06 July 2025: Clinical Research
Immobilization with a Short Leg Cast in Acute Peroneus Brevis Tendon Tears
Muhammed Taha Demir DOI: 10.12659/MSM.948836
Med Sci Monit 2025; 31:e948836






Abstract
BACKGROUND: Acute ankle inversion sprain (AAIS) is a musculoskeletal condition commonly seen in emergency departments, often leading to peroneus brevis tendon (PBT) injuries. These injuries are usually treated with conservative management. The aim of this study was to determine the effectiveness of immobilization with a short leg cast in treatment of incomplete split PBT tears compared to when immobilization is not used.
MATERIAL AND METHODS: A group of 49 patients with PBT split injury occured by AAIS, as verified by magnetic resonance imaging (MRI), were evaluated from 2013 to 2021. Patients were divided into 2 groups: Group 1 (n=27) received no immobilization, and Group 2 (n=22) received immobilization by a short leg cast. AOFAS (American Orthopedic Foot and Ankle Society) scores at baseline and the last follow-up were compared using the Mann-Whitney U test.
RESULTS: Of the 49 patients, 55.1% were female, with a mean age of 43.76±14.23 and an average follow-up of 14.9±4.9 months. The AOFAS score of Group 1 improved from 38 (range 35-43) to 74 (range 68-82) (P<0.001), and Group 2 improved from 36 (range 31.5-38.5) to 86 (range 78.75-92) (P<0.001). The final AOFAS scores were significantly higher in Group 2 (P=0.007). Seven patients (25.9%) in Group 1 and 3 patients (13.6%) in Group 2 required surgical intervention (P=0.288).
CONCLUSIONS: For partial split PBT tears after AAIS, 4 weeks of cast immobilization led to better clinical outcomes at 14.9±4.9 months follow-up compared to no immobilization, but did not affect surgical intervention rates.
Keywords: Tendon Injuries, Ankle Injuries, Tendons, Humans, Female, Male, adult, Immobilization, Casts, Surgical, Middle Aged, Magnetic Resonance Imaging, Treatment Outcome
Introduction
The peroneus brevis tendon (PBT) inserts at the level of the fifth metatarsal base and plays a critical role in foot eversion and dorsiflexion movements [1]. It passes through the retro-malleolar groove accompanied by the peroneus longus tendon (PLT) [2]. PBT tears can occur due to various etiologies, including direct trauma, foot abnormalities, repeated subluxations, and tenosynovitis due to systemic diseases. A concave or flat shape of the retro-malleolar groove, peroneal tubercle hypertrophy, the presence of an os peroneum, or an accessory peroneus quartus muscle can predispose the ankle to PBT tears [3]. Moreover, administration of fluoroquinolone antibiotics and corticosteroids has been implicated in tendon lesions [4]. Histopathological studies demonstrate that PBT tears are predominantly of a mechanical etiology [5]. Although the PBT has a flat and elliptical shape, the PLT is more rounded. The PLT travels parallel to the PBT, applying compression forces on the latter posterior to the fibula. This close anatomy leads to a mechanical tension on the PBT that causes the formation of tears [3]. The tears are usually in a longitudinal split type, and transverse tears are rare [3,4].
Injuries to the ankle are among the most frequently encountered musculoskeletal injuries in the emergency department, with acute ankle sprains (AAS) accounting for about one-quarter of these [6]. Bone, cartilage, tendon, or ligament structure injuries can occur due to AAS. Failure to correctly diagnose AAS or delay in management can lead to substantial morbidity [7]. Most non-surgical treatments have good outcomes, but neglected cases may require surgical intervention [8]. It is believed that about 80–90% of all AAS are due to an inversion mechanism [9]. In acute ankle inversion sprain (AAIS), peroneal tendon (PT) injuries are seen at a rate of 13% [10]. Of these, 70–80% are peroneal brevis tendon (PBT) injuries [11]. PBT injuries occur mainly longitudinally due to forceful dorsiflexion movements [12–14]. Approximately 40% of PT injuries are missed in the primary examination after trauma [8,15]. If a PT injury is suspected, magnetic resonance imaging (MRI) is the imaging method of choice [3,15]. Moreover, MRI also helps to identify associated soft tissue, cartilage, or bone injuries that can occur with PT injuries [3,15].
In partial split PBT tears, conservative treatment methods are commonly used [1,4,13–17]. Casting can be used to decrease tension on the tendon. A short leg cast applied for 4–8 weeks can facilitate tendon healing [15]. In addition, the use of orthotics, cryotherapy, NSAIDs, activity modification, and physical therapy that strengthens the muscular-tendinous junction can be used [4,8,14,15]. There is little evidence on the effectiveness of conservative treatment of partial split PBT injury [12,13,16], and the specific effect of immobilization therapy on outcomes is unclear. The AOFAS (American Orthopedic Foot and Ankle Society) scoring system is used to measure improvement of pain, functional capacity, range of movement, and ankle stability after conservative treatment [18]. The scoring system awards points for pain (40 points), function (50 points), and alignment (10 points), with a combined highest score of 100. In the present study, it was also used to objectively evaluate the effect of conservative treatment on functional outcomes.
Other non-surgical modalities used in the treatment of partial split PBT tears might include steroid or platelet-rich plasma injection therapy [8,17,19,20]. Surgical treatment is generally used for full-thickness tears and partial tears that respond negatively to conservative treatment [1,14,15,21–24].
The aim of this study was to compare the effectiveness of immobilization therapy with a short leg cast versus no immobilization in treatment of partial split PBT tears due to AAIS.
Material and Methods
PATIENT SELECTION:
The study was approved by our university ethics committee (E-22686390-050.99-58779). Informed consent was obtained from all patients meeting the inclusion criteria. Of the 907 patients with presumed soft tissue injury of the AAIS presenting during 2013–2021, and admitted for an MRI scan at an injury care center, 98 patients with a partial split tear of the PBT were identified by 2 specialist orthopedic physicians. The contact details of these patients were obtained from the institutional collection of data, following which a telephone contact was attempted with them and they were requested to undergo a follow-up examination. The AOFAS scores of Group 1 (no immobilization) and Group 2 (immobilization with a short leg cast) were reassessed in follow-up consultations by the same 2 surgeons who had provided the initial AOFAS scoring and the treatment strategy following the injury. Comparative statistical analysis was performed to compare the 2 groups.
INCLUSION CRITERIA:
We included patients 18 years and older with MRI-confirmed grade 2 partial split PBT tears resulting from AAIS and showing no fracture on the initial plain radiographic evaluations at the time of injury.
EXCLUSION CRITERIA:
We excluded patients with full-thickness PBT tears, full-thickness lateral ligament tears, occurrence of fractures on the injury day, PT dislocation, instability, prior history of surgical treatment of the foot or ankle, foot structure abnormalities, chronic ankle pain, lack of AOFAS scoring from initial evaluations, or failure to attend the last follow-up appointment. The study enrolled a total of 49 patients.
TREATMENT GROUPS:
In this study, 2 conservative treatment methods for PBT tears were performed by 2 orthopedic surgeons in the same clinical setting. One of the surgeons used a short leg cast consistently as part of the treatment protocol, while the other used a non-immobilization approach. The patients were divided into 2 groups based on the treatment modality used: Group 1 (n=27) received conservative treatment with rest in combination with an ankle support orthosis with no cast immobilization; Group 2 (n=22) received treatment with immobilization using a 3M Scotch Cast (St. Paul, MN, USA) short leg cast.
DIAGNOSIS AND IMAGING:
At the final follow-up examination, patients were inspected for tenderness localized at the PT, PT dislocation, and signs of joint instability. All participants had radiographic imaging at the time of initial trauma to rule out fractures, followed by MRI evaluation due to suspected soft tissue injury. The severity of the tendon injuries was graded according to the findings of the MRI [14]:
The study only examined partial-thickness tears graded as grade 2, as shown in Figure 1. All patients had 2 reviews of their MRI scans, and patients with only confirmed grade 2 tears were included in the analysis. All the diagnostic MRI scans were performed using a 3.0 Tesla Signa Pioneer magnet (97 channels, GE, USA) and a 17-channel in vivo coil.
TREATMENT PROTOCOL:
Group 2 received a 4-week immobilization, followed by a further period of rest of 2 weeks with the assistance of an ankle support orthosis. The Group 1 received treatment using a static ankle support orthosis with a rest period that added up to 6 weeks. Patients in both groups were advised not to perform high-impact sports and activities for the first 6 months after the injury.
DATA PROCESSING AND DISTRIBUTION ASSESSMENT:
The data were analyzed using IBM SPSS Statistics for Windows, Version 24.0 (released in 2016, Armonk, NY: IBM Corp.). Categorical variables are presented as absolute frequencies (n) and corresponding percentages (%), providing a clear depiction of the distribution of categories within the dataset. The Shapiro-Wilk test, a statistical procedure designed to assess whether a dataset is normally distributed, was employed to evaluate the normality of the data. This test is especially appropriate when the sample size is less than 50, as it provides a more reliable assessment of normality under these conditions. Since the continuous data did not meet the assumptions of normality, variables are summarized using the median and interquartile range (IQR), with the median representing the central tendency and the IQR (25th–75th percentile) indicating the variability. This approach is particularly appropriate for data that are not normally distributed, as the median and IQR are robust measures less influenced by extreme values.
STATISTICAL TESTING AND SIGNIFICANCE:
The Mann-Whitney U test was used to compare the distributions of numerical variables between study groups. The Wilcoxon signed-rank test, a non-parametric statistical method which assesses whether there is a statistically significant difference in the median values of paired observations, was used to compare pre- and post-intervention scores within each group. Fisher’s exact test, a non-parametric statistical method that is particularly appropriate when sample sizes are small or when the assumptions required for the chi-square test are not met, was used to assess the association between categorical variables across groups. The test calculates the exact probability of observing the data under the null hypothesis of no association between the variables. In the analysis, a p-value threshold of less than 0.05 was established to determine statistical significance. This conventional cutoff implies that if the p-value obtained from a statistical test is below 0.05, there is sufficient evidence to reject the null hypothesis, suggesting that the observed effect is unlikely to have occurred by random chance alone.
Additionally, a post hoc power analysis based on the observed AOFAS score difference and estimated effect size (Cohen’s d≈1.2) was performed using G*Power software, demonstrating a statistical power of approximately 90–95%.
Results
GENERAL PATIENT DATA:
Of the 49 patients included in the study, 55.1% were female, with a mean±SD age of 43.76±14.23 years and a mean follow-up duration of 14.9±4.9 months. Group 1 consisted of 27 patients, and Group 2 consisted of 22 patients.
FINDINGS OF GROUP 1:
In Group 1, which consisted of 27 patients, 59% were females. The median age was 51 years, ranging from 33 to 59, and the median follow-up period was 15 months, ranging from 11 to 18. The mean pre-treatment AOFAS score (AOFAS 1) was 38, with scores ranging between 35 and 43. The mean at final follow-up (AOFAS 2) was 74, ranging from 68 to 82. The difference between the AOFAS 1 and AOFAS 2 scores was statistically significant (p<0.001), as shown in Figure 2A.
FINDINGS OF GROUP 2:
In Group 2 (n=22), 50% of patients were female, with a median age of 38.5 years (range: 29.75–53.25), and a median follow-up duration of 14 months (range: 11–16.5). The mean AOFAS 1 score was 36 (range: 31.5–38.5), and the mean AOFAS 2 score was 86 (range: 78.75–92). The increase between AOFAS 1 and AOFAS 2 scores was also found to be statistically significant (p<0.001) (Figure 2B).
COMPARISON BETWEEN GROUPS:
In comparing Group 1 and Group 2 outcomes, median age, follow-up time, and baseline AOFAS 1 scores were similar in both groups (p>0.05 for all). However, the mean AOFAS 2 score was significantly higher in Group 2 compared to Group 1, at 86 (78.75–92) versus 74 (68–82), with a p-value of 0.007 (Figure 3).
Surgical intervention was recommended in 7 patients (25.9%) in Group 1 and in 3 patients (13.6%) in Group 2, due to clinical and radiological progression. The difference between these rates was not statistically significant (p=0.288). Post hoc power analysis of the 49 patients was performed. It used the observed difference of around 12 points (86 vs 74), and the statistical power obtained was 90% to 95%. This result confirmed that the sample size used was suitable for the observed difference.
Discussion
LIMITATIONS:
This study has a number of acknowledged limitations. First, longer follow-up would have allowed more thorough assessment of tendon healing and functional recovery. Secondly, the retrospective nature of the study reduces the validity of the statistical analysis. A prospective randomized controlled clinical trial might provide stronger and more reliable outcomes, counteract selection bias, and allow more thorough delineation of the functional consequences of immobilization. Serial follow-up MRIs ideally would have provided an objective method of tendon healing monitoring; however, practicality and financial restrictions made this impossible in all patients.
Conclusions
In the case of partial split PBT tears after AAIS, immobilization with a short leg cast for 4 weeks produced better clinical results compared with no immobilization, within a follow-up period of 14.9±4.9 months, but the surgical rates were similat between groups. It is important that physicians are aware of the potential for PBT tears in patients who have lateral ankle pain after AAIS, and when they detect partial split PBT tears, they should consider the possibility of using a short leg cast.
Figures
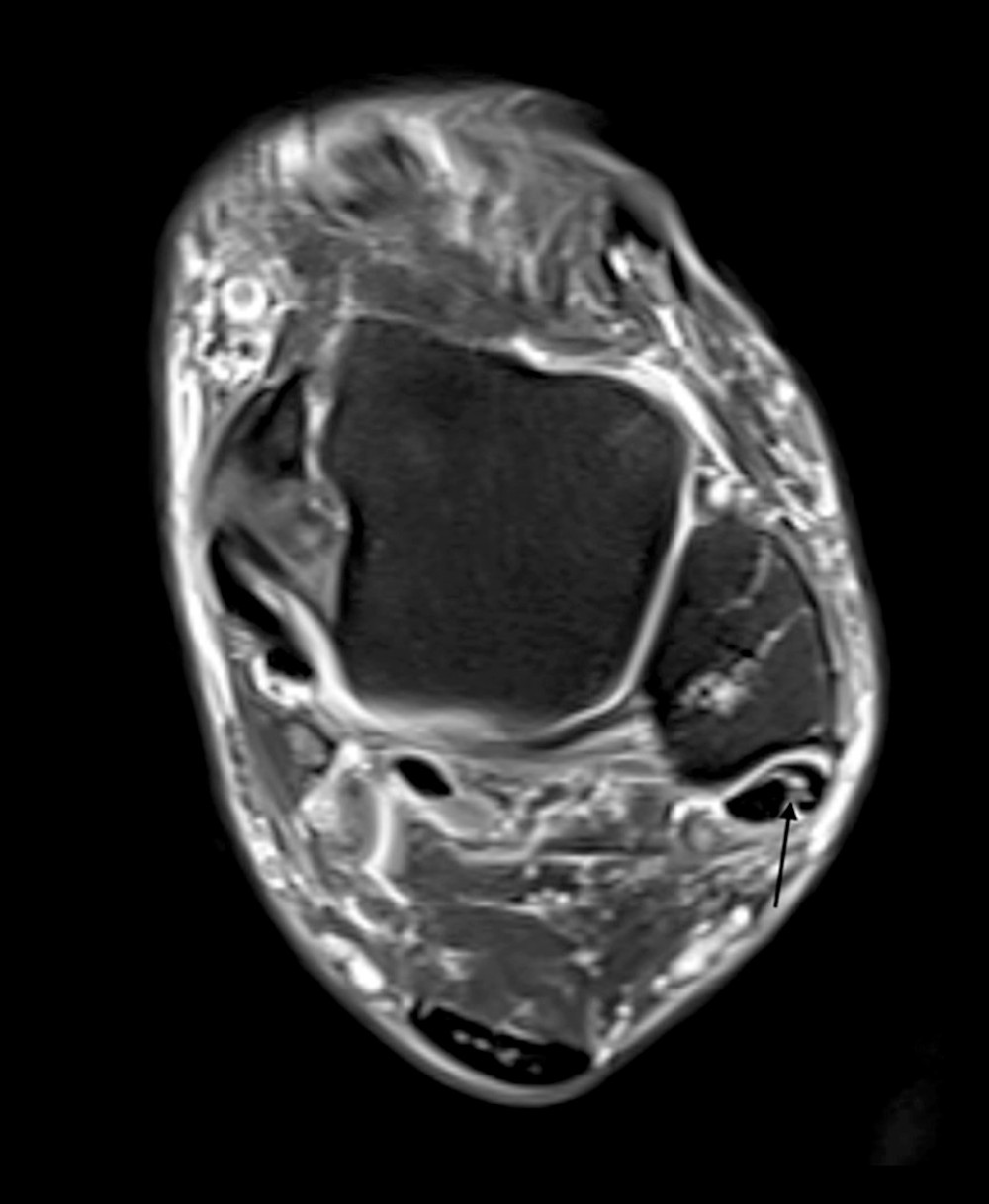 Figure 1. An axial magnetic resonance image that shows a partial tear of the peroneus brevis tendon (PBT), which is marked with the black arrow. The magnetic resonance imaging (MRI) data was obtained from a Picture Archiving and Communication System (PACS) and then exported to the RadiAnt DICOM Viewer (version 2021.2; Medixant) for analysis.
Figure 1. An axial magnetic resonance image that shows a partial tear of the peroneus brevis tendon (PBT), which is marked with the black arrow. The magnetic resonance imaging (MRI) data was obtained from a Picture Archiving and Communication System (PACS) and then exported to the RadiAnt DICOM Viewer (version 2021.2; Medixant) for analysis. 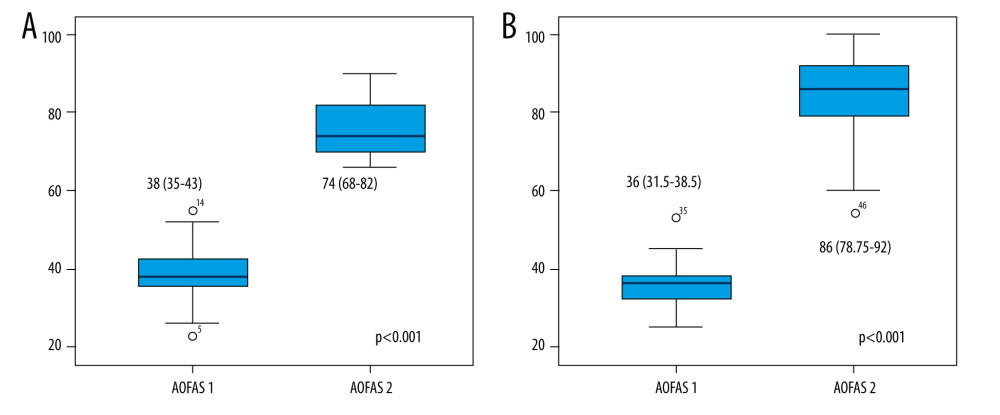 Figure 2. The comparison of the median and the interquartile range of AOFAS 1 and 2 in patients divided into A) Group 1 and B) Group 2. The increases observed in both groups were statistically significant (p<0.001).
Figure 2. The comparison of the median and the interquartile range of AOFAS 1 and 2 in patients divided into A) Group 1 and B) Group 2. The increases observed in both groups were statistically significant (p<0.001). ![Comparison of median (interquartile range) AOFAS 1 and AOFAS 2 between Group 1 and Group 2. AOFAS 2 median score was significantly higher in Group 2 compared with Group 1 (86 [78.75–92] vs 74 [68–82], respectivelt, p=0.007).](https://jours.isi-science.com/imageXml.php?i=medscimonit-31-e948836-g003.jpg&idArt=948836&w=1000) Figure 3. Comparison of median (interquartile range) AOFAS 1 and AOFAS 2 between Group 1 and Group 2. AOFAS 2 median score was significantly higher in Group 2 compared with Group 1 (86 [78.75–92] vs 74 [68–82], respectivelt, p=0.007).
Figure 3. Comparison of median (interquartile range) AOFAS 1 and AOFAS 2 between Group 1 and Group 2. AOFAS 2 median score was significantly higher in Group 2 compared with Group 1 (86 [78.75–92] vs 74 [68–82], respectivelt, p=0.007). References
1. Basit H, Shah J, Siccardi MA: Anatomy, bony pelvis and lower limb, foot peroneus brevis muscle April 4, 2023, National Library of Medicine Available from: https://www.ncbi.nlm.nih.gov/books/NBK535427/
2. Mabit C, Salanne P, Boncoeur-Martel MPThe lateral retromalleolar groove: A radio-anatomic study: Bull Assoc Anat (Nancy), 1996; 80(249); 17-21 [in French]
3. Taljanovic MS, Alcala JN, Gimber LH, High-resolution US and MR ımaging of peroneal tendon ınjuries: Radiographics, 2015; 35(1); 179-99
4. Walt J, Massey P: Peroneal tendon syndromes, 2023, National Institutes of Health Available from: https://www.ncbi.nlm.nih.gov/books/NBK544354/
5. Sobel M, DiCarlo EF, Bohne WH, Collins L, Longitudinal splitting of the peroneus brevis tendon: An anatomic and histologic study of cadaveric material: Foot Ankle, 1991; 12(3); 165-70
6. Meehan TM, Martinez-Salazar EL, Torriani M, Aftermath of ankle ınversion ınjuries: Spectrum of MR ımaging findings: Magn Reson Imaging Clin N Am, 2017; 25(1); 45-61
7. Scoty WM, Victoria LS: Acute ankle sprain, 2025, StatPearls Publishing
8. Civan O, Ürgüden M, Peroneal tendon problems in sports: Totbid Dergisi, 2018; 17; 12-22 [in Turkish]
9. Mackenzie MH, Zachary YK, Stephen WM, Erik AW, Epidemiology of ankle sprains and chronic ankle ınstability: J Athl Train, 2019; 54(6); 603-10
10. Fallat L, Grimm DJ, Saracco JA, Sprained ankle syndrome: prevalence and analysis of 639 acute injuries: J Foot Ankle Surg, 1998; 37(4); 280-85
11. Sobel M, Bohne WH, Markisz JA, Peroneal tendon injuries: Foot and Ankle Clinics, 1996; 1(2); 369-79
12. Huuskonen M, Borkmann S, Bengtsson A, Radiological features accompanying peroneus brevis split rupture revealed on magnetic resonance imaging: A cohort study: J Foot Ankle Res, 2023; 16(1); 10
13. Rademaker J, Rosenberg ZS, Delfaut EM, Tear of the peroneus longus tendon: MR imaging features in nine patients: Radiology, 2000; 214(3); 700-4
14. Chauhan B, Panchal P, Szabo E, Wilkins T, Split peroneus brevis tendon: An unusual cause of ankle pain and ınstability: J Am Board Fam Med, 2014; 27(2); 297-302
15. Danna NR, Brodsky JW, Diagnosis and operative treatment of peroneal tendon tears: Foot Ankle Orthop, 2020; 5(2); 1-11
16. Ersoz E, Tokgoz N, Kaptan AY, Anatomical variations related to pathological conditions of the peroneal tendon: Evaluation of ankle MRI with a 3D Space sequence in symptomatic patients: Skeletal Radiol, 2019; 48(8); 1221-31
17. Roster B, Michelier P, Giza E, Peroneal tendon disorders: Clin Sports Med, 2015; 34(4); 625-41
18. Kitaoka HB, Alexander IJ, Adelaar RS, Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes: Foot Ankle Int, 1994; 15(7); 349-53
19. Dallaudière B, Meyer P, Hummel V, Efficacy of second intra-tendinous platelet-rich-plasma injection in case of incomplete response of the first injection: three-year follow up experience: Diagn Interv Imaging, 2013; 94(9); 871-77
20. Dallaudière B, Pesquer L, Meyer P, Intratendinous injection of platelet-rich plasma under US guidance to treat tendinopathy: A long-term pilot study: J Vasc Interv Radiol, 2014; 25(5); 717-23
21. Bokwa-Dąbrowska K, Mocanu D, Alexiev A, Peroneus brevis split rupture is underreported on magnetic resonance imaging of the ankle in patients with chronic lateral ankle pain: Eur J Radiol Open, 2024; 11; 100591
22. Kumar Y, Alian A, Ahlawat S, Peroneal tendon pathology: Pre- and post-operative high resolution US and MR imaging: Eur J Radiol, 2017; 92; 132-44
23. Pitarini A, Anastasia M, Kennedy D, The surgical procedure in managing peroneal tendon ınjury: A case series: Orthop Res Rev, 2022; 14; 255-62
24. Götz J, Schenkel A, Grifka J, Springorum HR. Postural stability and pedobarography after reconstruction of peroneus brevis tendon split lesion: Int Orthop, 2024; 48(9); 2311-18
25. Squires N, Myerson MS, Gamba C, Surgical treatment of peroneal tendon tears: Foot Ankle Clin, 2007; 12; 4
26. Georgias T, Nikolas M, Nikolas T, Paylos K, Non-operative treatment of peroneal split syndrome: A case report: Acta Orthop Belg, 2012; 78(6); 804-7
27. Jeng C, Peroneal tendon disorders: Foot and Ankle Sports Medicine, 2013; 141-49, Philadelphia, Lippincott Williams & Wilkins
28. Mercer NP, Gianakos AL, Mercurio AM, Kennedy JG, Clinical outcomes of peroneal tendon tears: A systematic review: J Foot Ankle Surg, 2021; 60(5); 1008-13
29. Sammarco GJ, Peroneus longus tendon tears: Acute and chronic: Foot Ankle Int, 1995; 16(5); 245-53
30. Dombek MF, Lamm BM, Saltrick K, Peroneal tendon tears: A retrospective review: J Foot Ankle Surg, 2003; 42(5); 250-58
31. Kennedy JG, Van Dijk PA, Murawski CD, Functional outcomes after peroneal tendoscopy in the treatment of peroneal tendon disorders: Knee Surg Sports Traumatol Arthrosc, 2016; 24(4); 1148-54
32. van Dijk PAD, van Dijk CN, Peroneal tendons: Muscle and tendon ınjuries – evaluation and management, 2017; 373-80, Berlin Heidelberg, Springer
33. Davda K, Malhotra K, O’Donnell P, Peroneal tendon disorders: EFORT Open Rev, 2017; 2(6); 281-92
34. Van dijk CN, Kort N, Tendoscopy of the peroneal tendons: Arthroscopy, 1998; 14(5); 471-78
Figures
Figure 1. An axial magnetic resonance image that shows a partial tear of the peroneus brevis tendon (PBT), which is marked with the black arrow. The magnetic resonance imaging (MRI) data was obtained from a Picture Archiving and Communication System (PACS) and then exported to the RadiAnt DICOM Viewer (version 2021.2; Medixant) for analysis.Figure 2. The comparison of the median and the interquartile range of AOFAS 1 and 2 in patients divided into A) Group 1 and B) Group 2. The increases observed in both groups were statistically significant (p<0.001).Figure 3. Comparison of median (interquartile range) AOFAS 1 and AOFAS 2 between Group 1 and Group 2. AOFAS 2 median score was significantly higher in Group 2 compared with Group 1 (86 [78.75–92] vs 74 [68–82], respectivelt, p=0.007). In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387