04 November 2020: Clinical Research
Percutaneous Reduction and Hollow Screw Fixation Versus Open Reduction and Internal Fixation for Treating Displaced Intra-Articular Calcaneal Fractures
Ming Li1BCEF, Xiaodong Lian1BCE, Weijie Yang1DF, Kai Ding1DF, Lin Jin1BC, Zhenqin Jiao1BC, Lijie Ma1A*, Wei Chen12ADOI: 10.12659/MSM.926833
Med Sci Monit 2020; 26:e926833






Abstract
BACKGROUND: We investigated the outcomes of displaced intra-articular calcaneal fractures (DIACFs) treated by percutaneous reduction and hollow screw fixation (PRHCF) versus open reduction and internal fixation (ORIF).
MATERIAL AND METHODS: Seventy-one patients were randomly allocated to group A (by PRHCF) and group B (by ORIF). Operative time, visual analogue scale (VAS) score, time from injury to operation, postoperative hospital stay, preoperative and postoperative radiographic measurements, and complications were recorded. Functional outcomes were assessed using the American Orthopaedic Foot and Ankle Society (AOFAS) scores.
RESULTS: Finally, 59 patients were followed up for at least 12 months (range, 12–24 months). Group A showed significantly more advantages than group B in term of operative time, intraoperative blood loss, time to operation, postoperative hospital stay, and postoperative pain relief during the first 3 days (P<0.001). However, more intraoperative fluoroscopy was required in group A than in group B (P<0.001). The calcaneal width, height, length, Böhler angle, and Gissane angle in each group were significantly improved postoperatively (all P<0.001), although not significantly different in the postoperative comparisons between both groups. The AOFAS scores were slightly superior in group A than in group B (88.3 vs. 86.4, P=0.08). The rate of incidence of postoperative complications was lower in group A than in group B (3.2% vs. 10.8%, respectively; OR, 0.28, 95% CI, 0.03 to 2.84), although there was no significant difference (P=0.337).
CONCLUSIONS: PRHCF showed comparable clinical and radiological outcomes as ORIF, demonstrating it is a safe and effective alternative in treating DIACFs.
Keywords: Calcaneus, Internal Fixators, Surgical Procedures, Minimally Invasive, Bone Screws, Fracture Fixation, Internal, Fractures, Bone, intra-articular fractures, Open Fracture Reduction, Postoperative Complications, visual analog scale, young adult
Background
Calcaneal fractures comprise approximately 2% of all human fractures, and approximately 75% of these are displaced intra-articular fractures (DIACFs), which are more common in adults [1,2]. These fractures are considered to be a consequence of high-energy injuries such as from traffic accidents or a fall from height, among which 15% are open injuries and 5–10% are bilateral fractures [3]. DIACFs especially damage the subtalar joint, cause joint stiffness and other complications, and even lead to disability in severe cases.
Currently, DIACFs require surgery for mainly restoring the consistency of the subtalar joint and the width, height, and shape of the calcaneus, thereby avoiding medial and lateral impacts and restoring their normal function in patients [4]. Open reduction and internal fixation (ORIF), which is considered the criterion standard for treating DIACFs [3], can provide good exposure and allow direct reduction to better restore the anatomical position of the subtalar joint. However, the incidence of ORIF wound complications such as wound infection, dehiscence, skin necrosis, and soft-tissue damage has been reported to be as high as 30% [5]. These complications have been the main cause of poor prognosis. To reduce postoperative complications, scholars have proposed various minimally invasive treatment alternatives such as external fixation, percutaneous fixation, Schanz assisted reduction and fixation, and arthroscopically assisted operation [6–8]. These techniques effectively reduce soft-tissue damage, thereby decreasing the incidence of wound-related complications, while still allowing satisfactory fracture reduction [9–11].
To further explore the optimal treatment for DIACFs, we aimed to compare the therapeutic effects and complications between ORIF with L-shaped lateral approach and percutaneous reduction and hollow screw fixation in treating DIACFs.
Material and Methods
PREOPERATIVE MANAGEMENT:
A researcher who was not involved in the clinical treatment of patients used a random number table to divide patients into group A (percutaneous reduction and hollow screw fixation) and group B (ORIF), and collected information such as age, sex, fracture side, and Sanders classification. All patients were evaluated using lateral and axial radiographs and computed tomography (CT) scans preoperatively. According to the CT scan results, the degree of injury was graded according to Sanders classification, and the radiological parameters of the calcaneus were measured. All surgeries were performed by 2 orthopedic surgeons with >10 years of experience in managing orthopedic trauma. The radiological parameters were measured using PACS (medSynapse 5.0.1.3) by a third orthopedic surgeon who was not involved in the surgery. Each value was measured 3 times, and the average was recorded for final analysis. Postoperative pain and functional outcomes at follow-ups were evaluated by an experienced orthopedic surgeon who was blind to the patient grouping to ensure impartial and comparable evaluation.
SURGICAL PROCEDURE:
Group A patients underwent percutaneous reduction and hollow screw fixation with minimally invasive technology (Figure 1). One 3.5-mm Steinmann pin was first inserted at the calcaneal tubercle transversely from the medial to lateral sides and was used as the traction pin. The pin was then pulled along the axis of the posterior part of the calcaneus to primarily restore the height and length. Another 3.5-mm Steinmann pin was introduced from the superoposterior portion of the calcaneus into the fracture fragment along its axis to reduce the posterior facet. The pin tip was placed on the major fracture fragment and not beyond the fracture line. Subsequently, the surgeon performed repeated percutaneous leverage by using the pins inserted sagittally through the calcaneus fragment. The reduction was assessed under fluoroscopic control. If satisfactory reduction could not be achieved after repeated leverage, a 0.3-cm stab incision was made at the bottom side of the calcaneus below the lateral malleolus. The top of the vascular forceps or a 3.5-mm Kirchner wire was placed under the collapsed articular bone, which was pulled up to correct the angular malformation of the calcaneus and reduce the collapsed articular surface. Thereafter, the calcaneal width was restored by manually squeezing the surface of both sides of the calcaneal bone, and the 2.0-mm Kirchner wire was used for temporary fixation. After satisfactory reduction confirmed using the C-arm fluoroscopy intensifier, a guide pin was inserted adjacent to the lateral edge of the Achilles tendon from the superoposterior portion of the calcaneal tubercle to the distal part of the fracture. Another guide needle was inserted percutaneously from the site 0.5 cm below the insertion point of the Achilles tendon across the fracture line to the anterior part of the calcaneus. After the satisfactory position of the guide pin was confirmed radiologically, a 6.5-mm diameter hollow screw was inserted to achieve the axial support fixation of the calcaneus. If the fracture of the lateral wall of the calcaneus expanded outwards, 1 to 3 guide pins were inserted percutaneously at the bone block of the lateral side of the calcaneus below the lateral malleolus, and a 4.0-mm hollow screw was inserted to maintain the calcaneal width. Gaskets were used for incomplete bone block.
The standard extended lateral approach with an L-shaped incision was used in group B (Figure 2). A curvilinear, L-shaped incision was made at the affected foot. Once the lateral wall of the calcaneus and the subtalar joints were exposed, the full-thickness flap was held in place with three 2.0-mm Kirschner wires (1 each in the fibula, talar neck, and navicular). A Steinmann pin or traction bow was used for reducing the displaced articular surface to allow restoration of the calcaneal shape. After satisfactory reduction, a lateral plate designed for the calcaneus was generally used for rigid fixation. The rubber drains were then inserted into the incision, and the incision was closed in a layered fashion followed by compression bandaging.
POSTOPERATIVE MANAGEMENT AND FOLLOW-UP:
All patients underwent the same postoperative management protocol in both groups. Postoperatively, the patients were encouraged to move the toes and ankles frequently and elevate the affected limbs, and they were provided antithrombotic treatment. A visual analogue scale (VAS) was used to evaluate the pain degree of the patients at 24 h, 48 h, and 72 h postoperatively. Non-weight-bearing exercises involving extension and plantar flexion were performed on the first day (group A) and 2–3 days (group B) postoperatively, and the incision sutures were removed 2 weeks later. Partial weight-bearing was allowed after 4 postoperative weeks, and then gradually increased until X-ray photographs confirmed bone healing (generally 12–16 weeks postoperatively) to allow full weight-bearing. The patients were seen for follow-up at one, 3, 6, and 12 months postoperatively and then yearly thereafter. A physical examination was performed, and lateral and axial radiographs of the injured foot were taken at each follow-up evaluation. The Böhler angle, Gissane angle, and calcaneal height, width, and length were measured on the radiographs. The functional outcomes were evaluated according to the American Orthopaedic Foot and Ankle Society (AOFAS) hindfoot scores during the follow-up.
STATISTICAL ANALYSIS:
SPSS 21.0 software (SPSS, Chicago, IL, USA) was used for statistical analysis. Categorical data were statistically analyzed using the chi-square test or Fisher’s exact test (n<40 or t<1). Continuous data with a normal distribution were expressed as mean±standard deviation. Preoperative and postoperative calcaneal anatomical parameters were compared by a paired
Results
VAS SCORE:
Both groups of patients had pain after complete anesthesia failure. Twenty-seven patients in group A could tolerate pain with analgesic drug use, and the other 4 patients consciously tolerated pain without analgesic drug intervention. In contrast, all patients in group B had significant pain and received analgesic drugs, and among them 7 needed multiple pain medications. As shown in Table 3, the pain scores of patients in group A were significantly lower than those in group B on the first 3 postoperative days (P<0.001). All patients in group A had no evident pain 72 h postoperatively, while 2 patients in group B still had pain, although this had no significant difference between groups.
RADIOLOGICAL ASSESSMENT:
The calcaneal width, height, and length, Böhler angle, and Gissane angle of both groups significantly improved postoperatively (all P<0.001), although there were no significant differences in preoperative and postoperative values of these between groups (all P>0.05, Table 4).
AOFAS SCORE:
As shown in Tables 5 and 6, according to the AOFAS scoring system, good-excellent outcomes were reported in 27 cases (87.0%) in group A, and the good-excellent rate in group B was 85.8%. Although the AOFAS scores were slightly higher in group A, no significant differences were found between the groups (88.3 vs. 86.4, P=0.08).
COMPLICATIONS:
Postoperative infection occurred in 4 cases (Table 7). One case in group A had superficial infection, and the infection resolved after dressing changes. In group B, 3 patients had infections, wherein 1 (3.6%) patient had superficial infection which later healed and infection that disappeared after dressing changes, 1 (3.6%) patient had deep infection which involved the hardware and required hardware removal, and 1 (3.6%) case had wound edge necrosis that was cured after debriding twice and dressing changes. Group A showed a lower rate of overall incidence of postoperative complications than group B (3.2% vs. 10.8%, respectively; OR, 0.28, 95% CI, 0.03 to 2.84), although there was no significant difference (P=0.337).
Discussion
Our study results showed that the calcaneal width, height, and length, Böhler angle, and Gissane angle of both groups significantly improved postoperatively, and a good reduction effect was achieved. However, percutaneous reduction and internal fixation was significantly inferior than ORIF in terms of operative time and blood loss. Koski et al. [12] found that longer operative time is an important risk factor for wound complications. Levine et al. [13] found that use of small incisions could reduce postoperative swelling and scar formation around the joints, and the range of motion was also significantly improved compared with open reduction, which played a positive role in fracture prognosis. As percutaneous reduction requires reduction under X-ray monitoring, the number of intraoperative fluoroscopy images was significantly more here than in ORIF, although the reduction effect was not affected. Tornetta et al. [14] reported 46 patients with calcaneal fractures treated by percutaneous internal fixation and found that 85% of patients obtained good results. Therefore, compared with ORIF, percutaneous reduction and hollow screw fixation results in less soft-tissue damage and can restore the calcaneal anatomical shape with significant advantages.
Calcaneal fractures are often accompanied by severe tissue swelling. To reduce the complications associated with wound rupture, open surgery should be delayed sufficiently until the tissue swelling subsides, which occurs generally around 7 to 14 days after trauma [15,16]. However, percutaneous reduction and hollow screw fixation can eliminate hematoma and reduce postoperative swelling because it causes less interference with soft tissue [17], thereby eliminating the need to wait for the subsidence of swelling to allow surgery. Here, all patients who underwent percutaneous reduction and hollow screw fixation had the operation performed 2–3 days after the injury, and the operative time was relatively shorter, which reduced soft-tissue complications. None of the patients in this group had postoperative skin necrosis, and they were discharged from the hospital 3–5 days postoperatively. Compared with the open reduction group, the postoperative hospital stay was an average of 4 days.
Intra-articular calcaneal fractures caused by high-energy injuries often have serious deformities and even joint collapse. Therefore, calcaneal shape is essential for foot and ankle functions, and the best function can only be obtained after the anatomical reconstruction of the calcaneal fracture [18]. Leung et al.4[19] reported the relationship between subtalar joint reconstruction and clinical outcomes, and found that postoperative calcaneal radiological parameters are important indicators for achieving a good prognosis. Here, calcaneal traction was used to restore the length of the calcaneal bone, while percutaneous push of the bone block was effective for reduction. To avoid damaging the lateral calcaneal bone block, we opted to insert the instrument to push through the fracture line below the lateral bone block. After the joint block reduction, the lateral bone block was pressed to restore the calcaneus width, and the axial length of the calcaneus and the reduced articular surface were maintained with an internal fixator. Our reduction results showed that all cases achieved anatomical reduction, and no case was lost, which was consistent with the results of the open reduction group and confirmed the safety, reliability, and stability of the method.
Due to the dense tissue around the calcaneus, the inflammatory reaction and swelling of the tissue commonly cause severe pain, especially during the first 3 postoperative days [20]. Severe pain often greatly affects the patient’s sleep. Here, the patients who underwent the minimally invasive procedure on the day of the operation mostly felt moderate pain, which was tolerable for them. Most of them could fall asleep after taking analgesic drugs. Four cases only had mild pain, and no postoperative analgesia treatment was needed. In contrast to percutaneous internal fixation, all patients who underwent ORIF had severe postoperative pain and could not fall asleep even with analgesic drugs. Therefore, the influence of postoperative pain is also one of the key issues in the prognosis of calcaneal fracture.
The ORIF with L-shaped lateral approach has been the most commonly used operative technique for calcaneal fractures [21]. However, prolonged operative time and extensive exposure of incisions can significantly increase the incidence of infection complications [22,23]. Our study showed that the complication rate of group B was high, at 10.8%, while that of group A was only at 3.2%. The incidence of complications from the incision for percutaneous reduction and hollow screw fixation was significantly reduced, which may be related to the smaller incision and shorter operative time. A study by Zhang et al. [24] showed that the shortened operative time could reduce the incidence of wound complications. Agren et al. [25] also indicated that the reduction of soft-tissue complications was a beneficial factor for postoperative functional recovery. Percutaneous reduction and hollow screw fixation enabled patients to perform functional exercise earlier due to less trauma and pain. Chen et al. [26] demonstrated that early functional exercise and weight-bearing activity can smooth and shape the subtalar joint and reduce the residual displacement of the articular surface, thereby facilitating the functional recovery of the affected foot. Therefore, we recommend that early functional exercise should start on postoperative day 1 to improve the clinical outcomes.
A few study limitations should be noted. First, the sample size was relatively small (type II error). Therefore, further studies with larger samples are needed to obtain overall clinical data. Moreover, it was very difficult to assign all patients to only 1 surgeon in our hospital. Therefore, the differences in surgeons’ performances might have decreased the ability to extrapolate the results of this study. Finally, the validated PROMs are important parameters to evaluate functional outcomes. However, we did not include them in the initial study design. This study lays a foundation for future studies to further clarify the advantages of percutaneous reduction and hollow screw fixation in treating DIACFs.
Conclusions
Percutaneous reduction and hollow screw fixation can achieve comparable reduction and functional outcomes to ORIF in treating DIACFs. Percutaneous reduction and hollow screw fixation can minimize damage to the surrounding tissues, which can subsequently result in shorter operative time and hospital stay, and reduced intraoperative blood loss, postoperative pain, and complication rates. Therefore, percutaneous reduction and hollow screw fixation is a safe and effective treatment choice for DIACFs, and a further randomized controlled trial with a larger sample size is warranted.
Figures
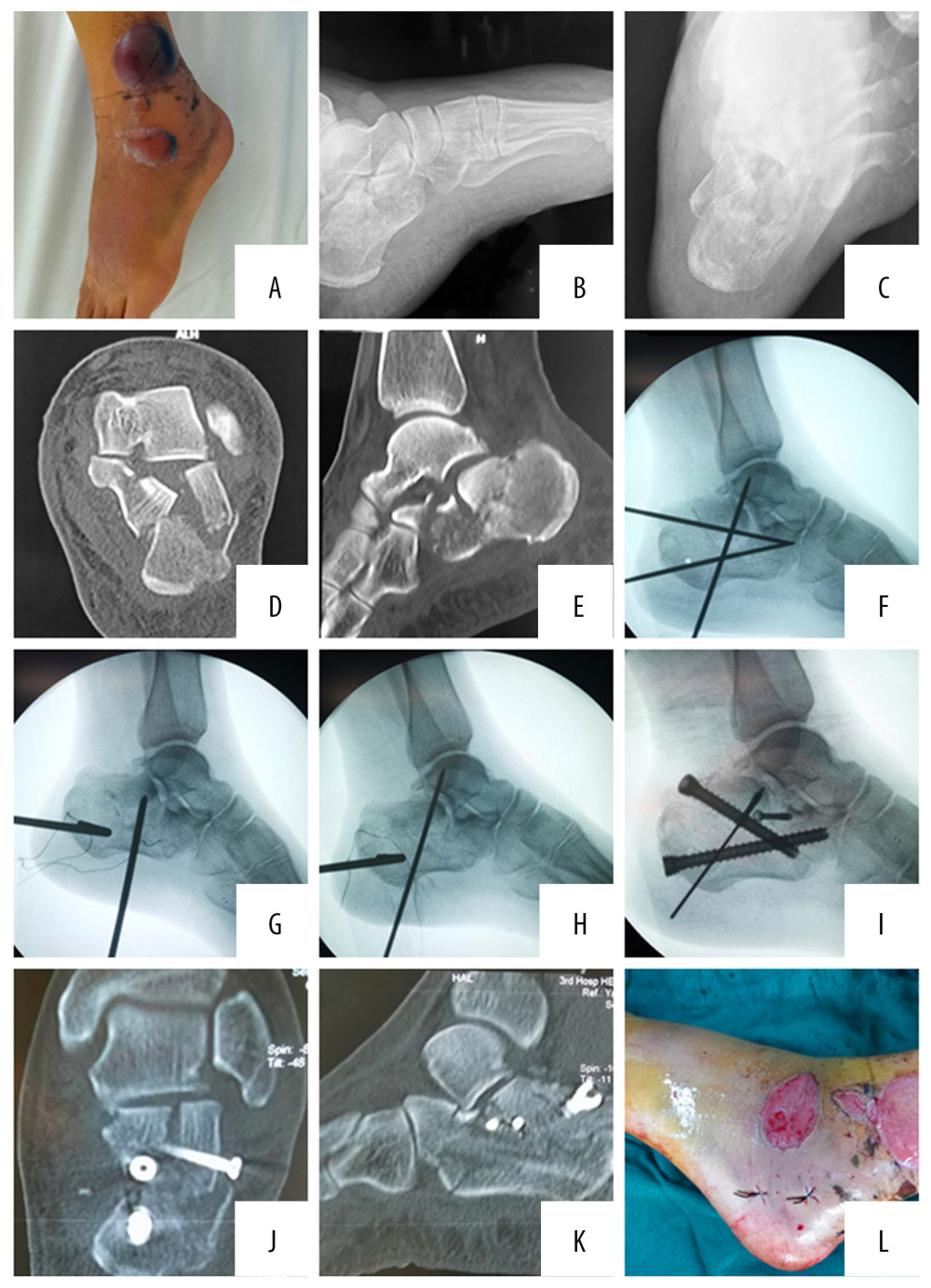 Figure 1. A 53-year-old woman had a left lateral calcaneal fracture caused by a fall from height. Preoperative skin condition of the patient (A). Preoperative X-ray: lateral view (B) and axial view (C) showed intra-articular calcaneal fractures. A preoperative CT scan (D, E) showed a Sanders Type-III. 3.5-mm Steinmann pins as the traction pins were inserted at the calcaneal (F); and the top of the 3.5 mm Kirchner wire was placed under the collapsed articular bone to reduce the collapsed articular surface (G); then the 2.0-mm Kirchner wire was used for temporary fixation (H); and the hollow screw was inserted to achieve the axial support fixation of the calcaneus (I). Postoperative CT scan (J, K) showed smooth articular surface and restoration of the width of calcaneus, and postoperative minimally invasive skin incision (L).
Figure 1. A 53-year-old woman had a left lateral calcaneal fracture caused by a fall from height. Preoperative skin condition of the patient (A). Preoperative X-ray: lateral view (B) and axial view (C) showed intra-articular calcaneal fractures. A preoperative CT scan (D, E) showed a Sanders Type-III. 3.5-mm Steinmann pins as the traction pins were inserted at the calcaneal (F); and the top of the 3.5 mm Kirchner wire was placed under the collapsed articular bone to reduce the collapsed articular surface (G); then the 2.0-mm Kirchner wire was used for temporary fixation (H); and the hollow screw was inserted to achieve the axial support fixation of the calcaneus (I). Postoperative CT scan (J, K) showed smooth articular surface and restoration of the width of calcaneus, and postoperative minimally invasive skin incision (L).  Figure 2. A 47-year-old woman had a left lateral displaced intra-articular calcaneal fracture caused by a fall from height, which was treated with the standard extended lateral approach with L-shaped incision. A curvilinear, L-shaped incision was made on the affected foot (A); a lateral plate designed for the calcaneus was used for rigid fixation (B, C).
Figure 2. A 47-year-old woman had a left lateral displaced intra-articular calcaneal fracture caused by a fall from height, which was treated with the standard extended lateral approach with L-shaped incision. A curvilinear, L-shaped incision was made on the affected foot (A); a lateral plate designed for the calcaneus was used for rigid fixation (B, C). Tables
Table 1. The general information of patients between the 2 groups preoperatively.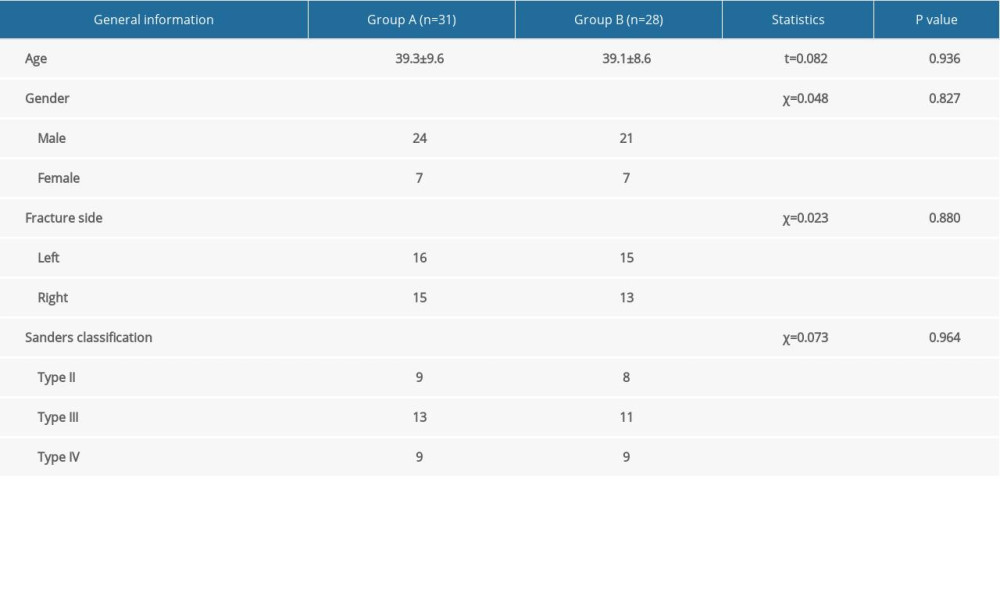 Table 2. Operative information on the patients in the 2 groups.
Table 2. Operative information on the patients in the 2 groups.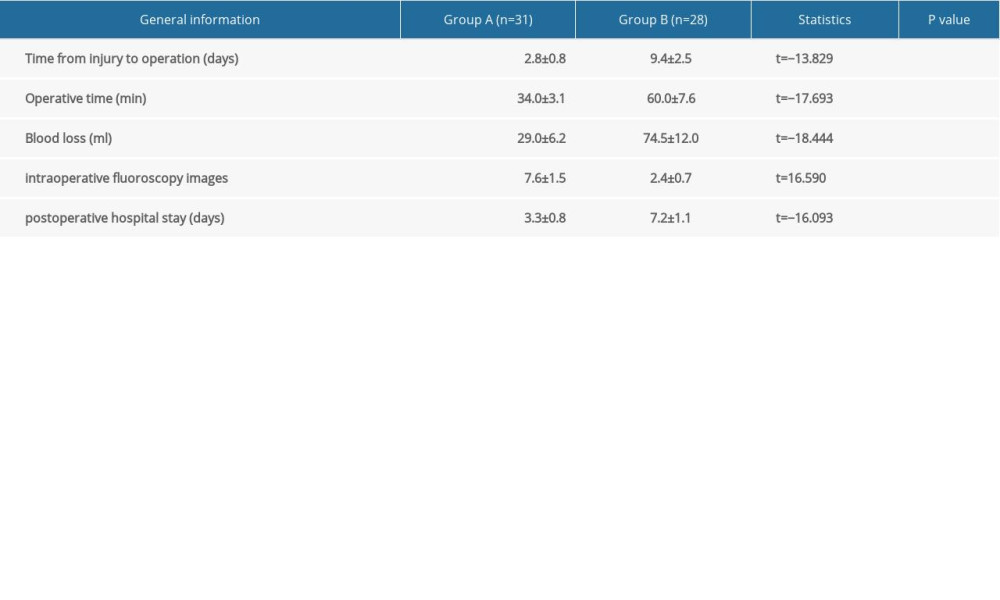 Table 3. The comparison of VAS scores postoperatively.
Table 3. The comparison of VAS scores postoperatively.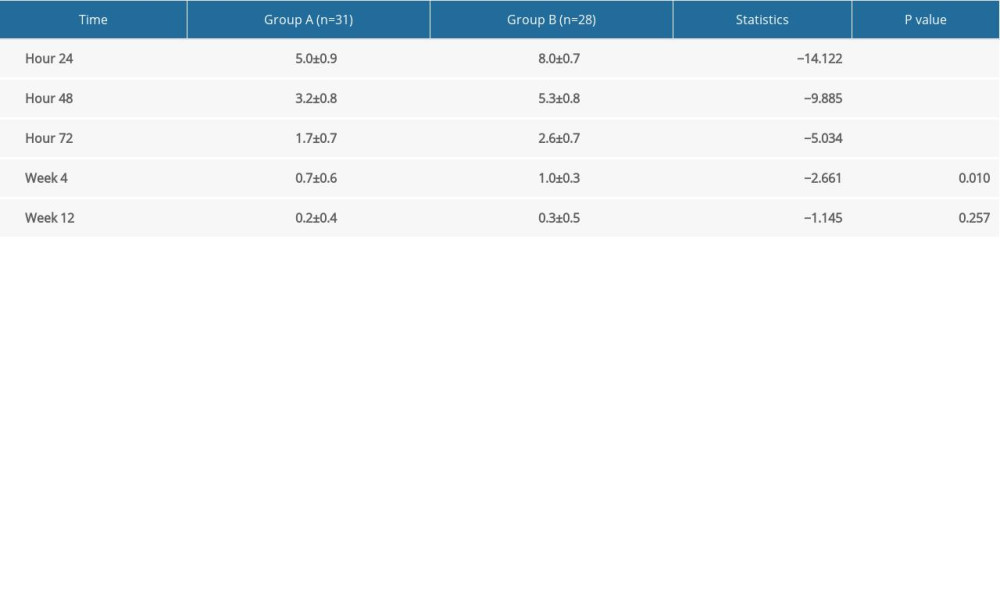 Table 4. Radiological assessment for the 2 groups.
Table 4. Radiological assessment for the 2 groups.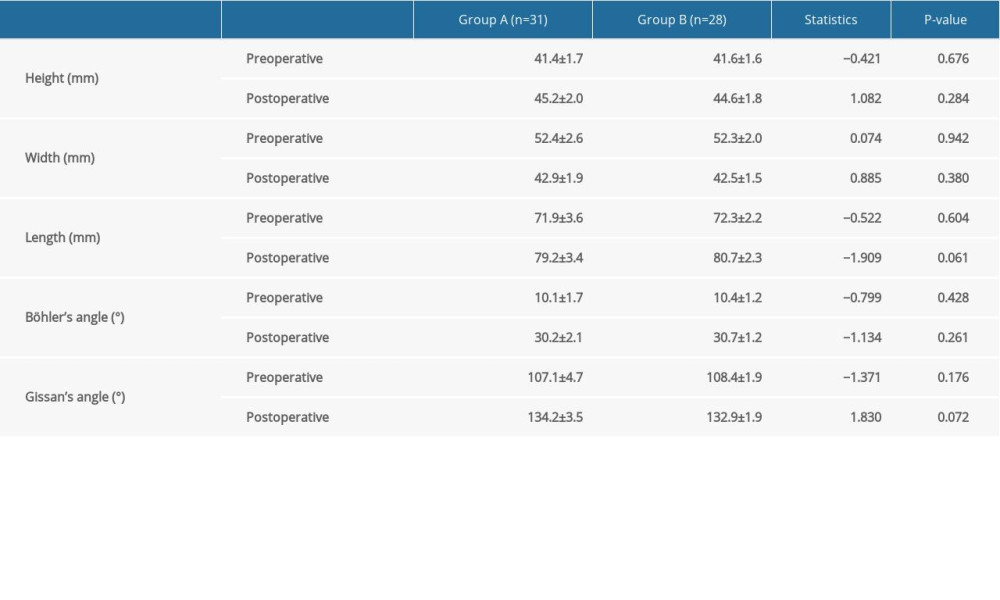 Table 5. AOFAS score versus Sanders classification in group A.
Table 5. AOFAS score versus Sanders classification in group A.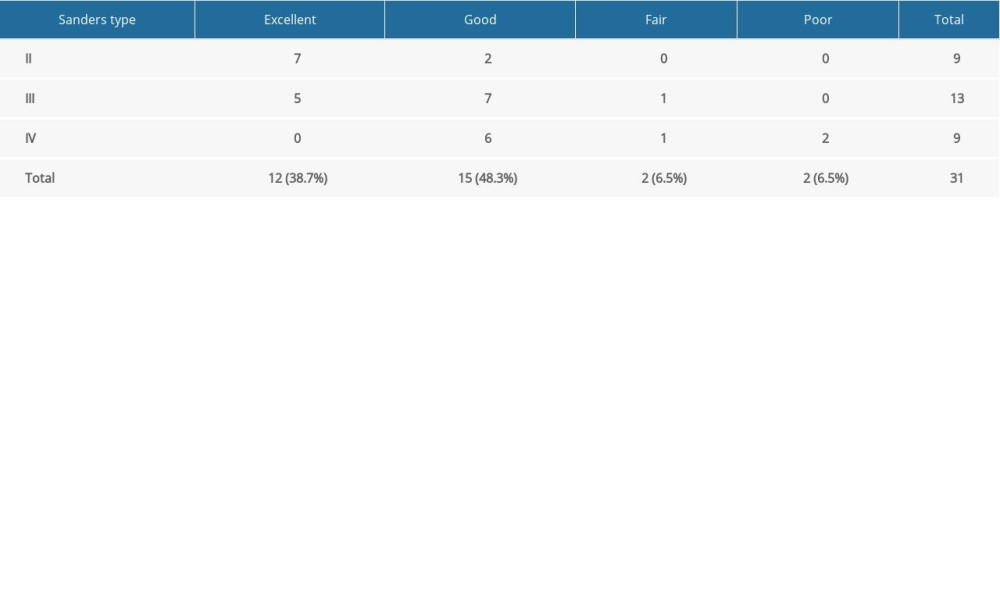 Table 6. AOFAS score versus Sanders classification in group B.
Table 6. AOFAS score versus Sanders classification in group B.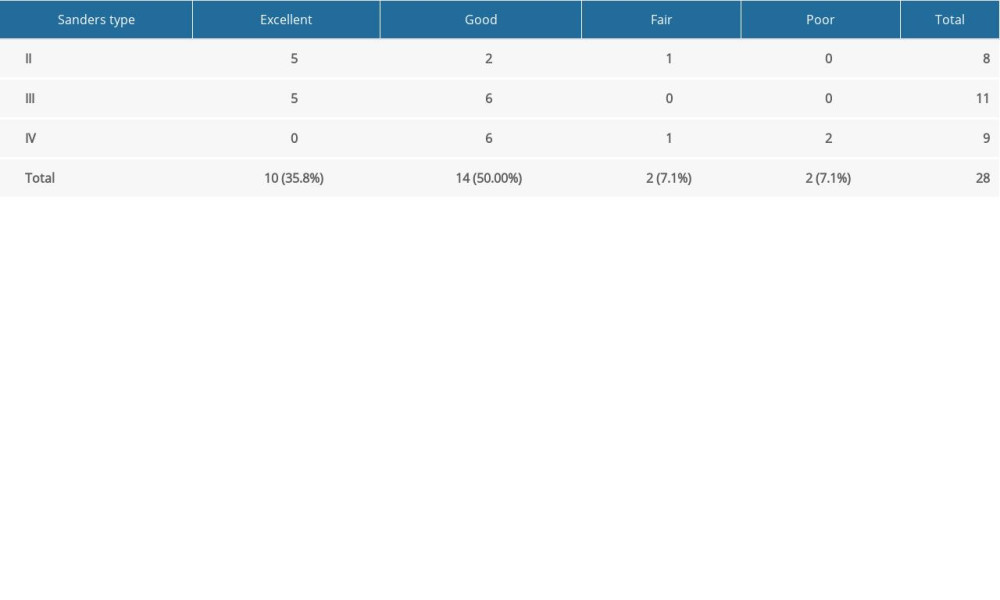 Table 7. Soft tissue complications.
Table 7. Soft tissue complications.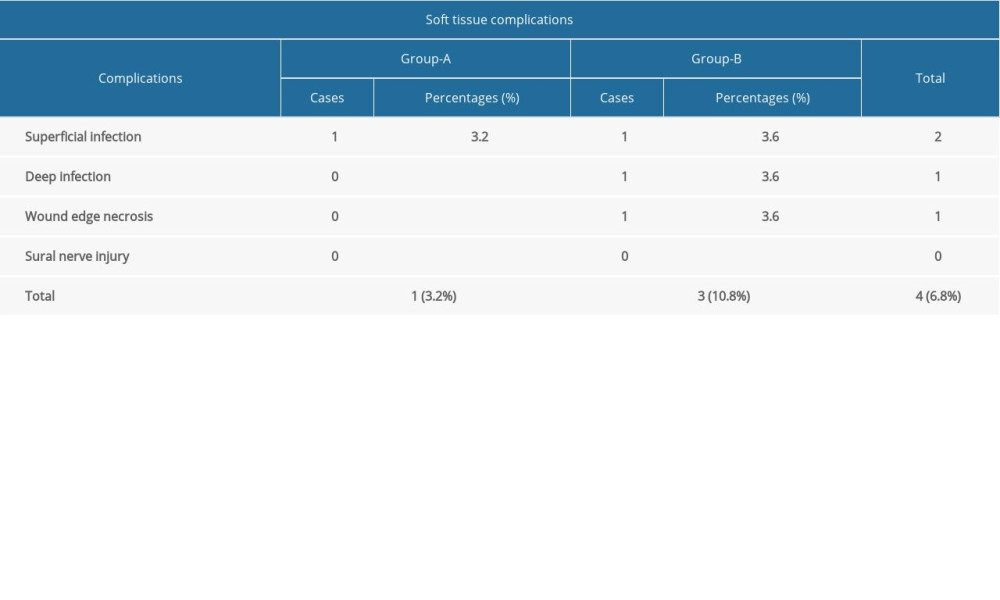
References
1. Molloy AP, Lipscombe JS, Hindfoot arthrodesis for management of bone loss following calcaneus fractures and nonunions: Foot Ankle Clin, 2011; 16(1); 165-79
2. Ibrahim T, Rowsell M, Rennie W, Displaced intra-articular calcaneal fractures: 15-year follow-up of a randomised controlled trial of conservative versus operative treatment: Injury, 2007; 38(7); 848-55
3. Sanders R, Displaced intra-articular fractures of the calcaneus: J Bone Joint Surg Am, 2000; 82(2); 225-50
4. Schepers T, The sinus tarsi approach in displaced intra-articular calcaneal fractures: A systematic review: Int Orthop, 2011; 35(5); 697-703
5. Benirschke SK, Kramer PA, Wound healing complications in closed and open calcaneal fractures: J Orthop Trauma, 2004; 18(1); 1-6
6. Hospodar P, Guzman C, Johnson P, Uhl R, Treatment of displaced calcaneus fractures using a minimally invasive sinus tarsi approach: Orthopedics, 2008; 31(11); 1112
7. Ramos RR, de Castro Filho CD, Ramos RR, Surgical treatment of intra-articular calcaneal fractures: description of a technique using an adjustable uniplanar external fixator: Strategies Trauma Limb Reconstr, 2014; 9(3); 163-66
8. Sampath KV, Marimuthu K, Subramani S, Prospective randomized trial comparing open reduction and internal fixation with minimally invasive reduction and percutaneous fixation in managing displaced intra-articular calcaneal fractures: Int Orthop, 2014; 38(12); 2505-12
9. Kikuchi C, Charlton TP, Thordarson DB, Limited sinus tarsi approach for intra-articular calcaneus fractures: Foot Ankle Int, 2013; 34(12); 1689-94
10. Tornetta P, The Essex-Lopresti reduction for calcaneal fractures revisited: J Orthop Trauma, 1998; 12(7); 469-73
11. Schuberth JM, Cobb MD, Talario RH, Minimally invasive arthroscopic-assisted reduction with percutaneous fixation in the management of intra-articular calcaneal fractures: A review of 24 cases: J Foot Ankle Surg, 2009; 48(3); 315-22
12. Koski A, Kuokkanen H, Tukiainen E, Postoperative wound complications after internal fixation of closed calcaneal fractures: A retrospective analysis of 126 consecutive patients with 148 fractures: Scand J Surg, 2005; 94(3); 243-45
13. Levine DS, Helfet DL, An introduction to the minimally invasive osteosynthesis of intra-articular calcaneal fractures: Injury, 2001; 32; SA51-54
14. Tornetta P, The Essex-Lopresti reduction for calcaneal fractures revisited: J Orthop Trauma, 1998; 12(7); 469-73
15. Dhillon MS, Bali K, Prabhakar S, Controversies in calcaneus fracture management: A systematic review of the literature: Musculoskelet Surg, 2011; 95(3); 171-81
16. Zeman P, Zeman J, Matejka J, Koudela K, Long-term results of calcaneal fracture treatment by open reduction and internal fixation using a calcaneal locking compression plate from an extended lateral approach: Acta Chir Orthop Traumatol Cech, 2008; 75(6); 457-64
17. Mulcahy DM, McCormack DM, Stephens MM, Intra-articular calcaneal fractures: Effect of open reduction and internal fixation on the contact characteristics of the subtalar joint: Foot Ankle Int, 1998; 19(12); 842-48
18. Makki D, Alnajjar HM, Walkay S, Osteosynthesis of displaced intra-articular fractures of the calcaneum: A long-term review of 47 cases: J Bone Joint Surg Br, 2010; 92(5); 693-700
19. Leung KS, Yuen KM, Chan WS, Operative treatment of displaced intra-articular fractures of the calcaneum. Medium-term results: J Bone Joint Surg Br, 1993; 75(2); 196-201
20. Chou LB, Wagner D, Witten DM, Postoperative pain following foot and ankle surgery: A prospective study: Foot Ankle Int, 2008; 29(11); 1063-68
21. Eastwood DM, Irgau I, Atkins RM, The distal course of the sural nerve and its significance for incisions around the lateral hindfoot: Foot Ankle, 1992; 13(4); 199-202
22. Jiang N, Lin Q, Diao X, Surgical versus nonsurgical treatment of displaced intra-articular calcaneal fracture: A meta-analysis of current evidence base: Int Orthop, 2012; 36(8); 1615-22
23. Benirschke SK, Sangeorzan BJ, Extensive intraarticular fractures of the foot. Surgical management of calcaneal fractures: Clin Orthop Relat Res, 1993; 292; 128-34
24. Zhang T, Su Y, Chen W, Displaced intra-articular calcaneal fractures treated in a minimally invasive fashion: Longitudinal approach versus sinus tarsi approach: J Bone Joint Surg Am, 2014; 96(4); 302-9
25. Agren PH, Wretenberg P, Sayed-Noor AS, Operative versus nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial: J Bone Joint Surg Am, 2013; 95(15); 1351-57
26. Chen W, Liu B, Lv H, Radiological study of the secondary reduction effect of early functional exercise on displaced intra-articular calcaneal fractures after internal compression fixation: Int Orthop, 2017; 41(9); 1953-61
Figures
Figure 1. A 53-year-old woman had a left lateral calcaneal fracture caused by a fall from height. Preoperative skin condition of the patient (A). Preoperative X-ray: lateral view (B) and axial view (C) showed intra-articular calcaneal fractures. A preoperative CT scan (D, E) showed a Sanders Type-III. 3.5-mm Steinmann pins as the traction pins were inserted at the calcaneal (F); and the top of the 3.5 mm Kirchner wire was placed under the collapsed articular bone to reduce the collapsed articular surface (G); then the 2.0-mm Kirchner wire was used for temporary fixation (H); and the hollow screw was inserted to achieve the axial support fixation of the calcaneus (I). Postoperative CT scan (J, K) showed smooth articular surface and restoration of the width of calcaneus, and postoperative minimally invasive skin incision (L).Figure 2. A 47-year-old woman had a left lateral displaced intra-articular calcaneal fracture caused by a fall from height, which was treated with the standard extended lateral approach with L-shaped incision. A curvilinear, L-shaped incision was made on the affected foot (A); a lateral plate designed for the calcaneus was used for rigid fixation (B, C). Tables
Table 1. The general information of patients between the 2 groups preoperatively.Table 2. Operative information on the patients in the 2 groups.Table 3. The comparison of VAS scores postoperatively.Table 4. Radiological assessment for the 2 groups.Table 5. AOFAS score versus Sanders classification in group A.Table 6. AOFAS score versus Sanders classification in group B.Table 7. Soft tissue complications.Table 1. The general information of patients between the 2 groups preoperatively.Table 2. Operative information on the patients in the 2 groups.Table 3. The comparison of VAS scores postoperatively.Table 4. Radiological assessment for the 2 groups.Table 5. AOFAS score versus Sanders classification in group A.Table 6. AOFAS score versus Sanders classification in group B.Table 7. Soft tissue complications. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387