30 January 2021: Clinical Research
Quantification of the Masseter Muscle Hardness of Stroke Patients Using the MyotonPRO Apparatus: Intra- and Inter-Rater Reliability and Its Correlation with Masticatory Performance
Chao Song1ACFG, Yi-Fu Yu1BCDE, Wen-Long Ding1BCD, Jian-Yong Yu2BDF, Li Song1BCF, Ya-Nan Feng3CEF, Zhi-Jie Zhang3AFG*DOI: 10.12659/MSM.928109
Med Sci Monit 2021; 27:e928109






Abstract
BACKGROUND: Chewing dysfunction is one of the most common serious complications after a stroke. It may be influenced by the hardness of the masseter muscle and masticatory performance; however, the association between these 2 factors is not explicit. Thus, it is meaningful to explore the functional status of the masseter muscle among stroke patients. The main objectives of this study were to examine the intra- and inter-rater reliability of the MyotonPRO apparatus in measuring masseter muscle hardness in stroke patients and to investigate the correlation between the bilateral masseter muscle hardness and masticatory performance in these patients.
MATERIAL AND METHODS: A total of 20 stroke patients participated in our study. The hardness of the masseter muscle was measured by 2 physiotherapists using the MyotonPRO apparatus. Overall, each patient masticated 2 pieces of red-blue bicolor chewing gum for 20 chewing cycles each. The chewing pieces were analyzed using ViewGum software for masticatory performance.
RESULTS: The intra- and inter-rater reliability of the MyotonPRO apparatus for measuring bilateral masseter hardness of stroke patients was excellent. The correlation analysis showed that the hardness index of the masseter muscle on the affected side was moderately correlated with the masticatory performance of the same side.
CONCLUSIONS: The MyotonPRO device can be used for measuring the masseter muscle hardness of stroke patients, with excellent reliability. This study established the construct validity between the stiffness of the masseter muscle and masticatory performance.
Keywords: Hardness, Masseter Muscle, Reproducibility of Results, Stroke, Chewing Gum, Electromyography, Mastication
Background
Stroke is a serious disease that threatens health and life, and it is accompanied by high rates of disability, mortality, and recurrence. The dysfunction in the aftermath of a stroke can be intricate and comprehensive [1]. The most common dysfunctions after a stroke include a variety of functional disabilities caused by the acute local cerebral circulation disorders, limb paralysis, difficulty eating and swallowing, speech disorders, and cognitive disorders. Eating difficulties represent a key problem affecting the quality of life of stroke patients. Several studies have indicated that these difficulties may be caused by a decline in occlusal strength and disuse atrophy of paralyzed muscles in stroke patients. The incidence of eating difficulties has been found to be as high as 80% in hospitalized stroke patients [2,3]. Further, 66% of hospitalized stroke patients had difficulties eating after 6 months of hospitalization [4]. As a key muscle for biting and chewing, the masseter muscle has a critical role in the process of eating. Hence, it is essential to measure the mechanical properties of the masseter muscle and to further investigate its functional status in stroke patients.
Occlusal equilibrium disorders in stroke patients are increased when complicated by disuse atrophy of the muscles around the temporal-mandibular joint. The consequences may not only include occlusal overloading of the teeth on the healthy side but also may also result in decreased masticatory performance and ability to eat [5]. Several studies have indicated that bite force and masticatory performance are related to the biomechanical properties of the masseter muscle. Ahlgren [6] examined the myoelectricity waveform and value of the masticatory muscle to diagnosis the auxiliary bite force, and the results showed that the electrical activity of the masticatory muscle was related to bite force. Cakir et al. [7] also reported the electrical activity of the masticatory muscle during chewing, finding significant correlations between the hardness of the muscle and its activity. In addition, Ariji et al. [8] assessed masseter muscle hardness using shear-wave sonoelastography in healthy volunteers and defined normal values. They also found significant differences between the values at rest and during jaw clenching. Biomechanical assessment of soft tissue is critical in basic and clinical research, including studies on musculoskeletal disorders, neuromuscular diseases, and rehabilitation exercise [9,10]. At present, few studies have been conducted on the hardness of masseter muscle and masticatory performance and the relationship between them in stroke patients. Therefore, investigating the biomechanical properties of the masseter muscle in stroke patients is essential for supporting clinical therapy after strokes.
Muscle rigidity is a basic physiological characteristic that ensures the proper functioning of the human motor system. Previously, muscle hardness was commonly evaluated by palpation during clinical examination, but the method relied on subjective evaluation that cannot quantify the hardness of the muscle and may yield incorrect assessments. At present, shear-wave sonoelastography and the MyotonPRO apparatus have been applied to examine the hardness of soft tissue, and these methods have been confirmed to have excellent credibility. The MyotonPRO apparatus is more efficient and easier to use, however, and our previous report has also verified that the MyotonPRO apparatus is a useful tool to assess the hardness of the gastrocnemius muscle [11], plantar fascia [12], and patellar tendon [13]. Thus, we used the MyotonPRO as a convenient handheld apparatus to evaluate the masseter muscle stiffness of stroke patients objectively and quantitatively in this study.
The objectives of our research were to: (1) examine the intra- and inter-rater reliability of using the MyotonPRO apparatus to assess the hardness of the masseter muscle in stroke patients, and (2) explore the correlation between the hardness of the masseter muscle and masticatory performance in stroke patients.
Material and Methods
ETHICS STATEMENT:
The research received institutional approval by the Human Subjects Ethics committee of Luoyang Orthopaedic Hospital of Henan Province (No. 2019-001-01). The research protocol strictly followed the Declaration of Helsinki. Prior to the experiment, written consent was obtained from each participant.
INCLUSION AND EXCLUSION CRITERIA:
Twenty patients (male to female ratio 1: 1) with stroke were recruited from the Department of Neurorehabilitation in our hospital for this study. All participants had experienced an ischemic stroke, which was diagnosed as cerebral infarction by magnetic resonance imaging and other medical imaging methods. The mean parameters for age, height, weight, and body mass index of the stroke patients were 47.65±9.16 years, 168.95±0.07 cm, 69.15±15.08 kg, and 24.16±2.86 kg/m2, respectively. All patients were in stable condition and able to take care of themselves. The activities of daily living (ADL) score was over 60, and the limb function level of the affected side was more than Brunnstrom IV. Exclusion criteria were ages <18 or >60 years, systemic disease, cognitive disorder, elapsed time of over 12 months since the stroke, periodontal treatment, absence of teeth, use of dentures or prosthesis, symptoms of acute oral infections, pregnancy or breastfeeding, and smoking and alcohol consumption. Patients were also excluded if they were taking nonsteroidal anti-inflammatory drugs, prescription steroids, or antibiotics, and if they had immunosuppressive or psychiatric drug use within the previous 6 months prior or were currently using pharmaceutical preparations that affected muscle tone.
MEASUREMENT OF THE MASSETER MUSCLE STIFFNESS:
The hardness of the masseter muscle was measured using the handheld MyotonPRO apparatus. Prior to the evaluation, each patient was in a seated position with the head held in a relaxed, neutral position for 5 min. The measurement point was marked with pen 3 cm above the angle of the mandible in the masseter muscle where it bulges when it is contracted (Figure 1). The hardness of the masseter muscle was measured as the subjects bit tightly to the intercuspal position for 5 s. For the inter-rater reliability, each measurement point was assessed 3 times by assessors YYF and DWL (both physical therapists) and the average value was calculated. For the intra-rater reliability, each patient was retested by the assessor YYF after 5 days to standardize the study procedures and to minimize the effect of time on muscle stiffness. The whole experiment was carried out in a quiet room kept at 23°C.
MEASUREMENT OF MASTICATORY PERFORMANCE:
Each participant masticated 2 pieces of red-blue bicolor chewing gum, one on the affected side and the other on the unaffected side, for 20 chewing cycles, respectively. Each piece of gum was formed into a mixture bolus through chewing and spat into a vacuum bag. The front and back of each bolus were flattened and scanned, with consistent conditions for light, a white background, and camera parameters. Each pair of images was then imported into Photoshop software and assembled into 1 composite image. All digital photographs were analyzed 3 times using ViewGum software, and the “Ch0 st.dev” value shown in the right box of the software interface was recorded (Figure 2). The values ranged from 0 to 1 and represented the standard deviation of hue after color values of each pixel were normalized in the gum image. Smaller values indicated greater masticatory performance.
STATISTICAL ANALYSES:
SPSS 19.0 software was used for data analysis in this study. All variables were found to be normally distributed by the Kolmogorov-Smirnov test. The mean difference of stiffness value of masseter muscle was calculated using a paired
The sample significance level was 0.05, and all numerical values are shown as mean±SD [14,15]. To test the correlations between the intra- and inter-rater reliability and masticatory performance, multivariable stepwise regression method was used with masticatory performance as an attributive variable. Prior to this, the association between explanatory variables was tested. The parametric variables were compared by Pearson’s correlation coefficient, and the nonparametric variables were compared by Spearman’s rank correlation coefficient.
Results
INTRA- AND INTER-RATER RELIABILITY:
The bilateral masseter muscle hardness values are shown in Table 1. Both intra- and inter-rater reliability for assessing the bilateral masseter stiffness of stroke patients were excellent at a 95% confidence interval, with an ICC value >0.90, SEM <27 N/m, and MDC <74 N/m. For intra-rater reliability, the consistency of the masseter muscle hardness value of the Bland-Altman figure is presented in Figure 3A and 3B; for inter-rater reliability, results are shown in Figure 3C and 3D. For intra-rater reliability, the mean difference was −0.8 or 0.3 N/m and the 95% limits of agreement were −11.0 to 9.4 N/m or −6.2 to 6.7 N/m. For inter-rater reliability, the mean difference was −1.5 or −1.6 N/m and the 95% limits of agreement were −11.9 to 8.8 N/m or −6.3 to 3.0 N/m.
DIFFERENCE IN BILATERAL MASSETER MUSCLE OF STROKE PATIENTS:
A significant difference was found in the bilateral masseter muscle hardness in stroke patients. On the affected side, the hardness index of the masseter muscle was 546.10 N/m, and on the unaffected side, the index value was 787.53 N/m; the mean difference between the masseter muscle on the affected side and that on the unaffected side was −241.43 N/m (Figure 4). The masseter muscle hardness on the unaffected side was significantly greater than on the affected side. The mean value of masticatory performance was 0.63 on the affected side and 0.53 on the unaffected side. The masticatory performance of the masseter muscle of the affected side was significantly less than the unaffected side. The results demonstrated that the MyotonPRO apparatus can be used to evaluate the hardness of the masseter muscle in stroke patients.
CORRELATION BETWEEN THE HARDNESS OF MASSETER MUSCLES AND MASTICATORY PERFORMANCE:
The correlation between the hardness of the masseter muscle and masticatory performance are presented in Table 2. A negative moderate correlation was found between the masseter muscle hardness of the affected side and the masticatory performance of the affected side (r=−0.65, P=0.0018) and between the masseter muscle hardness of the affected side and the masticatory performance of the unaffected side (r=−0.62, P=0.0038). In contrast, no significant correlation was found between the masseter muscle hardness of the unaffected side and the masticatory performance of the affected side (=−0.35, P=0.14) and between the masseter muscle hardness of the unaffected side and the masticatory performance of unaffected side (r=−0.35, P=0.13).
Discussion
INTRA- AND INTER-RATER RELIABILITY:
Our findings showed that intra-rater (ICC=0.986) and inter-rater (ICC=0.989) reliability for evaluating the masseter muscle hardness of the affected side were excellent, and the intra-operator (ICC=0.989) and inter-operator (ICC=0.994) reliability for evaluating the masseter muscle hardness of the unaffected side were also excellent. The results of the reliability test were in accordance with other investigators’ findings quantifying soft tissue characteristics with the MyotonPRO apparatus. One study by Schneebeli et al. [16] demonstrated high intra-rater and inter-rater reliability in measuring Achilles tendon hardness in different positions with the MyotonPRO apparatus. Leonard et al. [17] used the Myotonometer to assess the lateral gastrocnemius and biceps brachii muscles of participants and found excellent intra- and inter-rater reliabilities, with ICC values ranging from 0.85 to 0.95. Further, Liu et al. [15] obtained good intra-operator and inter-operator reliability for measuring tendon hardness bilaterally, with an ICC above 0.87, and established excellent repeatability using the MyotonPRO to evaluate tendon hardness. Additionally, Chuang et al. [18] reported high test-retest reliability in assessing the properties of the affected and unaffected extensor digitorum, flexor carpi radialis, and flexor carpi ulnaris in stroke patients, using the Myotonometer (ICCs, 0.75–0.96). The results from our research established high test-retest reliability with the MyotonPRO device in quantifying the stiffness of the bilateral masseter muscle in stroke patients. The results also demonstrated that the MyotonPRO device can yield credible, effective, and responsive outcome assessments for evaluating muscle biomechanical properties.
Bland-Altman figures served as a visual representation of reliability in comprehensively analyzing data consistency in the current study. As shown in Figure 3, almost all the intra-rater and inter-rater results are more than 90%, with a 95% confidence interval. Thus, the measurement results can be considered to have excellent consistency.
In addition, the value of the minimum detectable change was calculated and showed a true variation. We found that the hardness values of the masseter muscle should be greater than 74 N/m to show a true variation.
DIFFERENCE IN THE STIFFNESS OF BILATERAL MASSETER MUSCLES IN STROKE PATIENTS:
We found that the masseter muscle hardness was significantly greater on the unaffected side than on the affected side in stroke patients (P<0.01), and the masticatory performance of the masseter muscle was significantly greater on the unaffected side than on the affected side (P<0.01). These results were similar to those of previous studies assessing masseter muscles in hemispheric stroke patients. One study by Wang et al. [19] demonstrated that the activation of the masseter muscle in the early biting period was less in elderly stroke patients than in healthy individuals, and the muscle activation was greater on the unaffected side than on the affected side. Cruccu et al. [20] found a significant reduction in strength of paralysis masseter, and voluntary activity at maximum strength was reduced on the side with paralysis. Furthermore, Schimmel et al. [21] reported that the thickness of the masseter muscle is reduced to a greater extent on the affected side than on the unaffected side under relaxation and contraction conditions in stroke patients. These findings suggest that the masticatory efficiency and masseter function may be negatively affected by asymmetrical masseter muscles, leading to a longer oral period and chewing cycle in stroke patients. Cerebrovascular accidents often cause extensive paralysis of the muscles and asymmetric movement patterns. It is important to understand that treatment for masticatory dysfunction involves both compensation and reconstruction methods. Effective activation of the paralysis masseter muscle could enhance the masticatory efficiency, and improvement of the function of the masseter muscle could promote the masticatory performance as a whole [22].
CORRELATION BETWEEN MASSETER MUSCLE HARDNESS AND MASTICATORY PERFORMANCE:
An important result from our study was the finding of a statistically negative moderate correlation between the masseter muscle stiffness of the affected side and the masticatory performance of both the affected and unaffected sides. In contrast, no significant correlation was found between the masseter muscle stiffness of the unaffected side and the masticatory performance of the affected side and unaffected side. These results imply that the stiffness of the masseter muscle potentially only reflects the strength generated by the masseter muscle during forceful biting. Masticatory efficiency was not indicated by the stiffness of the masseter muscle alone in stroke patients in a previous study [23]. Mastication movements are under highly precise control by the nervous system, and they involve comprehensive coordination of the masseter muscle, temporalis, lips, tongue, and oral proprioception [19,21]. Cerebrovascular accidents often cause neurological dysfunction, and such neurological injuries can disrupt the complex control of mastication and decrease masticatory performance [24]. Schimmel et al. [25] have demonstrated that cerebrovascular accidents can cause decreased oral sensory function, thereby potentially affecting masticatory performance. Engelen et al. [26] reported that the oral proprioceptors are important for distinguishing the form of food and therefore are vital for masticatory efficiency. Yamaguchi et al. [27] indicated that tongue thickness is also correlated with masticatory efficiency in healthy adults. In summary, the effects of central nervous system injury can be extensive and complex for masticatory function in stroke patients. The differences in masticatory function and efficiency between healthy adults and stroke patients need further in-depth study, and a more comprehensive evaluation of the oral-facial system of stroke patients is necessary to guide clinical treatment.
LIMITATIONS:
The results of this study need to be considered in light of some limitations. First, this study had a small sample size. More subjects will be recruited for further studies. Second, the MyotonPRO apparatus could not be used to examine multiple muscles at the same time; only the masseter muscle was examined in our study. The temporalis, buccinators, orbicularis oris, and other muscles contribute to bite action, and further research with different muscles could be done to analyze comprehensive masticatory function in stroke patients. Third, the results revealed a moderate correlation in masseter muscle hardness and masticatory performance in stroke patients. In addition to muscle stiffness, masticatory efficiency involves tongue thickness, oral sensation, bite force, and other factors. Future research needs to analyze more indicators of oral function in stroke patients. Finally, patients with cerebral hemorrhage and those with cerebral infarction may have different manifestations of dysfunction and a differential analysis is needed in further study.
Conclusion
Our findings indicate that the MyotonPRO apparatus is a reliable tool for examining masseter muscle stiffness in stroke patients and has excellent intra- and inter-rater reliability. The masticatory function of stroke patients was significantly greater on the unaffected side than on the affected side. A negative moderate correlation was found between masseter muscle stiffness and masticatory performance. The construct validity between the stiffness of the masseter muscle and masticatory performance was established in this study.
Figures
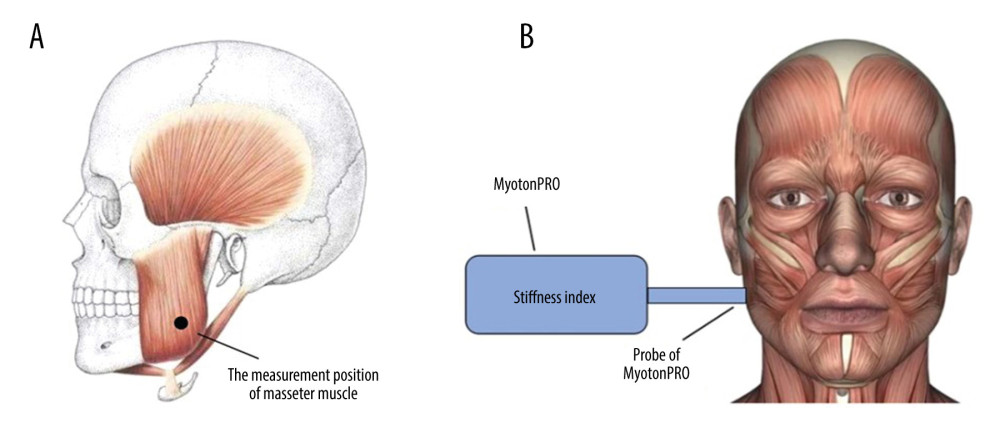 Figure 1. (A) The measurement position of the masseter muscle. (B) The direction of the probe of the MyotonPRO apparatus.
Figure 1. (A) The measurement position of the masseter muscle. (B) The direction of the probe of the MyotonPRO apparatus. 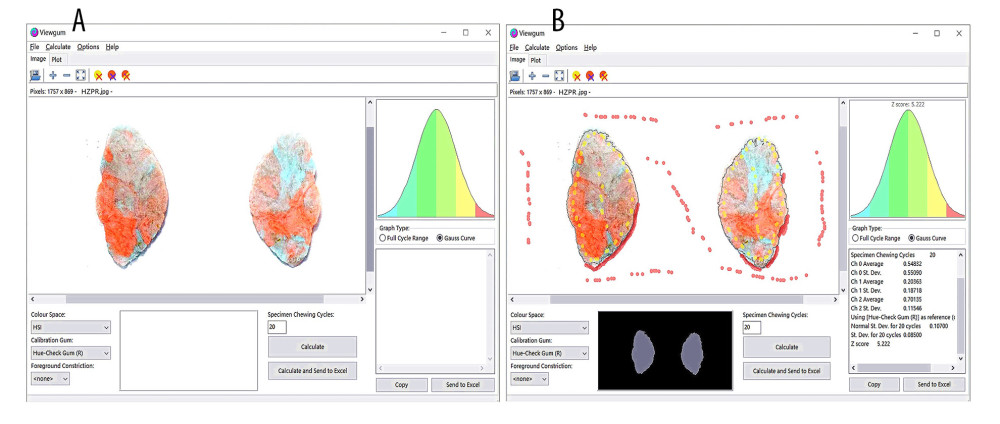 Figure 2. (A) The images of bicolor mixture bolus were imported into the ViewGum software. (B) The results of the image color analysis for masticatory performance.
Figure 2. (A) The images of bicolor mixture bolus were imported into the ViewGum software. (B) The results of the image color analysis for masticatory performance. 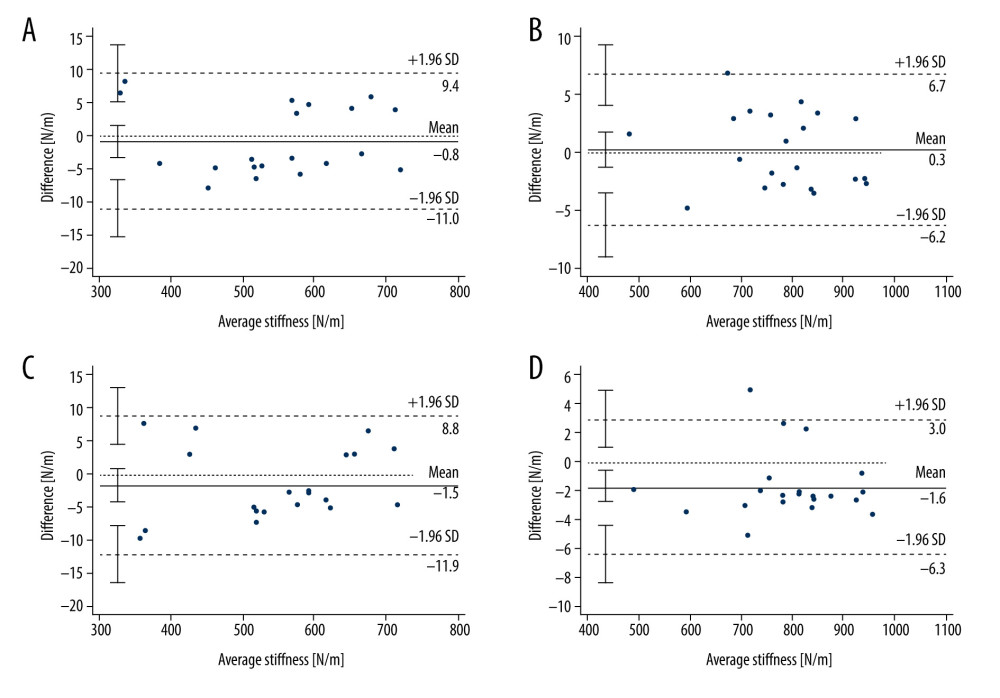 Figure 3. Bland-Altman image of intra-rater credibility and inter-rater credibility of bilateral masseter muscle hardness in stroke patients. The agreement in the hardness value of the bilateral masseter muscle in stroke patients between 2 tests is presented by the mean value of the masseter muscle stiffness (mean value of test for assessor A) for each patient on the affected side (A) and the unaffected side (B). The agreement in the hardness value of the bilateral masseter muscle of stroke patients between different assessors (assessor A and assessor B) is presented by the mean value of the masseter muscle hardness for each patient on the affected side (C) and unaffected side (D). In each Bland-Altman image, the solid line represents the discrepancy of the mean value of the masseter muscle hardness and the dummy lines represent the range of standard deviations.
Figure 3. Bland-Altman image of intra-rater credibility and inter-rater credibility of bilateral masseter muscle hardness in stroke patients. The agreement in the hardness value of the bilateral masseter muscle in stroke patients between 2 tests is presented by the mean value of the masseter muscle stiffness (mean value of test for assessor A) for each patient on the affected side (A) and the unaffected side (B). The agreement in the hardness value of the bilateral masseter muscle of stroke patients between different assessors (assessor A and assessor B) is presented by the mean value of the masseter muscle hardness for each patient on the affected side (C) and unaffected side (D). In each Bland-Altman image, the solid line represents the discrepancy of the mean value of the masseter muscle hardness and the dummy lines represent the range of standard deviations. 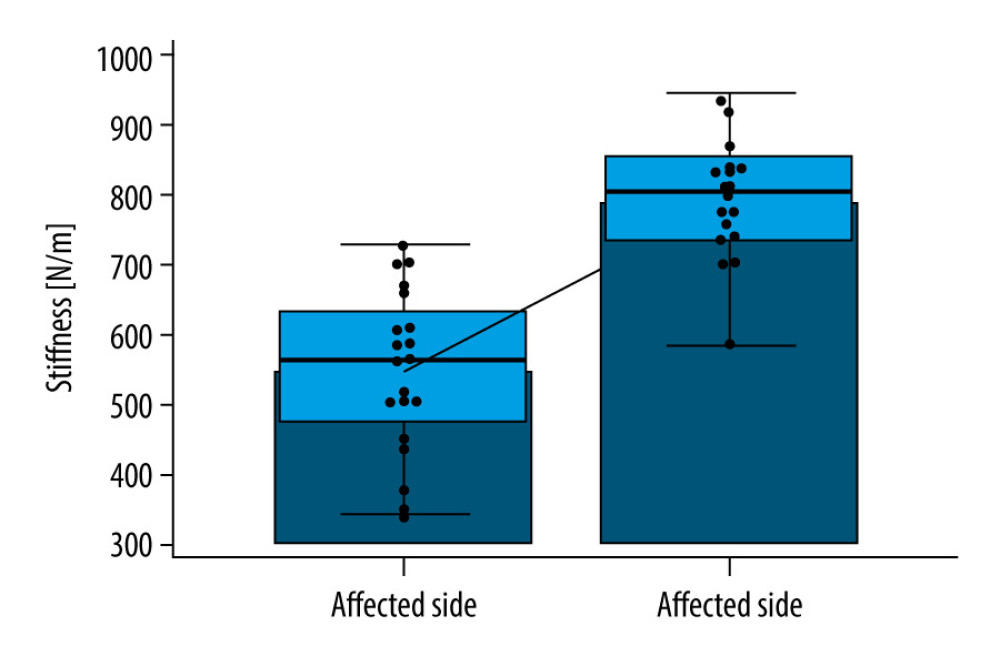 Figure 4. Comparison of the masseter muscle hardness values of the affected side and the unaffected side.
Figure 4. Comparison of the masseter muscle hardness values of the affected side and the unaffected side. References
1. Kirkevold M, Bronken BA, Martinsen R, Promoting psychosocial well-being following a stroke: Developing a theoretically and empirically sound complex intervention: Int J Nurs Stud, 2012; 49(4); 386-97
2. Westergren A, Karlsson S, Andersson P, Eating difficulties, need for assisted eating, nutritional status and pressure ulcers in patients admitted for stroke rehabilitation: J Clin Nurs, 2001; 10(2); 257-69
3. Axelsson K, Norberg A, Asplund K, Eating after a stroke – towards an integrated view: Int J Nurs Stud, 1984; 21(2); 93-99
4. Perry L, McLaren S, Eating disabilities and dietary intake after stroke: Clin Eff Nurs, 2001; 5(2); 88-92
5. Alkan A, Keskiner I, Arici S, Sato S, The effect of periodontitis on biting abilities: J Periodontol, 2006; 77(8); 1442-45
6. Ahlgren J, EMG pattern of temporalis in normal occlusion: Eur J Orthod, 1986; 8(3); 185-91
7. Cakir E, Vinyard CJ, Essick G, Interrelations among physical characteristics, sensory perception and oral processing of protein based soft-solid structures: Food Hydrocolloids, 2012; 29(1); 234-45
8. Ariji Y, Nakayama M, Nishiyama W, Shear-wave sonoelastography for assessing masseter muscle hardness in comparison with strain sonoelastography: Study with phantoms and healthy volunteers: Dentomaxillofac Radiol, 2016; 45(2); 20150251
9. Witvrouw E, Danneels L, Asselman P, Muscle flexibility as a risk factor for developing muscle injuries in male professional soccer players. A prospective study: Am J Sports Med, 2003; 31; 41-46
10. Kubo K, Morimoto M, Komuro T, Effects of plyometric and weight training on muscle-tendon complex and jump performance: Med Sci Sports Exerc, 2007; 39; 1801-10
11. Li YP, Feng YN, Liu CL, Zhang ZJ, Paraffin therapy induces a decrease in the passive stiffness of gastrocnemius muscle belly and Achilles tendon: A randomized controlled trial: Medicine (Baltimore), 2020; 99(12); e19519
12. Huang J, Qin K, Tang C, Assessment of passive stiffness of medial and lateral heads of gastrocnemius muscle, Achilles tendon, and plantar fascia at different ankle and knee positions using the MyotonPRO: Med Sci Monit, 2018; 24; 7570-76
13. Zhang ZJ, Ng GY, Lee WC, Fu SN, Changes in morphological and elastic properties of patellar tendon in athletes with unilateral patellar tendinopathy and their relationships with pain and functional disability: PLoS One, 2014; 9(10); e108337
14. Lin KC, Hsieh YW, Wu CY, Minimal detectable change and clinically important difference of the Wolf Motor Function Test in stroke patients: Neurorehabil Neural Repair, 2009; 23(5); 429-34
15. Liu CL, Li YP, Wang XQ, Zhang ZJ, Quantifying the stiffness of Achilles tendon: Intra- and inter-operator reliability and the effect of ankle joint motion: Med Sci Monit, 2018; 24; 4876-81
16. Schneebeli A, Falla D, Clijsen R, Barbero M, Myotonometry for the evaluation of Achilles tendon mechanical properties: A reliability and construct validity study: BMJ Open Sport Exerc Med, 2020; 6(1); e000726
17. Leonard CT, Deshner WP, Romo JW, Myotonometer intra- and interrater reliabilities: Arch Phys Med Rehabil, 2003; 84(6); 928-32
18. Chuang LL, Wu CY, Lin KC, Reliability, validity, and responsiveness of myotonometric measurement of muscle tone, elasticity, and stiffness in patients with stroke: Arch Phys Med Rehabil, 2012; 93(3); 532-40
19. Wang JS, Lee JH, Kim NJ, Effects of neuromuscular electrical stimulation on masticatory muscles in elderly stroke patients: J Phys Ther Sci, 2015; 27(9); 2767-70
20. Cruccu G, Fornarelli M, Manfredi M, Impairment of masticatory function in hemiplegia: Neurology, 1988; 38(2); 301-6
21. Schimmel M, Leemann B, Christou P, Masseter muscle thickness in hospitalised stroke patients: J Oral Rehabil, 2010; 37(9); 726-30
22. Lee KW, Kim SB, Lee JH, Effects of neuromuscular electrical stimulation for masseter muscle on oral dysfunction after stroke: Ann Rehabil Med, 2019; 43(1); 11-18
23. Hara K, Namiki C, Yamaguchi K, Association between myotonometric measurement of masseter muscle stiffness and maximum bite force in healthy elders: J Oral Rehabil, 2020; 47(6); 750-56
24. Bakke M, Møller E, Thomsen CE, Chewing in patients with severe neurological impairment: Arch Oral Biol, 2007; 52; 399-403
25. Schimmel M, Voegeli G, Duvernay E, Oral tactile sensitivity and masticatory performance are impaired in stroke patients: J Oral Rehabil, 2017; 44(3); 163-71
26. Engelen L, van der Bilt A, Bosman F, Relationship between oral sensitivity and masticatory performance: J Dent Res, 2004; 83(5); 388-92
27. Yamaguchi K, Tohara H, Hara K, Tongue thickness is associated with masticatory performance of perioral muscles: Ultrasonographic study of perioral muscle characteristics in healthy young subjects: J Oral Rehabil, 2020; 47(3); 325-31
Figures
Figure 1. (A) The measurement position of the masseter muscle. (B) The direction of the probe of the MyotonPRO apparatus.Figure 2. (A) The images of bicolor mixture bolus were imported into the ViewGum software. (B) The results of the image color analysis for masticatory performance.Figure 3. Bland-Altman image of intra-rater credibility and inter-rater credibility of bilateral masseter muscle hardness in stroke patients. The agreement in the hardness value of the bilateral masseter muscle in stroke patients between 2 tests is presented by the mean value of the masseter muscle stiffness (mean value of test for assessor A) for each patient on the affected side (A) and the unaffected side (B). The agreement in the hardness value of the bilateral masseter muscle of stroke patients between different assessors (assessor A and assessor B) is presented by the mean value of the masseter muscle hardness for each patient on the affected side (C) and unaffected side (D). In each Bland-Altman image, the solid line represents the discrepancy of the mean value of the masseter muscle hardness and the dummy lines represent the range of standard deviations.Figure 4. Comparison of the masseter muscle hardness values of the affected side and the unaffected side. Tables
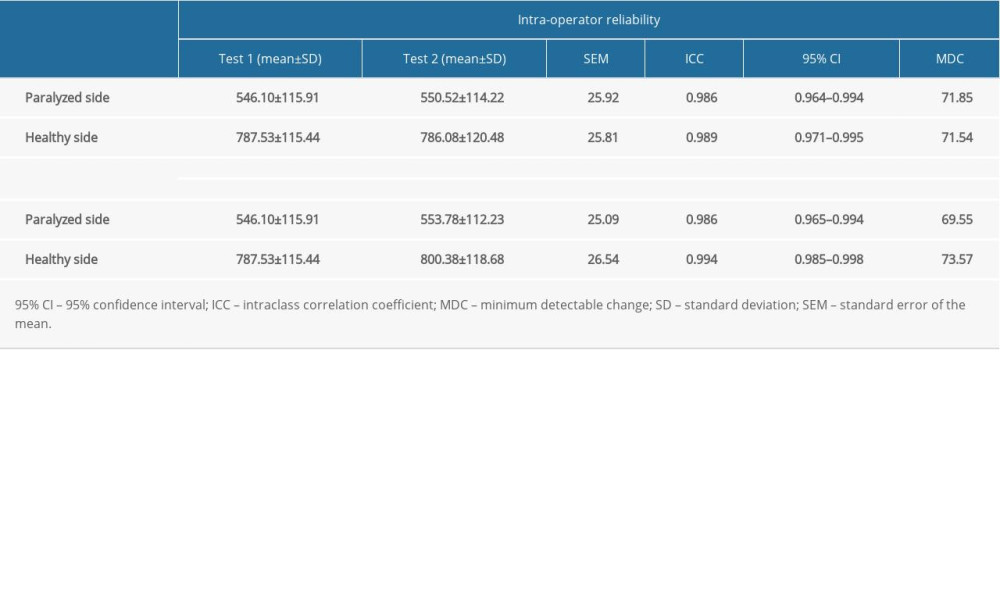 Table 1. Intra- and inter-operator reliability of MyotonPRO in measurement of bilateral masseter muscle stiffness in stroke patients.
Table 1. Intra- and inter-operator reliability of MyotonPRO in measurement of bilateral masseter muscle stiffness in stroke patients.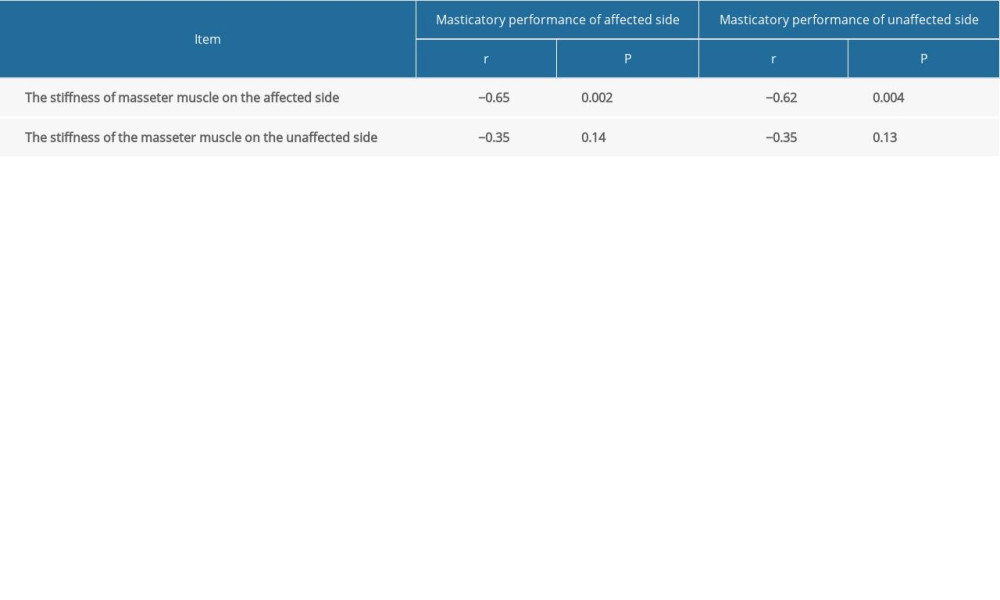 Table 2. Spearman’s correlation coefficients (r) between the stiffness of the bilateral masseter muscle and masticatory performance.Table 1. Intra- and inter-operator reliability of MyotonPRO in measurement of bilateral masseter muscle stiffness in stroke patients.Table 2. Spearman’s correlation coefficients (r) between the stiffness of the bilateral masseter muscle and masticatory performance.
Table 2. Spearman’s correlation coefficients (r) between the stiffness of the bilateral masseter muscle and masticatory performance.Table 1. Intra- and inter-operator reliability of MyotonPRO in measurement of bilateral masseter muscle stiffness in stroke patients.Table 2. Spearman’s correlation coefficients (r) between the stiffness of the bilateral masseter muscle and masticatory performance. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387