14 June 2023: Clinical Research
A Case-Control Study of 40 Patients with Piriformis Muscle Syndrome to Evaluate Diagnostic Findings Using Two-Dimensional Ultrasound and Shear Wave Elastography
Mingmin XuABCDEFG, Bin MengABCD, Yan XuABCD, Zhe GengABCD, Jichao HuABCD, Xiaofang ZhengABCDEFDOI: 10.12659/MSM.940214
Med Sci Monit 2023; 29:e940214






Abstract
BACKGROUND: Piriformis muscle syndrome (PMS) is a neuropathy caused by compression of the sciatic nerve by the piriformis muscle. This case-control study included 40 patients with PMS and aimed to evaluate the diagnostic findings using two-dimensional ultrasound and shear wave elastography (SWE), as non-invasive and cost-effective diagnostic methods.
MATERIAL AND METHODS: In order to evaluate the value of two-dimensional ultrasound diagnosis, a new imaging technique called shear wave elastography (SWE) was used in the screening of PMS, with a total of 40 PMS patients and 40 healthy individuals participating in our study. We analyzed the correlation and area under the curve (AUC) of changes in thickness (mm) and Young’s modulus (kpa) of the bilateral piriformis muscle (PM).
RESULTS: We found that PM thickness and Young’s modulus on the lesion sides were significantly higher in PMS patients than in controls (P<0.05). Also, we determined that there was a positive correlation between PM thickness and Young’s modulus (r=0.454, P<0.05). Using two-dimensional ultrasonic diagnosis and the SWE technique, a specificity of 95.8% and sensitivity of 78.8% were demonstrated in the clinical diagnosis of PM.
CONCLUSIONS: Two-dimensional ultrasound with SWE technology has demonstrated its superior sensitivity and specificity in diagnosing PMS in the clinic.
Keywords: Imaging, Three-Dimensional, Piriformis Muscle Syndrome, Ultrasonography, Humans, Elasticity Imaging Techniques, Case-Control Studies, Sciatic Nerve
Background
Piriformis muscle syndrome (PMS) is a form of sciatica that is relatively uncommon and is an important cause of sciatica [1]. About 5–6% of sciatica cases are caused by PMS [1–4]. PMS causes pain in the glutes and groin [3], and is a neuromuscular condition caused by the entrapment of the sciatic nerve by the piriformis muscle (PM). When the PM is injured, it will result in spasm, hyperemia, and hypertrophy, which in turn can lead to compression of the sciatic nerve, further causing pain and soreness in one or both glutes [5]; this is sometimes accompanied by radiating pain and numbness on the same side of the lower extremity, as is limited flexion of the lower limbs [6]. PMS can seriously affect a patient’s quality of life. Recent research on cellular signaling and molecular pathology found a link to, PMS which will advance the understanding of this syndrome [7–12]. However, at present, diagnosis and treatment of PMS are challenging, and there is no criterion standard diagnostic test. Despite the use of several invasive and non-invasive diagnostic methods, most orthopedic and other related departments use a diagnosis of exclusion [13,14].
Invasive nerve block remains the most reliable diagnostic tool due to the lack of a gold standard test for PMS. Delayed diagnosis can lead to chronic somatic dysfunction and muscle weakness, and a high-sensitivity screening test would be very helpful in guiding clinical diagnosis of PMS [13,14]. Several reports have shown that magnetic resonance imaging (MRI) can be useful in the diagnosis of PMS [15–19], but the examination time is significantly longer and the cost is higher, which limits its wide application in clinical practice. In recent years, with the continuous advancement of ultrasound technology and diagnostic concepts, ultrasonic shear wave elastography (SWE) presents a new imaging method, which has been applied to the quantitative assessment of tissue elasticity [20]. SWE technology has been used to assess the elasticity of the upper trapezius muscle and its influencing factors [21], in joint laxity [20], identifying plantar fasciitis [22], in the examination of polymyositis (PM) and dermatomyositis (DM) [23], and in differentiating between benign and malignant thickening of the gallbladder wall [24]. Some scholars have used SWE technology to evaluate the relationship between quadriceps muscle tension and patellar tendinopathy [25], and SWE technology has been used to evaluate gastrocnemius muscle elasticity and influencing factors in healthy people [2,5]. Therefore, this case-control study included 40 patients with PMS and aimed to evaluate the diagnostic findings using two-dimensional ultrasound and shear wave elastography (SWE) as non-invasive and cost-effective diagnostic methods.
Material and Methods
PATIENTS:
A total of 40 patients (15 males, 25 females) were included in the observation group in this study assessing the clinical utility of two-dimensional ultrasound combined with SWE technology in the diagnosis of PMS. Of these 40 PMS patients, 32 had unilateral disease and 8 had bilateral disease, and all were diagnosed and treated at Zhejiang Rongjun Hospital from January 2020 to August 2022. The patients were aged 20–76 years, with a mean age of 53.78±14.08 years, and the duration of the disease ranged from 2 weeks to 3 years. Diagnostic criteria were as follows: (1) Buttock pain was the main symptom, and severe pain was accompanied by radiating pain in the lower extremities, with limping or inability to walk. (2) Tenderness in the PM area, and a cord-like induration could be palpated, or the piriformis muscle tension test was positive. (3) There may be a history of trauma or cold. (4) Most common in middle-aged and elderly people. Inclusion criteria were as follows: (1) Those who meet the above clinical diagnosis of PMS. (2) Age 20–76 years old. (3) All subjects voluntarily participate and cooperate in this research. Exclusion criteria were as follows: (1) History of hip joint trauma. (2) Patients with hip and lower limb pain caused by diseases of the spine, femur, and pelvis. (3) Patients with other serious primary respiratory and cardiovascular diseases, and those with mental illness or those who cannot cooperate with the examination and are unwilling to cooperate with the research.
The control group consisted of 40 healthy volunteers, including 20 males and 20 females, aged 25–69 years, with a mean of 50.88±9.28 years. They had no low back pain, back trauma, or history of surgery, and the results of their neurosurgery physical examination were negative, with no systemic disease. This study was reviewed and approved by the Ethics Committee of Zhejiang Rongjun Hospital (No. 2020018), and all subjects signed the informed consent form.
METHODS:
We used the color Doppler ultrasound diagnostic instrument Philips EPIQ5 (Philips Ultrasound, Inc., Bothell, Washington, USA) with SWE function, and a convex array probe with a frequency of 1–5 MHz to measure the elastic modulus of muscles in musculoskeletal conditions. The clinician had more than 10 years of experience in musculoskeletal ultrasound examination, and the temperature of the examination environment was maintained at an average of 24.8±1.1°C.
The patient assumed a natural prone position, with the lower limbs in a neutral position, exposing the glutes, and fully relaxing the gluteal muscles, and applying an appropriate amount of coupling agent between the probe and the skin of the glutes. The clinician was careful to use the appropriate operating force and did not apply force to the glutes. The probe was gently place obliquely in the upper outer quadrant of the glutes on the side of the lesion, with the image showing the gluteus minimus, gluteus maximus, and iliac crest. The ilium was used as a landmark to slowly move the probe inward and downward and place it at the iliac crest. The place where the bony echo was interrupted was the greater sciatic foramen. At this time, the sonogram of the piriformis muscle can be detected. Adjusting the direction of the probe until it showed the maximum longitudinal section of the PM (the probe is always perpendicular to the piriformis muscle during the surgery). At this time, the maximum thickness of the PM muscle belly was measured 3 times. Then, SWE imaging was started, and the sampling frame was placed in the center of the PM muscle belly. After the SWE detection imaging was stable for 3–5 seconds, the measurement was started when the frozen elastic image was filled without defects, and the Young’s modulus on the lesion side was obtained. Modulus values were measured 3 times. The same method was used to measure PM thickness and Young’s modulus on both sides of the contralateral in the control groups, where detection was performed 3 times, and the results were averaged.
STATISTICAL ANALYSIS:
This study used SPSS 22.0 statistical software for statistical analysis. Measurement data conforming to normal distribution are represented by “x±s”, and the comparison between 2 groups of subjects used the independent sample
Results
GENERAL DATA OF PATIENTS IN COMPARISON:
To rule out the influence of patient heterogeneity, we analyzed differences between the 2 groups, and we found that there were no significant differences in age, weight, or height between the 2 groups (P=0.076) (Table 1).
THE STANDARD USE OF SWE DETECTION IMAGING IN PATIENTS:
The SWE detection imaging was stable for 3–5 seconds, the measurement started when the frozen elastic image was filled without defects, and the Young’s modulus in PM on the lesion side was obtained. Young’s modulus values were measured 3 times. The same method was used to measure PM thickness and Young’s modulus on both sides in the control groups, where detection was performed 3 times, and the results were averaged (Figure 1).
TWO-DIMENSIONAL ULTRASONOGRAPHY AND SWE EXAMINATION IN PM:
In the observation group, 96.8% (31/32 cases) of patients with unilateral PMS had thicker PM than in controls, and 90.6% (29/32 cases) of patients had larger Young’s modulus compared to that in the controls. The comparison of two-dimensional ultrasound imaging in the PM is shown in Figure 2. The use of SWE imaging of the PM is shown in Figure 3.
THE ANALYSIS OF UNILATERAL LESION SIDE AND ITS HEALTHY SIDE OF PM IN THE PATIENTS:
In the observation group, the maximum average thickness of PM on the sides of the lesions was 18.58±4.28 mm, and the average Young’s modulus (mean elastic modulus, E-mean) was 18.49±10.16 kPa. In its healthy unilateral sides, the maximum average thickness of PM was 14.42±3.37 mm, and the average Young’s modulus was 8.56±4.06 kPa, suggesting that the PM on the affected side was thicker than on the healthy side, and the Young’s modulus on the affected side was higher than on the healthy side. Differences in bilateral PM thickness and mean Young’s modulus were statistically significant between groups (P=0.0046, P<0.01) (Table 2).
THE ANALYSIS OF ALL LESION SIDES OF PM IN THE PATIENTS AND CONTROLS:
In the observation groups, the maximum average thickness of PM on all sides of the lesion (including unilateral and bilateral lesions) was 18.23±3.84 mm, and the mean Young’s modulus was 19.36±9.68 kPa. In the control group, the maximum average thickness of PM on both sides was 13.70±2.39 mm, and the average Young’s modulus was 8.85±2.31 kPa, and the difference in the maximum thickness of PM and the average value of Young’s modulus (E-mean) were statistically significant between groups (P=0.0078, P<0.01) (Table 3).
THE CORRELATION ANALYSIS BETWEEN PM THICKNESS AND YOUNG’S MODULUS IN PATIENTS:
To further reveal the correlation between PM thickness and Young’s modulus in patients, we further analyzed the correlation between PM thickness and Young’s modulus values. There was a moderate positive correlation between PM thickness and Young’s modulus values in the observation group and control group (r=0.454,
SPECIFICITY AND SENSITIVITY ANALYSIS BASED ON ROC CURVE AREA IN PMS PATIENTS:
The AUC of PM thickness in the diagnosis of PS using two-dimensional ultrasonography imaging was 0.841 (95% confidence interval: 0.766–0.915), the best cut-off point was 17.85 mm, and the calculated sensitivity and specificity were 60.4% and 95%, respectively (Figure 4A). The AUC of detecting Young’s modulus values using two-dimensional ultrasonography test was 0.886 (95% confidence interval: 0.813–0.958), the best cut-off value was 10.50, the sensitivity was 85.4%, and the specificity was 88.7% (Figure 4B). The AUC of the combined diagnosis using two-dimensional ultrasonography and SWE in the screening of PMS was 0.939 (95% confidence interval: 0.891~0.986), the sensitivity was 95.8%, and the specificity was 78.8% (Figure 4C, 4D), suggesting a high specificity and sensitivity of screening using two-dimensional ultrasonography and SWE in the diagnosis of patients with PMS.
Discussion
PMS currently lacks a uniform criterion standard diagnosis. In this study, we demonstrated that the use of two-dimensional ultrasound and SWE technology is superior to image PM thickness and Young’s modulus under physiological and pathological conditions to reveal its correlation and demonstrates a superior diagnosis of PM. In the past, it was often diagnosed with the leg raise test and piriformis muscle tone test, including the Pace test, the Thiele test, and the Freiberg test, which was subjective [1,4]. MRI is a good imaging technique for screening patients with PS. MRI and ultrasound have also shown a good correlation in the diagnosis of PMS, which may provide valuable information for clinical diagnosis in patients with PMS [15,26]. Ultrasound images have a higher detection rate. The combined use of ultrasound and MRI imaging can improve the diagnosis of patients with PMS, but the widespread application of MRI is still limited in clinical practice [15–19].
Several different protocols have been used to measure PM thickness. Some suggested that when measuring PM thickness, the leg is abducted at 45°, and the thickness of the piriformis muscle is measured on the inside of the ischial apex parallel to the longitudinal plane at the sciatic notch [13]. Some researchers use the maximum anteroposterior diameter in the piriformis muscle in the long-axis view and the short-axis view to measure PM thickness [13,27]. Others think that the maximum thickness of the PM muscle belly is best measured at the maximum longitudinal section of the PM [3]. It has been reported that the PM thickness on the side of the PMS lesion side varies from 11 mm to 31 mm [13,27,28]. This range is relatively large, which is related to the individual conditions, including race, age, sex, and course of the disease. In our study, we measured the thickness of the PM spasm or edema at the largest longitudinal section of the PM. Due to the finding that ambient temperature can change the biomechanical properties of soft tissues [28], and low temperature can reduce the temperature of human muscle, the muscle stiffness measurement increases significantly [29]; therefore, we kept the temperature at an average of 24.8±1.1°C [30] in order to maintain the biomechanical properties of muscles during the detection. In addition, PM is individual-dependent, meaning that it may vary in different people based on race, age, sex, and course of disease. In our study, we also found an exceptional case of a 55-year-old male patient who also had left-sided PMS disease and had prolonged the course of the disease for 1 month. The PM on the affected side in this patient was thinner than on the healthy side and the Young’s modulus on the affected side was higher than on the healthy side. This may be because the patient was older, with PM muscle fat and atrophy, so the bilateral PM thickness was not comparably sex-related. In addition, the course of the patient’s disease was short, and the PM may not have been in the acute stage of convulsion or edema, so the thickness of the PM on its healthy side is biased.
Ultrasonic SWE is a new imaging method that has been applied to the quantitative assessment of tissue elasticity [20,31–33]. SWE technology has been used to assess the elasticity of the upper trapezius muscle and its influencing factors [21], in joint laxity [20], identifying plantar fasciitis [22], in the screening of polymyositis (PM) and dermatomyositis (DM) [23], and assessment of the difference between benign and malignant thickening of the gallbladder wall [24]. In our study, we found that 96.8% (31/32 cases) of the diseased side had thicker PM than on the healthy side in unilateral patients, and the results were similar to those shown in the published literature [4,7,18,25,26,29,34–37]. Our SWE imageshowed that 90.6% (29/32 cases) of the PM Young’s modulus value on the lesion side were than on the healthy side, indicating that the PM on the lesion side was stronger than on the healthy side. There was a moderate positive correlation between PM thickness and Young’s modulus values in all subjects in our study (r=0.454,
Conclusions
In summary, the use of two-dimensional ultrasound imaging combined with SWE technology provides valuable diagnostic screening for PMS. SWE technology is a promising quantitative indicator to evaluate the degree of PM lesions in the diagnosis of PMS patients.
Figures
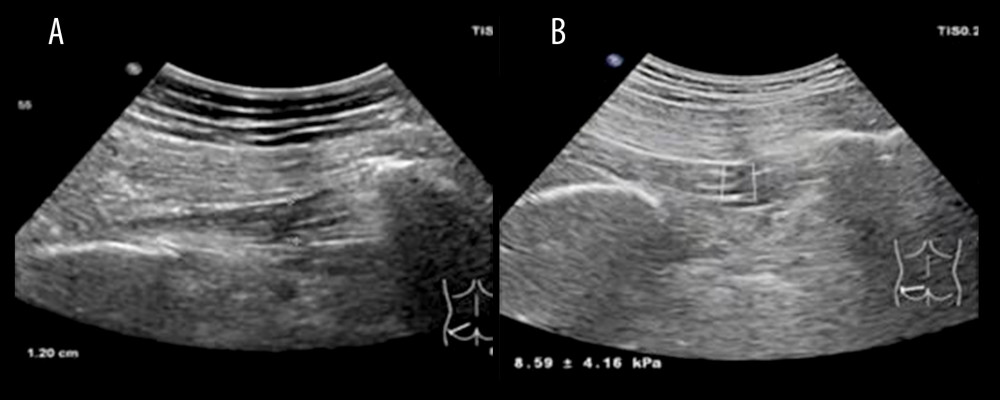 Figure 1. Two-dimensional ultrasound images, thickness measurements, and ultrasonic shear wave elastography (SWE) use in controls(A) The measured value of piriformis muscle (PM) thickness on the left side of the control group was 12.0 mm. (B) The Young’s modulus value of the left PM of the control group was 8.59±4.16 kPa.
Figure 1. Two-dimensional ultrasound images, thickness measurements, and ultrasonic shear wave elastography (SWE) use in controls(A) The measured value of piriformis muscle (PM) thickness on the left side of the control group was 12.0 mm. (B) The Young’s modulus value of the left PM of the control group was 8.59±4.16 kPa. 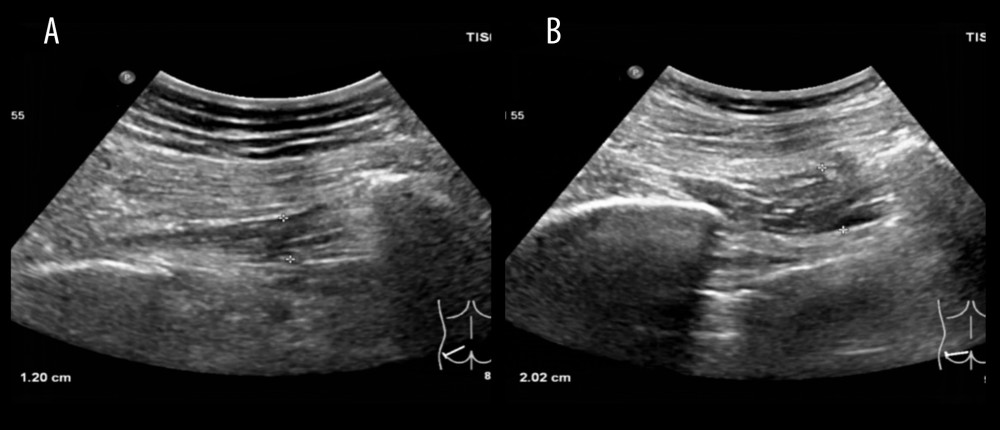 Figure 2. Two-dimensional ultrasonography thickness measurements in piriformis muscle(A) A female patient in the control group, 55 years old, having a thickness of the left piriformis muscle of 12.0 mm. (B) A patient in the observation group, a female, 53 years old, having a thickness of the left piriformis muscle of 20.2 mm.
Figure 2. Two-dimensional ultrasonography thickness measurements in piriformis muscle(A) A female patient in the control group, 55 years old, having a thickness of the left piriformis muscle of 12.0 mm. (B) A patient in the observation group, a female, 53 years old, having a thickness of the left piriformis muscle of 20.2 mm. 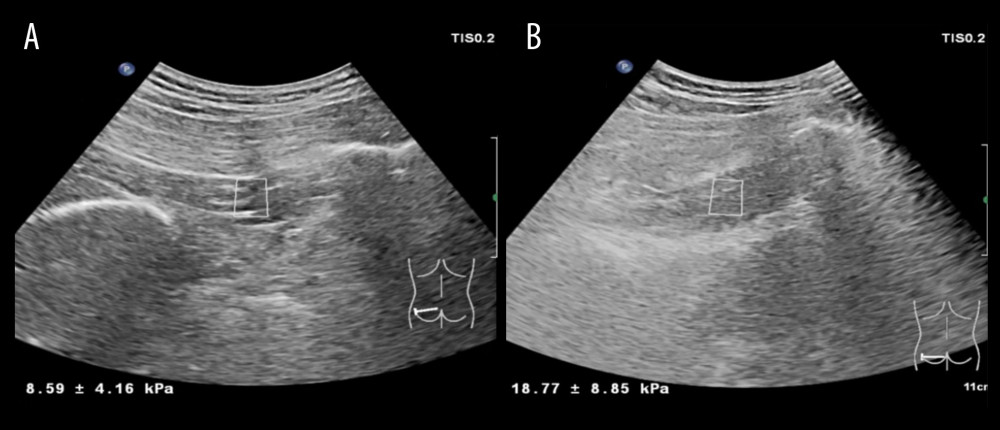 Figure 3. Use of ultrasonic shear wave elastography (SWE) measurement of piriformis muscle(A) In control group, a female, 55 years old, the Young’s modulus value of the left piriformis muscle was 8.59±4.16 kPa. (B) In observation group patient, a female, 53 years old, the Young’s modulus of the left piriformis muscle was 18.77±8.85 kPa.
Figure 3. Use of ultrasonic shear wave elastography (SWE) measurement of piriformis muscle(A) In control group, a female, 55 years old, the Young’s modulus value of the left piriformis muscle was 8.59±4.16 kPa. (B) In observation group patient, a female, 53 years old, the Young’s modulus of the left piriformis muscle was 18.77±8.85 kPa. 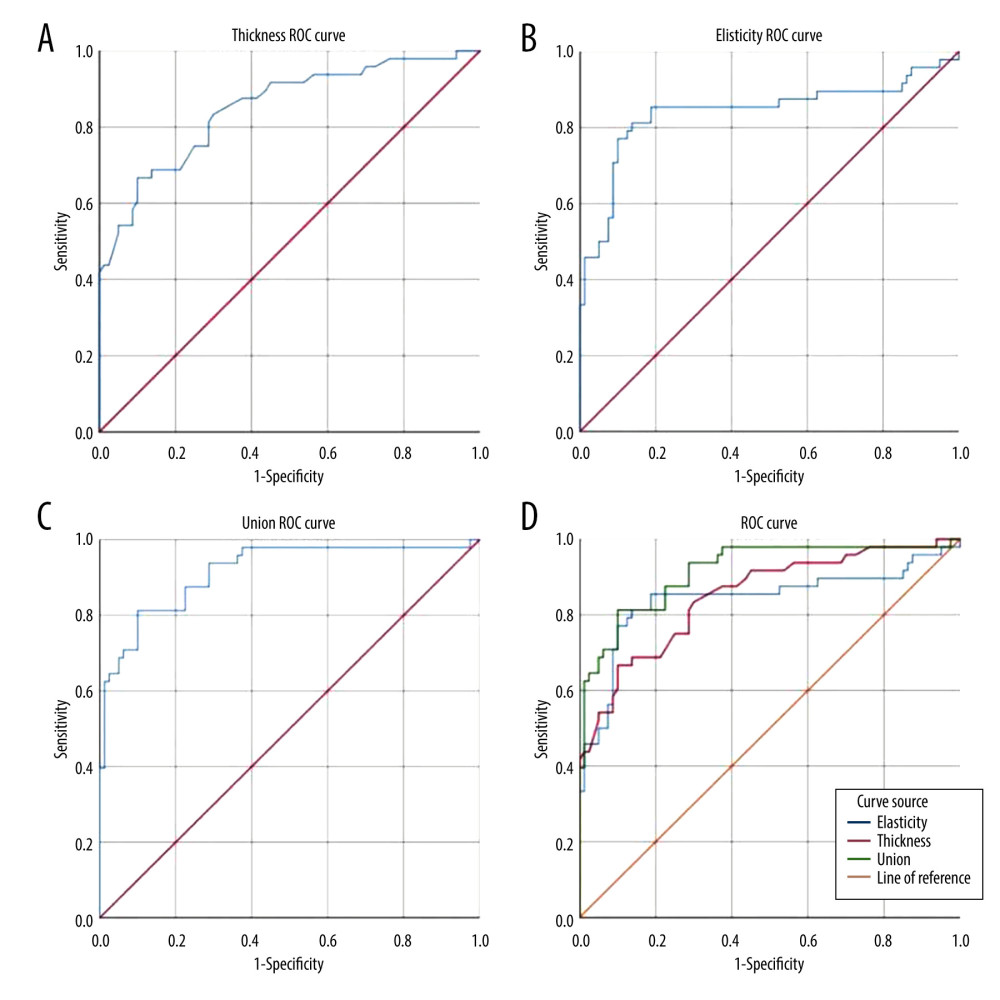 Figure 4. Receiver Operating Characteristic (ROC) curve analysis in PM thickness and Young’s modulus in Piriformis muscle syndrome (PMS) patients(A) ROC curve for the diagnosis of PMS according to piriformis muscle (PM) thickness using two-dimensional ultrasonography. (B) ROC curve for the diagnosis of PMS according to PM Young’s modulus using two-dimensional ultrasonography. (C) ROC curve for the combined diagnosis of PMS. (D) ROC curves were compiled together.
Figure 4. Receiver Operating Characteristic (ROC) curve analysis in PM thickness and Young’s modulus in Piriformis muscle syndrome (PMS) patients(A) ROC curve for the diagnosis of PMS according to piriformis muscle (PM) thickness using two-dimensional ultrasonography. (B) ROC curve for the diagnosis of PMS according to PM Young’s modulus using two-dimensional ultrasonography. (C) ROC curve for the combined diagnosis of PMS. (D) ROC curves were compiled together. References
1. Probst D, Stout A, Hunt D, Piriformis Syndrome: A narrative review of the anatomy, diagnosis, and treatment: PM R, 2019; 11(Suppl 1); S54-S63
2. Cao J, Xiao Y, Qiu W, Reliability and diagnostic accuracy of corrected slack angle derived from 2D-SWE in quantitating muscle spasticity of stroke patients: J Neuroeng Rehabil, 2022; 19(1); 15
3. Zhang W, Luo F, Sun H, Ding H, Ultrasound appears to be a reliable technique for the diagnosis of piriformis syndrome: Muscle Nerve, 2019; 59(4); 411-16
4. Fishman LM, Hosseini M, Piriformis syndrome – a diagnosis comes into its own: Muscle Nerve, 2019; 59(4); 395-96
5. Hicks BL, Lam JC, Varacallo M: Piriformis Syndrome, 2023, StatPearls, Treasure Island (FL)
6. Siddiq MA, Khasru MR, Rasker JJ, Piriformis syndrome in fibromyalgia: Clinical diagnosis and successful treatment: Case Rep Rheumatol, 2014; 2014; 893836
7. Son BC, Lee C, Piriformis syndrome (sciatic nerve entrapment) associated with type C sciatic nerve variation: A report of two cases and literature review: Korean J Neurotrauma, 2022; 18(2); 434-43
8. Larionov A, Yotovski P, Filgueira L, Novel anatomical findings with implications on the etiology of the piriformis syndrome: Surg Radiol Anat, 2022; 44(10); 1397-407
9. Liao J, Huang Y, Wang Q, Gene regulatory network from cranial neural crest cells to osteoblast differentiation and calvarial bone development: Cell Mol Life Sci, 2022; 79(3); 158
10. Juma SN, Gong X, Hu S, Shark new antigen receptor (IgNAR): Structure, characteristics and potential biomedical applications: Cells, 2021; 10(5); 1140
11. Chen G, Xu H, Yao Y, BMP Signaling in the development and regeneration of cranium bones and maintenance of calvarial stem cells: Front Cell Dev Biol, 2020; 8; 135
12. Chen G, Yao Y, Xu G, Zhang X, Regional difference in microRNA regulation in the skull vault: Dev Dyn, 2019; 248(10); 1009-19
13. Siahaan YMT, Tiffani P, Tanasia A, Ultrasound-guided measurement of piriformis muscle thickness to diagnose piriformis syndrome: Front Neurol, 2021; 12; 721966
14. Chang C, Jeno SH, Varacallo M: Anatomy, bony pelvis and lower limb, piriformis muscle, 2022, StatPearls, Treasure Island (FL)
15. Ayhan S, Nabiyev VN, Yetisyigit Y, Complementary specific pelvic sequences on routine lumbar magnetic resonance imaging scans: An imaging-based study focused on piriformis syndrome: Turk Neurosurg, 2019; 29(5); 698-704
16. Ro TH, Edmonds L, Diagnosis and management of piriformis syndrome: A rare anatomic variant analyzed by magnetic resonance imaging: J Clin Imaging Sci, 2018; 8; 6
17. Sen A, Rajesh S, Accessory piriformis muscle: An easily identifiable cause of piriformis syndrome on magnetic resonance imaging: Neurol India, 2011; 59(5); 769-71
18. Pecina HI, Boric I, Smoljanovic T, Surgical evaluation of magnetic resonance imaging findings in piriformis muscle syndrome: Skeletal Radiol, 2008; 37(11); 1019-23
19. Hu B, Wu T, Zhao Y, Physiological signatures of dual embryonic origins in mouse skull vault: Cell Physiol Biochem, 2017; 43(6); 2525-34
20. Yoshikawa T, Inui A, Mifune Y, Assessment of the ulnar collateral ligament of the elbow using ultrasonic shear wave elastography in professional baseball players: Orthop J Sports Med, 2022; 10(12); 23259671221138134
21. Ertekin E, Kasar ZS, Turkdogan FT, Is early diagnosis of myofascial pain syndrome possible with the detection of latent trigger points by shear wave elastography?: Pol J Radiol, 2021; 86; e425-e31
22. Albano D, Messina C, Gitto S, Shear-wave elastography of the plantar fascia: A systematic review and meta-analysis: J Ultrasound, 2023; 26(1); 59-64
23. Li M, Guo R, Tang X, Quantitative assessment of muscle properties in polymyositis and dermatomyositis using high-frequency ultrasound and shear wave elastography: Quant Imaging Med Surg, 2023; 13(1); 428-40
24. Soundararajan R, Dutta U, Bhatia A, Two-dimensional shear wave elastography: Utility in differentiating gallbladder cancer from chronic cholecystitis: J Ultrasound Med, 2023 [Online ahead of print]
25. Zhang ZJ, Ng GYF, Lee WC, Fu SN, Increase in passive muscle tension of the quadriceps muscle heads in jumping athletes with patellar tendinopathy: Scand J Med Sci Sports, 2017; 27(10); 1099-104
26. Demirel A, Baykara M, Koca TT, Berk E, Ultrasound elastography findings in piriformis muscle syndrome: Indian J Radiol Imaging, 2018; 28(4); 412-18
27. Wu YY, Guo XY, Chen K, Feasibility and reliability of an ultrasound examination to diagnose piriformis syndrome: World Neurosurg, 2020; 134; e1085-e92
28. Wu T, Felmlee JP, Greenleaf JF, Assessment of thermal tissue ablation with MR elastography: Magn Reson Med, 2001; 45(1); 80-87
29. Muraoka T, Omuro K, Wakahara T, Effects of muscle cooling on the stiffness of the human gastrocnemius muscle in vivo: Cells Tissues Organs, 2008; 187(2); 152-60
30. Akagi R, Takahashi H, Acute effect of static stretching on hardness of the gastrocnemius muscle: Med Sci Sports Exerc, 2013; 45(7); 1348-54
31. Toker C, Marquetand J, Symmank J, Shear wave elastography in bruxism-not yet ready for clinical routine: Diagnostics (Basel), 2023; 13(2); 276
32. Wang C, Wang H, Zhou Y, Evaluation of the clinical value of shear wave elastography for early detection and diagnosis of diabetic peripheral neuropathy: A controlled preliminary prospective clinical study: BMC Musculoskelet Disord, 2022; 23(1); 1120
33. Tyloch DJ, Tyloch JF, Adamowicz J, Comparison of strain and shear wave elastography in prostate cancer detection: Ultrasound Med Biol, 2023; 49(3); 889-900
34. Siddiq MA, Hossain MS, Uddin MM, Piriformis syndrome: A case series of 31 Bangladeshi people with literature review: Eur J Orthop Surg Traumatol, 2017; 27(2); 193-203
35. Menu P, Fouasson-Chaillou A, Dubois C, Dauty M, Piriformis syndrome diagnosis: On two professional cyclists: Ann Phys Rehabil Med, 2014; 57(4); 268-74
36. Wang Z, Zhu Y, Han D, Effect of hip external rotator muscle contraction on pelvic floor muscle function and the piriformis: Int Urogynecol J, 2022; 33(10); 2833-39
37. Gulsaran U, Ustabasioglu F, Gunay B, Ustabasioglu FE, Evaluation of accuracy of shear wave elastography and superb microvascular imaging methods in diagnosis of piriformis syndrome: A preliminary study: Ultrasound Med Biol, 2022; 48(12); 2521-29
38. Becchetti C, Lange NF, Delgado MG, 2D shear wave elastography of the rectus femoris muscle in patients with cirrhosis: Feasibility and clinical findings. A pilot study: Clin Res Hepatol Gastroenterol, 2023; 47(3); 102080
Figures
Figure 1. Two-dimensional ultrasound images, thickness measurements, and ultrasonic shear wave elastography (SWE) use in controls(A) The measured value of piriformis muscle (PM) thickness on the left side of the control group was 12.0 mm. (B) The Young’s modulus value of the left PM of the control group was 8.59±4.16 kPa.Figure 2. Two-dimensional ultrasonography thickness measurements in piriformis muscle(A) A female patient in the control group, 55 years old, having a thickness of the left piriformis muscle of 12.0 mm. (B) A patient in the observation group, a female, 53 years old, having a thickness of the left piriformis muscle of 20.2 mm.Figure 3. Use of ultrasonic shear wave elastography (SWE) measurement of piriformis muscle(A) In control group, a female, 55 years old, the Young’s modulus value of the left piriformis muscle was 8.59±4.16 kPa. (B) In observation group patient, a female, 53 years old, the Young’s modulus of the left piriformis muscle was 18.77±8.85 kPa.Figure 4. Receiver Operating Characteristic (ROC) curve analysis in PM thickness and Young’s modulus in Piriformis muscle syndrome (PMS) patients(A) ROC curve for the diagnosis of PMS according to piriformis muscle (PM) thickness using two-dimensional ultrasonography. (B) ROC curve for the diagnosis of PMS according to PM Young’s modulus using two-dimensional ultrasonography. (C) ROC curve for the combined diagnosis of PMS. (D) ROC curves were compiled together. Tables
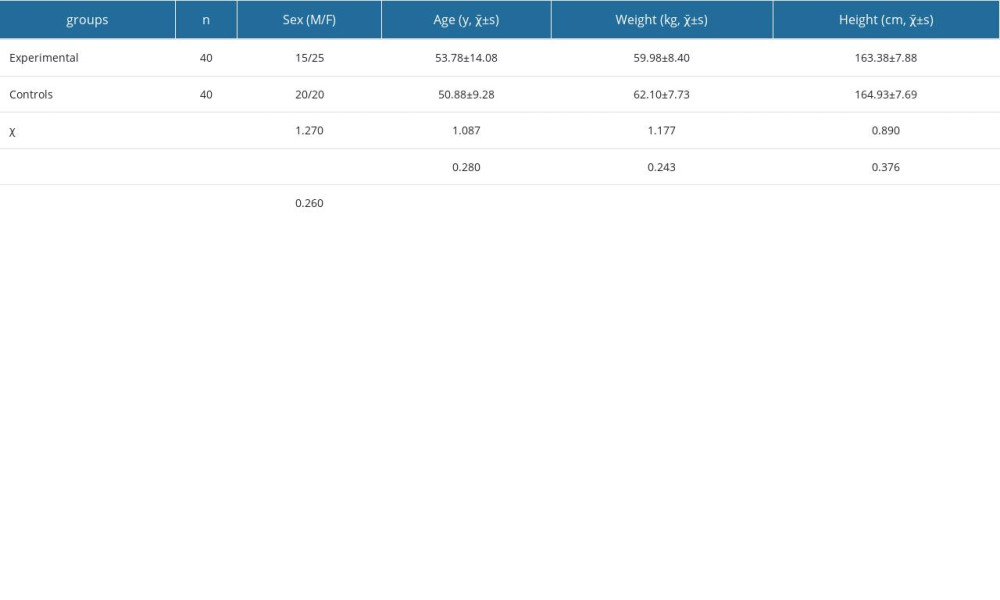 Table 1. General data comparison in patients within the groups (χ̄±s).
Table 1. General data comparison in patients within the groups (χ̄±s).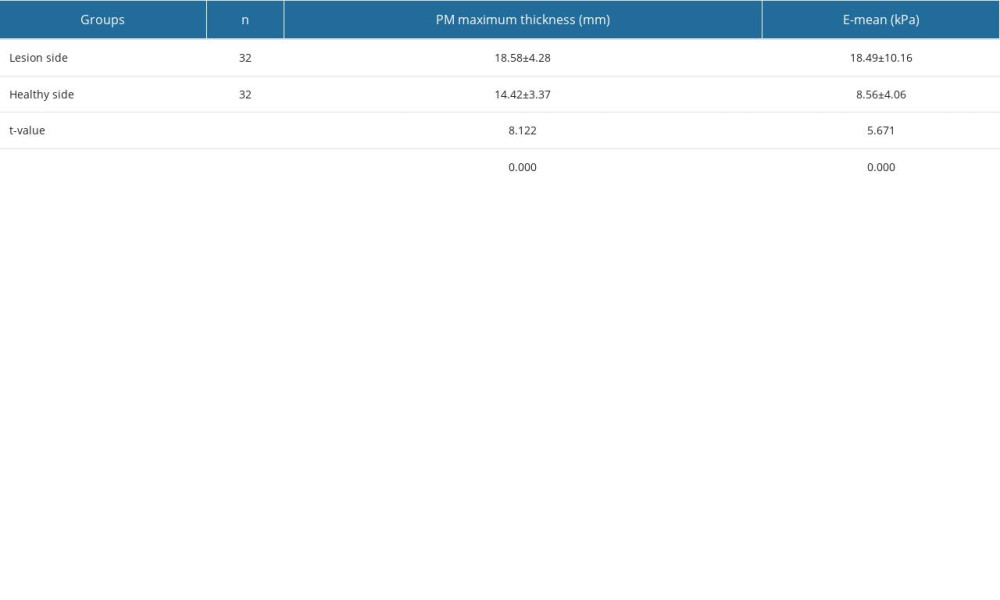 Table 2. Comparison of piriformis muscle (PM) on the affected side and healthy side in patients (χ̄±s).
Table 2. Comparison of piriformis muscle (PM) on the affected side and healthy side in patients (χ̄±s).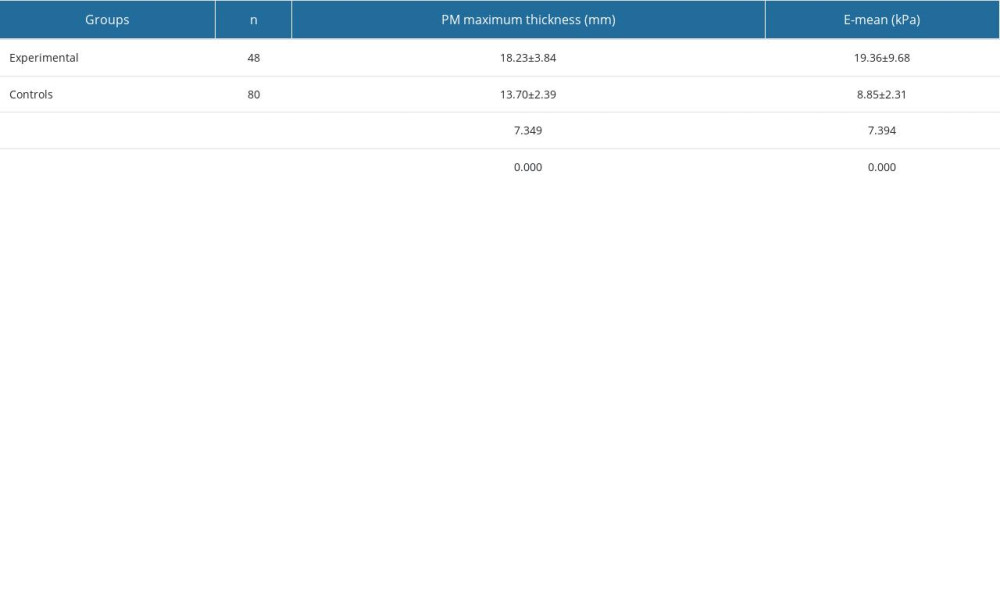 Table 3. Piriformis muscle (PM) analysis between the groups (χ̄±s).Table 1. General data comparison in patients within the groups (χ̄±s).Table 2. Comparison of piriformis muscle (PM) on the affected side and healthy side in patients (χ̄±s).Table 3. Piriformis muscle (PM) analysis between the groups (χ̄±s).
Table 3. Piriformis muscle (PM) analysis between the groups (χ̄±s).Table 1. General data comparison in patients within the groups (χ̄±s).Table 2. Comparison of piriformis muscle (PM) on the affected side and healthy side in patients (χ̄±s).Table 3. Piriformis muscle (PM) analysis between the groups (χ̄±s). In Press
07 Mar 2024 : Clinical Research
Knowledge of and Attitudes Toward Clinical Trials: A Questionnaire-Based Study of 179 Male Third- and Fourt...Med Sci Monit In Press; DOI: 10.12659/MSM.943468
08 Mar 2024 : Animal Research
Modification of Experimental Model of Necrotizing Enterocolitis (NEC) in Rat Pups by Single Exposure to Hyp...Med Sci Monit In Press; DOI: 10.12659/MSM.943443
18 Apr 2024 : Clinical Research
Comparative Analysis of Open and Closed Sphincterotomy for the Treatment of Chronic Anal Fissure: Safety an...Med Sci Monit In Press; DOI: 10.12659/MSM.944127
08 Mar 2024 : Laboratory Research
Evaluation of Retentive Strength of 50 Endodontically-Treated Single-Rooted Mandibular Second Premolars Res...Med Sci Monit In Press; DOI: 10.12659/MSM.944110
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952