11 December 2020: Clinical Research
The Predictive Value of the Follicular Output Rate on Pregnancy Outcome of Patients with Polycystic Ovary Syndrome Undergoing Fertilization and Embryo Transfer
Haiyan Yang1ABCEF, Jia Lin1ABE, Congcong Jin1BCF, Lvhe Meng1CDF, Suichun Wu1CDE, Ya Chen1ABDEG*DOI: 10.12659/MSM.916175
Med Sci Monit 2020; 26:e916175






Abstract
BACKGROUND: This retrospective study aimed to evaluate the predictive value of the follicular output rate (FORT) on the pregnancy outcome of patients with polycystic ovary syndrome (PCOS) undergoing in vitro fertilization and embryo transfer (IVF-ET).
MATERIAL AND METHODS: Between January 2012 and June 2016, a total of 1,541 patients with PCOS who underwent IVF-ET at our center were enrolled in the study. FORT was calculated as the pre-ovulatory follicle count (PFC)/antral follicle count (AFC)×100%.
RESULTS: According to the FORT, patients were divided into low, medium, and high FORT groups. With an increase in the FORT, the PFC and serum estradiol at the day of human chorionic gonadotropin (hCG) injection, the number of retrieved oocytes, metaphase II (MII) oocytes, total number of embryos, and number of high-quality embryos significantly increased (P<0.05 and P<0.001) from the low to high FORT groups, while the AFC, gonadotropin (Gn) stimulation day, and total Gn decreased significantly (P<0.001). The live birth rate from frozen embryo transfer and the cumulative live birth rate was the lowest in middle FORT group but increased significantly in high FORT group (P<0.05). The correlation analysis between FORT and related factors showed that the FORT was negatively correlated with body mass index (BMI), Gn stimulation days, and total Gn (P<0.05).
CONCLUSIONS: FORT is a powerful tool for measuring ovarian reactivity. For patients with PCOS, a high FORT to obtain high-quality embryos and perform frozen embryo transplantation can achieve good pregnancy outcome.
Keywords: Embryo Transfer, Pregnancy Complications, Reproductive Techniques, Assisted, Fertilization in Vitro, Live Birth, Ovarian Follicle, Ovulation Induction, Predictive Value of Tests, Pregnancy, Pregnancy Outcome, Sperm Injections, Intracytoplasmic
Background
Controlled superovulation is essential in the implementation of assisted reproductive technology. Optimization of the ovulation program will ensure that the antral follicle will respond appropriately to follicle-stimulating hormone (FSH). Also, the use of high-quality oocytes is a prerequisite for a good pregnancy outcome [1]. Although the antral follicle count (AFC), basal follicle stimulating hormone (FSH), and anti-Müllerian hormone (AMH) have been used to predict ovarian reactivity [2–8], they have certain limitations.
Currently, no indicator can predict both the potential ovarian response to ovulation and oocyte development [2–8]. Genro et al. proposed the concept of the follicular output rate (FORT) [9]. In 2012, Gallot et al. studied the patients with regular menstrual cycles and found that the FORT could be a quantitative indicator to reflect the potential for follicular development [10], and showed that a higher FORT was associated with improved pregnancy outcome. Also, Hassan et al. investigated patients with unexplained infertility and showed that the number of high-quality embryos and the clinical pregnancy rate increased with increased FORT [11], and that FORT was an independent variable affecting the outcome of pregnancy.
In patients with polycystic ovary syndrome (PCOS), the number of follicles for
Therefore, this retrospective study aimed to evaluate the predictive value of the follicular output rate (FORT) on the pregnancy outcome of patients with polycystic ovary syndrome (PCOS) undergoing
Material and Methods
PATIENTS STUDIED:
A retrospective study included a total of 1,541 patients with polycystic ovary syndrome (PCOS) undergoing
Study participants were included based on the diagnostic criteria recommended by the 2004 European Society of Human Reproduction and Embryology (ESHRE) and the American Society of Reproductive Medicine (ASRM) consensus [14]. Women were diagnosed with PCOS if they had two of the following three conditions, oligo-ovulation or anovulation, clinical or biochemical signs of hyperandrogenism, and polycystic ovaries. Patients with a history of ovarian surgery, or pelvic surgery within six months before the study, or having significant impairment of ovarian function due to radiotherapy or chemotherapy were excluded. Also, patients with contraindications for treatment with gonadotropin (Gn), endometriosis, adenomyosis, hydrosalpinx, uterine cavity abnormalities, thyroid dysfunction, congenital adrenal hyperplasia, Cushing syndrome, or patients with androgen-secreting tumors were excluded. Patients included in the study were aged between 21–43 years, and the duration of infertility was 2–15 years. All patients underwent a standardized long agonist protocol. The Clinical Research Ethics Committee of the First Affiliated Hospital of Wenzhou Medical University (Approval No. 2017-209) approved the study and written informed consent was obtained from all study participants.
TREATMENT PROTOCOL OF THE SUPEROVULATION PROGRAM:
All patients received a standardized pituitary down-regulation protocol with the gonadotropin-releasing hormone (GnRH) analog, decapeptyl (Ferring, Saint-Prex, Switzerland) at 5 days and 7 days after ovulation, or 14 days after the blended short-acting oral contraceptive pill was offered. At 13–14 days after pituitary down-regulation, serum follicle-stimulating hormone (FSH), luteinizing hormone (LH), estradiol (E2) and progesterone (P) were measured using a chemiluminescence microparticle immunoassay with a Unicel DXI800 chemiluminescence analyzer (Beckman Coulter, Brea, CA, USA) according to manufacturer’s instructions. The antral follicle count (AFC) was assessed by transvaginal ultrasound using a color Doppler ultrasound scanner (Polytron Technologies, Shenzhen, China). If E2 was <50 pg/ml, LH was <5 IU/L, FSH was <5 IU/L, and endometrial thickness was <5 mm, complete pituitary desensitization was achieved. The initial Gn was administered with a recombinant follicle stimulating hormone (rFSH), gonal F (Merck Serono, Geneva, Switzerland) or puregon (N.V. Organon, Molenstraat, the Netherlands) at doses between 75–150 IU/day according to the age, serum hormone levels and AFC, and body mass index (BMI) of patients. The Gn dose was adjusted according to the number and development of follicles, endometrial thickness, and serum hormone levels. 200–250 μg trigger of human chorionic gonadotropin (rhCG) ovidrel (Merck Serono, Geneva, Switzerland) was given when the diameter of dominant follicle was >18 mm, or the diameters of two dominant follicles were >17 mm, or the diameters of three dominant follicles were >16 mm.
FOLLICULAR OUTPUT RATE (FORT) CALCULATION AND PATIENT GROUPING:
The antral follicle count (AFC) with a diameter of 3–10 mm at baseline and the pre-ovulatory follicle count (PFC) with a diameter of 16–22 mm on the day of hCG injection were recorded. FORT was calculated as PFC/AFC×100%. All patients were divided into low, medium, and high groups according to FORT tertile values.
OOCYTE RETRIEVAL, TRANSFER, LUTEAL SUPPORT, AND SELECTION OF HIGH-QUALITY EMBRYOS:
Oocyte retrieval was performed 34–36 h after the administration of hCG and oocytes were fertilized either by conventional IVF or by intracytoplasmic sperm injection (ICSI) or by half ICSI based on the semen condition, the couple’s history and the guidelines of our center. Conventional IVF was usually performed for patients with female factors of infertility (such as tubal factor or ovulation dysfunction). ICSI was usually performed for patients with a male factor of infertility, such as severe oligospermia, teratospermia, azoospermia, or cyclocephalospermia. Half the ICSI was usually performed for Patients with primary infertility with normal semen when the period of sterility exceeded five years. From the day of oocyte retrieval, intramuscular progesterone (40–60 mg/day) (Xianju Pharmaceuticals, Zhejiang, China) or crinone (90 mg/day) (Merck Serono, Geneva, Switzerland) and dydrogesterone (20 mg/day) (Abbott Labs, Abbott Park, Ill, USA) were administered as luteal support until 10 weeks after conception. Morphological observation and fresh-embryo transfer were performed 3 days after oocyte retrieval. Embryos were assessed according to the number of embryonic cells, embryo size, morphology, and the percentage of fragmentation. Embryos with two prokaryotic nuclei (2PN) sources, <0% debris, and 7–9 cells were judged to be high-quality. If possible, 1–2 embryos were transferred, and the remaining embryos were cryopreserved. If the patient was found to be at high risk for ovarian hyperstimulation syndrome (OHSS), the transfer was cancelled, and all high-quality embryos were cryopreserved for later transfer.
OUTCOMES OF PREGNANCY:
Serum β-hCG was measured 2 weeks after embryo transfer, and 28 days after embryo transfer, vaginal ultrasound examination was made using a Hi-Vision Preirus digital color ultrasonic scanner (Hitachi, Tokyo, Japan). Clinically, pregnancy was defined as the presence of a gestational sac in the uterine cavity 4 weeks after embryo transfer. Live birth rate was defined as the delivery of any viable infant after embryo transfer. The cumulative live birth rate was defined as the delivery of any viable infant after the first embryo transfer and subsequent frozen embryo transfer (FET).
FROZEN EMBRYO TRANSFER (FET):
FET was performed if fresh embryo transfer failed. Serum FSH, LH, E2, and P were assessed, and the endometrium was assessed by transvaginal ultrasound scan 2–5 days after the menstrual cycle. If these examinations were normal, oral estradiol valerate (4–8 mg/day) (Delpharm, Lille, France) was administered for endometrial preparation. Intramuscular progesterone (40 mg/day) or utrogestan (600 mg/day) and dydrogesterone (40 mg/day) (Laboratoires Besins International, Montrouge, France) were administered when the endometrial thickness reached 8 mm, and E2 was ≥200 pg/ml. FET and pregnancy outcome were performed, as described above.
CALCULATION OF CUMULATIVE LIVE BIRTH RATE:
The cumulative live birth rate was calculated as the number of live births after fresh embryo transfer and FET cycles/number of cycles.
STATISTICAL ANALYSIS:
Power analysis was performed before study initiation to determine sample size. Using an estimated cumulative live birth rate 5% change in subsequent trial analysis, We determined that a sample size of 1,500 patients (500 patients per group) was necessary to achieve a power of 80% at an α of 5%. Data were expressed using the mean ± standard deviation (SD) and compared using the Student’s t-test, analysis of variance (ANOVA) and Tukey’s post hoc test. The rate was compared using Pearson’s chi-squared (χ2) test. Correlation between FORT and other factors was analyzed using the Spearman correlation, and the importance of different variables in multiple linear regression was calculated. All statistical analysis was performed using SPSS version 19.0 (IBM, Chicago, IL, USA). A P-value of 0.05 was considered as statistically significant.
Results
BASELINE STATUS:
The follicular output rate (FORT) on the pregnancy outcome of 1541 women with polycystic ovary syndrome (PCOS) undergoing
COMPARISON OF PARAMETERS BETWEEN PREGNANCY AND NON-PREGNANCY, AND LIVE BIRTHS AND NON-LIVE BIRTHS AFTER FRESH TRANSFER CYCLES:
Our results showed that the FORT was not significantly different between 669 clinical and 391 non-pregnancy cycles. However, the number of fertilized oocytes (8.38±4.03 vs. 7.51±4.14, P<0.05), the fertilization rate (73.89±17.71 vs. 70.16±20.50, P<0.05), the total number of embryos (7.61±3.99 vs. 6.67±4.14) (P<0.001), the number of transferred embryos (2.03±0.21 vs. 1.97±0.28, P<0.001) and the number of high-quality embryos (4.17±2.95 vs. 3.30±2.73, P<0.001) were significantly higher in clinical pregnancy group (Table 1). Similarly, no difference in FORT values was found between 545 live births and 515 non-live births.
However, the duration of infertility (3.86±2.44 vs. 4.27±2.67, P<0.05), the number of metaphase II (MII) oocytes (11.59±4.87 vs. 10.82±5.15, P<0.05), fertilized oocytes (8.43±3.96 vs. 7.6 6±0.67, P<0.05), the total number of embryos (7.64±3.94 vs. 6.92±4.16, P<0.05), the number of high-quality embryos (4.247±2.95 vs. 3.40±2.673, P<0.001) were significantly higher in patients giving live births than in patients giving non-live births (Table 2).
COMPARISON OF PARAMETERS AMONG THE FORT GROUPS:
The average FORT was 25.49. According to the FORT tertile values, the patients were divided into high, medium and low groups, with 516 low FORT cases with FORT values below the 33rd percentile, 529 medium FORT cases with FORT values between the 33rd and the 67th percentile, and 498 high FORT cases with FORT values above the 67th percentile.
Post hoc power analysis showed that the differences among the groups were significant for AFC (P=0.00), PFC (P=0.00), serum estradiol on the hCG day (P=0.00), MII oocytes (P=0.00), freeze-all rate (P=0.00, between low and high FORT groups for stimulation days (P=0.04), total FSH dose (P=0.00), between low and middle or middle and high FORT groups for fertilized oocytes (P=0.000, P=0.002), retrieved oocytes (P=0.00, P=0.01), total number of embryos (P=0.000, P=0.002), number of excellent quality embryos (P=0.000, P=0.01), live birth rate of frozen- embryos transfer (P=0.029, P=0.004), and between middle and high FORT groups in cumulative live birth rate (P=0.006).
We found that with the increase of FORT, PFC, serum E2 at the day of hCG injection, the number of retrieved oocytes, MII oocytes, the total number of embryos, the number of high-quality embryos, embryo-frozen rate and the number of subsequent FET cycles increased significantly (P<0.001), while AFC, Gn stimulation days and total Gn amount decreased significantly (P<0.001) in the three groups (Table 3). However, the clinical pregnancy rate and the live birth rate of the new transplant cycles did not increase with the increase of these parameters, such as the number of high-quality embryos. The pregnancy loss rate was the highest, and the live birth rate was the lowest in the high FORT group, although the differences were not significant among the groups. The clinical pregnancy rate in high FORT group following subsequent FET was similar to those in the other groups, but the pregnancy loss rate was the lowest, leading to the higher live birth rates and the highest cumulative live birth rates as compared to the other two groups (P<0.001).
CORRELATION BETWEEN THE FORT AND RELATED FACTORS:
Spearman correlation analysis showed that there was no correlation between FORT and age, basal FSH, or basal E2. However, FORT was negatively correlated with BMI (r=−0.80, P<0.05), total Gn (r=−0.50, P<0.05) and Gn stimulation day (r=−0.067, P<0.05) (Table 4).
Discussion
The findings from this study showed that the numbers of retrieved oocytes, metaphase II (MII) oocytes, high-quality embryos, pre-ovulatory follicle count (PFC), and estradiol (E2) on the day of human chorionic gonadotropin (hCG) injection increased significantly and progressively with the increase in the follicular output rate (FORT). This finding is consistent with the results previously reported in non-PCOS patients [10,11], but different from the results obtained with patients with PCOS [13]. It was found that in patients with PCOS, PFC and retrieved oocytes, but not fertilization rate and the number of high-quality embryos, increased correspondingly with the increase of FORT, which was the highest in medium FORT group [13]. Also, we did not find any difference in fertilization rate between the three groups. This finding is consistent with the earlier results in non-PCOS patients [10,13], but is different from other studies in patients with PCOS [11,13]. The difference between our results and other studies may be due to the difference in the study populations and the number of cases investigated. Despite these inconsistencies, these results showed that the FORT is a predictor for ovarian response to follicle-stimulating hormone (FSH), oocyte development potential, and embryo quality.
The results from the present study showed that in the lowest FORT group, antral follicle count (AFC), gonadotropin (Gn) stimulation days and total Gn were the highest, and were significantly higher than other two groups. Zhang et al. also found the highest AFC, Gn stimulation days but not total Gn in the low FORT group [15]. Gallon et al. and Hassan et al. showed that AFC was also the highest in the low FORT group, but there was no difference in Gn stimulation days and total Gn [10,11]. Even though more Gn and longer Gn duration were used to promote ovulation, the final PFC, E2 on the day of hCG injection, the number of retrieved oocytes, MII oocytes, the total number of embryos and the number of high-quality embryos were far lower in the low FORT group than in the high FORT group. As for the difference between patients with PCOS and non-PCOS patients, we speculate that there may be several unknown differences except for the difference in the quantity of the follicles between PCOS and non-PCOS patients. For example, it has been shown that ovarian IGF system in patients with PCOS is abnormal [15], which may affect the production of follicles in superovulation therapy. Liu et al. found that in patients with PCOS, ANGPTL1, and ANGPTL2 mRNA were expressed abnormally in cumulus [16], leading to reduced oocyte quality and decreased development potential. Therefore, an increased number of antral follicles in patients with PCOS may result in more reduced response to FSH, leading to less PFC, lower fertilization rate, lower number of high-quality embryos and the total number of embryos despite more and more prolonged Gn treatment. It is also possible that due to a higher number of antral follicles in patients with PCOS, they are more likely to have ovarian hyperstimulation syndrome (OHSS) when ovulation is stimulated, and it is not suitable to use a high trigger dose of Gn. As a result, the optimal time for the recruitment and development of follicles might have missed, ultimately leading to reduced follicular reactivity, fewer retrieved oocytes, fewer mature oocytes, and fewer high-quality embryos.
In the present study, the number of subsequent frozen embryo transfer (FET) cycles were the highest in the high FORT group. The average FORT of patients with PCOS was much lower than that of non-PCOS patients, but because of large number of antral follicles, high FORT also increased the number of oocytes with an increased risk of ovarian hyperstimulation syndrome (OHSS), resulting in a higher rate of freeze-all and a more significant number of subsequent FET cycles. Although the number of high-quality embryos increased with FORT, the clinical pregnancy rate and live birth rate of new transplant cycle did not increase significantly with the increase of FORT, the abortion rate was the highest in high FORT group, resulting in the lowest live birth rate in the group. Our study also shows that there is no difference in FORT values between pregnant and non-pregnant patients and between patients giving live and non-live births during the new transfer cycles. This finding was different from the results obtained in non-PCOS patients but was similar to those obtained in patients with PCOS, where patients with medium FORT had the best pregnancy outcome [15].
The reason for the different results in patients with PCOS and non-PCOS patients may be because of differences in the endometrium. Huang et al. found that serum factor X (FX) of patients with PCOS significantly increased at the day of hCG injection and the embryo transfer day, serum factor VIII (FVIII) level significantly reduced at embryo transfer day, and hypercoagulability during the peri-implantation period resulted in poor microcirculation in the endometrium [17]. For the high FORT patients with PCOS, they had the highest levels of E2 on the day of hCG injection, which had most significant impact on the endometrium. As a result, the pregnancy outcome is not as good as expected after fresh embryo transfer. The best cumulative live birth rate also confirms this, following subsequent FET treatment in high FORT patients, a result that is consistent with the earlier study [18]. Therefore, the adverse effects of high E2 on the endometrium in the high FORT group are eliminated during FET, leading to the lowest abortion rate and highest live birth rate and consequently the best pregnancy outcome in the high FORT group.
The correlation analysis showed that the FORT does not correlate with age, basal FSH and E2 negatively correlated with BMI, AFC, Gn stimulation days and total Gn, and positively correlated with PFC, suggesting that the FORT was a relatively independent indicator. FORT in combination with AFC could have a stable and independent assessment of ovarian functional reserve and the prediction of IVF-ET outcome. This finding also suggests that AFC does not lose its response to FSH sith increased age [19]. Unfortunately, this study did not analyze the correlation between FORT and anti-Müllerian hormone (AMH). Additionally, we showed that the FORT was negatively correlated with body mass index (BMI), which is consistent with earlier work [20]. They believed that leptin inhibits the synthesis and stimulation of granulocyte steroid hormone in obese patients, and obesity could be an independent factor that negatively affects IVF-ET [20].
This study had several limitations. As a retrospective study, there may have been some changes in the antral follicular count and follicular size on hCG day as assessed by different physicians. Superovulation was performed by different physicians, leading to different medications. Also, because PCOS is a high-responsive population, if it is unclear whether the Gn dosage and duration were controlled, this may have an impact on the outcome. Nevertheless, we calculated the cumulative pregnancy rate, which can reflect the utilization rate of eggs and embryos in each cycle. The findings from this study provide a relatively more objective evaluation of treatment outcome of IVF-ET.
Conclusions
This retrospective study aimed to evaluate the predictive value of the follicular output rate (FORT) on the pregnancy outcome of patients with polycystic ovary syndrome (PCOS) undergoing
Tables
Table 1. Baseline characteristics and ovarian stimulation data in pregnant and non-pregnant women in 1060 fresh-embryo transfers.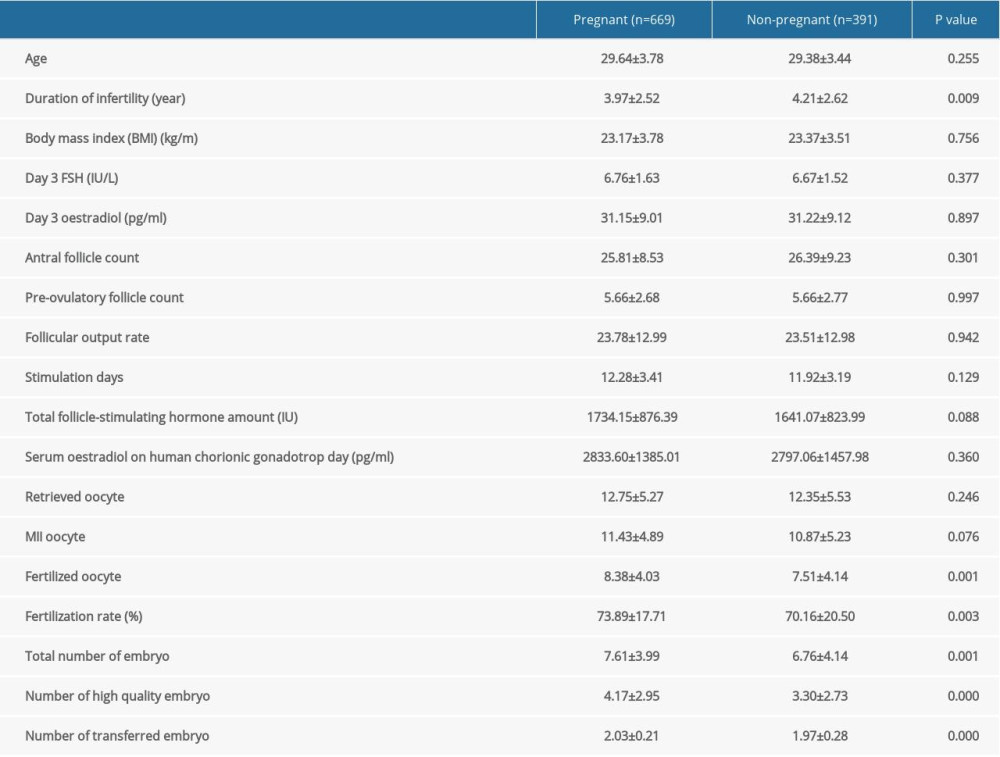 Table 2. Baseline characteristics and ovarian stimulation data in live birth and non-live birth women in 1060 fresh-embryo transfer.
Table 2. Baseline characteristics and ovarian stimulation data in live birth and non-live birth women in 1060 fresh-embryo transfer.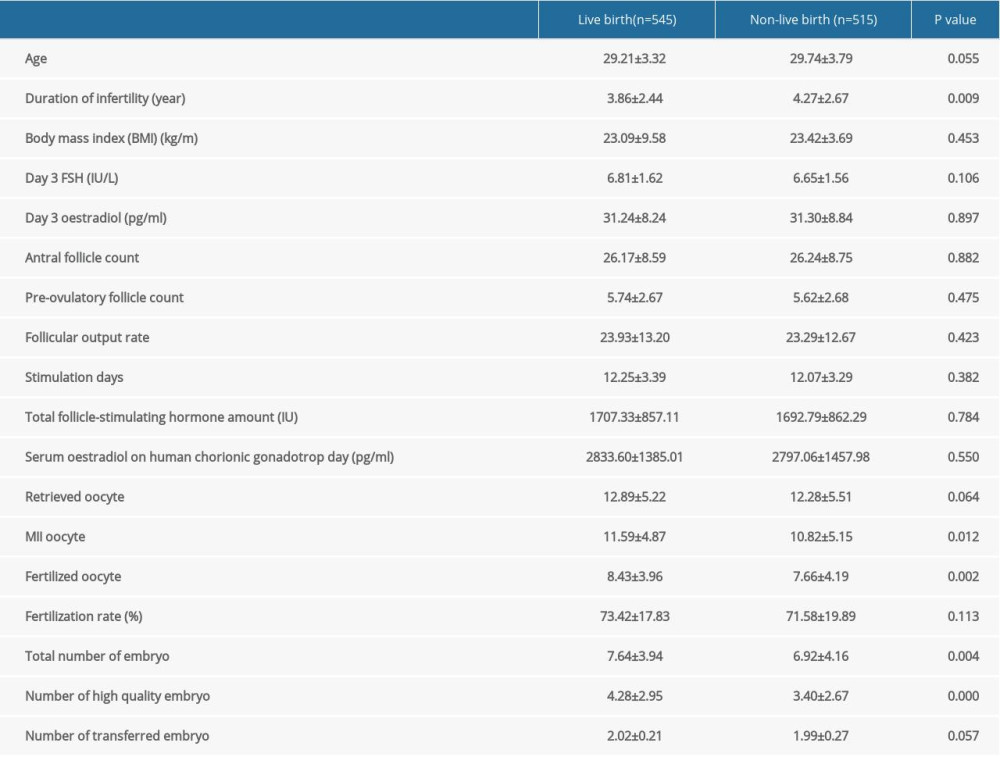 Table 3. Baseline characteristics, ovarian stimulation data and IVF/ICSI outcomes in the low, medium and high FORT groups.
Table 3. Baseline characteristics, ovarian stimulation data and IVF/ICSI outcomes in the low, medium and high FORT groups.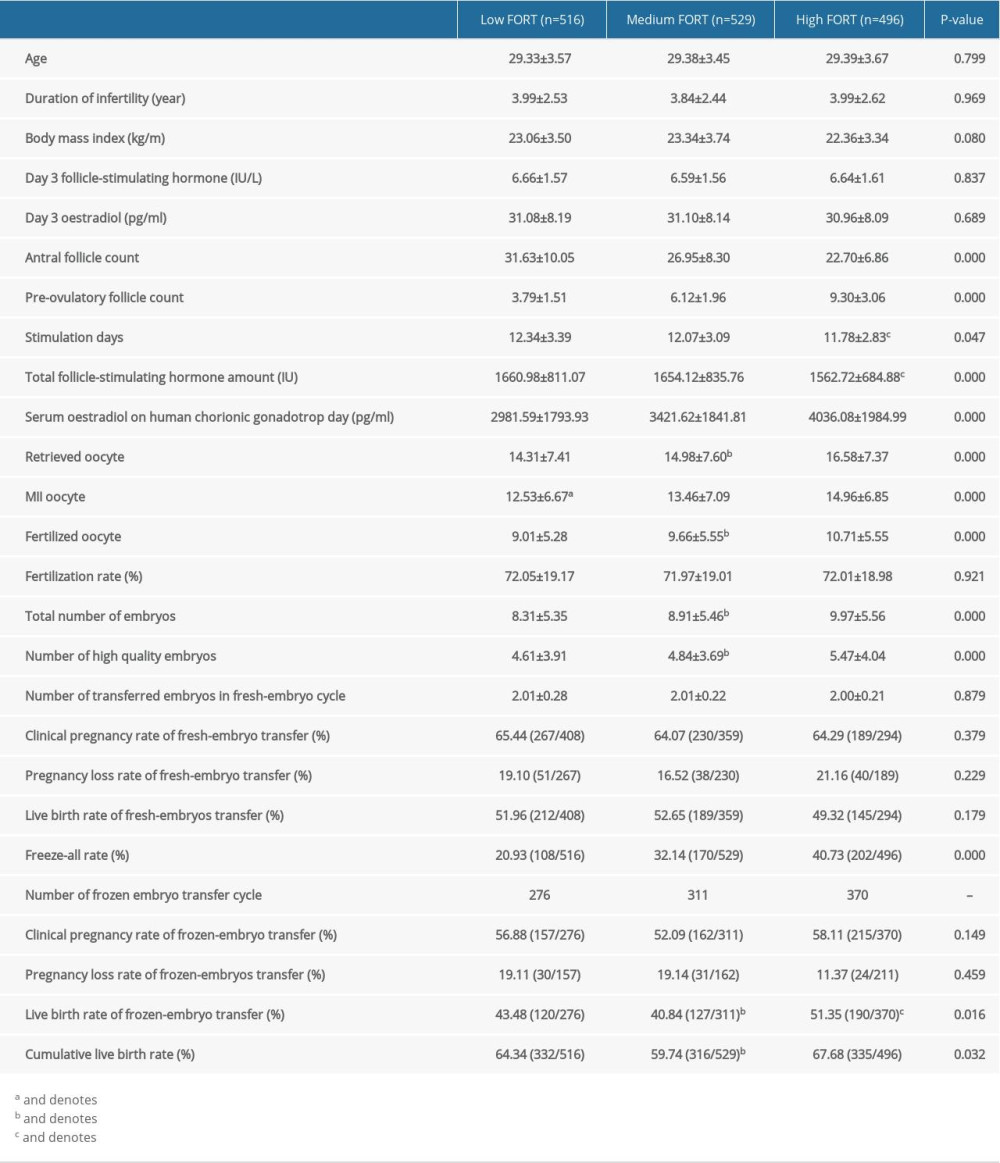 Table 4. Univariate analysis of factors associated with FORT.
Table 4. Univariate analysis of factors associated with FORT.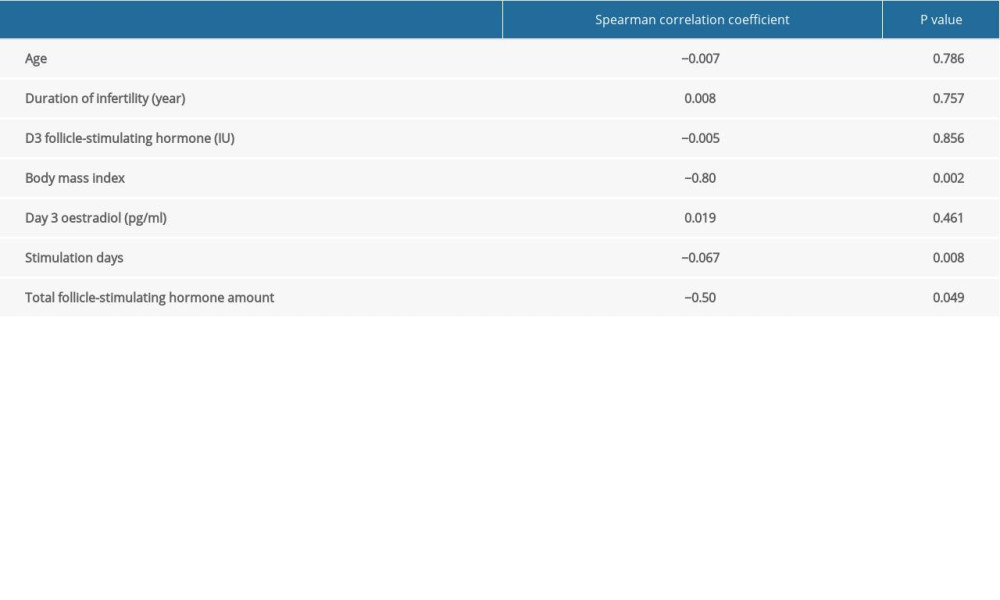
References
1. Arce JC, Andersen AN, Fernandez-Sanchez M: Fertil Steril, 2014; 102(6); 1633-40
2. de Carvalho BR, Rosa E, Silva AC, Ovarian reserve evaluation: State of the art: J Assist Reprod Genet, 2008; 25(7); 311-22
3. Barad DH, Weghofer A, Gleicher N, Comparing anti-Mullerian hormone (AMH) and follicle-stimulating hormone (FSH) as predictors of ovarian function: Fertil Steril, 2009; 91(4 Suppl); 1553-55
4. Wunder DM, Guibourdenche J, Birkhauser MH, Bersinger NA: Fertil Steril, 2008; 90(6); 2203-10
5. Lee TH, Liu CH, Huang CC, Serum anti-Mullerian hormone and estradiol levels as predictors of ovarian hyperstimulation syndrome in assisted reproduction technology cycles: Hum Reprod, 2008; 23(1); 160-67
6. Bancsi LF, Broekmans FJ, Mol BW: Fertil Steril, 2003; 79(5); 1091-100
7. Broer SL, Mol BW, Hendriks D, Broekmans FJ, The role of antiMullerian hormone in prediction of outcome after IVF: Comparison with the antral follicle count: Fertil Steril, 2009; 91(3); 705-14
8. Melo MA, Garrido N, Alvarez C: Fertil Steril, 2009; 91(1); 148-56
9. Genro VK, Grynberg M, Scheffer JB, Serum anti-Mullerian hormone levels are negatively related to Follicular Output Rate (FORT) in normo-cycling women undergoing controlled ovarian hyperstimulation: Hum Reprod, 2011; 26(3); 671-77
10. Gallot V, Berwanger da Silva AL, Genro V: Hum Reprod, 2012; 27(4); 1066-72
11. Hassan A, Kotb M, AwadAllah A, Follicular output rate can predict clinical pregnancy in women with unexplained infertility undergoing IVF/ICSI: A prospective cohort study: Reprod Biomed Online, 2017; 34(6); 598-604
12. Heijnen EM, Eijkemans MJ, Hughes EG, A meta-analysis of outcomes of conventional IVF in women with polycystic ovary syndrome: Hum Reprod Update, 2006; 12(1); 13-21
13. Zhang N, Hao CF, Zhuang LL, Prediction of IVF/ICSI outcome based on the follicular output rate: Reprod Biomed Online, 2013; 27(2); 147-53
14. Rotterdam ESHRE/ASRM-Sponsored PCOS consensus workshop group, Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS): Hum Reprod, 2004; 19(1); 41-47
15. Zhong G, Chen B, Serum and follicular fluid levels of IGF-II, IGF-binding protein-4 and pregnancy-associated plasma protein-A in controlled ovarian hyperstimulation cycle between polycystic ovarian syndrome (PCOS) and non-PCOS women: Gynecol Endocrinol, 2011; 27(2); 86-90
16. Liu Z, Liu C, Hao C, Aberrant expression of angiopoietin-like proteins 1 and 2 in cumulus cells is potentially associated with impaired oocyte developmental competence in polycystic ovary syndrome: Gynecol Endocrinol, 2016; 32(7); 557-61
17. Huang Y, Zhao Y, Yan L, Changes in coagulation and fibrinolytic indices in women with polycystic ovarian syndrome undergoing controlled ovarian hyperstimulation: Int J Endocrinol, 2014; 2014 731498
18. Chen ZJ, Shi Y, Sun Y, Fresh versus frozen embryos for infertility in the polycystic ovary syndrome: N Engl J Med, 2016; 375(6); 523-33
19. Hanoch J, Lavy Y, Holzer H, Young low responders protected from untoward effects of reduced ovarian response: Fertil Steril, 1998; 69(6); 1001-4
20. Dayer D, Nikbakht R, Kadkhodai Elyaderani M, Comparison of leptin concentrations between infertile women with polycystic ovary syndrome and fertile women: Iran J Reprod Med, 2013; 11(12); 1033-34
Tables
Table 1. Baseline characteristics and ovarian stimulation data in pregnant and non-pregnant women in 1060 fresh-embryo transfers.Table 2. Baseline characteristics and ovarian stimulation data in live birth and non-live birth women in 1060 fresh-embryo transfer.Table 3. Baseline characteristics, ovarian stimulation data and IVF/ICSI outcomes in the low, medium and high FORT groups.Table 4. Univariate analysis of factors associated with FORT. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387