20 September 2020: Lab/In Vitro Research
The Clinical Role of Preoperative Serum CA19-9 and Carcinoembryonic Antigen (CEA) Levels in Evaluating the Resectability of Advanced Gallbladder Cancer
Wencong Ma1BCF, Wei Li1DE, Jinghan Wang1DF, Rui Wu1BC, Chen Liu1D, Feiling Feng1AF*, Xiaoqing Jiang1AEFDOI: 10.12659/MSM.925017
Med Sci Monit 2020; 26:e925017






Abstract
BACKGROUND: The present study was designed to study the ability of preoperative serum concentrations of the tumor-associated biomarkers carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA19-9) and adjusted CA19-9 to assess the resectability of advanced gallbladder cancer (GBC).
MATERIAL AND METHODS: This retrospective study included patients with potentially resectable stage II–IV (AJCC 8th) GBC examined at our institution between January 2012 and December 2016. Receiver operating characteristic (ROC) curve analysis was used to determine the predictive value and optimal cut-off point of tumor-associated biomarkers for curative resection.
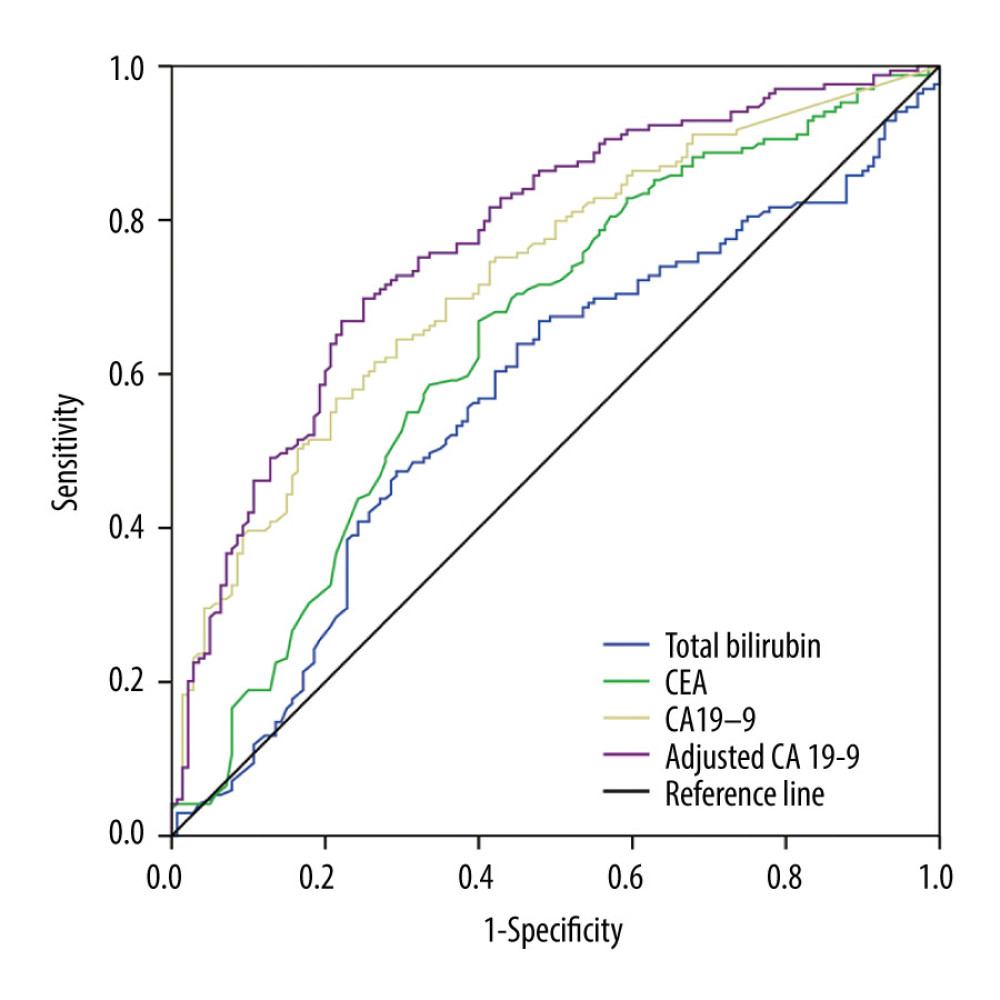
RESULTS: Pathological examination of the 309 patients included in this study found that 169 (54.7%) underwent R0 (curative) resection, whereas 121 (39.2%) underwent R1/2 (non-curative) resection, and 19 (6.1%) were unresectable. The mean serum concentrations of CEA, CA19-9 and adjusted CA19-9 were significantly lower in patients who underwent R0 resection than in the other groups. ROC curve analysis showed that adjusted CA19-9 concentration was better able to predict resectability (area under the curve, 0.774; 95% confidence interval, 0.722–0.826; P<0.001) than total bilirubin, CEA, and CA19-9 concentrations. The optimal cut-off for adjusted CA19-9 concentration was 47.63 U/mL, which had a sensitivity of 69.82%, a specificity of 75%, a positive predictive value of 77.12% and a negative predictive value of 67.31%.
CONCLUSIONS: Adjusted CA19-9 concentration is an easily calculated parameter superior to CA19-9 and CEA concentrations in predicting the resectability of advanced gallbladder cancer.
Keywords: Biological Markers, CA-19-9 Antigen, Carcinoembryonic Antigen, Antigens, Tumor-Associated, Carbohydrate, Preoperative Care
Background
Gallbladder cancer (GBC) is a relatively rare but highly lethal tumor of the biliary tract system, accounting for about 165000 cancer-related deaths per year worldwide [1,2]. The overall prognosis of patients with GBC is poor, with a 5-year mean survival rate of 5% to 10% [3]. Despite most patients being diagnosed at an advanced stage, because of the non-obvious symptoms and highly invasive nature of GBC, patients with advanced stage may benefit from aggressive radical resection, which may be the only potentially curative treatment [4,5]. Eligibility for radical resection is dependent on tumor stage and tumor biology [2,6], making preoperative assessment of the feasibility of curative resection for patients with advanced stage GBC essential. Moreover, accurate evaluation can avoid unnecessary surgery in patients ineligible for resection and reduce mortality rates.
Carcinoembryonic antigen (CEA) and carbohydrate antigen 19-9 (CA19-9) are cancer-associated antigens, measurements of which have been widely used to determine the diagnosis and prognosis of patients with tumors of the digestive system, including pancreatic [7], bile duct [8], colorectal [9], and gastric [10] cancer. Moreover, measurements of CEA and CA19-9 concentrations can be used to evaluate the resectability of various cancers [11,12], including GBCs [13]. Radical resection is possible in most patients with early stage GBC (stage 0–I, AJCC 8th), with a satisfactory prognosis [14,15]. However, the radical resection rate of advanced GBC (stages II–IV) is much lower and variable. The present study therefore evaluated the ability of serum concentrations of CEA, CA19-9 and CA19-9 relative to serum total bilirubin concentration (adjusted CA19-9) to determine the resectability of advanced (stages II–IV) GBC.
Material and Methods
STATISTICAL ANALYSIS:
Continuous data were reported as the mean±standard deviation (SD) and compared by one-way ANOVA or the Kruskal-Wallis test. Categorical data were compared by Pearson’s chi-squared test or Fisher’s exact test. The optimal cut-offs for tumor-associated biomarkers were determined by receiver operating characteristic (ROC) curve analysis and determination of the area under the ROC curve (AUC). The sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) for resectability were calculated for each cutoff value of each biomarker. Survival was analyzed by the Kaplan-Meier method and compared by log-rank tests. All statistical analyses were performed using SPSS 22.0 software, with
Results
During the study period from January 2012 to December 2016, 309 patients at our institution underwent surgery for potentially resectable of stage II–IV GBC, Of these 169 (54.7%) underwent R0 resection, as determined by postoperative pathological examination, 121 (39.2%) underwent R1/2 resection and 19 (6.1%) were unresectable. The demographic and clinical characteristics of these patients are summarized in Table 1. Patients were of mean age 60.0 years (range, 24 to 84 years), and 178 (57.6%) were women. Tumors were located in the body and fundus of the gallbladder in 169 (54.7%) patients, and in the neck and duct of the gallbladder in 140 (45.3%). Tumors in 238 (77.0%) patients were histologically classified as well and moderately differentiated, whereas tumors in 71 (23.0%) patients were poorly differentiated. Sex distribution, tumor site, and tumor differentiation did not differ significantly in the three groups of patients with R0, R1/2, and unresectable tumors. In contrast, AJCC stage correlated significantly with tumor resectability (
The mean concentrations of CA19-9, CEA, and adjusted CA19-9 were significantly lower in patients who underwent R0 resection than in those who underwent R1/2 resection and those with unresectable tumors (Table 2). These three concentrations were higher in patients with elevated (>23 μmol/L) than with lower (≤23 μmol/L) serum total bilirubin concentrations and correlated significantly with AJCC stages. Taken together these findings indicate that the serum concentrations of these three parameters correlated with the severity of GBC.
ROC curves were constructed and AUC analysis performed to evaluate the predictive value of each parameter. Adjusted CA19-9 had greater predictive value (AUC, 0.774; 95% confidence interval [CI], 0.722–0.826;
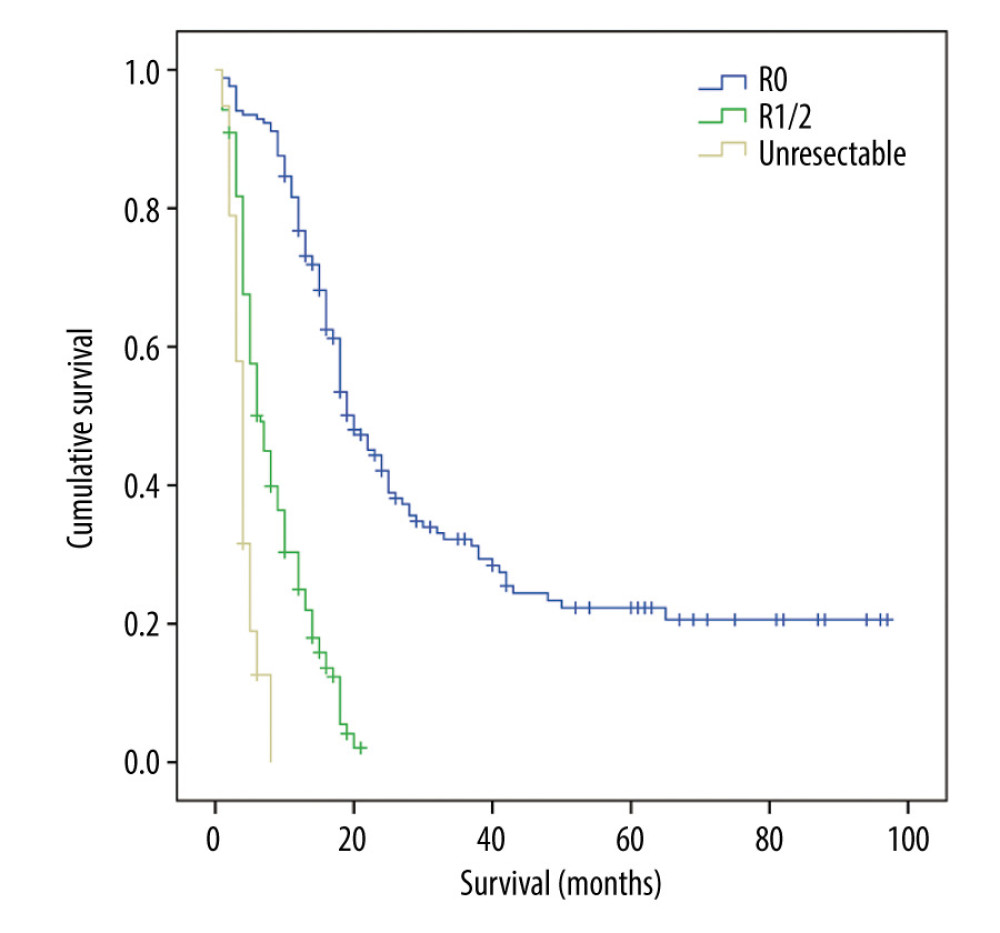
The 309 patients had a median survival time of 12 months and a 5-year survival rate of 5.83% (Figure 2). The 1-, 2-, and 5-year cumulative survival rates in patients who underwent R0 resection for GBC were 73.96%, 31.36%, and 9.47%, respectively, significantly better than for patients who underwent R1/2 resection. None of the patients with unresectable GBC survived for more than one year.
Discussion
GBC is the most common cancer of the biliary tract and the sixth most common gastrointestinal cancer [18]. Due to their atypical symptoms, frequent local invasion, early and frequent metastases, most tumors are diagnosed at advanced stage, with only about 1 in 5 GBCs diagnosed in early stages [19]. Despite improvements in surgical methods, only 25% of patients are eligible for potentially curative surgery [20]. The radical resection rate in patients with for advanced GBC, remains low and the proportion of fatal postoperative complications remains high. Moreover, unnecessary surgery for advanced GBC may delay appropriate systemic chemotherapy and increase health-care costs. An reliable and accurate preoperative assessment of GBC resectability is therefore of significant clinical importance.
Currently, the resectability of GBC is evaluated primarily by assessing clinical manifestations and performing radiological tests. Endoscopic ultrasonography (EUS) was regarded as the most sensitive diagnostic method for GB polypoid lesions, with a diagnostic sensitivity of 86% [21]. Multi-slice CT (MSCT) and MRI can provide more information about depth of tumor invasion, local extension and lymph node metastasis, but these methods frequently miss small occult hepatic and peritoneal metastases, resulting in unnecessary surgical exploration [22–24]. Although PET can be used for early detection of GBCs, as well as small (<1 cm) metastatic lymph nodes and lesions [25,26], its application is limited by the need for experienced radiologists and high costs. Staging laparoscopy has been recommended before laparotomy, as up to 37% of GBCs were determined to be unresectable by simple laparoscopy [27]. However, a study of 46 patients with potentially resectable GBC found that tumors were unresectable in 10 patients, two found by laparoscopy and eight at the time of laparotomy [28]. Simple and cost-effective measurements of tumor markers in serum may supplement radiological tests and staging laparoscopy to predict the resectability of GBCs.
CEA and CA19-9 are tumor-associated biomarkers in serum widely used to diagnose gastrointestinal cancers, including GBCs and to predict patient prognosis [29,30], indicating their importance in evaluating GBC resectability GBC. Serum CEA and CA19-9 concentrations may also predict the resectability of pancreatic cancers [31–33], whereas preoperative measurements of serum CEA, CA125, and CA19-9 concentrations can assist in evluating the resectability of cholangiocarcinomas, a type of biliary tract cancer [12]. Moreover, a study of 292 patients with stage I–IV GBC reported that preoperative CA19-9 could predict tumor resectability [13], although that study did not consider the effect of tumor-associated elevation of total bilirubin concentration on serum levels of CEA and CA19-9.. The radical resection rate of stage 0-I GBC is high, with these patients having a 5-year survival rate over 60% [15,19].
The present study assessed the ability of CEA, CA19-9 and adjusted CA19-9 concentrations to predict the resectability of advanced stage GBC. An AUC between 0.5 and 0.7 is regarded as having low diagnostic value, whereas an AUC between 0.7 and 0.9 has moderate diagnostic value. In assessing the ability of these potential biomarkers to predict the resectability of GBC, we found that the AUCs were 0.648 for CEA, 0.728 for CA19-9 and 0.774 for adjusted CA19-9, making the latter parameter more diagnostic of GBC respectability than CEA and C19-9 concentrations.
Because of the high mortality rate and limited role of palliative resection in patients with advanced GBC, resectability in the present study was defined as R0 resection. Kaplan-Meier survival analysis showed that survival rates were significantly higher in patients who underwent R0 resection than in those who underwent R1/2 resection and patients with unresectable tumors [13].
In general, it is not accurate and reasonable to assess the resectability of GBC only by measuring serum biomarkers. These markers, however, could supplement the clinical features, imaging findings, and other correlated factors, with comprehensive analysis providing better guidelines for treatment.
Conclusions
Adjusted CA19-9 concentration, which is easily calculated, is better than CA19-9 and CEA concentrations in predicting the resectability of advanced gallbladder cancer. Aberrantly high levels of adjusted CA19-9 and CA19-9 may indicate unresectable GBC. Prospective multicenter studies with larger patient cohorts are needed to assess this issue.
Tables
Table 1. Baseline characteristics of patients with gallbladder cancer.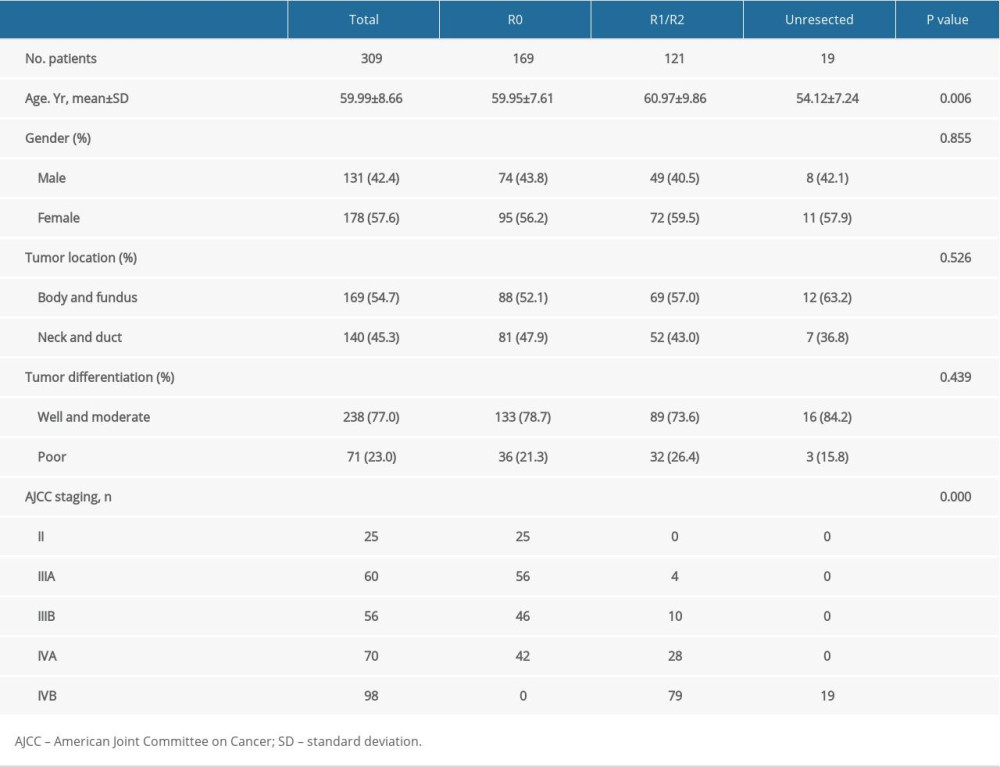 Table 2. Relationships of preoperative CEA, CA19-9, and adjusted CA19-9 concentrations with resectability, total bilirubin concentration and AJCC staging.
Table 2. Relationships of preoperative CEA, CA19-9, and adjusted CA19-9 concentrations with resectability, total bilirubin concentration and AJCC staging.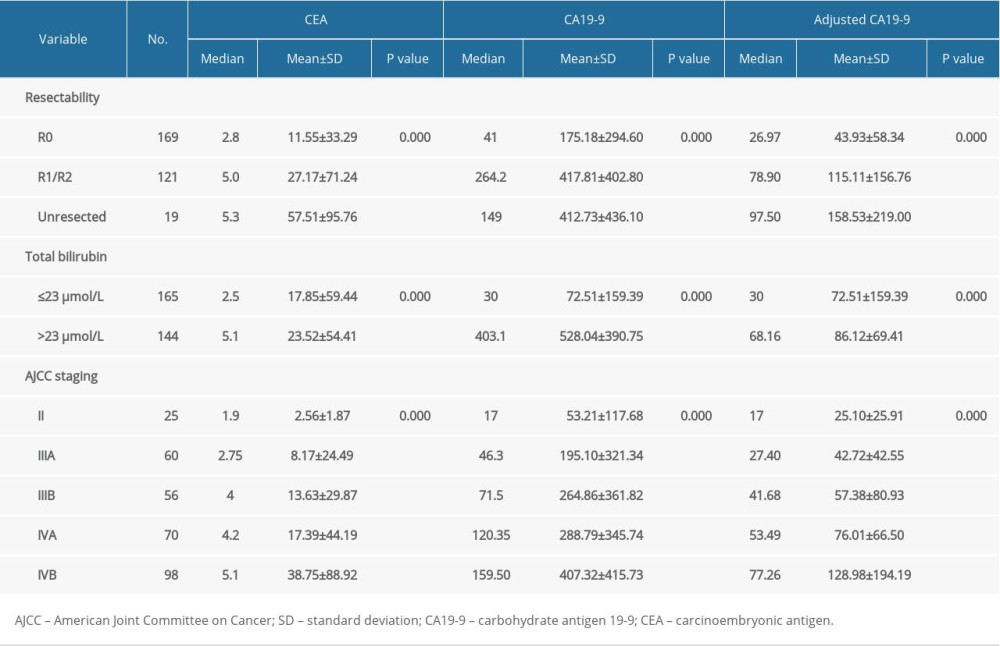 Table 3. The predictive accuracy of preoperative serum CEA, CA19-9, and adjusted CA19-9 concentrations for gallbladder cancer respectability.
Table 3. The predictive accuracy of preoperative serum CEA, CA19-9, and adjusted CA19-9 concentrations for gallbladder cancer respectability.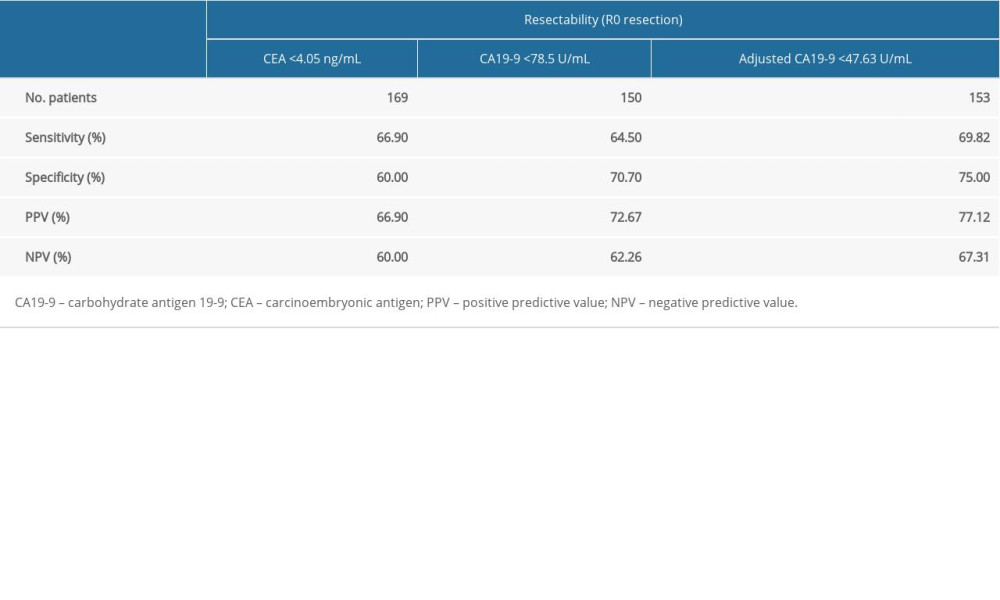
References
1. Bray F, Ferlay J, Soerjomataram I, Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries: Cancer J Clin, 2018; 68; 394-424
2. Puhalla H, Wild T, Bareck E, Long-term follow-up of surgically treated gallbladder cancer patients: Eur J Surg Oncol, 2002; 28; 857-63
3. Hueman MT, Vollmer CM, Pawlik TM, Evolving treatment strategies for gallbladder cancer: Ann Surg Oncol, 2009; 16; 2101-15
4. Kohya N, Miyazaki K, Hepatectomy of segment 4a and 5 combined with extra-hepatic bile duct resection for T2 and T3 gallbladder carcinoma: J Surg Oncol, 2008; 97; 498-502
5. Shirai Y, Wakai T, Sakata J, Hatakeyama K, Regional lymphadenectomy for gallbladder cancer: Rational extent, technical details, and patient outcomes: World J Gastroenterol, 2012; 18; 2775-83
6. Ito H, Matros E, Brooks DC, Treatment outcomes associated with surgery for gallbladder cancer: A 20-year experience: J Gastrointest Surg, 2004; 8; 183-90
7. Del Favero G, Fabris C, Plebani M, CA 19-9 and carcinoembryonic antigen in pancreatic cancer diagnosis: Cancer, 1986; 57; 1576-79
8. Grunnet M, Mau-Sorensen M, Serum tumor markers in bile duct cancer – a review: Biomarkers, 2014; 19; 437-43
9. Gao Y, Wang J, Zhou Y, Evaluation of serum CEA, CA19-9, CA72-4, CA125 and ferritin as diagnostic markers and factors of clinical parameters for colorectal cancer: Sci Rep, 2018; 8; 2732
10. Ning S, Wei W, Li J, Clinical significance and diagnostic capacity of serum TK1, CEA, CA 19-9 and CA 72-4 levels in gastric and colorectal cancer patients: J Cancer, 2018; 9; 494-501
11. Luo G, Xiao Z, Long J, CA125 is superior to CA19-9 in predicting the resectability of pancreatic cancer: J Gastrointest Surg, 2013; 17; 2092-98
12. Fang T, Wang H, Wang Y, Clinical significance of preoperative serum CEA, CA125, and CA19-9 levels in predicting the resectability of cholangiocarcinoma: Dis Markers, 2019; 2019 6016931
13. Liu F, Wang JK, Ma WJ, Clinical value of preoperative CA19-9 levels in evaluating resectability of gallbladder carcinoma: ANZ J Surg, 2019; 89; E76-80
14. Lee SE, Jang JY, Lim CS, Systematic review on the surgical treatment for T1 gallbladder cancer: World J Gastroenterol, 2011; 17; 174-80
15. Hickman L, Contreras C, Gallbladder cancer: Diagnosis, surgical management, and adjuvant therapies: Surg Clin North Am, 2019; 99; 337-55
16. Marrelli D, Caruso S, Pedrazzani C, CA19-9 serum levels in obstructive jaundice: Clinical value in benign and malignant conditions: Am J Surg, 2009; 198; 333-39
17. Mann DV, Edwards R, Ho S, Elevated tumour marker CA19-9: Clinical interpretation and influence of obstructive jaundice: Eur J Surg Oncol, 2000; 26; 474-79
18. Wistuba II, Gazdar AF, Gallbladder cancer: Lessons from a rare tumour: Nat Rev Cancer, 2004; 4; 695-706
19. Rawla P, Sunkara T, Thandra KC, Barsouk A, Epidemiology of gallbladder cancer: Clin Exp Hepatol, 2019; 5; 93-102
20. Aloia TA, Jarufe N, Javle M, Gallbladder cancer: Expert consensus statement: HPB (Oxford), 2015; 17; 681-90
21. Jang JY, Kim SW, Lee SE, Differential diagnostic and staging accuracies of high resolution ultrasonography, endoscopic ultrasonography, and multidetector computed tomography for gallbladder polypoid lesions and gallbladder cancer: Ann Surg, 2009; 250; 943-49
22. Kim SJ, Lee JM, Lee JY, Accuracy of preoperative T-staging of gallbladder carcinoma using MDCT: Am J Roentgenol, 2008; 190; 74-80
23. Oikarinen H, Diagnostic imaging of carcinomas of the gallbladder and the bile ducts: Acta Radiol, 2006; 47; 345-58
24. Kim SJ, Lee JM, Lee ES, Preoperative staging of gallbladder carcinoma using biliary MR imaging: J Magn Reson Imaging, 2015; 41; 314-21
25. Ramos-Font C, Gomez-Rio M, Rodriguez-Fernandez A, Ability of FDG-PET/CT in the detection of gallbladder cancer: J Surg Oncol, 2014; 109; 218-24
26. Chun YJ, Jeung HC, Park HS: Yonsei Med J, 2019; 60; 604-10
27. Goere D, Wagholikar GD, Pessaux P, Utility of staging laparoscopy in subsets of biliary cancers: laparoscopy is a powerful diagnostic tool in patients with intrahepatic and gallbladder carcinoma: Surg Endosc, 2006; 20; 721-25
28. Butte JM, Gonen M, Allen PJ, The role of laparoscopic staging in patients with incidental gallbladder cancer: HPB (Oxford), 2011; 13; 463-72
29. Wang YF, Feng FL, Zhao XH, Combined detection tumor markers for diagnosis and prognosis of gallbladder cancer: World J Gastroenterol, 2014; 20; 4085-92
30. Wen Z, Si A, Yang J, Elevation of CA19-9 and CEA is associated with a poor prognosis in patients with resectable gallbladder carcinoma: HPB (Oxford), 2017; 19; 951-56
31. Kim YC, Kim HJ, Park JH, Can preoperative CA19-9 and CEA levels predict the resectability of patients with pancreatic adenocarcinoma?: J Gastroenterol Hepatol, 2009; 24; 1869-75
32. Fujioka S, Misawa T, Okamoto T, Preoperative serum carcinoembryonic antigen and carbohydrate antigen 19-9 levels for the evaluation of curability and resectability in patients with pancreatic adenocarcinoma: J Hepatobiliary Pancreat Surg, 2007; 14; 539-44
33. Schlieman MG, Ho HS, Bold RJ, Utility of tumor markers in determining resectability of pancreatic cancer: Arch Surg, 2003; 138; 951-55 discussion 955–56
Figures
Tables
Table 1. Baseline characteristics of patients with gallbladder cancer.Table 2. Relationships of preoperative CEA, CA19-9, and adjusted CA19-9 concentrations with resectability, total bilirubin concentration and AJCC staging.Table 3. The predictive accuracy of preoperative serum CEA, CA19-9, and adjusted CA19-9 concentrations for gallbladder cancer respectability.Table 1. Baseline characteristics of patients with gallbladder cancer.Table 2. Relationships of preoperative CEA, CA19-9, and adjusted CA19-9 concentrations with resectability, total bilirubin concentration and AJCC staging.Table 3. The predictive accuracy of preoperative serum CEA, CA19-9, and adjusted CA19-9 concentrations for gallbladder cancer respectability. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387