07 March 2021: Clinical Research
Association of Leptin Receptor Gene Polymorphisms with Keloids in the Chinese Han Population
Jing Liu1ABCD, Limin Cai1CDEF, Zepeng Zhang1BCD, Yanli Ma1BCDF, Yongchen Wang2ADE*DOI: 10.12659/MSM.928503
Med Sci Monit 2021; 27:e928503






Abstract
BACKGROUND: The association between leptin receptor (LEPR) polymorphisms and keloids is still unclear. Our study aimed to explore the association between LEPR gene polymorphisms and keloids in the Chinese Han population.
MATERIAL AND METHODS: We implemented a case-control study in a cohort of 352 keloid patients and 299 healthy controls to analyze the correlation between 4 SNPs (rs1137101, rs1938496, rs6588147, and rs7555955) and keloids. Genomic DNA was extracted from peripheral blood by using TGuide M16 (Tiangen). Genotyping of LEPR SNPs was performed using an improved multiple ligase detection reaction (iMLDR) by Shanghai Genesky Bio-Tech Co., Ltd.
RESULTS: We found that patients caring the AA genotype of rs1137101 and the CC genotype rs1938496 tend to have the increased risk of keloids (P=0.026, P=0.047). Carrying the GA, AA gene type, and G allele frequencies of rs7555955, patients were more likely to have to keloids (P=0.030, P=0.016, P=0.018, respectively). There were no significant differences in genotype distribution and allele frequencies of rs6588147 between cases and controls. The association of rs1137101 and rs7555955 under dominant, recessive, and allele models exhibited significant differences among family-history keloid patients, no-family-history keloid groups, and normal controls (χ²=6.471, P=0.039; χ²=6.477, P=0.039; χ²=6.197, P=0.045, respectively). Similarly, the OR of rs1137101 in the recessive model was significantly higher in patients with a family history of keloids than those in controls. Nonetheless, there are significant ORs of rs1938496 and rs6588147 among the mild-moderate keloid, severe keloid, and control groups.
CONCLUSIONS: The LEPR gene polymorphisms are associated with keloid formation and severity, especially in patients with a positive family history.
Keywords: Genotyping Techniques, keloid, Polymorphism, Genetic, Asians, Case-Control Studies, Cohort Studies, ethnicity, Gene Frequency, Genetic Predisposition to Disease, Genotype, Polymorphism, Single Nucleotide, Receptors, Leptin
Background
Keloids are considered to be benign tumors because they continuously and aggressively grow outside the original wound [1]. Keloids are characterized by the excessive deposition of extracellular matrix collagen, which is synthesized by the increased number of fibroblasts [2]. The frequency of ritual practices of scarification, tattooing, and piercing coupled with the predisposition of the black skin to develop this anomaly make keloids a serious problem for sub-Saharan Africans, particularly when these lesions are located on uncovered areas [3]. However, the pathogenic mechanisms at the molecular level are still unknown. Keloid scars are aesthetically unpleasant and functional disabilities that cause physical and psychological pain. Genetic risk factors contribute to keloid formation by a higher prevalence in certain races, increased familial aggregation, parallelism in identical twins, and alterations in gene expression [4].
Leptin consists of 167 amino acids; it is a product of the obese gene and a member of the type I helical cytokine family [5]. Previous studies have indicated that leptin shows a great increase during acute inflammation and infection, suggesting that leptin is a pro-inflammatory cytokine. Meanwhile, leptin promotes the activity of macrophage phagocytosis and provokes them to generate a variety of pro-inflammatory cytokines, such as IL-1, TNF-a, and IL6 [6]. Many studies have demonstrated that leptin may be involved in wound healing [7,8], organ fibrosis, and scar formation by regulating fibroblasts, keratinocytes, and inflammatory cells [9,10]. Seleit et al [11] reported that leptin is overexpressed in both keloid and hypertrophic scars when compared with normal skin. The expression of leptin is further associated with keloid patients with a positive family history [12]. As a family member of the cytokine receptors, the leptin receptor (LEPR) plays a key role in leptin functions [13]. LEPR are widely expressed in basal cell layer, fibroblasts, sebaceous gland cells, and vascular endothelial cells [14]. In human and animal cell lines, LEPR has been reported to have associations with both increased tumor cell proliferation in vitro and in vivo and promotion of angiogenesis in malignant and benign epithelial breast cells [15]. Zhai et al [16] found increased expression of leptin and LEPR in keloids. The combination of leptin and LEPR stimulates fibroblast proliferation and collagen deposition and synthesis, which also affects myofibroblasts and scar remodeling [17,18]. Recent genetic studies have focused on the relationship between keloid and single-nucleotide polymorphisms (SNPs) of specific genes. Several polymorphisms in the LEPR gene may affect the functionality of the receptor, modify its signaling capacity, and develop disease, including NEDD4 [19], IL-6 [20], and ADAM33 [21]. However, the association between LEPR polymorphisms and keloids is still unclear. Hence, we aimed to explore the role of LEPR gene polymorphisms in Chinese patients with keloids by conducting a case-control study to examine the association of 4 SNPs in the LEPR gene with keloid phenotypes to provide genetic evidence for keloid susceptibility loci in the Chinese Han population.
Material and Methods
STUDY SUBJECTS:
A total of 352 keloid patients and 299 healthy controls were consecutively recruited from May 2015 to December 2016 at the Department of Dermatology, the First Affiliated Hospital of Harbin Medical University. All patients were self-reported to be of Chinese Han ancestry and were examined by at least 2 dermatologists in an outpatient clinic. In this study, patients with some symptoms and a hypertrophic scar of keloid were excluded. These keloid scars were confirmed by whether they proliferated outside the boundaries of the original wound and made a continuous growth. The control groups were healthy individuals without systemic disease, as well as autoimmune and family history of keloids (including first-, second-, and third-degree relatives). Participants were excluded if they were obese. The clinical and demographic features were collected by a standardized questionnaire and reviewed by experienced dermatologists. After obtaining written informed consent, venous blood samples were collected from all keloid patients and the control subjects. This study received approval from the Ethics Committee of the First Affiliated Hospital of Harbin Medical University.
The severity of keloids was categorized into mid-moderate and severity [22,23], based on color, scar height, pliability, pain, and itching of keloid scars. Each indicator was given 0–3 points according to the clinical assessment. A score of 0–10 points indicated mid-moderate keloids, while 11–15 points indicated severe keloids.
SNPS SELECTION AND GENOTYPING:
The selection of LEPR SNPs was based on 3 main criteria: (i) the SNPs are located in the 3′UTR of the LEPR gene; (ii) the LEPR SNPs can regulate the expression of the corresponding gene; (iii) the LEPR SNPs have been reported to be associated with diseases [5], although some have not been investigated in keloid disease. The genomic DNA was extracted from peripheral blood using TGuide M16 (Tiangen). Genotyping of LEPR SNPs was performed with an improved multiple ligase detection reaction (iMLDR) by Shanghai Genesky Bio-Tech Co., Ltd. (http://biotech.geneskies.com/index.html). The primer sequences of the selected SNPs are listed in Table 1. As a result, a total of 4 SNPs (rs1137101, rs1938496, rs6588147, and rs7555955) were included for genotyping in our cohort.
STATISTICAL ANALYSIS:
SPSS 19.0 (SPSS, Inc., Chicago, USA) was used for all statistical analyses. The chi-square test was used to evaluate statistically significant differences of clinical and demographic data between patients with keloid and controls. Hardy-Weinberg equilibrium test for genotyping data was performed using Plink (version 1.07). For the allelic association between SNP and keloid, the
Results
DISTRIBUTION OF GENOTYPE AND ALLELE FREQUENCIES OF LEPR SNPS:
We enrolled a total of 352 keloid patients and 299 healthy controls in this study. All measurement data are expressed as mean±standard deviation. In the case group, there were 183 females and 169 males with a mean age of 32.69±12.19 years. In the control group, there were 153 females and 146 males with a mean age of 34.16±9.00 years. The demographic and clinical characteristics of all participants are listed in Table 2. No significant differences were observed between the keloid patients and controls for age and sex distributions. The mild-to-moderate rate of keloids was 80%, and 16% of keloid cases had a family history. The observed genotype frequencies of all detected SNPs were consistent with the Hardy-Weinberg of controls (P>0.05).
The results of allele frequency and gene type frequencies of the 4 SNPs in cases and controls are shown in Table 3. The AA genotype of rs1137101 and the CC genotype of rs1938496 were significantly different between patients with keloids and the control groups (P=0.026, OR=4.790, 95% CI=1.053–21.785; P=0.047, OR=2.115, 95% CI=0.994–4.497; respectively). The GA and AA gene types and G allele frequencies of rs7555955 showed significant differences between cases and controls (P=0.03, OR=1.475, 95% CI=1.038–2.097; P=0.016, OR=0.660, 95% CI=0.471–0.925; P=0.018, OR=1.420, 95% CI=1.061–1.900, respectively). However, there were no significant differences in genotype distribution and allele frequencies of rs6588147 between cases and controls (P > 0.05).
ASSOCIATIONS OF LEPR SNPS WITH KELOID SEVERITY AND FAMILY HISTORY:
We examined the associations between LEPR SNPs and keloid severity (Table 4). Assessment of rs1137101 and rs1938496 revealed that in the recessive models of inheritance, there were significant ORs among mild-moderate keloid, severe keloid, and control groups (c2=12.191, P=0.002; c2=7.693, P=0.021). Further statistical analysis of rs1137101 showed that in the recessive model, the OR of the severe keloid group was significantly higher than in the mild-moderate keloid group and controls (OR=0.283, 95% CI=0.084–0.955, P=0.031; OR=11.432, 95% CI=2.168–60.176, P=0.000; respectively). However, we found that in the recessive model of rs1938496, there was a significant difference between the severe keloid groups and control groups (P=0.005, OR=3.729, 95% CI=1.415–9.830). Notably, analysis of rs6588147 and rs7555955 showed that in the dominant, recessive, and allelic models, the severe keloid group had significantly higher ORs of mild-moderate keloid and controls (P<0.01) (Table 4). In addition, no significant ORs were found between mild-moderate keloid group and control group with LEPR SNPs.
Further, we evaluated the associations between the 4 LEPR SNPs and family history of keloids (Table 5). The association of rs1137101 in the recessive model and rs7555955 in the dominant model and allele model was significantly different among the family-history keloid patients, no-family-history keloid groups, and normal controls (rs1137101 recessive model: c2=6.471, P=0.039; rs7555955 dominant model: c2=6.477, P=0.039; allelic model: c2=6.197, P=0.045). Similarly, the OR of rs1137101 in the recessive model was significantly higher in patients with a family history of keloids than in control groups (OR=8.100 95% CI=1.323–49.603, P=0.008). Assessment of rs7555955 demonstrated that in the dominant and allele models, the keloid patients with family history (dominant model: P=0.041, OR=1.830, 95% CI=1.019–3.287; allele model: P=0.043, OR=1.652 95% CI=1.011–2.700) had significant ORs as compared with both the controls and those without family history (dominant model: P=0.036, OR=1.457, 95% CI=1.025–2.073; allele model: P=0.039, OR=1.375 95% CI=1.015–1.864). Nonetheless, there were no significant ORs of rs1938496 and rs6588147 among the family-history keloid patients, no-family-history keloid groups, and normal controls.
Discussion
Keloids are benign fibro-proliferative tumors that are unique to humans, resulting from abnormal healing of injured or irritated skin. Keloid scars are thought to be a polygenic disease, affected by both hereditary and environmental factors [24]. In recent years, with the development of genome-wide association study, we have made great progress in defining the genetic basis of keloids. We have found various susceptibility loci containing association of LEPR SNPs with keloids in the Chinese Han population. In our present study, there were no significant differences in genotype distribution and allele frequencies of rs6588147 between patients with keloid and controls. However, we found that patients carrying the AA genotype of rs1137101 and the CC genotype of rs1938496 tend to have increased risk of keloids. Carrying the GA, AA gene type and G allele frequencies of rs7555955 makes patients were more susceptible to keloids.
However, it should be noted the severe keloid groups had significantly higher ORs as compared with the mild-moderate keloid and control groups. These differences can be ascribed to the small sample size and/or disparities in the minor allele frequencies. Assessment of rs1137101 and rs1938496 revealed that in the recessive models of inheritance, there were significant ORs among mild-moderate keloid, severe keloid, and control groups. Analysis of rs6588147 and rs7555955 showed that in the dominant, recessive, and allele models, the severe keloid groups had significantly higher ORs compared to the mild-moderate keloid group and controls. In addition, no significant ORs were found between the mild-moderate keloid group and control group with LEPR SNPs.
Further, we evaluated the associations between the 4 LEPR SNPs and family history of keloids. The association of rs1137101 and rs7555955 in the dominant, recessive, and allele models exhibited significant differences among family-history keloid patients, no-family-history keloid groups, and normal controls. Similarly, the OR of rs1137101 in the recessive model was significantly higher in patients with a family history of keloids than those in control groups. Nonetheless, there were no significant ORs of rs1938496 and rs6588147 among the mild-moderate keloid, severe keloid, and control groups.
SNP rs1137101 (Gln223Arg) has been receiving increased research attention; it is located in the intron region exon 4 of LEPR and can alter the structure and function of LEPR protein. This SNP has a significant association with knee osteoarthritis in northwest Chinese population with Han ethnicity [25], and obesity in Pacific Islanders [26]. LEPR rs6588147 is an intron SNP. Slattery et al [5] found this SNP caused colon cancer susceptibility among men. It was found to decrease the risk of HCC in an eastern Chinese Han population [27]. SNP rs7555955 is the intronic region of the LEPR gene; it can regulate the expression of its corresponding protein. LEPR rs1938496 is a 3′UTP SNP, which may play an active role in post-transcriptional gene regulation. However, our study only analyzed 4 SNPs in the LEPR gene that were associated with the severity of keloid disease. Further investigations are needed to identify other SNPs in the LEPR gene related to keloid severity.
Conclusions
In summary, our study confirmed that LEPR gene polymorphisms are associated with the development and progression of keloids in the northeastern Chinese Han population. Genetic factors of LEPR might influence keloid severity, especially in patients with a positive family history. The 4 SNPs in the LEPR gene could serve as biomarkers for early detection and targeted therapeutics of keloids.
Tables
Table 1. Primer sequences of the studied LEPR SNPs.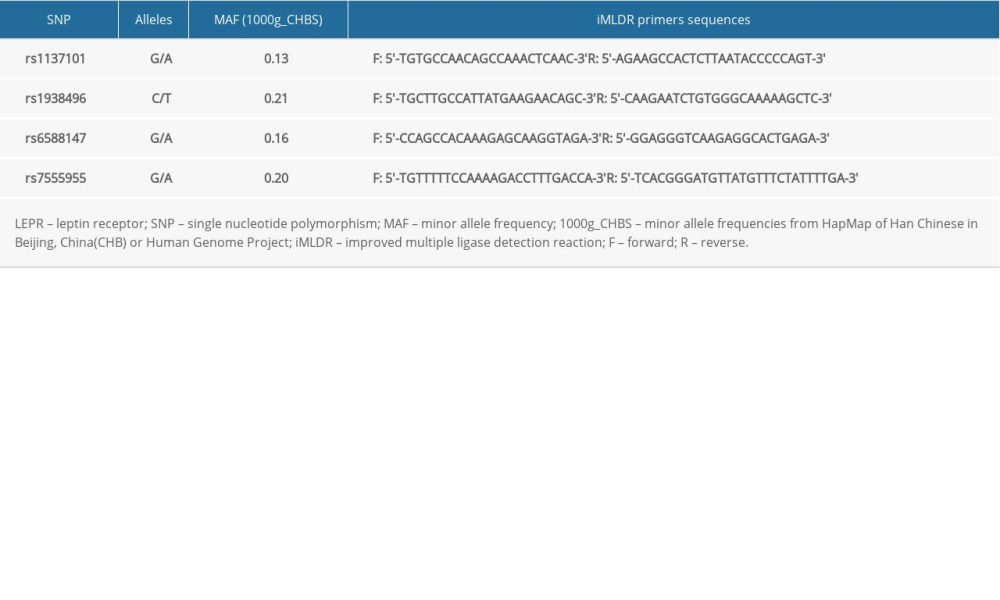 Table 2. Demographic and clinical characteristics of study subjects.
Table 2. Demographic and clinical characteristics of study subjects.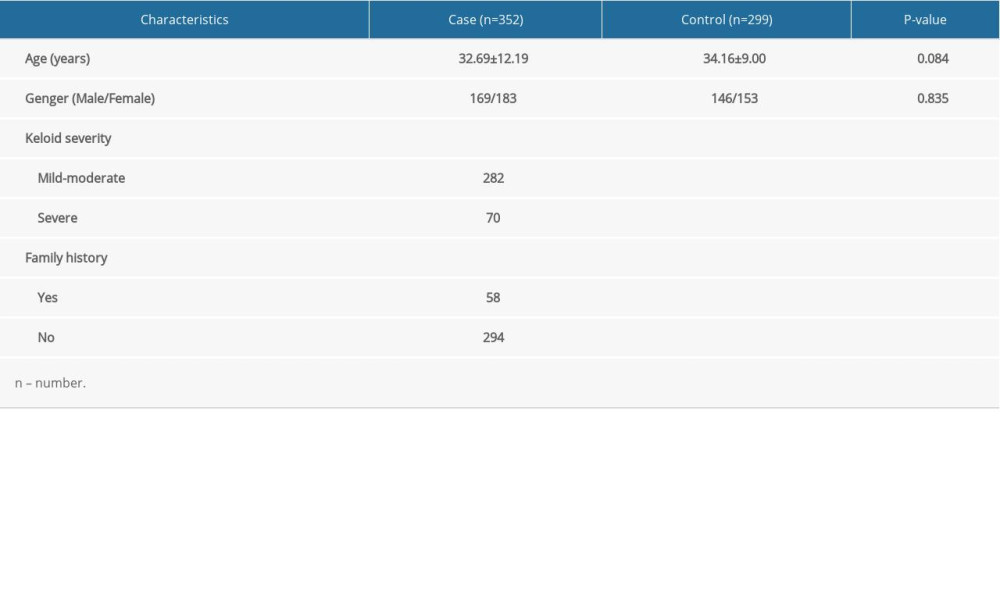 Table 3. The frequencies of genotypes and alleles in LEPR gene.
Table 3. The frequencies of genotypes and alleles in LEPR gene.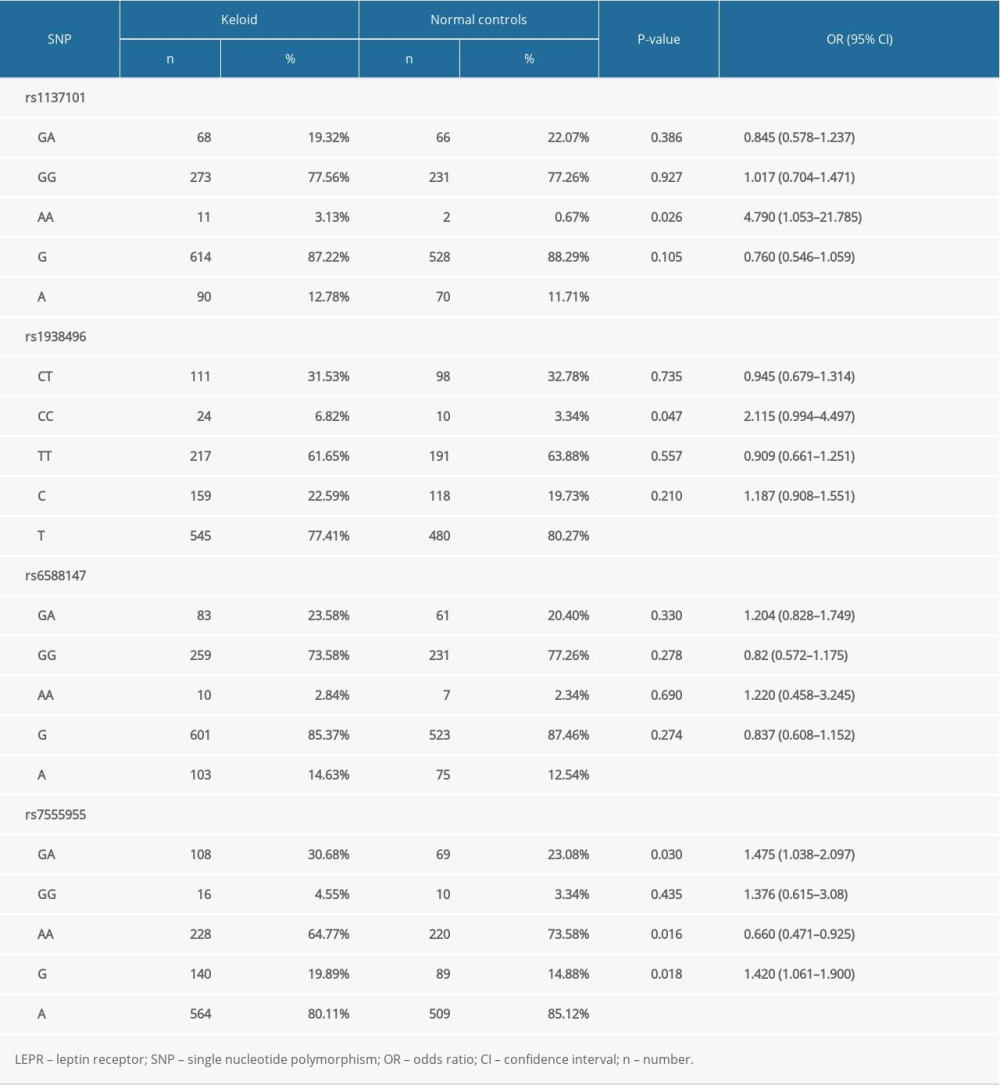 Table 4. Associations between LEPR SNPs and keloid severity.
Table 4. Associations between LEPR SNPs and keloid severity.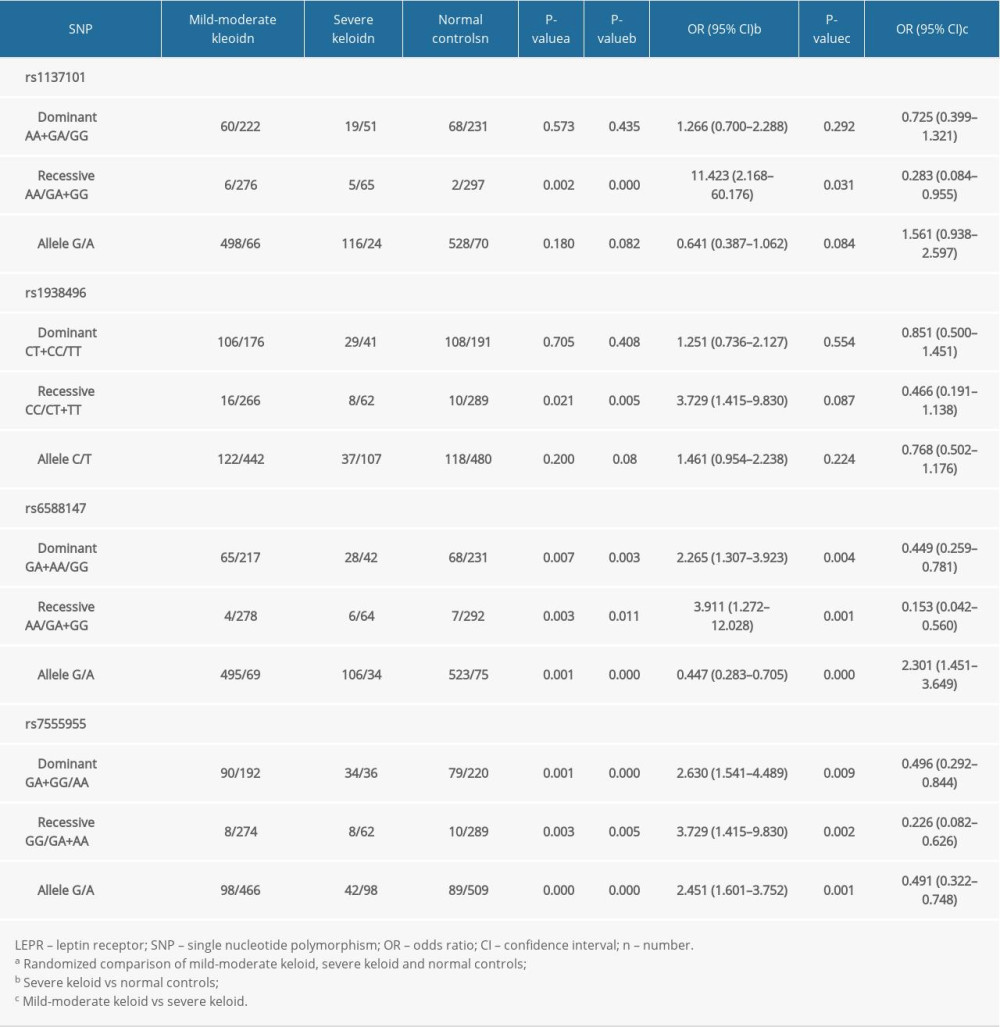 Table 5. Associations between LEPR SNPs and family history of keloids.
Table 5. Associations between LEPR SNPs and family history of keloids.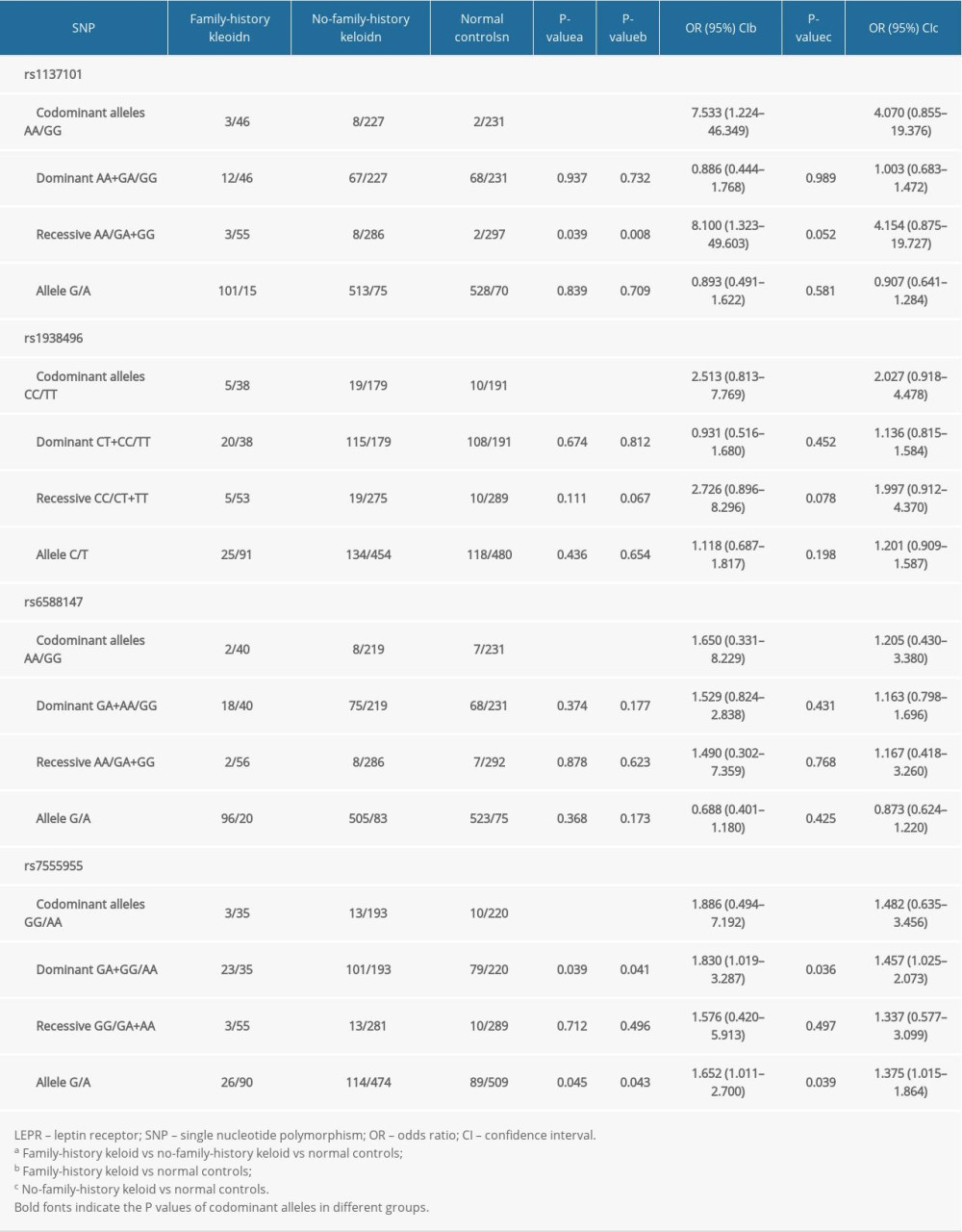
References
1. Gauglitz GG, Korting HC, Pavicic T, Hypertrophic scarring and keloids: pathomechanisms and current and emerging treatment strategies: Mol Med, 2011; 17; 113
2. Ho JD, Chung HJ, Ms Barron A, Extensive CD34-to-CD90 fibroblast transition defines regions of cutaneous reparative, hypertrophic, and keloidal scarring: Am J Dermatopathol, 2019; 41; 16-28
3. Kouotou EA, Nansseu JR, Omona Guissana E, Epidemiology and clinical features of keloids in Black Africans: A nested case-control study from Yaoundě, Cameroon: Int J Dermatol, 2019; 58; 1135-40
4. Bayat A, Arscott G, Ollier WER, “Aggressive keloid”: A severe variant of familial keloid scarring: J R Soc Med, 2003; 96; 554-55
5. Slattery ML, Wolff RK, Herrick J, Leptin and leptin receptor genotypes and colon cancer: Gene–gene and gene–lifestyle interactions: Int J Cancer, 2008; 122; 1611-17
6. Versini M, Jeandel P-Y, Rosenthal E, Shoenfeld Y, Obesity in autoimmune diseases: Not a passive bystander: Autoimmun Rev, 2014; 13; 981-1000
7. Umeki H, Tokuyama R, Ide S, Leptin promotes wound healing in the oral mucosa: PLoS One, 2014; 9; e101984
8. Murad A, Nath AK, Cha S-T, Leptin is an autocrine/paracrine regulator of wound healing: FASEB J, 2003; 17; 1895
9. Cao Y, Gao F, Li C-Z, Xue Y-M, Expression of leptin and its long-form receptor in the marginal cutaneous tissues of diabetic foot ulcers: Acta Diabetol, 2012; 49; 205
10. Tadokoro S, Ide S, Tokuyama R, Leptin promotes wound healing in the skin: PLoS One, 2015; 10; e0121242
11. Seleit I, Bakry OA, Samaka RM, Tawfik AS, Immunohistochemical evaluation of leptin expression in wound healing: A clue to exuberant scar formation: Appl Immunohistochem Mol Morphol, 2016; 24; 296-306
12. Park TH, Park JH, Tirgan MH, Clinical implications of single-versus multiple-site keloid disorder: A retrospective study in an Asian population: Ann Plast Surg, 2015; 74; 248-51
13. Gorska E, Popko K, Stelmaszczyk-Emmel A, Leptin receptors: Eur J Med Res, 2010; 15(Suppl 2); 50-54
14. Stallmeyer B, Kämpfer H, Podda M, A novel keratinocyte mitogen: Regulation of leptin and its functional receptor in skin repair: J Invest Dermatol, 2001; 117; 98-105
15. Hu X, Juneja SC, Maihle NJ, Cleary MP, Leptin – a growth factor in normal and malignant breast cells and for normal mammary gland development: J Natl Cancer Inst, 2002; 94; 1704-11
16. Zhai X-X, Tang Z-M, Ding J-C, Lu X-L, Expression of TGF-b1/mTOR signaling pathway in pathological scar fibroblasts: Mol Med Rep, 2017; 15; 3467-72
17. Baumeister S, Dragu A, Jester AThe role of plastic and reconstructive surgery within an interdisciplinary treatment concept for diabetic ulcers of the foot: Dtsch Med Wochenschr, 2004; 129; 676-80 [in German]
18. Goren I, Kampfer H, Podda M, Leptin and wound inflammation in diabetic ob/ob mice: Differential regulation of neutrophil and macrophage influx and a potential role for the scab as a sink for inflammatory cells and mediators: Diabetes, 2003; 52; 2821-32
19. Zhu F, Wu B, Li P: PLoS One, 2013; 8; e62377
20. Zhu XJ, Li WZ, Li H, Association of interleukin-6 gene polymorphisms and circulating levels with keloid scars in a Chinese Han population: Genet Mol Res, 2017; 16 gmr16029110
21. Han J, Han J, Yu D, Association of ADAM33 gene polymorphisms with keloid scars in a northeastern Chinese population: Cell Physiol Biochem, 2014; 34; 981-87
22. Hirshowitz B, Lindenbaum E, Har-Shai Y, Static-electric field induction by a silicone cushion for the treatment of hypertrophic and keloid scars: Plast Reconstr Surg, 1998; 101; 1173-83
23. Idriss N, Maibach HI, Scar assessment scales: A dermatologic overview: Skin Res Technol, 2009; 15; 1-5
24. Halim AS, Emami A, Salahshourifar I, Kannan TP, Keloid scarring: Understanding the genetic basis, advances, and prospects: Arch Plast Surg, 2012; 39; 184-89
25. Yang J, Du H, Lv J, Zhang L, Association of rs1137101 polymorphism in LEPR and susceptibility to knee osteoarthritis in a Northwest Chinese Han population: BMC Musculoskelet Disord, 2016; 17; 311
26. Furusawa T, Naka I, Yamauchi T, Natsuhara K, The Q223R polymorphism in LEPR is associated with obesity in Pacific Islanders: Hum Genet, 2010; 127; 287-94
27. Zhang S, Jiang J, Chen Z, Investigation of LEP and LEPR polymorphisms with the risk of hepatocellular carcinoma: A case-control study in Eastern Chinese Han population: Onco Targets Ther, 2018; 11; 2083
Tables
Table 1. Primer sequences of the studied LEPR SNPs.Table 2. Demographic and clinical characteristics of study subjects.Table 3. The frequencies of genotypes and alleles in LEPR gene.Table 4. Associations between LEPR SNPs and keloid severity.Table 5. Associations between LEPR SNPs and family history of keloids. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387