08 July 2020: Clinical Research
Comparison of the Posterior and Anterolateral Surgical Approaches in the Treatment of Humeral Mid-Shaft Fractures: A Retrospective Study
Yihan Li1ABCDEF, Qingxian Tian1ABCDEFG*, Kungpeng Leng1BCDF, Meng Guo1BCDEDOI: 10.12659/MSM.924400
Med Sci Monit 2020; 26:e924400






Abstract
BACKGROUND: The aim of this study was to retrospectively assess and compare the functional outcomes and complications following anterolateral versus posterior surgical approaches for the treatment of mid-shaft fractures of the humerus.
MATERIAL AND METHODS: This study included 107 patients treated for mid-shaft fractures between May 2015 and July 2018. Demographic and surgical data were collected for each patient. During follow-up visits, radiographs were acquired and evaluated. The clinical outcomes of the involved joints were assessed by the Constant scoring system, range of motion (ROM), and the Mayo Elbow Performance Scoring system at the 12-month follow-up.
RESULTS: The posterior approach was performed in 57 patients with type A fractures (group I, n=28) and type B or C fractures (group III, n=29). The anterolateral approach was performed in 50 patients with type A fractures (group II, n=32) and type B or C fractures (group IV, n=18). There were no significant differences between group I and group II nor between group III and group IV with respect to patient demographic data, surgical data, Constant score, ROM, or Mayo Elbow Performance score. A significant difference in the total complication rate was observed between group I and II.
CONCLUSIONS: The anterolateral approach showed an advantage over the posterior approach for treating simple humeral mid-shaft fractures. However, this advantage was not observed in treating comminuted fractures.
Keywords: Diaphyses, Fracture Fixation, humeral fractures, Postoperative Complications, Bone Plates, Elbow Joint, Fracture Fixation, Internal, Fracture Healing, Fractures, Comminuted, Humerus, Range of Motion, Articular
Background
Acute humeral shaft fractures are common in trauma patients. These fractures account for approximately 1–2% of all fractures [1,2]. As described by Sarmiento et al. [3–5], middle humeral diaphyseal fractures can be treated conservatively with satisfactory union rates and excellent functional outcomes with the use of functional bracing. However, long-term immobilization also results in many complications, including elbow joint stiffness, difficulty in maintaining fracture reduction, fracture malunions, and skin problems [6–9]. Therefore, some patients might benefit from surgical treatment, including those interested in an earlier return to activities or those in which conservative treatment has failed. Humeral mid-shaft fractures can be treated surgically with a variety of techniques [10,11]. Although there is no consensus as to which surgical treatment is superior, longer times to achieve fracture union and lower rates of good to excellent functional results have been found in patients treated with intramedullary nails [12]. Therefore, many surgeons prefer open reduction and internal fixation (ORIF) for its reliability in treating shaft fractures of the humerus [13].
Several surgical approaches are conventionally used to internally fix humeral shaft fractures. Mid-shaft and distal fractures are typically treated with the posterior approach [14]. However, ORIF via the posterior approach is reportedly associated with a subsequent iatrogenic radial nerve palsy rate of 11.5%, which is regarded as the most common post-operative complication [15]. Additionally, the posterior approach requires prone or lateral positioning, which might be not suitable or might even be contraindicated in patients with multiple traumas [16]. The anterolateral approach is becoming increasingly popular because it provides adequate exposure to proximal-third and mid-shaft fractures of the humerus. Additionally, some authors have found that, compared with the posterior approach, the iatrogenic radial nerve palsy rate following ORIF via the anterolateral approach is lower [17]. However, to the best of our knowledge, few prospective or retrospective studies have compared the functional outcomes and complications, including non-union and radial or cutaneous neurological palsy, of the posterior and anterolateral surgical approaches.
The aim of the current study was to retrospectively compare and evaluate the functional outcomes and complications following the anterolateral versus posterior surgical approach for the treatment of humeral mid-shaft fractures.
Material and Methods
PATIENT DATA:
Ethics approval was obtained from the local institution’s Investigational Ethical Review Board, approval number 2019-sci-24. Between May 2015 and July 2018, 158 patients with humeral mid-shaft fractures underwent surgery at our hospital with either the posterior or anterolateral approach. The inclusion criteria for this study included: 1) mid-shaft fracture of the humerus, 2) closed fracture, and 3) patient aged 18 years or over. The exclusion criteria included: 1) pathological fractures, 2) open fractures, 3) fractures fixed 14 days or more after the initial injury, 4) concomitant fractures or ligament or tendon ruptures of the elbow or shoulder joints in conjunction with a humeral mid-shaft fracture, 5) partial or complete disability of the elbow or shoulder joint on the affected side before occurrence of the humeral mid-shaft fracture, 6) surgical treatment of the elbow or shoulder joints on the affected side before occurrence of the humeral mid-shaft fracture, 7) patient lost to follow-up before the post-operative 12 month follow-up, 8) serious nervous or vascular injury complications, and 9) apparent dementia or other psychological problems. In total, 107 patients who satisfied the inclusion/exclusion criteria were included in this study. Before deciding on whether to adopt a conservative treatment or surgical treatment, surgeons evaluated each patient’s clinical manifestations and radiological features and discussed all benefits and risks of the surgical treatment with the patient. If the patient decided to accept surgical treatment, the surgeon chose the appropriate technique based upon the type of fracture, the associated skin and soft tissue injuries, any anesthetic problems encountered, and the surgeon’s preference, after the patient provided written informed consent. Patients treated with intramedullary nails or minimally invasive percutaneous plate osteosynthesis (MIPPO) were not included in the current study.
The posterior approach was performed in 57 patients with type A fractures (group I, n=28) and type B or C fractures (group III, n=29). The anterolateral approach was performed in 50 patients with type A fractures (group II, n=32) and type B or C fractures (group IV, n=18). Patient demographic and surgical data were collected, including gender, age, affected side, mechanism of injury, fracture type according to the AO foundation and orthopedic trauma association (AO/OTA) system, interval between injury and surgery, amount of blood loss, surgical approach, and the time taken for surgical treatment (from incision to wound closure).
SURGICAL TECHNIQUES:
In groups I and III, the patient was placed in the lateral position. Surgery was performed with either a blunt dissection along the fibers in the belly of the triceps or with the triceps reflection technique, as described by Gerwin et al. [18]. In groups II and IV, the patient was in the supine position and the affected arm was abducted. The skin and deep fascia along the middle line of the lateral surface of the biceps brachii was incised, while paying attention to the preservation of the cephalic vein [17]. The brachialis muscle was dissected bluntly along its middle line; at the same time, the radial nerve and its branches were exposed with care and protected throughout the whole surgical procedure. The radial nerve could be identified 5 cm above the external condyle of the humerus at its fixed position between the brachialis and brachioradialis muscles. In the current study, identification without exploration of the radial nerve was recommended to avoid iatrogenic damage and unexpected scar formation around the nerve. The choice of plate (dynamic compression plate or locking angled plate) and placement of the plate on the surface of the mid-shaft of the humerus (anterolateral or anteromedial) was made by the surgeon during the surgery. For oblique fractures or butterfly fragments, the use of lag screws was encouraged to achieve anatomic reduction and facilitate fixation. At a minimum, implantation of 3 screws was required for distal and proximal fragments. All surgical treatments were performed by 2 experienced and certified orthopedic surgeons.
FOLLOW-UP AND STATISTICAL ANALYSIS:
All patients were followed-up in the orthopedic clinic 1, 3, 6, and 12 months following surgery, at a minimum. Further 3-monthly follow-ups were advised for patients with non-union fractures or sensory or motor deficits in the upper extremity. At each follow-up, the patient was examined, and anteroposterior (AP) and lateral (LAT) plain radiographs were evaluated. At the 12-month follow-up, functional outcomes of the shoulder and elbow joints were evaluated by the Constant scoring system and the Mayo Elbow Performance Scoring (MEPS) system, and range of motion (ROM) was determined with the elbow joint flexed and extended and with the shoulder joint abducted and elevated. A radiological doctor and 2 orthopedic surgeons assessed and recorded the time of fracture union, post-operative complications, the Constant score, and the MEPS. The data were analyzed with SPSS 22.0 software. Independent
Results
Patient demographic characteristics are shown in Table 1 and the functional results and follow-up data are shown in Table 2. There were no significant differences in gender, age, affected side of fracture, mechanism of injury, fracture type, time of fracture union, interval between injury and surgery, time taken for surgical treatment, follow-up period, surgical approach, peri-operative blood loss, ROM of both joints, MEPS, or Constant score between groups I and II nor between groups III and IV (Figures 1, 2).
Post-operative complications are shown in Table 3. There was no significant difference in iatrogenic radial nerve palsy rate (group I: 17.9%
Discussion
In the current retrospective comparative study, functional outcomes and complications following anterolateral surgical treatment of humeral mid-shaft fractures were evaluated and compared with those following posterior surgical treatment. The results of the study showed that both approaches achieved excellent outcomes; however, group I (patients with simple humeral fractures treated via the posterior approach) had a significantly higher total complication rate than group II (patients with simple humeral fractures treated via the anterolateral approach).
Conservative treatment of mid-shaft fractures of the humerus with the use of functional bracing can achieve excellent clinical outcomes; however, this treatment is associated with a variety of complications including a non-union rate ranging from 0% to 23% [3,4]. Surgeons tend to favor surgery for treating mid-shaft fractures due to the potentially quicker recovery of function [10,19]. Compared to ORIF, the intramedullary nailing technique carries higher risks of restricted shoulder movement and fixation failure [12,20,21]. One study analyzed patients with diaphyseal fractures of the humerus who underwent ORIF or MIPPO and reported no significant differences in functional outcomes or complications [22]. However, higher mal-rotation and mal-union rates in patients treated with MIPPO are reportedly associated with shoulder joint degeneration in the long term [23,24]. Although it remains controversial as to which technique is superior, ORIF is generally considered to be the more reliable osteosynthesis method [10,12,25].
In the current study, we found a significantly higher total rate of complications in group I (patients with type A fractures treated via posterior approach) compared to group II (patients with type A fractures treated via anterolateral approach). The posterior approach (using the triceps splitting or triceps reflecting approach) is recommended for middle-third humeral fractures [13]. Many authors have conducted retrospective clinical studies and have reported excellent functional outcomes of the posterior approach, with union rates of 90% to 100% [18,26,27]. The posterior approach has been commonly used over the past decade due to its intrinsic advantages, including the intra-operative protection of the radial nerve under direct visualization and the suitability of the posterior humeral surface for plate fixation [26]. However, from an anesthetic standpoint, patients with multiple traumas are in potential danger due to the lateral or prone position used in the posterior approach [28]. Alternatively, mid-shaft fractures can be treated with the anterolateral approach [13]. The advantages of this approach include the supine positioning of the patient and the availability of distal and proximal extensions to achieve excellent exposure of the humeral shaft during surgery. Several retrospective clinical studies of patients with humeral diaphyseal fractures have reported no iatrogenic radial nerve palsy and high union rates after ORIF via the anterolateral approach [29,30]. Further, evidence suggests that during anterolateral surgery, patients are safer due to the supine position and the adequate exposure of the proximal and middle humeral shaft that can be achieved via this approach.
The delayed union rates (7% in groups I and III
The treatment for iatrogenic radial nerve palsy remains controversial [36]. Some authors recommend early exploration while others advise a 4- or 6-month observation period [37,38]. As described by Seddon [39], neuropraxia is a reversible injury characterized by muscle dysfunction without atrophy, the presence of perspiration, and incomplete loss of sensation in the zone innervated by the radial nerve. Cases of axonotmesis or neurotmesis show complete sensory and motor deficits combined with a strong Tinel sign; in these cases, surgical intervention is urgently needed to recover radial nerve function [40,41]. In a retrospective study of 29 patients surgically treated for iatrogenic radial nerve palsy, revision surgery within 6 weeks resulted in better functional outcomes compared to revision surgery after 12 weeks. Further, revision surgery within 6 weeks was easier to perform due to less scar formation. Considering the findings of these studies, we advised the patients with complete sensory and motor deficits to undergo a revision surgery immediately. In our study, 85.7% of patients with radial nerve palsy completely recovered. Therefore, we favor an immediate revision for iatrogenic radial nerve palsy.
In the current study, the Constant scores and MEPS in group II (95.1 and 91.9, respectively) and group IV (94.4 and 91.1, respectively) were high, consistent with the excellent functional results reported by Chang et al. [30]. In the current study, the rate of lateral antebrachial cutaneous nerve damage was 2.0%, similar to the results reported by Idoine et al. [15]. In terms of rates of implant removal for pain relief, there was no significant difference between the anterolateral approach group (10.0%) and the posterior approach group (12.3%). Kim et al. [45] reported a similar rate of implant removal (16.1%) following surgery using the anterolateral approach to that reported in the current study. However, in current study, implant removal was difficult in the posterior approach group due to scar tissue formation around the radial nerve.
The current study had several limitations, including its retrospective nature and the relatively small sample size. In the current retrospective study, selection bias and recall bias could not be avoided, and some patients could not be included due to heterogeneous data or a lack of data integrity. Although we found a dramatic difference in the radial nerve palsy rate between group I and group II, the difference was not statistically significant, mainly due to the small sample size. A multi-center prospective randomized controlled study is recommended to confirm our results.
Conclusions
We found that the anterolateral approach was advantageous over the posterior approach for treating simple humeral mid-shaft fractures. Patients with type A humeral fractures treated via the anterolateral approach (group II) had a significantly lower complication rate compared to patients with type A humeral fractures treated via the posterior approach (group I). However, this advantage was not observed in treating comminuted fractures.
Figures
 Figure 1. X-ray films of a 48-year-old female with right mid-humeral shaft fracture caused by fall treated via the anterolateral approach (AO type A): (A) before surgery; (B) at immediate after surgery; (C) at 12 months after surgery.
Figure 1. X-ray films of a 48-year-old female with right mid-humeral shaft fracture caused by fall treated via the anterolateral approach (AO type A): (A) before surgery; (B) at immediate after surgery; (C) at 12 months after surgery. 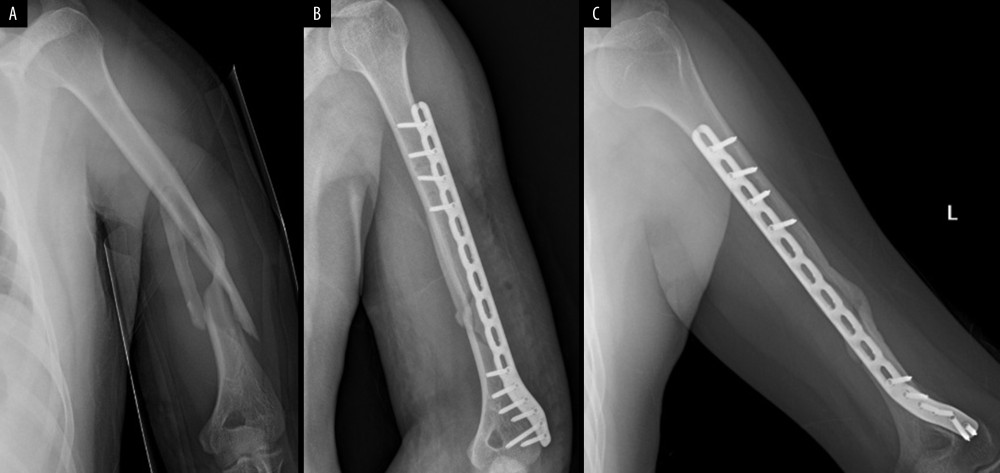 Figure 2. X-ray films of a 25-year-old male with left mid-humeral shaft fracture caused by traffic accident treated via the anterolateral approach (AO type C): (A) before surgery; (B) at immediate after surgery; (C) at 12 months after surgery.
Figure 2. X-ray films of a 25-year-old male with left mid-humeral shaft fracture caused by traffic accident treated via the anterolateral approach (AO type C): (A) before surgery; (B) at immediate after surgery; (C) at 12 months after surgery. 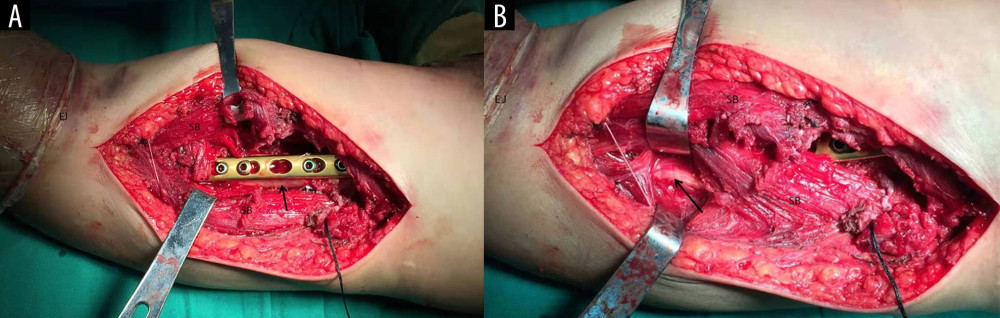 Figure 3. Anterolateral approach used in all cases of group II and IV. (A) arrow, humeral shaft; (B) arrow, radial nerve. SB – split brachialis; EJ – elbow joint.
Figure 3. Anterolateral approach used in all cases of group II and IV. (A) arrow, humeral shaft; (B) arrow, radial nerve. SB – split brachialis; EJ – elbow joint. Tables
Table 1. Demographic characteristics data, operation time and the amount of blood loss of all groups.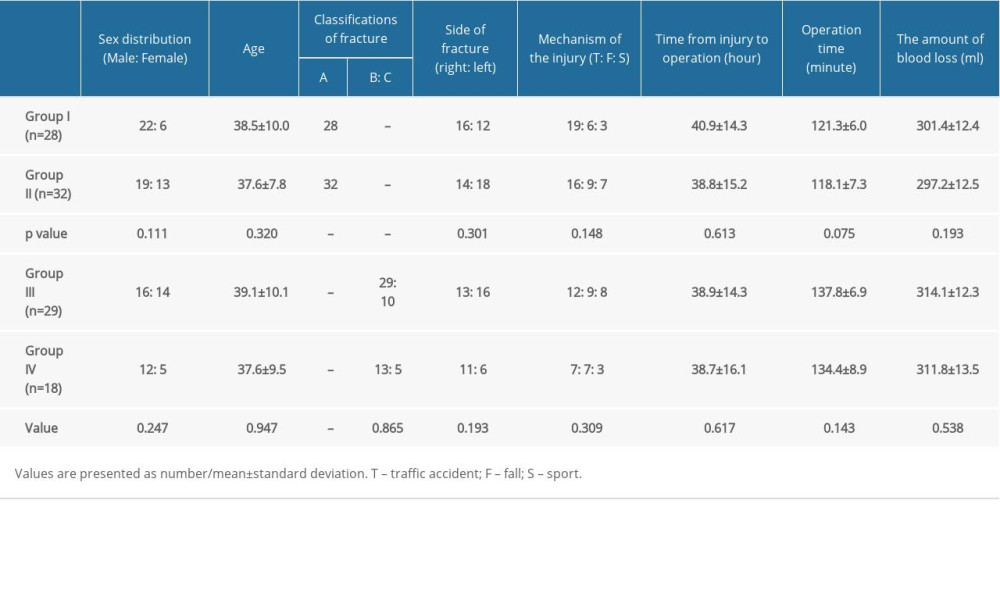 Table 2. Comparison of functional results and follow-up periods between all groups.
Table 2. Comparison of functional results and follow-up periods between all groups. Table 3. Comparison of complications between all groups.
Table 3. Comparison of complications between all groups.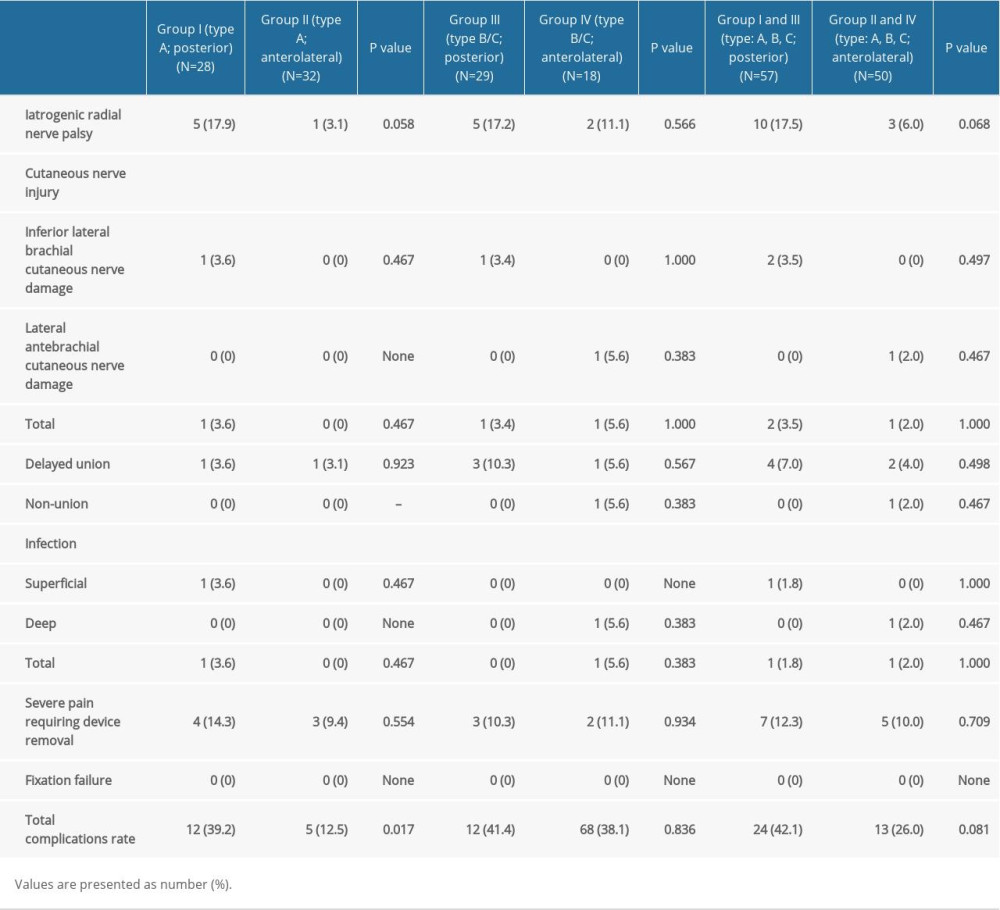 Table 4. The cause of radial nerve palsy, treatment and clinical outcomes of the patients with complete sensory and motor deficit.
Table 4. The cause of radial nerve palsy, treatment and clinical outcomes of the patients with complete sensory and motor deficit.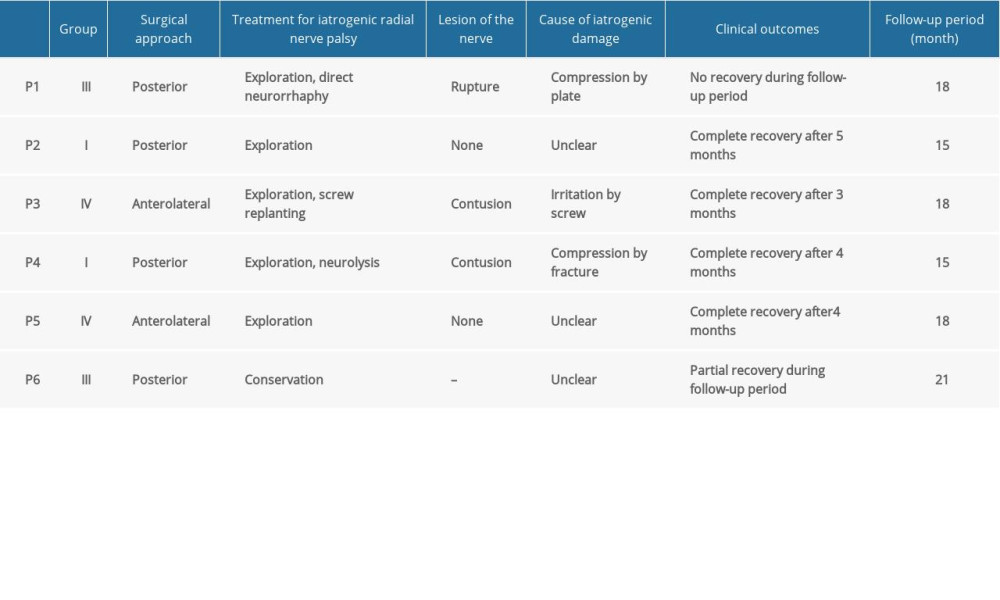
References
1. Brinker MR, O’Connor DP, The incidence of fractures and dislocations referred for orthopaedic services in a capitated population: J Bone Joint Surg Am, 2004; 86-A; 290-97
2. Court-Brown CM, Caesar B, Epidemiology of adult fractures: A review: Injury, 2006; 37; 691-97
3. Leung KS, Kwan M, Wong J, Therapeutic functional bracing in upper limb fracture-dislocations: J Orthop Trauma, 1988; 2(4); 308-13
4. Toivanen JA, Nieminen J, Laine HJ, Functional treatment of closed humeral shaft fractures: Int Orthop, 2005; 29(1); 10-13
5. Sarmiento A, Zagorski JB, Zych GA, Functional bracing for the treatment of fractures of the humeral diaphysis: J Bone Joint Surg Am, 2000; 82; 478-86
6. Aitken GK, Rorabeck CH, Distal humerai fractures in the adult: Clin Orthop Reiat Res, 1986; 207; 191-97
7. Epps CH, Grant RE, Fractures of the shaft of the humérus: Rockwood and Green’s fractures in adults, 1991; 1; 843-69, Philadelphia (PA), JB Lippincott
8. Jawa A, McCarty P, Doornberg J, Extra-articular distal-third diaphyseal fractures of the humerus: A comparison of functional bracing and plate fixation: J Bone Joint Surg, 2006; 88; 2343-47
9. Lee TJ, Kwon DG, Na SI, Cha SD, Modified combined approach for distal humerus shaft fracture: Anterolateral and lateral bimodal approach: Clin Orthop Surg, 2013; 5; 209-15
10. Niall DM, O’Mahony J, McElwain JP, Plating of humeral shaft fractures – has the pendulum swung back?: Injury, 2004; 35(6); 580-86
11. Changulani M, Jain UK, Keswani T, Comparison of the use of the humerus intramedullary nail and dynamic compression plate for the management of diaphyseal fractures of the humerus. A randomised controlled study: Int Orthop, 2007; 31(3); 391-95
12. Singisetti K, Ambedkar M, Nailing versus plating in humerus shaft fractures: A prospective comparative study: Int Orthop, 2010; 34(4); 571-76
13. Zhiquan A, Bingfang Z, Xiaojian H, Plating osteosynthesis of mid-distal humeral shaft fractures: minimally invasive versus conventional open reduction technique: International Orthopaedics (SICOT), 2010; 34; 131-35
14. Perez EA, Fractures of the shoulder, arm, and forearm: Campbell’s operative orthopaedics, 2013; III; 2854, Elsevier
15. Yin P, Zhang L, Mao Z, Comparison of lateral and posterior surgical approach in management of extra-articular distal humeral shaft fractures: Injury, 2014; 45; 1121-25
16. Idoine J, French B, Opalek J, Plating of acute humeral diaphyseal fractures through an anterior approach in multiple trauma patients: J Orthop Trauma, 2012; 26; 9-18
17. Tomas L, Hobie S, William L, Bernstein M, Surgical technique: Aterolateral approach to the humerus: J Orthop Trauma, 2018; 32; S6-S7
18. Gerwin M, Hotchkiss RN, Weiland AJ, Alternative operative exposures of the posterior aspect of the humeral diaphysis with reference to the radial nerve: J Bone Joint Surg Am, 1996; 78(11); 1690-95
19. Yang Q, Wang F, Wang Q, Surgical treatment of adult extra-articular distal humeral diaphyseal fractures using an oblique metaphyseal locking compression plate via a posterior approach: Med Prin Pract, 2011; 21; 40-45
20. Chao TC, Chou WY, Chung JC, Hsu CJ, Humeral shaft fractures treated by dynamic compression plates, Ender nails and interlocking nails: Int Orthop, 2005; 29(2); 88-91
21. Ajmal M, O’Sullivan M, McCabe J, Curtin W, Antegrade locked intramedullary nailing in humeral shaft fractures: Injury, 2001; 32(9); 692-94
22. Hu X, Xu S, Lu H: J Orthop Surg Res, 2016; 11(1); 59
23. Esmailiejah AA, Abbasian MR, Safdari F, Ashoori K, Treatment of humeral shaft fractures: Minimally invasive plate osteosynthesis versus open reduction and internal fixation: Trauma Mon, 2015; 20; e26271
24. Wang C, Li J, Li Y, Is minimally invasive plating osteosynthesis for humeral shaft fracture advantageous compared with the conventional open technique?: J Shoulder Elb Surg, 2015; 24; 1741-48
25. Meekers FS, Broos PL, Operative treatment of humeral shaft fractures. The Leuven experience: Acta Orthop Belg, 2002; 68; 462-70
26. Gausden EB, Christ AB, Warner SJ, The triceps-sparing posterior approach to plating humeral shaft fractures results in a high rate of union and low incidence of complications: Arch Orthop Trauma Surg, 2016; 136(12); 1683-89
27. Yatinder H, Yashwant ST, Vishal S, Retrospective analysis of extra-articular distal humerus shaft fractures treated with the use of pre-contoured lateral column metaphyseal LCP by triceps-sparing posterolateral approach: Strategies Trauma Limb Reconstr, 2017; 12(1); 1-9
28. McKee MD, Larsson S, Humeral shaft fractures: Rockwood and Green’s fractures in adults, 2009; 7; 1000-17, Philadelphia (PA), Lippincott Williams & Wilkins
29. Zhang L, Chen LW, Zhang WJ, Treatment of proximal and middle one-third humeral fractures with lateral distal tibial helical plate: Eur J Orthop Surg Traumatol, 2012; 22(8); 673-79
30. Chang AC, Ha NB, Sagar C, The modified anterolateral approach to the humerus: J Orthop Surg (Hong Kong), 2019; 27(3) 2309499019865954
31. Boschi V, Pogorelic Z, Gulan G, Subbrachial approach to humeral shaft fractures: New surgical technique and retrospective case series study: Can J Surg, 2013; 56(1); 27-34
32. Sebastian L, Clemens H, Valentin R, Open reduction and internal fixation of humeral midshaft fractures: Anterior versus posterior plate fixation: BMC Musculoskelet Disord, 2019; 20; 527
33. Femke C, Rinne P, Diederik V, Factors associated with radial nerve palsy after operative treatment of diaphyseal humeral shaft fractures: J Shoulder Elbow Surg, 2015; 24(11); e307-11
34. Prasarn ML, Ahn J, Paul O, Dual plating for fractures of the distal third of the humeral shaft: J Orthop Trauma, 2011; 25(1); 57-63
35. Gouse M, Albert S, Inja DB, Nithyananth M, Incidence and predictors of radial nerve palsy with the anterolateral brachialis splitting approach to the humeral shaft: Chin J Traumatol, 2016; 19(4); 217-20
36. Xun W, Ping Z, Youqing Z, Chunping Z, Secondary radial nerve palsy after internal fixation of humeral shaft fractures: Eur J Orthop Surg Traumatol, 2014; 24(3); 331-33
37. Kwasny O, Maier R, Kutscha-Lissberg F, Scharf W, Treatment procedure in humeral shaft fractures with primary or secondary radial nerve damage: Unfallchirurgie, 1992; 18(3); 168-73
38. Wang JP, Shen WJ, Chen WM, Iatrogenic radial nerve palsy after operative management of humeral shaft fractures: J Trauma, 2009; 66(3); 800-3
39. Seddon HJ, Nerve lesions complicating certain closed bone injuries: JAMA, 1947; 135; 691-94
40. Lim R, Tay SC, Yam A, Radial nerve injury during double plating of a displaced intercondylar fracture: J Hand Surg Am, 2012; 37; 669-72
41. Seddon HJ: Peripheral nerve injuries. Medical Research Council, 1954, London, Her Majesty’s Stationery Office
42. Reichert P, Wnukiewicz W, Jarosław W, Causes of secondary radial nerve palsy and results of treatment: Med Sci Monit, 2016; 22; 554-62
43. Boschi V, Pogorelic Z, Gulan G, Subbrachial approach to humeral shaft fractures: New surgical technique and retrospective case series study: Can J Surg, 2013; 56(1); 27-34
44. Frazer EA, Hobson M, McDonald SW, The distribution of the radial and musculocutaneous nerves in the brachialis muscle: Clin Anat, 2007; 20(7); 785-89
45. Kim SJ, Lee SH, Son H, Surgical result of plate osteosynthesis using a locking plate system through an anterior humeral approach for distal shaft fracture of the humerus that occurred during a throwing motion: Int Orthop, 2016; 40(7); 1489-94
Figures
Figure 1. X-ray films of a 48-year-old female with right mid-humeral shaft fracture caused by fall treated via the anterolateral approach (AO type A): (A) before surgery; (B) at immediate after surgery; (C) at 12 months after surgery.Figure 2. X-ray films of a 25-year-old male with left mid-humeral shaft fracture caused by traffic accident treated via the anterolateral approach (AO type C): (A) before surgery; (B) at immediate after surgery; (C) at 12 months after surgery.Figure 3. Anterolateral approach used in all cases of group II and IV. (A) arrow, humeral shaft; (B) arrow, radial nerve. SB – split brachialis; EJ – elbow joint. Tables
Table 1. Demographic characteristics data, operation time and the amount of blood loss of all groups.Table 2. Comparison of functional results and follow-up periods between all groups.Table 3. Comparison of complications between all groups.Table 4. The cause of radial nerve palsy, treatment and clinical outcomes of the patients with complete sensory and motor deficit.Table 1. Demographic characteristics data, operation time and the amount of blood loss of all groups.Table 2. Comparison of functional results and follow-up periods between all groups.Table 3. Comparison of complications between all groups.Table 4. The cause of radial nerve palsy, treatment and clinical outcomes of the patients with complete sensory and motor deficit. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387