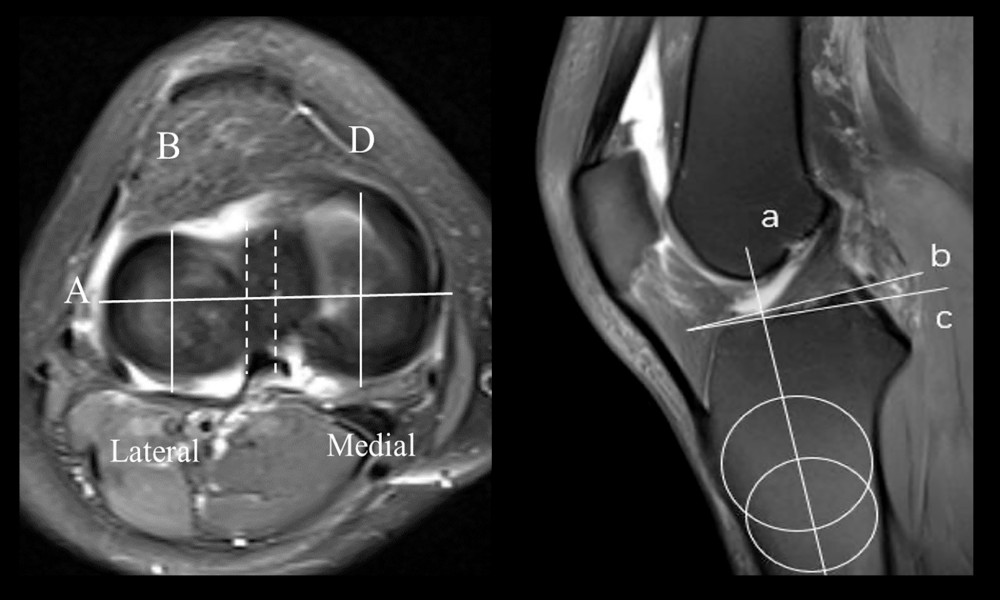 Figure 1. In this image, magnetic resonance images of the knee joint are axial and sagittal. B and D are the medial and lateral tibial plateau midline in the sagittal plane, respectively. A is the medial and lateral plateau midline in the coronal plane. a is the tibial axis, b is the vertical line of a, c is the tangent line of the tibial plateau, and the angle between b and c represents the posterior tibial slope angle.
Figure 1. In this image, magnetic resonance images of the knee joint are axial and sagittal. B and D are the medial and lateral tibial plateau midline in the sagittal plane, respectively. A is the medial and lateral plateau midline in the coronal plane. a is the tibial axis, b is the vertical line of a, c is the tangent line of the tibial plateau, and the angle between b and c represents the posterior tibial slope angle. 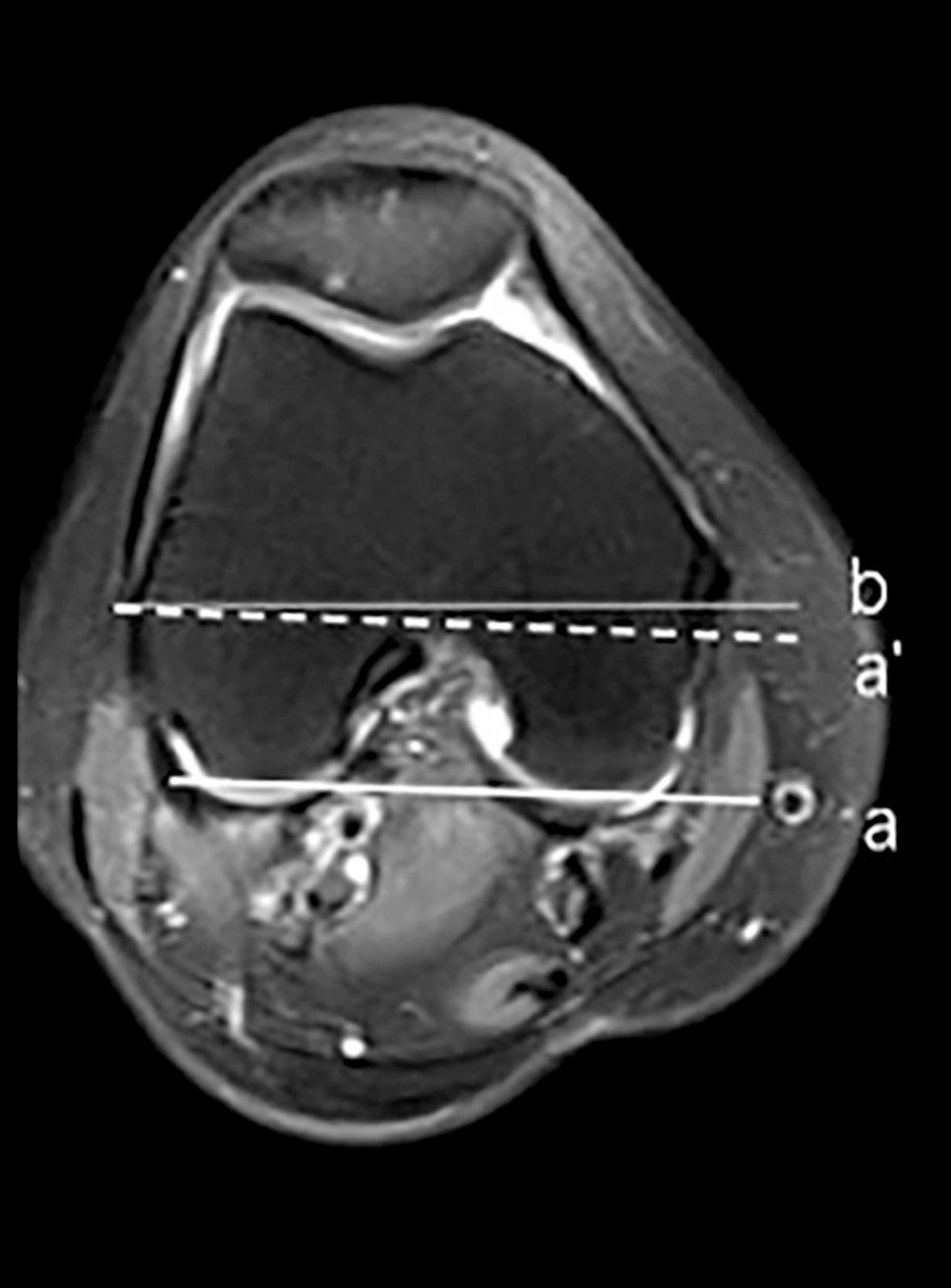 Figure 2. a is the tangent line of the posterior condyle on the magnetic resonance axial image of the knee joint, a′ is its parallel line, and b is the line of the internal and external epicondyle of the knee joint, representing the central axis of the knee joint movement. The angle between a′ and b is the rotation angle of the knee joint.
Figure 2. a is the tangent line of the posterior condyle on the magnetic resonance axial image of the knee joint, a′ is its parallel line, and b is the line of the internal and external epicondyle of the knee joint, representing the central axis of the knee joint movement. The angle between a′ and b is the rotation angle of the knee joint. ![This measurement method was described by Yang et al [18]. a is the posterior tangent line of the distal shaft of the femoral shaft, a′ is its horizontal line, b is the transepicondylar axis, and the angle between the posterior tangent of the distal femoral shaft and the transepicondylar axis (PTFS-TEA) is defined as the angle between a′ and b.](https://jours.isi-science.com/imageXml.php?i=medscimonit-31-e948366-g003.jpg&idArt=948366&w=1000) Figure 3. This measurement method was described by Yang et al [18]. a is the posterior tangent line of the distal shaft of the femoral shaft, a′ is its horizontal line, b is the transepicondylar axis, and the angle between the posterior tangent of the distal femoral shaft and the transepicondylar axis (PTFS-TEA) is defined as the angle between a′ and b.
Figure 3. This measurement method was described by Yang et al [18]. a is the posterior tangent line of the distal shaft of the femoral shaft, a′ is its horizontal line, b is the transepicondylar axis, and the angle between the posterior tangent of the distal femoral shaft and the transepicondylar axis (PTFS-TEA) is defined as the angle between a′ and b. 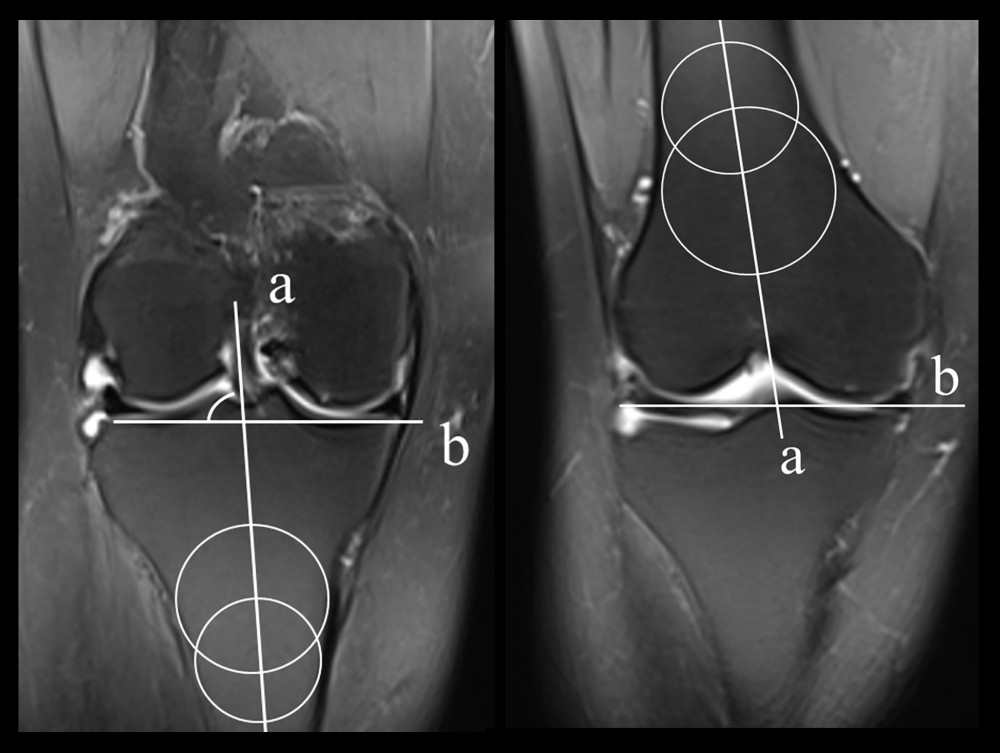 Figure 4. In this figure, the axis of the femur or tibia is represented. b is the tangent line of the tibial plateau or distal femur, and the angle of inversion or valvaration of the femur or tibia is measured by the angle between the 2 lines.
Figure 4. In this figure, the axis of the femur or tibia is represented. b is the tangent line of the tibial plateau or distal femur, and the angle of inversion or valvaration of the femur or tibia is measured by the angle between the 2 lines. 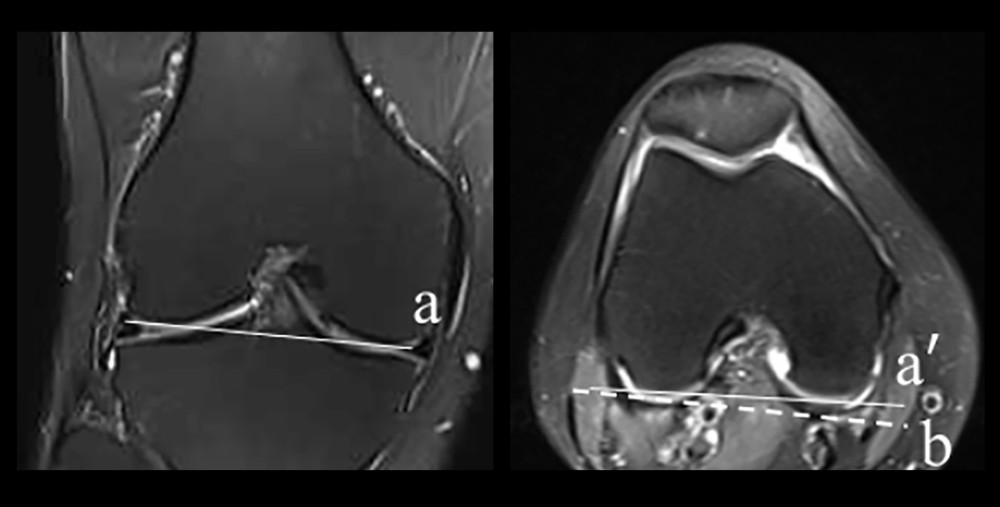 Figure 5. a is the tangent line of the distal femur, b is the horizontal line of a, and a′ is the tangent line of the posterior condyle of the femur. The distal condylar angle (DCA) is defined as the angle between the 2 lines.
Figure 5. a is the tangent line of the distal femur, b is the horizontal line of a, and a′ is the tangent line of the posterior condyle of the femur. The distal condylar angle (DCA) is defined as the angle between the 2 lines. 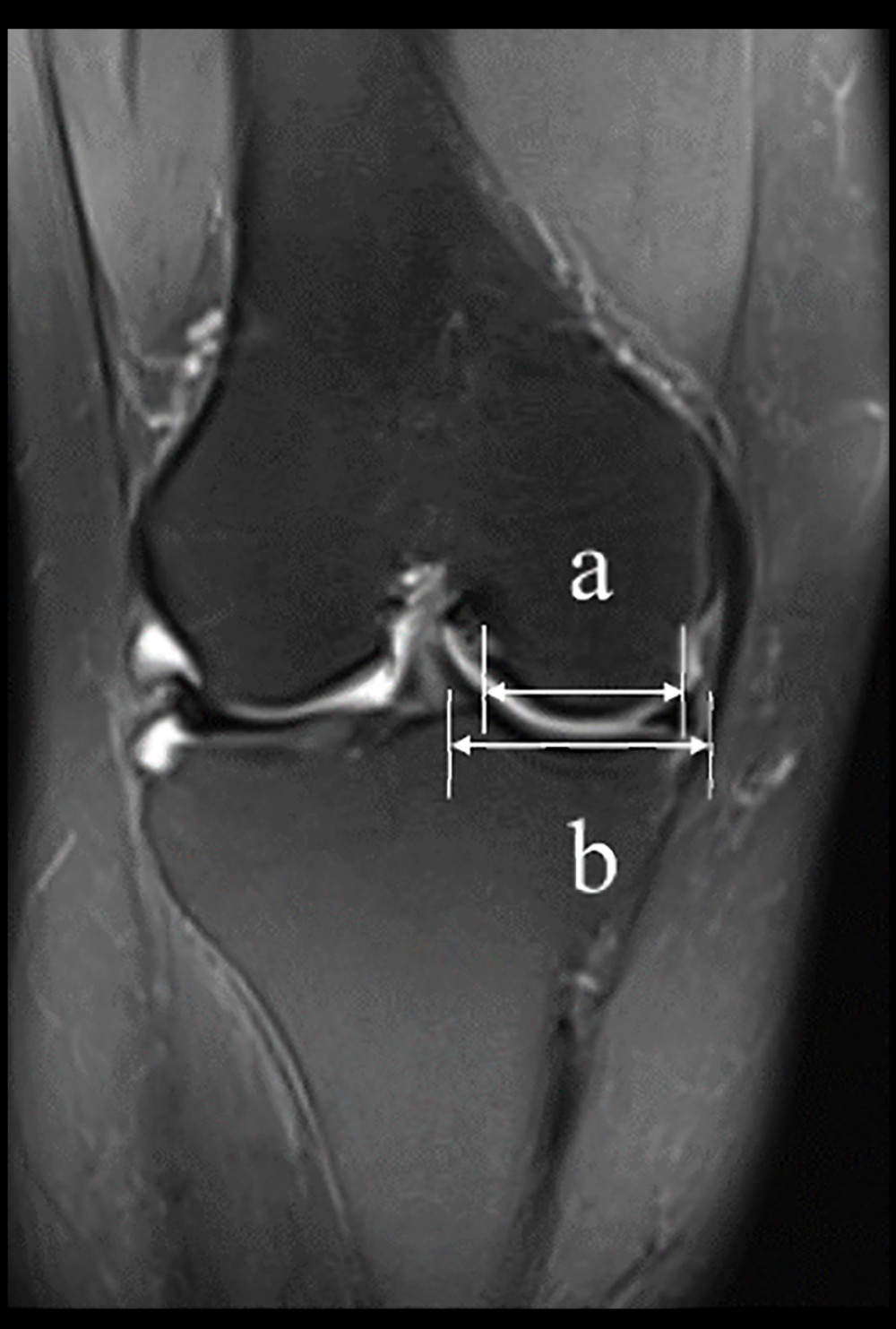 Figure 6. a and b represent the width of the medial and lateral condyles of the femur, respectively.
Figure 6. a and b represent the width of the medial and lateral condyles of the femur, respectively. Tables
Table 1. Comparisons between the 2 groups were made under several parameters, including age, sex, and leg side.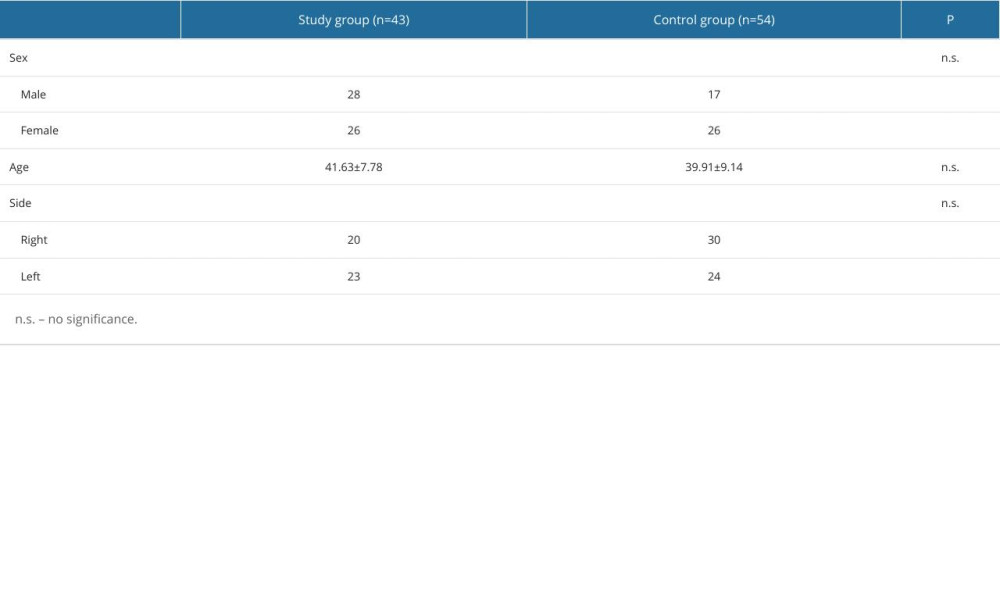 Table 2. Comparisons between the 2 groups were made under several parameters, including PCA, PTFS-AFE, MTS, LTS, MTS-LTS, and aLDFA.
Table 2. Comparisons between the 2 groups were made under several parameters, including PCA, PTFS-AFE, MTS, LTS, MTS-LTS, and aLDFA.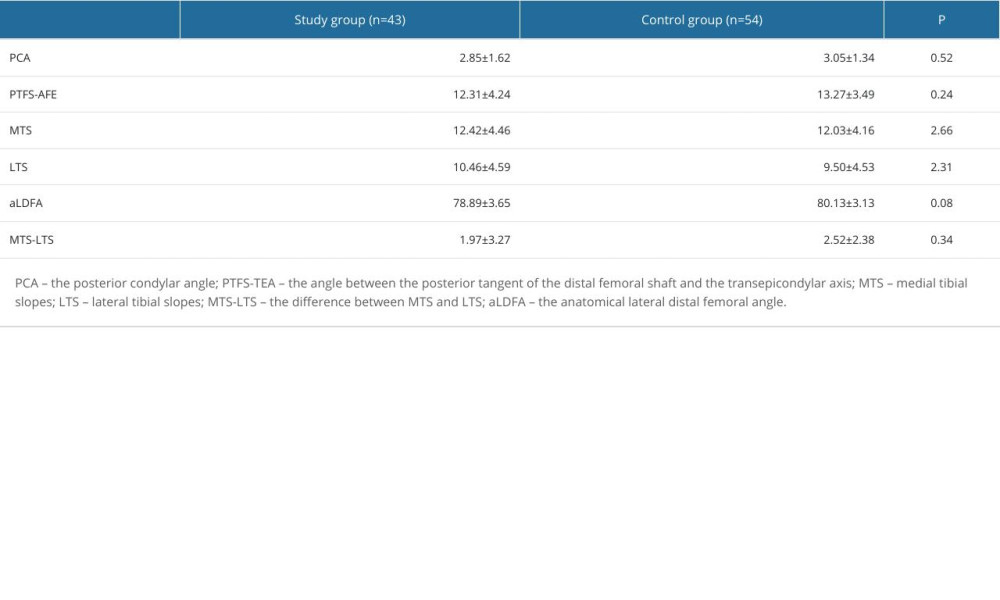 Table 3. Comparisons between the 2 groups were made under several parameters, including DCA, MFL/MTL, and aMPTA.
Table 3. Comparisons between the 2 groups were made under several parameters, including DCA, MFL/MTL, and aMPTA.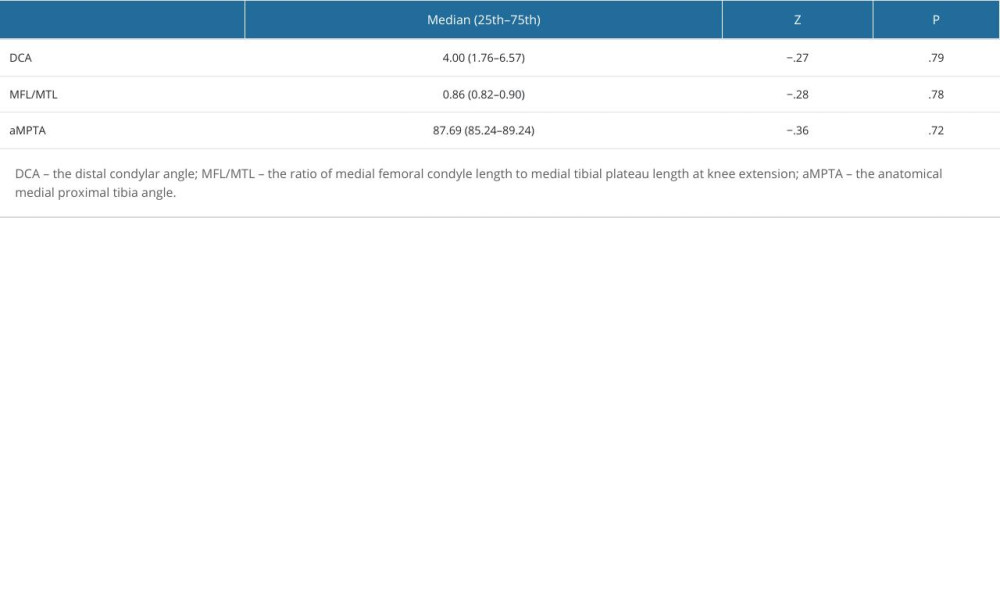 Table 4. Comparison of 2 groups of parameters of males and females.
Table 4. Comparison of 2 groups of parameters of males and females.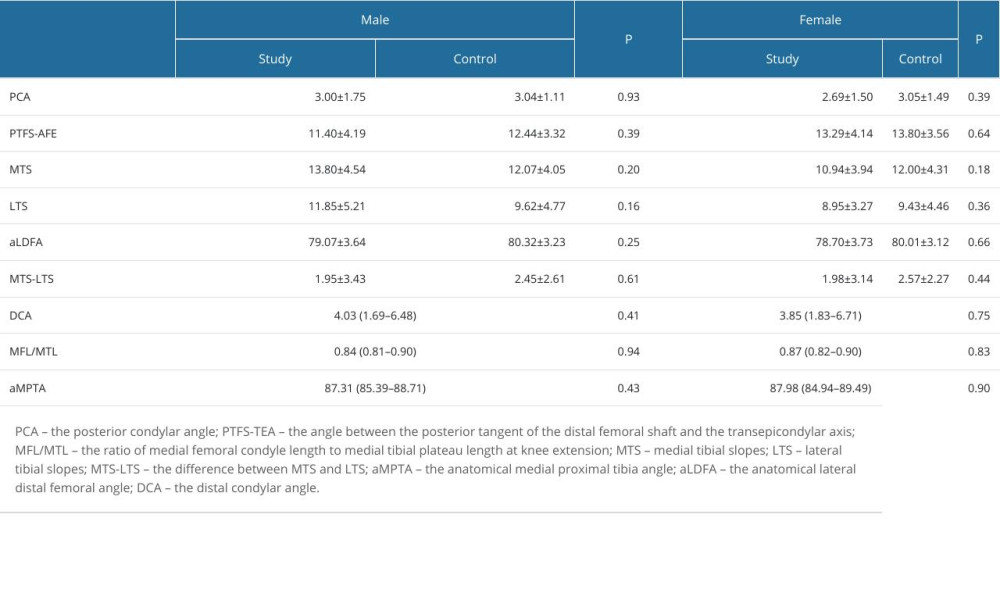
References
1. Alici T, Esenyel CZ, Esenyel M, Relationship between meniscal tears and tibial slope on the tibial plateau: Eurasian J Med, 2011; 43(3); 146-51
2. Makris EA, Hadidi P, Athanasiou KA, The knee meniscus: Structure-function, pathophysiology, current repair techniques, and prospects for regeneration: Biomaterials, 2011; 32(30); 7411-31
3. Bhatia S, LaPrade CM, Ellman MB, LaPrade RF, Meniscal root tears: Significance, diagnosis, and treatment: Am J Sports Med, 2014; 42(12); 3016-30
4. Bhattacharyya T, Gale D, Dewire P, The clinical importance of meniscal tears demonstrated by magnetic resonance imaging in osteoarthritis of the knee: J Bone Joint Surg Am, 2003; 85(1); 4-9
5. Ozkoc G, Circi E, Gonc U, Radial tears in the root of the posterior horn of the medial meniscus: Knee Surg Sports Traumatol Arthrosc, 2008; 16(9); 849-54
6. Raj MA, Bubnis MA, Knee Meniscal Tears. [Updated 2023 Jul 17]: StatPearls [Internet], 2025, Treasure Island (FL), StatPearls Publishing Available from: https://www.ncbi.nlm.nih.gov/books/NBK431067/
7. Bin SI, Kim JM, Shin SJ, Radial tears of the posterior horn of the medial meniscus: Arthroscopy, 2004; 20(4); 373-78
8. Hwang BY, Kim SJ, Lee SW, Risk factors for medial meniscus posterior root tear: Am J Sports Med, 2012; 40(7); 1606-10
9. Balcarek P, Terwey A, Jung K, Influence of tibial slope asymmetry on femoral rotation in patients with lateral patellar instability: Knee Surg Sports Traumatol Arthrosc, 2013; 21(9); 2155-63
10. Hashemi J, Chandrashekar N, Gill B, The geometry of the tibial plateau and its influence on the biomechanics of the tibiofemoral joint: J Bone Joint Surg Am, 2008; 90(12); 2724-34
11. Lee JJ, Choi YJ, Shin KY, Choi CH, Medial meniscal tears in anterior cruciate ligament-deficient knees: Effects of posterior tibial slope on medial meniscal tear: Knee Surg Relat Res, 2011; 23(4); 227-30
12. Khan N, McMahon P, Obaid H, Bony morphology of the knee and non-traumatic meniscal tears: is there a role for meniscal impingement?: Skeletal Radiol, 2014; 43(7); 955-62
13. Mansori AE, Lording T, Schneider A, Incidence and patterns of meniscal tears accompanying the anterior cruciate ligament injury: Possible local and generalized risk factors: Int Orthop, 2018; 42(9); 2113-21
14. Vo TT, Nguyen DT, Dinh Le NA, Evaluation of meniscal injury on magnetic resonance imaging and knee arthroscopy in patient with anterior cruciate ligament tear: SICOT J, 2024; 10; 56
15. Okazaki Y, Furumatsu T, Kodama Y, Steep posterior slope and shallow concave shape of the medial tibial plateau are risk factors for medial meniscus posterior root tears: Knee Surg Sports Traumatol Arthrosc, 2021; 29(1); 44-50
16. Laskin RS, Flexion space configuration in total knee arthroplasty: J Arthroplasty, 1995; 10(5); 657-60
17. Chien A, Weaver JS, Kinne E, Omar I, Magnetic resonance imaging of the knee: Pol J Radiol, 2020; 85; e509-e31
18. Yang G, Dai Y, Dong C, Distal femoral morphological dysplasia is correlated with increased femoral torsion in patients with trochlear dysplasia and patellar instability: Bone Joint J, 2020; 102-b(7); 868-73
19. Kwak YH, Lee S, Lee MC, Han HS, Large meniscus extrusion ratio is a poor prognostic factor of conservative treatment for medial meniscus posterior root tear: Knee Surg Sports Traumatol Arthrosc, 2018; 26(3); 781-86
20. Markl I, Zantop T, Zeman F, The effect of tibial slope in acute ACL-insufficient patients on concurrent meniscal tears: Arch Orthop Trauma Surg, 2015; 135(8); 1141-49
21. Papalia R, Vasta S, Franceschi F, Meniscal root tears: from basic science to ultimate surgery: Br Med Bull, 2013; 106; 91-115
22. Fox AJ, Bedi A, Rodeo SA, The basic science of human knee menisci: Structure, composition, and function: Sports Health, 2012; 4(4); 340-51
23. Walker PS, Erkman MJ, The role of the menisci in force transmission across the knee: Clin Orthop Relat Res, 1975(109); 184-92
24. Kim JG, Lee YS, Bae TS, Tibiofemoral contact mechanics following posterior root of medial meniscus tear, repair, meniscectomy, and allograft transplantation: Knee Surg Sports Traumatol Arthrosc, 2013; 21(9); 2121-25
25. LaPrade CM, Foad A, Smith SD, Biomechanical consequences of a nonanatomic posterior medial meniscal root repair: Am J Sports Med, 2015; 43(4); 912-20
Figures
Figure 1. In this image, magnetic resonance images of the knee joint are axial and sagittal. B and D are the medial and lateral tibial plateau midline in the sagittal plane, respectively. A is the medial and lateral plateau midline in the coronal plane. a is the tibial axis, b is the vertical line of a, c is the tangent line of the tibial plateau, and the angle between b and c represents the posterior tibial slope angle.Figure 2. a is the tangent line of the posterior condyle on the magnetic resonance axial image of the knee joint, a′ is its parallel line, and b is the line of the internal and external epicondyle of the knee joint, representing the central axis of the knee joint movement. The angle between a′ and b is the rotation angle of the knee joint.Figure 3. This measurement method was described by Yang et al [18]. a is the posterior tangent line of the distal shaft of the femoral shaft, a′ is its horizontal line, b is the transepicondylar axis, and the angle between the posterior tangent of the distal femoral shaft and the transepicondylar axis (PTFS-TEA) is defined as the angle between a′ and b.Figure 4. In this figure, the axis of the femur or tibia is represented. b is the tangent line of the tibial plateau or distal femur, and the angle of inversion or valvaration of the femur or tibia is measured by the angle between the 2 lines.Figure 5. a is the tangent line of the distal femur, b is the horizontal line of a, and a′ is the tangent line of the posterior condyle of the femur. The distal condylar angle (DCA) is defined as the angle between the 2 lines.Figure 6. a and b represent the width of the medial and lateral condyles of the femur, respectively. Tables
Table 1. Comparisons between the 2 groups were made under several parameters, including age, sex, and leg side.Table 2. Comparisons between the 2 groups were made under several parameters, including PCA, PTFS-AFE, MTS, LTS, MTS-LTS, and aLDFA.Table 3. Comparisons between the 2 groups were made under several parameters, including DCA, MFL/MTL, and aMPTA.Table 4. Comparison of 2 groups of parameters of males and females.Table 1. Comparisons between the 2 groups were made under several parameters, including age, sex, and leg side.Table 2. Comparisons between the 2 groups were made under several parameters, including PCA, PTFS-AFE, MTS, LTS, MTS-LTS, and aLDFA.Table 3. Comparisons between the 2 groups were made under several parameters, including DCA, MFL/MTL, and aMPTA.Table 4. Comparison of 2 groups of parameters of males and females. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387