17 June 2020: Clinical Research
Clinical and Demographic Characteristics of Cluster Cases and Sporadic Cases of Coronavirus Disease 2019 (COVID19) in 141 Patients in the Main District of Chongqing, China, Between January and February 2020
Peng Chen1ABE, Ying Zhang1BCF, Yongsheng Wen1DE, Jinjun Guo1BD, Weizhi Bai1BCE, Jinwei Jia1EF, Yu Ma1ACG*, Yi Xu1BDEGDOI: 10.12659/MSM.923985
Med Sci Monit 2020; 26:e923985






Abstract
BACKGROUND: In December 2019, an outbreak of coronavirus disease 2019 (COVID-19), due to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), occurred in Wuhan, China. Patients with COVID-19 were also identified in Chongqing. This study aimed to investigate the clinical and demographic characteristics of cluster cases and sporadic cases of COVID-19 in 141 patients in the main district of Chongqing during one month, between January and February 2020.
MATERIAL AND METHODS: A retrospective study included 141 patients with a diagnosis of COVID-19. The diagnosis was confirmed using real-time reverse transcription-polymerase chain reaction (RT-PCR) for SARS-CoV-2. The patients were divided into cluster cases (n=90) and sporadic cases (n=51). Demographic and clinical characteristics were compared between the two study groups and included the presence of comorbidities, the presenting symptoms, chest computed tomography (CT) imaging findings, and laboratory findings.
RESULTS: The mean age of the 141 patients diagnosed with COVID-19 was 47.3 years, and the most common presenting symptom was a persistent cough (48.9%). The 90 cluster cases (63.8%) were older than the sporadic cases, and cross-infection from family gathering occurred in 82.2%, and cough was more common than fever, and there was an increased prevalence of asymptomatic, mild, and moderate cases. Cluster cases showed fewer typical manifestations of COVID-19 on chest CT. However, the laboratory findings between the cluster and sporadic cases showed no significant differences.
CONCLUSIONS: There were demographic and clinical differences between cluster cases and sporadic cases of COVID-19 in the main district of Chongqing during the month between January to February 2020.
Keywords: Cluster Analysis, Human Characteristics, Pneumonia, Viral, COVID-19, Betacoronavirus, COVID-19, Coronavirus Infections, Demography, Pandemics, SARS-CoV-2, Tomography, X-Ray Computed
Background
In December 2019, an outbreak of coronavirus disease 2019 (COVID-19) due to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) occurred in Wuhan, China and cases were also confirmed in Chongqing from January 20th, 2020 [1–3]. By February 25th, 2020, there were 576 confirmed cases of COVID-19 in Chongqing, including more than 150 cases in the main district of Chongqing [3].
With the continued increase in patient numbers, the proportion of cluster cases with COVID-19 due to crowd-gathering and family-gathering exceeded 60%, which has resulted in measures to prevent the spread of infection by home quarantine. Compared with sporadic cases, the clinical characteristics of cluster cases are unclear, and there have been few studies to compare cluster and sporadic cases of COVID-19. Therefore, this study aimed to investigate the clinical and demographic characteristics of cluster cases and sporadic cases of COVID-19 in 141 patients in the main district of Chongqing during one month, between January and February 2020.
Material and Methods
ETHICAL APPROVAL:
This retrospective study was conducted in accordance with the declaration of Helsinki and was approved by the Institutional Ethics Board of Chongqing Emergency Medical Center (No. 202006). Patient clinical data used in this study were anonymized.
DATA COLLECTION:
The study included 141 patients who had a confirmed diagnosis of COVID-19 using real-time reverse transcription-polymerase chain reaction (RT-PCR) for SARS-CoV-2. Patients were transferred to the designated hospitals in the main district of Chongqing from January 25th to February 25th, 2020. The patients were divided into cluster cases (n=90) and sporadic cases (n=51). Demographic and clinical characteristics were compared between the two study groups and included the presence of comorbidities, the presenting symptoms, chest computed tomography (CT) imaging findings, and laboratory findings.
Patient comorbidities that were evaluated included hypertension, diabetes, coronary heart disease, and chronic obstructive pulmonary disease (COPD). Symptoms included fever, cough, fatigue, muscle ache, sore throat, headache, rhinorrhea, dyspnea, nausea or vomiting, diarrhea, and palpitations. Chest computed tomography (CT) imaging findings and laboratory findings were recorded. The patients were divided into mild, moderate, and severe, according to clinical symptoms and the prevalence of acute respiratory distress syndrome (ARDS), acute cardiac injury, shock, and acute kidney injury (AKI). Two reviewers extracted the clinical data from the patient records, and two independent reviewers analyzed the data.
DEFINITION OF THE CLUSTER CASES AND SPORADIC CASES:
The cluster cases were cases of COVID-19 that were diagnosed in the previous 14 days in involving two or more cases caused by direct human-to-human transmission in the home, residence, workplace, and other communal places. The sporadic cases occurred in isolated individuals and were not associated with communal infection with others.
:
The clinical symptoms of patients in both groups of cluster and sporadic cases of COVID-19 were defined as mild, moderate, and severe [4]. Mild cases had mild clinical symptoms with no signs of pneumonia on CT chest imaging [4]. Moderate cases presented with fever and respiratory symptoms with no signs of pneumonia on CT chest imaging [4]. Severe cases had hypoxia with a respiratory rate of more than 30 breaths per minute, oxygen saturation <93% at rest, the Carrico index, or the ratio of oxygen partial pressure to fractional inspired oxygen (PaO2/FiO2) <300 mmHg. Some patients developed respiratory failure requiring mechanical ventilation, and some patients developed shock and organ failure and required monitoring and treatment in the Intensive Care Unit (ICU).
STATISTICAL ANALYSIS:
Data were presented as the mean±standard deviation (SD) for continuous variables and percentages for categorical variables. Statistical analysis was performed using Student’s t-test for quantitative variables and Pearson’s chi-squared (χ2) test or Fisher’s exact test for categorical variables. Data were analyzed using SPSS version 22.0 (IBM, Chicago, IL, USA). A P-value <0.05 was considered to be statistically significant.
Results
CLINICAL AND DEMOGRAPHIC PATIENT CHARACTERISTICS:
The study included 141 patients who had a confirmed diagnosis of coronavirus disease 2019 (COVID-19) in the main district of Chongqing, China, from January 25th to February 25th, 2020. The patients were divided into cluster cases (n=90) and sporadic cases (n=51). Table 1 summarizes the demographic and clinical characteristics of the 141 patients included in the study. The mean age was 47.3 years. Five patients (3.5%) were children <12 years of age, and 17 patients (12.1%) were >65 years of age. The youngest patient diagnosed with COVID-19 was 4 years of age, and the oldest was 89 years of age. There were 73 male patients (51.8%) and 68 female patients (48.2%). Comorbidities included hypertension (24.1%), diabetes (18.4%), coronary heart disease (16.3%), and chronic obstructive pulmonary disease (COPD) (12.1%). The mean time from contact to symptomatic illness, or the incubation period, was 7.9 days. The mean time from the onset of symptoms to hospital admission was 3.3 days (Table 1).
The most common presenting symptoms of COVID-19 were cough (48.9%), fever (47.5%), and fatigue (13.5%), and only 14 patients (9.9%) had symptoms of dyspnea. In 34% of patients, dry cough was present, and a productive cough was present in 14.9%. Early symptoms of COVID-19 included muscle aches (12.1%), a sore throat (9.9%), headache (9.2%), and rhinorrhea (7.8%). Nausea or vomiting occurred in 6.3% of patients, and diarrhea was present in 3.5%. Sixteen patients (11.3%) had palpitations, and 11 patients (7.8%) had an increased heart rate (≥100 bpm) (Table 1).
The cases were clinically divided into mild, moderate, and severe [4]. Mild cases accounted for 40.5%, moderate cases for 48.9%, and severe cases for 10.6%. Acute respiratory distress syndrome (ARDS) was the most common presentation in severe cases and was found in 12 patients (8.5%). Acute cardiac injury occurred in seven patients (5.0%), shock occurred in six patients (4.2%), and acute kidney injury (AKI) occurred in four patients (2.8), who required dialysis therapy.
Table 2 shows the radiology and laboratory findings in 141 patients with COVID-19. Radiological examination of the chest showed that bilateral lung involvement was most common (78.7%), and 111 patients (78.7%) showed typical manifestations of COVID-19 on chest computed tomography (CT) [3,5,6]. The findings from laboratory investigations were consistent with the features of COVID-19 infection, including a normal white blood cell count and lymphocyte count, and an increased level of C-reactive protein (CRP). Laboratory results in the moderate and severe cases showed that 27.5% of the patients had abnormal myocardial enzymes, with an increase in creatine kinase myocardial band (CK-MB) being most common. Increased levels of troponin were found in 26.7% of patients. Some moderate and severe cases (18.1%) showed acute kidney injury (AKI) with increased levels of blood urea nitrogen (BUN) and serum creatinine (Table 2).
DIFFERENCES BETWEEN THE CLUSTER CASES AND THE SPORADIC CASES:
Of the 141 patients included in the study, 90 patients (63.8%) were cluster cases, which included 74 patients who acquired COVID-19 by family-gathering (74/90, 82.2%). Of the 141 patients included in the study, 51 cases (36.2%) were sporadic. Comparison of clinical characteristics between the cluster cases and sporadic cases are shown in Table 3. In the cluster cases, the mean patient age was 50.1 years, and there were 43 male patients (47.8%). In the sporadic cases, the mean patient age was 42 years, and there were 30 male patients (58.8%). The cluster cases were significantly older than the sporadic cases of COVID-19, but there were no significant differences between the two groups in terms of gender, comorbidities, and length of the incubation period for infection (Table 3).
The clinical characteristics of the 141 patients showed that the most common symptoms in the cluster cases were cough (44.4%), followed by fever (40%). However, in sporadic cases, the most common symptoms were fever (60.8%), followed by cough (56.9%). Patients in the sporadic case group were significantly more likely to have a moderate or high fever (≥38°C). There was no significant difference between the cases for the prevalence of early symptoms of COVID-19, including symptoms of fatigue, muscle ache, sore throat, headache, and rhinorrhea. There were no significant differences between the cases for the prevalence of gastrointestinal symptoms such as nausea, vomiting, and diarrhea, for cardiac symptoms, including palpitations, or the incidence of dyspnea. However, in the cluster cases, 32.3% (29/90) of patients were asymptomatic, which was significantly higher than that in the sporadic cases in which 5.9% (3/51) of patients were asymptomatic. Cluster patients were significantly more likely to be clinically mild or moderate. Only five patients with severe symptoms were found in the cluster cases, which was significantly less than for the sporadic cases.
The prevalence of bilateral lung involvement showed no significant difference between the cluster cases and the sporadic cases. However, chest CT identified fewer typical manifestations of COVID-19 in the cluster cases, which was significantly different from sporadic cases. The laboratory findings showed that both the cluster cases and sporadic cases had normal white blood cell and lymphocyte counts and increased C-reactive protein (CRP), with no significant differences.
Compared with the sporadic cases of the COVID-19, the cluster cases were significantly older, and unlike sporadic cases, where fever was the dominant symptom, the cluster cases were more likely to present with cough and a significantly increased proportion were asymptomatic. The cluster cases were more likely to be mild or moderate cases with fewer typical manifestations of COVID-19 on chest CT when compared with the sporadic cases. Figures 1 and 2 show representative chest CT images in an example of a cluster case and a sporadic case, respectively.
Discussion
As of February 25, 2020, the number of confirmed cases of infection from coronavirus disease 2019 (COVID-19) due to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in Wuhan, and mainland China increased leading to increased prevention programs [1,7–10]. The number of confirmed cases in many other provinces and cities outside Hubei province continued to decline. However, for confirmed cases in the main district of Chongqing, almost cases were caused by crowd-gathering. Although early-stage prevention with home quarantine effectively controlled the spread of COVID-19, with the gradual resumption of work and production, the risk of crowd-gathering to spread disease would be expected to increase. The prevention of cluster spread of COVID-19 when work resumes in China is an important issue.
The characteristics of cluster cases of COVID-19 has remained unclear, which has hindered the assessment and prevention of the disease of cluster spread. This study aimed to investigate the clinical and demographic characteristics of cluster cases and sporadic cases of COVID-19 in 141 patients in the main district of Chongqing during one month, between January and February 2020. The findings may provide guidance for the prevention of local epidemics, and to provide a reference for the development of prevention strategies in other provinces and regions.
In the present study, out of 141 patients with COVID-19, the mean age was 47.3 years, and 51.8% of the cases were male patients. The findings from this study supported those of previous studies that there was a relationship between COVID-19 and patient comorbidity [11]. The most common comorbidity was hypertension, followed by diabetes and coronary heart disease. The mean incubation period of 7.9 days was longer than previously reported [12,13]. Also, the time from the onset of symptoms to hospital admission, of 3.3 days, was shorter than previously reported [7]. This finding may have reflected that because patients were more alert to COVID-19, minor symptoms prompted patients to seek rapid medical assistance.
In this study, some patients presented with muscle aches, a sore throat, and other early symptoms of COVID-19, which was different from some previous studies in which fever was the main symptom [7,14]. There were more patients with cough in this study, with a significantly higher proportion with a dry cough. The proportion of severe cases was also lower than that reported in Wuhan and Hubei province [3,7,15]. It is possible that the pathogenicity of the virus was reduced, or that treatment improved, leading to a reduction in the proportion of severe cases.
In most patients in this study, radiological examination showed bilateral lung involvement with typical chest computed tomography (CT) findings of COVID-19 in most patients. Laboratory examination showed normal white blood cell counts and lymphocyte counts and increased levels of C-reactive protein. These findings were similar to those previously reported in patients with COVID-19 in Wuhan and Hubei provinces [7,15].
In all the 141 patients, 90 patients (63.8%) were cluster cases, and 51 patients (36.2%) were sporadic cases. With the spread of COVID-19 in the main district of Chongqing, the number of cluster cases exceeded the sporadic cases. The cluster cases were significantly older and associated with family gatherings (82.2%). There was no difference in the proportion of comorbidities and the incubation period between cluster cases and sporadic cases [16].
Unlike sporadic cases, in which fever was the dominant symptom, the cluster cases included more patients who presented with a cough. Previous studies have shown that cluster cases of COVID-19 were prone to present with gastrointestinal symptoms, of which diarrhea was the most common symptom [16]. The findings from this study showed no significant differences between the cluster and sporadic cases for gastrointestinal symptoms of nausea, vomiting, and diarrhea, or cardiac symptoms, or dyspnea. However, in this study, a significantly greater proportion of asymptomatic patients were found in the cluster cases, with a significantly lower proportion of severe cases. Also, there were fewer typical manifestations of COVID-19 on chest CT in the cluster cases compared with the sporadic cases. It has previously been reported that asymptomatic individuals are potential sources of COVID-19 infection [17,18]. For cluster cases, although symptoms were less severe and included asymptomatic cases, mild and moderate cases were increased, which may indicate that more attention should be given to disease prevention in the cluster cases.
As a municipality directly under the central government, Chongqing is adjacent to the west of Hubei province and 940 kilometers from Wuhan. Chongqing has a population of about 31 million, of which the main district has a population of about 8.55 million. The spread of COVID-19 has recently been reduced using home quarantine strategy, but migration between Chongqing and Wuhan and the gradual resumption of work will increase the risk of crowd gatherings, which may result in an increased spread of disease. The prevention of infection caused by crowd gatherings, especially in shopping malls, schools, and supermarkets, should be the required next stage of disease control [19]. By comparing cluster cases and sporadic cases, the characteristics of cluster cases have been identified, which have shown that patients who had mild symptoms or who were asymptomatic had the potential to transmit COVID-19.
The results of this study highlighted the importance of formulating effective and targeted disease prevention measures. For example, more comprehensive measures are required for screening patients, especially for older people who gather in public places, equipping individuals with personal protection equipment (PPE) when they return to work, schools, and crowded places, and reducing unnecessary crowd gatherings [20,21]. Also, the findings from this study support that medical assistance should be sought quickly for symptoms of cough and fever [20,21].
This study had several limitations. Firstly, this was a retrospective study that included data obtained from designated hospitals in the main district of Chongqing. Future studies to compare cluster and sporadic cases of COVID-19 should increase the number of patients included in the study. This study was of a short duration of one month, and the length of hospital stay, cure rate, mortality, and other indicators such as other comorbidities, require further study. Also, to reduce infection risk, not all patients with COVID-19 patients had blood biochemistry, and electrocardiogram (ECG), ultrasound examination, and other investigations, which indicates that future prospective studies are required.
Conclusions
This study aimed to investigate the clinical and demographic characteristics of cluster cases and sporadic cases of COVID-19 in 141 patients in the main district of Chongqing during one month, between January and February 2020. There were demographic and clinical differences between cluster cases and sporadic cases of COVID-19, with more cluster cases. Cluster cases were older than sporadic cases, and infection occurred due to family gatherings and cross-infection. The spread of the disease was effectively controlled by home quarantine, which reduced the symptoms. There were fewer typical manifestations of COVID-19 on chest CT in cluster cases compared with sporadic cases. Cluster cases also included asymptomatic individuals. These findings may have implications for the spread of infection when the population begins to return to work, as the clinical characteristics of the cluster cases indicate that comprehensive measures may be required to prevent the further spread of COVID-19, including comprehensive surveillance, wearing masks in public places, reducing unnecessary social and family gathering, and timely medical treatment.
Figures
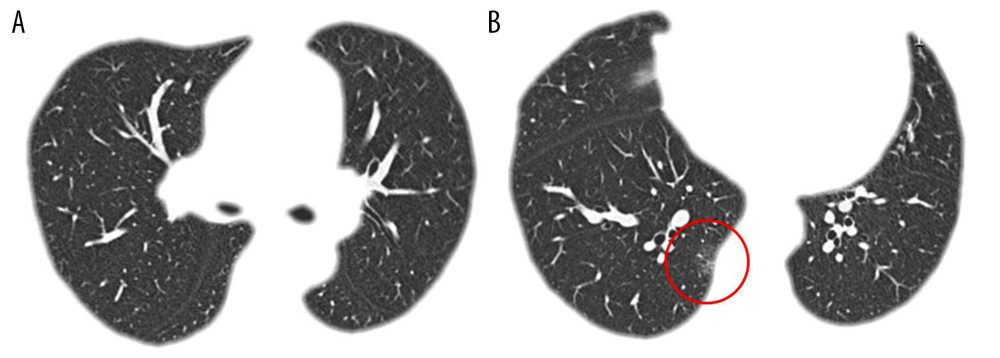 Figure 1. A cluster case of coronavirus disease 2019 (COVID-19). Transverse chest computed tomography (CT) images of a 30-year-old female patient on hospital admission. The patient had symptoms of a cough for three days. (A, B) Ground-glass opacities are shown in the posterior basal segment of the right lower lobe, indicating the presence of interstitial inflammation.
Figure 1. A cluster case of coronavirus disease 2019 (COVID-19). Transverse chest computed tomography (CT) images of a 30-year-old female patient on hospital admission. The patient had symptoms of a cough for three days. (A, B) Ground-glass opacities are shown in the posterior basal segment of the right lower lobe, indicating the presence of interstitial inflammation. 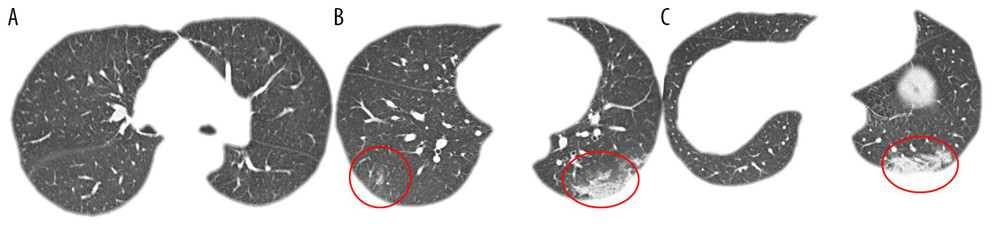 Figure 2. A sporadic case of coronavirus disease 2019 (COVID-19). Transverse chest computed tomography (CT) images of a 32-year-old female patient on hospital admission. The patient had symptoms of a fever and cough for two days. (A–C) Ground-glass opacities are shown in both lower lobes with a ‘crazy-paving’ pattern of lung consolidation in the posterior basal segment of the left lower lobe.
Figure 2. A sporadic case of coronavirus disease 2019 (COVID-19). Transverse chest computed tomography (CT) images of a 32-year-old female patient on hospital admission. The patient had symptoms of a fever and cough for two days. (A–C) Ground-glass opacities are shown in both lower lobes with a ‘crazy-paving’ pattern of lung consolidation in the posterior basal segment of the left lower lobe. Tables
Table 1. Clinical and demographic characteristics of 141 patients with a confirmed diagnosis of coronavirus disease 2019 (COVID-19) in the main district of Chongqing, China, from January 25th to February 25th, 2020.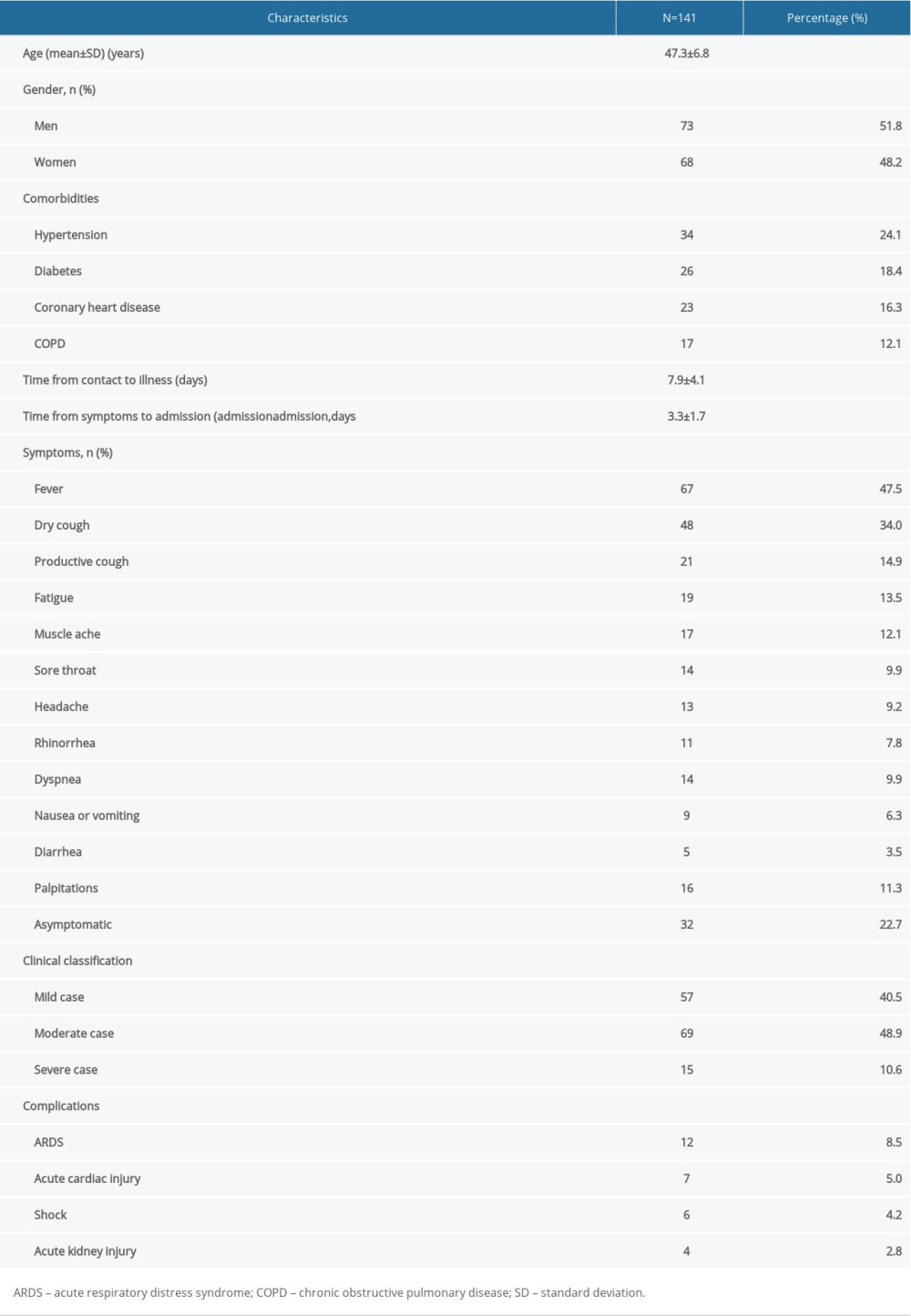 Table 2. Radiology and laboratory findings in 141 patients with a confirmed diagnosis of coronavirus disease 2019 (COVID-19) in the main district of Chongqing, China, from January 25th to February 25th, 2020.
Table 2. Radiology and laboratory findings in 141 patients with a confirmed diagnosis of coronavirus disease 2019 (COVID-19) in the main district of Chongqing, China, from January 25th to February 25th, 2020. Table 3. The clinical characteristics of cluster and sporadic cases of coronavirus disease 2019 (COVID-19) in the main district of Chongqing, China, from January 25th to February 25th, 2020.
Table 3. The clinical characteristics of cluster and sporadic cases of coronavirus disease 2019 (COVID-19) in the main district of Chongqing, China, from January 25th to February 25th, 2020.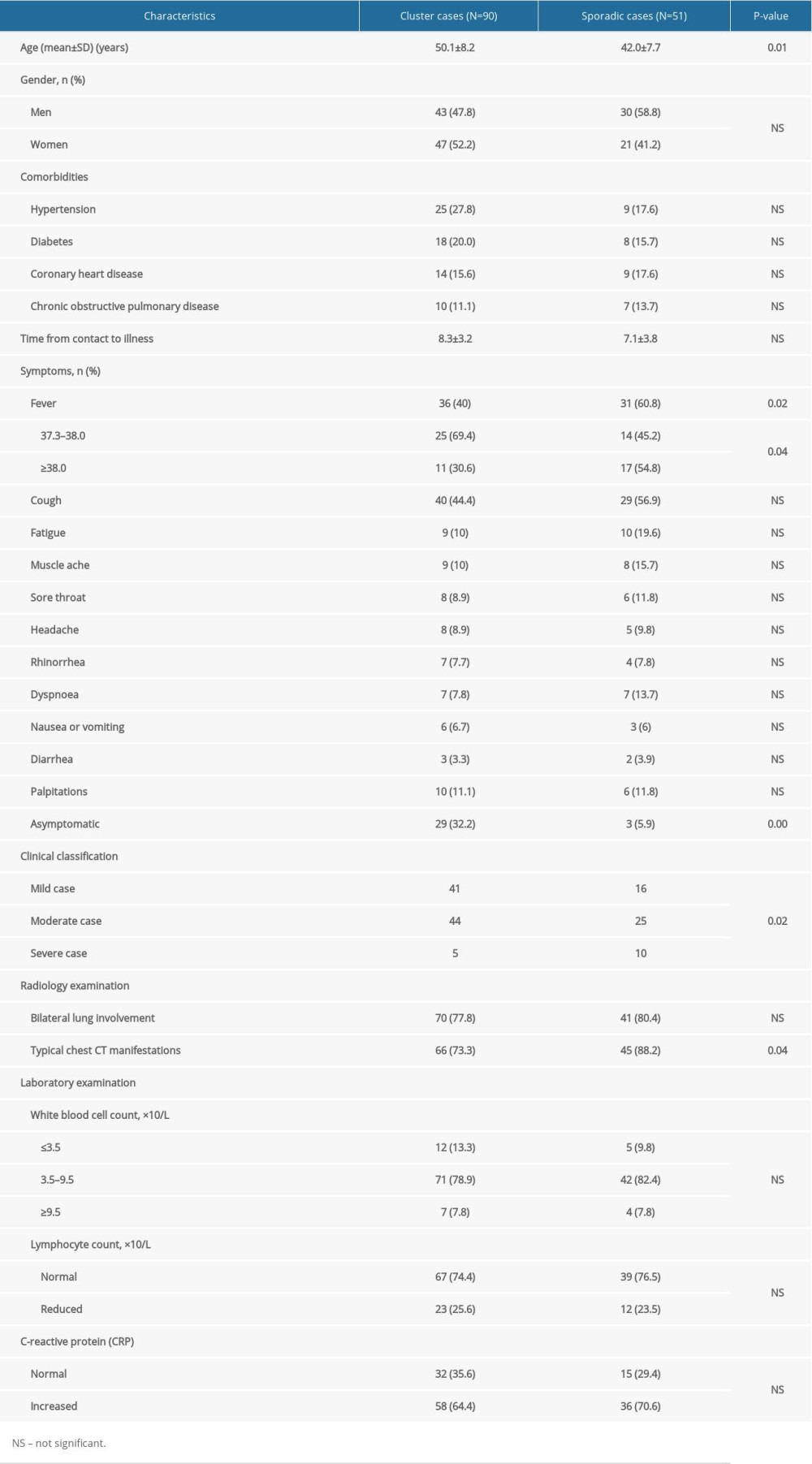
References
1. An update on the epidemiological characteristics of novel coronavirus pneumonia COVID-19: Zhonghua Liu Xing Bing Xue Za Zhi, 2020; 41; 139-44 [in Chinese]
2. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China: Zhonghua Liu Xing Bing Xue Za Zhi, 2020; 41; 145-51 [in Chinese]
3. Wang D, Hu B, Hu C, Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China: JAMA, 2020 [Epub ahead of print]
4. Lin L, Li TSInterpretation of “guidelines for the diagnosis and treatment of novel coronavirus (2019-nCoV) infection by the National Health Commission (Trial Version 5)”: Zhonghua Yi Xue Za Zhi, 2020; 100; E001 [in Chinese]
5. Kui L, Fang YY, Deng Y, Clinical characteristics of novel coronavirus cases in tertiary hospitals in Hubei Province: Chin Med J (Engl), 2020 [Epub ahead of print]
6. Zhao W, Zhong Z, Xie X, Relation between chest CT findings and clinical conditions of coronavirus disease (COVID-19) pneumonia: A multicenter study: Am J Roentgenol, 2020 [Epub ahead of print]
7. Huang C, Wang Y, Li X, Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China: Lancet, 2020; 395; 497-506
8. Li Q, Guan X, Wu P, Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia: N Engl J Med, 2020; 382(13); 1199-207
9. Jin YH, Cai L, Cheng ZS, A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version): Mil Med Res, 2020; 7(1); 4
10. She J, Jiang J, Ye L, 2019 novel coronavirus of pneumonia in Wuhan, China: Emerging attack and management strategies: Clin Transl Med, 2020; 9; 19
11. Yang J, Zheng Y, Gou X, Prevalence of comorbidities in the novel Wuhan coronavirus (COVID-19) infection: A systematic review and meta-analysis: Int J Infect Dis, 2020 [Epub ahead of print]
12. Lauer SA, Grantz KH, Bi Q, The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: Estimation and application: Ann Intern Med, 2020 [Epub ahead of print]
13. Backer JA, Klinkenberg D, Wallinga J, Incubation period of 2019 novel coronavirus (2019-nCoV) infections among travellers from Wuhan, China, 20–28 January 2020: Euro Surveill, 2020; 25(5)
14. Rodriguez-Morales AJ, Cardona-Ospina JA, Gutierrez-Ocampo E, Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis: Travel Med Infect Dis, 2020 [Epub ahead of print]
15. Chen N, Zhou M, Dong X, Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study: Lancet, 2020; 395; 507-13
16. Guan Q, Liu M, Zhuang YJEpidemiological investigation of a family clustering of COVID-19: Zhonghua Liu Xing Bing Xue Za Zhi, 2020; 41; 629-33 [in Chinese]
17. Hu Z, Song C, Xu C, Clinical characteristics of 24 asymptomatic infections with COVID-19 screened among close contacts in Nanjing, China: Sci China Life Sci, 2020 [Epub ahead of print]
18. Jiang F, Deng L, Zhang L, Review of the clinical characteristics of coronavirus disease 2019 (COVID-19): J Gen Intern Med, 2020 [Epub ahead of print]
19. Zhang Y, Su X, Chen WEpidemiological investigation on a cluster epidemic of COVID-19 in a collective workplace in Tianjin: Zhonghua Liu Xing Bing Xue Za Zhi, 2020; 41(5); 649-53 [in Chinese]
20. Chen W, Wang Q, Li YQEarly containment strategies and core measures for prevention and control of novel coronavirus pneumonia in China: Zhonghua Yu Fang Yi Xue Za Zhi, 2020; 54; 1-6 [in Chinese]
21. Gao ZCEfficient management of novel coronavirus pneumonia by efficient prevention and control in scientific manner: Zhonghua Jie He He Hu Xi Za Zhi, 2020; 43; E001
Figures
Figure 1. A cluster case of coronavirus disease 2019 (COVID-19). Transverse chest computed tomography (CT) images of a 30-year-old female patient on hospital admission. The patient had symptoms of a cough for three days. (A, B) Ground-glass opacities are shown in the posterior basal segment of the right lower lobe, indicating the presence of interstitial inflammation.Figure 2. A sporadic case of coronavirus disease 2019 (COVID-19). Transverse chest computed tomography (CT) images of a 32-year-old female patient on hospital admission. The patient had symptoms of a fever and cough for two days. (A–C) Ground-glass opacities are shown in both lower lobes with a ‘crazy-paving’ pattern of lung consolidation in the posterior basal segment of the left lower lobe. Tables
Table 1. Clinical and demographic characteristics of 141 patients with a confirmed diagnosis of coronavirus disease 2019 (COVID-19) in the main district of Chongqing, China, from January 25th to February 25th, 2020.Table 2. Radiology and laboratory findings in 141 patients with a confirmed diagnosis of coronavirus disease 2019 (COVID-19) in the main district of Chongqing, China, from January 25th to February 25th, 2020.Table 3. The clinical characteristics of cluster and sporadic cases of coronavirus disease 2019 (COVID-19) in the main district of Chongqing, China, from January 25th to February 25th, 2020.Table 1. Clinical and demographic characteristics of 141 patients with a confirmed diagnosis of coronavirus disease 2019 (COVID-19) in the main district of Chongqing, China, from January 25th to February 25th, 2020.Table 2. Radiology and laboratory findings in 141 patients with a confirmed diagnosis of coronavirus disease 2019 (COVID-19) in the main district of Chongqing, China, from January 25th to February 25th, 2020.Table 3. The clinical characteristics of cluster and sporadic cases of coronavirus disease 2019 (COVID-19) in the main district of Chongqing, China, from January 25th to February 25th, 2020. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387