19 March 2021: Clinical Research
Retrospective Analysis of Clinicopathological Characteristics of Lacrimal Gland Pleomorphic Adenoma and Mechanism of Tumorigenesis by the Imbalance Between Apoptosis and Proliferation
Meng Lv1ABCDEF, Zhi-Jun Dong1ABCEG, Yue-Xin Tong2BCDE, Tian Li1B, Yan Hei3BE, Xin-Ji Yang3BG, Wei-Li Dong1AE*DOI: 10.12659/MSM.929152
Med Sci Monit 2021; 27:e929152






Abstract
BACKGROUND: Lacrimal gland pleomorphic adenoma (LGPA) is the most common clinically benign epithelial tumor of the lacrimal gland and is predominantly comprised of epithelial cells and interstitial components. At present, the exact pathogenesis of LGPA remains unclear. Previous research has indicated that the occurrence of LGPA may be related to excessive cell proliferation.
MATERIAL AND METHODS: This study observed the clinicopathological characteristics of LGPA and investigated the tumorigenesis mechanism of cell over-proliferation caused by the imbalance between apoptosis and proliferation. A total of 27 cases were collected from the Department of Ophthalmology of the Affiliated Hospital of Chengde Medical University and the Third Medical Center of Chinese PLA General Hospital from April 2017 to November 2019. Hematoxylin-eosin (HE) staining and immunohistochemical staining were used to observe the pathological characteristics and analyze the expression of bcl-2 and bax in the lacrimal gland.
RESULTS: Compared with normal lacrimal gland tissues, LGPA tumor tissues had obvious changes in pathological morphology. The expression of bcl-2 in LGPA lesion tissues was dramatically higher (P<0.001), the expression of bax was not significantly different between groups (P=0.25), but the ratio of bcl-2/bax was significantly higher in tumor tissues (P=0.01).
CONCLUSIONS: We found that the lacrimal gland tumor tissues had obvious excessive proliferation in pathomorphology, which revealed the necessity of complete surgical removal of the capsule from the perspective of pathological morphology and provided a theoretical basis for the hypothesis that the imbalance between apoptosis and proliferation could lead to cell hyperproliferation.
Keywords: Adenoma, Pleomorphic, Lacrimal Apparatus, carcinogenesis, Eye Neoplasms, Lacrimal Apparatus Diseases, Neoplasms, Glandular and Epithelial, Proto-Oncogene Proteins c-bcl-2, Tomography, X-Ray Computed, bcl-2-Associated X Protein
Background
Lacrimal gland pleomorphic adenoma (LGPA), also known as benign mixed lacrimal gland tumor, is the most common type of benign epithelial tumor of the lacrimal gland and accounts for approximately 50% of benign epithelial tumors of the lacrimal gland [1,2]. The main clinical manifestations of the disease include progressive and painless monocular protrusion, displacement, swelling or sagging of the upper eyelid, with or without binocular diplopia, and a palpable lacrimal gland mass located above the orbit [3]. Since the clinical symptoms and imaging findings are non-specific, definite diagnosis of LGPA is dependent on the histologic and immunohistochemical confirmation [4]. According to Lai et al, fine-needle aspiration biopsy is an effective approach for confirmation of diagnosis and guidance of therapy because no correlation between the procedure and recurrence or malignant transformation of LGPA has been observed [5]. Despite recent developments in conservative therapy, the first choice for the treatment of LGPA is surgery [6]. Wang reported that complete and timely surgical resection was required if the tumor was suspected or diagnosed as LGPA, because it is sufficient to minimize the risk of recurrence and can effectively arrest tumor development [7]. However, Behshad et al [8] suggested the tumor might seed into the other tissues when the tumor envelope containing the pleomorphic adenoma was compromised due to attempted biopsy or incomplete surgical excision, which could lead to recurrence and potential malignant transformation over time. Harrison et al, in a retrospective study, found that the recurrence rate after surgical resection was still up to 32%, and there was a high tendency to malignancy after relapse, which seriously affected patient quality of life and resulted in a poor prognosis [9].
Various hypotheses of LGPA tumorigenesis have been proposed in previous studies, including abnormal gene expression, disordered cell cycle regulation, invasive tumor growth, and abnormal cell proliferation [10–12]. Among them, the hypothesis of excessive cell proliferation has increasingly become the focus of occurrence and development of LGPA. Liao et al [13] found that survivin, a member of the inhibitor of apoptosis family, affected abnormal cell proliferation of LGPA. Nevertheless, the relationship between the abnormal cell proliferation and the balance of apoptosis and proliferation in LGPA needs further investigation.
Thus, we started from the balance between cell apoptosis and proliferation to verify the hypothesis. The objective of our study was to observe the pathological features of lacrimal gland lesions and the expression of bcl-2 and bax in lacrimal gland tissues and to preliminarily explore its possible pathogenesis.
Material and Methods
PATIENT SELECTION:
All patients were admitted to the Department of Ophthalmology of the Affiliated Hospital of Chengde Medical College and the Third Medical Center of the PLA General Hospital from April 2017 to November 2019. Among them, 19 patients with 19 eyes of LGPA patients were selected into an experimental group and 8 patients with normal lacrimal glands were selected into a control group. The 2 groups were compared in terms of age, sex, and eye type, and the differences were not statistically significant (
This study was approved by the Ethics Committee of the Affiliated Hospital of Chengde Medical College and the Third Medical Center of the PLA General Hospital (approval number: LL057). All patients provided signed informed consent to participate in this study.
METHODS:
HE staining was used to observe the morphological changes and pathological characteristics of the 2 groups of lacrimal gland tissue specimens. We cut the 2 groups of wax blocks into slices with a thickness of 2 μm. The slices were incubated at 63°C, dewaxed by xylene, dehydrated with concentration-gradient alcohol, washed with water and high-definition contrast solution, and stained with hematoxylin. Slices were then differentiated, washed with water and 85% and 95% alcohol, stained with eosin, dehydrated with absolute ethyl alcohol, transparentized with xylene, and then sealed. Under a light microscope (×100, ×200), the pathomorphological features of the lacrimal glands in the 2 groups were observed.
Immunohistochemical staining was performed to detect the expression of bcl-2 and bax in the lacrimal gland tissues of the 2 groups. The main reagents used were: primary antibody rabbit anti-human bcl-2 monoclonal antibody [anti-bcl-2 antibody (E17), number: ab32124, 1: 150 dilution] and rabbit anti-human bax monoclonal antibody [anti-bax antibody (E63), number: ab32503, 1: 150 dilution] produced by Abcam. The two-step kit is a universal SP kit (number: SP-9000) produced by Hebei Benyuan Biotechnology Co. Ltd.
Positive standard used was the expression of bax in human lung cancer tissue provided by Hebei Benyuan Biotechnology Company, which is recognized as the positive standard of bax, and the expression of bcl-2 in human B cell lymphoma tissue is recognized as the positive standard of bcl-2.
For the negative control, PBS buffer was used instead of the corresponding primary antibody to make a negative standard.
We cut the wax blocks of the 2 groups into 2 slices with the thickness of 2 μm and oven-baked them at 63°C, followed by dewaxing with xylene and dehydration with concentration-gradient alcohol. Endogenous peroxidase activity was eliminated using 3% H2O2. Samples were incubated at room temperature, we repaired antigen with microwave and sodium citrate buffer solution, followed by incubation at room temperature with 5–10% normal goat serum blocking solution. We added primary antibody (negative control with PBS buffer) dropwise and placed the solution in a 4°C refrigerator overnight. After washing in PBS buffer and dropwise addition of biotinylated goat anti-rabbit secondary antibody, we incubated the solution at room temperature, washed with PBS buffer and dropwise added horseradish enzyme-labeled streptavidin working solution. Incubation at room temperature was followed by washing with PBS buffer and developing color with DAB, and we stopped color development after staining. Samples were counterstained and mounted, and we observed the expression of bcl-2 and bax in the lacrimal glands of the 2 groups under a light microscope (×200, ×400).
Image-pro Plus 6.0 software was used to calculate the positive expression area/HP of the lacrimal gland tissues of the 2 groups. Two groups of specimens were randomly selected under the microscope (×400), and the average expression area of each field was statistically calculated.
Judgment criteria: According to the standards of bcl-2 and bax expression sites, bcl-2 was stained with cytoplasm as yellow or brown, and bax is stained in the same way after DAB color development.
STATISTICAL METHODS:
SPSS 22.0 software was used for statistical analysis. The ages of the 2 groups of patients followed a normal distribution, the data are expressed as mean±sd, and the 2 groups were compared using the independent-samples
Results
HE STAINING RESULTS OF LACRIMAL GLAND TISSUE IN THE 2 GROUPS:
Under a light microscope, it could be easily seen that the lacrimal glands in the control group were mainly composed of acinars and ducts, the acinars were mainly composed of serous gland cells and that the ductal epithelial cells were neatly arranged to form lumens of various sizes, with scattered lymphocytes and blood vessels. The basic lesions in the experimental group were the mixture of glandular epithelial cells, myoepithelial cells, and interstitium. Epithelial cells were arranged into glandular tubes, strips, and clumps. The size and shape of glandular ducts were different. The inner layer was cuboid or columnar cells, and the outer layer was spindle-shaped epithelial cells, which were distributed in a sheet-like or papillary nest-like way, and gradually transitioned into ovals or astrocytes. Mucinous components, hyaline-like tissues, cartilage-like tissues and scattered lymphocytes were visible in the interstitium. At the same time, it was found that the margins of the completely resected tumor were coated by the eosin-stained envelope with acellular structure, the thickness of the envelope was different, and there were signs of lymphocyte infiltration. Some glandular epithelial and myoepithelial cells grew outwards and invaded the outside of the capsule with clusters in a “sprouting” manner to differing degrees (Figure 1).
RESULTS OF IMMUNOHISTOCHEMICAL STAINING OF LACRIMAL GLAND TISSUE IN THE 2 GROUPS:
Immunohistochemical staining results showed the positive expression products of bcl-2 and bax were brown-yellow particles, mainly located in the cytoplasm of glandular epithelial and myoepithelial cells in normal lacrimal and diseased tissues. The expression of bcl-2 in the experimental group was obviously higher than that of the control group, and the difference between them was statistically significant (P<0.001) (Figure 2). The expression of bax in the experimental group was compared with that of the control group, but the difference between them was not statistically significant (P=0.25) (Figure 3). The bcl-2/bax ratio of the experimental group was significantly higher than the bcl-2/bax ratio of the control group, and the difference between them was statistically significant (P=0.01). We found no correlation between the expression of bcl-2 and bax (r=0.06, P=0.77). The detailed demographic and clinicopathological information of the two groups were listed in Table 1.
Discussion
Pleomorphic adenoma is a benign mixed tumor caused by abnormal proliferation of various tissue components such as glandular epithelial and myoepithelial cells, which mostly occurs in the parotid gland, submandibular gland, and lacrimal gland [14]. Because of the high biological behavior similarity to salivary gland polymorphic adenoma, LGPA is also classified as a borderline tumor [15]. Along with the continuous development in imaging and surgical technology, the rate of inadvertent biopsy of LGPA has dramatically reduced, and the early diagnosis and surgical resection have improved the prognosis of LGPA patients [7,16]. However, in a large longitudinal study, it was reported that the patients with complete follow-up had a 5-year recurrence rate of 3–32% and had the propensity to transform into carcinoma ex pleomorphic adenoma (ca-ex-PA) after recurrence. After malignant transformation occurs, the prognosis is poor, with a median survival of 3 years [2,9,17]. Therefore, the correlation between the biological behavior of LGPA and clinical outcome is an issue that deserves much attention.
It is generally believed that the pathological characteristics of tumors are closely related to the processes of tumor-initiation and progression and prognosis of disease [18]. Ahn et al performed a systematic observation and summarized the pathological features of biopsied lacrimal gland masses, providing a theoretical basis for identification, diagnosis, and management of lacrimal gland-occupying lesions [19]. Nevertheless, the biological behavior of LGPA has not been discussed on the basis of pathological analysis. In this study, we aimed to establish the relationship and found that the epithelial cells were arranged neatly and no pathological change was observed in the control group, while the tumor cellular density, morphology, and components of the stroma (such as mucinous components, hyaline-like tissues, and cartilage-like tissues) were significantly altered in the experimental group. The pathologic findings mainly resulted from the complex mixtures of different cell types, which were in agreement with MRI findings reported in a previous study [7]. In addition, the envelopes of LGPA were very thin (only tens of micrometers thick or even less, under a light microscope), let alone on visual observation (naked eye), which illustrated that in the diagnosis and treatment process of these patients, the grossly invisible envelopes were extremely easy to break and make the tumor cells spread to the surrounding normal tissues even if performed gently. These findings add to a growing body of evidence suggesting the importance of keeping an intact envelope during the process of clinical diagnosis and surgery. So, from this point of view, biopsy should not be recommended for those patients who are highly suspected of LGPA, which may contribute to reducing the risk of tumor recurrence and metastasis. These findings are consistent with prior studies [16,17,20]. We also observed that some glandular epithelial and myoepithelial cells grew outwards and invaded the outside of the envelope with clusters in a “sprouting” manner of varying degrees, and the tumor cells were also visible outside of the envelope, although microscopic examination showed the envelope was complete. From a pathological perspective, this intriguing finding adds a new dimension to our understanding of LGPA and helps to explain why LGPA easily relapses after surgical resection and is prone to malignant transformation after recurrence.
In addition, we further investigated the exact pathogenesis of LGPA. Several reports have shown that the factors regulating cell survival, apoptosis, growth arrest, and cell turnover rates are important contributors to the development, progression, and regression of cell growth, and the dysregulation can result in loss of control over proliferation and lead to tumor development [13,21,22]. However, little attention has been paid to the impact of cell apoptosis and proliferation on LGPA. The present study started from the imbalance between apoptosis and proliferation to explore the pathogenesis of LGPA. Bcl-2 family proteins play a key role in regulating the balance, among them, bcl-2 is a representative anti-apoptotic factor, which can block the release of cytochrome C, maintain mitochondrial membrane integrity, and promote cell proliferation, while bax, a classic pro-apoptotic factor, can cause mitochondrial membrane damage and accelerate cell apoptosis [23,24]. Our results suggest that the expression level of bcl-2 and the bcl-2/bax ratio in the lacrimal gland tissues of patients with LGPA were significantly elevated, while no difference was disclosed in the expression of bax compared with normal lacrimal gland tissues. The trend of bcl-2 and bcl-2/bax ratio was consistent with that of salivary gland pleomorphic adenoma, so it was speculated that the occurrence of LGPA was also closely related to cell over-proliferation caused by imbalance between apoptosis and proliferation [25,26]. When the balance in cells was upset, apoptosis was inhibited and cell proliferation was stimulated, leading to a number of uncontrollable cellular changes that culminated in tumor formation. Surprisingly, this study also found that there was no correlation between bcl-2 and bax, which suggests that the disruption of the balance might be mainly due to the increased expression of bcl-2, and the change of bax was a non-essential condition. When the expression of bcl-2 was upregulated and the bcl-2/bax ratio increased, bcl-2 formed a heterodimer with bax that decreased the sensitivity of lacrimal gland histiocytes to apoptosis-stimulating factors, and mitochondrial permeability transition pore opening was prolonged or remained in an “off” state, which induced a decrease in mitochondrial membrane permeability. In this case, cytochrome C in the mitochondrial intermembrane space could not bind to apoptotic protease activating factor 1 in the cytoplasm to form the apoptosome. Therefore, the activation pathway of cysteinyl aspartate specific proteinase-3 (caspase-3) was blocked, cell apoptosis of lacrimal tissues was inhibited, and the over-proliferation of tumor cells was induced, which all contributed to LGPA tumorigenesis.
Unfortunately, the cause and mechanism of the overexpression of bcl-2 in the lacrimal gland tissues of patients with LGPA have not been clearly reported in the literature. Ashkenazi et al [27]] found that the bcl-2 gene was located on chromosome 18q21 in diffuse large B cell lymphoma, multiple myeloma, and chronic lymphocytic leukemia, and participates in the process of chromosome translocation t (14; 18) (q32; q21), which leads to the overexpression of bcl-2 protein because the gene is located at the immunoglobulin heavy chain of chromosome 14q32. Further genomic chromosome detection and molecule studies in biology and other aspects are needed to confirm whether it occurs with the same chromosomal translocation in the development of LGPA to strike the balance.
Our study has certain limitations. First, due to the small size and non-homogeneity of the sample, there may be bias in observing the positive expression, so we need to expand the sample size in further research. Due to limitations arising from cost and availability, the investigations of related factors were conducted to utilize immunohistochemical methods rather than the more specific approaches such as in situ hybridization or polymerase chain reaction. This study still provides not only novel insights into the biological behavior of LGPA, but also a promising starting point for further investigations into another effective management methods other than surgical excision.
Conclusions
We observed that LGPA had a pathological change in the mixture of glandular epithelial cells, myoepithelial cells, and interstitial components, which might be related to the excessive proliferation of cells caused by the imbalance between apoptosis and proliferation. Further and more detailed clinical and experimental studies in a wider and deeper range are needed to verify our results.
Figures
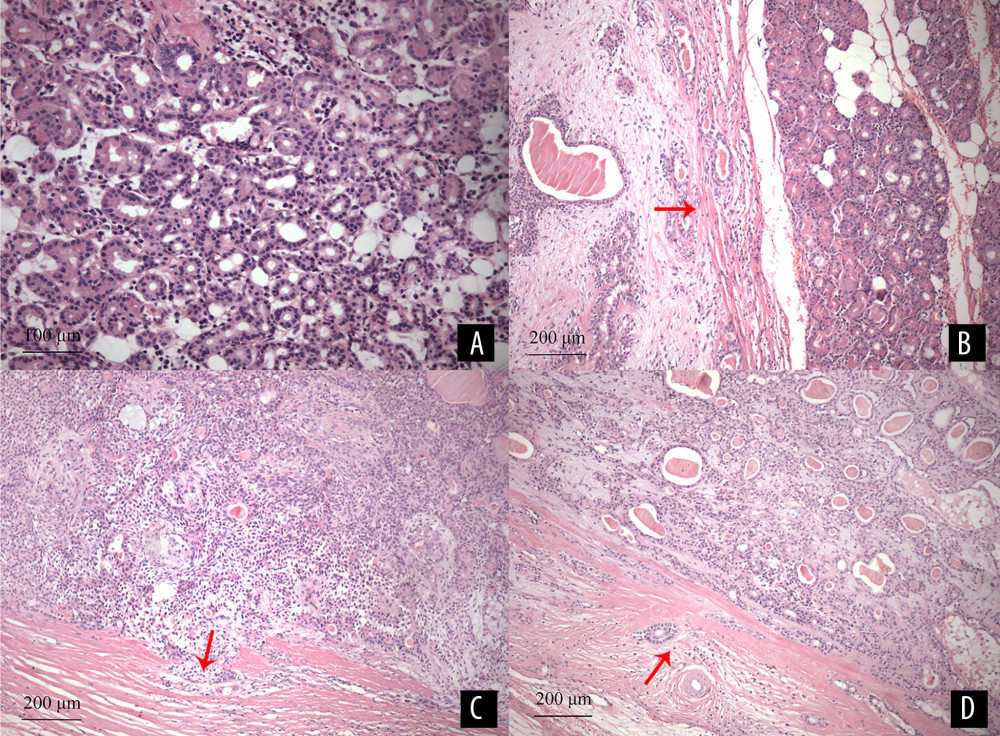 Figure 1. (A) Normal lacrimal glands are mainly composed of acinars and ducts. The acinars are composed of serous glandular cells, the ductal epithelial cells are neatly arranged to form lumens of various sizes, with scattered lymphocytes and blood vessels (HE staining×200). (B) The tumor tissues are a mixture of glandular epithelium, myoepithelial cells, and interstitium. The envelope structure of the tumor margin is loose, as indicated by the arrow. The remaining normal lacrimal gland tissues are visible on the right (HE staining ×100). (C) Some glandular epithelial and myoepithelial cells grew outwards and invaded the outside of the capsule with clusters in a “sprouting” manner, as indicated by the arrow (HE staining ×100). (D) the edge of the tumor envelope is roughly even, glandular epithelium, myoepithelial cells, and lymphocytes are scattered in the envelope, as indicated by the arrow (HE staining ×100).
Figure 1. (A) Normal lacrimal glands are mainly composed of acinars and ducts. The acinars are composed of serous glandular cells, the ductal epithelial cells are neatly arranged to form lumens of various sizes, with scattered lymphocytes and blood vessels (HE staining×200). (B) The tumor tissues are a mixture of glandular epithelium, myoepithelial cells, and interstitium. The envelope structure of the tumor margin is loose, as indicated by the arrow. The remaining normal lacrimal gland tissues are visible on the right (HE staining ×100). (C) Some glandular epithelial and myoepithelial cells grew outwards and invaded the outside of the capsule with clusters in a “sprouting” manner, as indicated by the arrow (HE staining ×100). (D) the edge of the tumor envelope is roughly even, glandular epithelium, myoepithelial cells, and lymphocytes are scattered in the envelope, as indicated by the arrow (HE staining ×100). 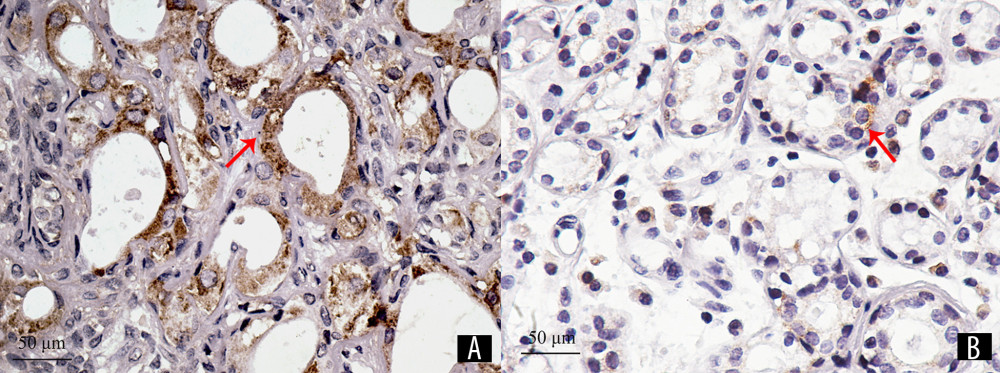 Figure 2. The positive expression products of bcl-2 are brown-yellow particles, mainly located in the cytoplasm of glandular epithelial and myoepithelial cells, as indicated by the arrow. The expression of bcl-2 in the experimental group (A) was 14928.76 pixels and 3975.40 pixels in the control group (B) (immunohistochemical staining×400).
Figure 2. The positive expression products of bcl-2 are brown-yellow particles, mainly located in the cytoplasm of glandular epithelial and myoepithelial cells, as indicated by the arrow. The expression of bcl-2 in the experimental group (A) was 14928.76 pixels and 3975.40 pixels in the control group (B) (immunohistochemical staining×400). 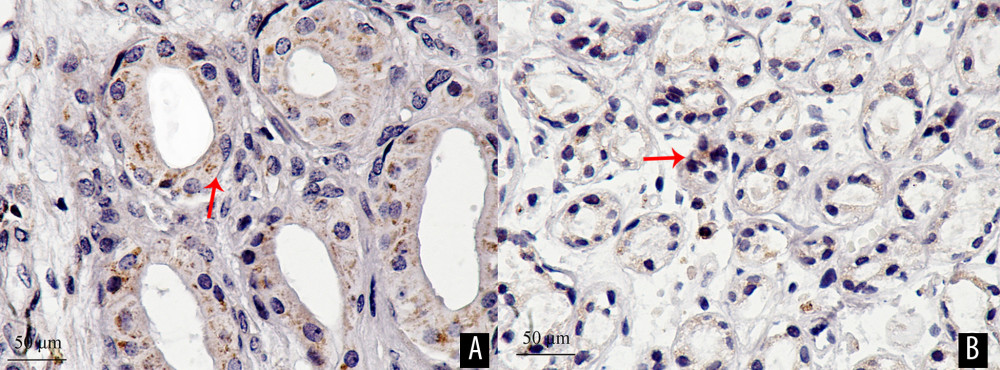 Figure 3. The positive expression products of bax are brown-yellow particles, mainly located in the cytoplasm of glandular epithelial and myoepithelial cells, as indicated by the arrow. The expression of bax in the experimental group (A) was 8364.82 pixels and 5149.36 pixels in the control group (B) (immunohistochemical staining ×400).
Figure 3. The positive expression products of bax are brown-yellow particles, mainly located in the cytoplasm of glandular epithelial and myoepithelial cells, as indicated by the arrow. The expression of bax in the experimental group (A) was 8364.82 pixels and 5149.36 pixels in the control group (B) (immunohistochemical staining ×400). References
1. Tao T, Yang J, Liu HClinical features and pathological analysis of lacrimal gland occupying lesions in 91 cases: Zhonghua Yan Ke Za Zhi, 2019; 55(11); 842-46 [in Chinese]
2. von Holstein SL, Coupland SE, Briscoe D, Epithelial tumours of the lacrimal gland: A clinical, histopathological, surgical and oncological survey: Acta Ophthalmologica, 2013; 91(3); 195-206
3. Venkatesulu BP, Pathy S, Vallonthaiel AG, Chawla B, Epithelial-myoepithelial carcinoma of lacrimal gland from an ex pleomorphic adenoma: BMJ Case Rep, 2015; 2015; bcr2015210795
4. Clarós P, Choffor-Nchinda E, Lopez-Fortuny M, Lacrimal gland pleomorphic adenoma. A review of 52 cases, 15-year experience: Acta Otolaryngol, 2019; 139(1); 100-4
5. Lai T, Prabhakaran VC, Malhotra R, Selva D, Pleomorphic adenoma of the lacrimal gland: Is there a role for biopsy?: Eye, 2009; 23(1); 2-6
6. Schittkowski MP, Storch MWDiseases of the lacrimal gland: Klin Monbl Augenheild, 2020; 237(5); 703-23 [in German]
7. Wang Y, Song L, Guo J, Xian J, Value of quantitative multiparametric MRI in differentiating pleomorphic adenomas from malignant epithelial tumors in lacrimal gland: Neuroradiology, 2020; 62(9); 1141-47
8. Behshad S, Sethi P, Valenzuela AA, The malignancy masquerader: Hyperostosis and bone marrow hypertrophy after pleomorphic adenoma removal: Can J Ophthalmol, 2015; 50(6); e104-6
9. Harrison W, Pittman P, Cummings T, Pleomorphic adenoma of the lacrimal gland: A review with updates on malignant transformation and molecular genetics: Saudi J Ophthalmol, 2018; 32(1); 13-16
10. Andreasen S, von Holstein SL, Homøe P, Heegaard S, Recurrent rearrangements of the PLAG1 and HMGA2 genes in lacrimal gland pleomorphic adenoma and carcinoma ex pleomorphic adenoma: Acta Ophthalmol, 2018; 96(7); e768-71
11. Zhang P, Tang LJ, Gao HH, Immunohistochemical features of carcinoma ex pleomorphic adenoma and pleomorphic adenoma in the lacrimal gland: Int J Ophthalmol, 2019; 12(8); 1238-42
12. Andreasen S, Heegaard S, Grauslund M, Homøe P, The interleukin-6/Janus kinase/STAT3 pathway in pleomorphic adenoma and carcinoma ex pleomorphic adenoma of the lacrimal gland: Acta Ophthalmol, 2016; 94(8); 798-804
13. Liao Y, Zeng H, Wang X, Expression patterns and prognostic significance of inhibitor of apoptosis proteins in adenoid cystic carcinoma and pleomorphic adenoma of lachrymal gland: Exp Eye Res, 2009; 88(1); 4-11
14. Verma V, Mendenhall WM, Werning JW, Polymorphous low-grade adenocarcinoma of the head and neck: Am J Clin Oncol, 2014; 37(6); 624-26
15. von Holstein SL, Tumours of the lacrimal gland. Epidemiological, clinical and genetic characteristics: Acta Ophthalmol, 2013; 91; 1-28 Thesis 6
16. Vahdani K, Rose GE, Palpebral pleomorphic adenomas of the lacrimal gland: Ophthalmic Plast Reconstr Surg, 2020 [Online ahead of print]
17. Xiao LHThe importance for improving the cure rate of lacrimal gland benign pleomorphic adenoma: Zhonghua Yan Ke Za Zhi, 2016; 52(4); 241-43 [in Chinese]
18. Nagendran S, Alsamnan M, Strianese D, Malhotra R, Ectopic lacrimal gland tissue: A systematic review: Ophthalmic Plast Reconstr Surg, 2020; 36(6); 540-44
19. Ahn C, Kang S, Sa HS, Clinicopathologic features of biopsied lacrimal gland masses in 95 Korean patients: Graefes Arch Clin Exp Ophthalmol, 2019; 257(7); 1527-33
20. von Sonnleithner C, Zorn M, Bertelmann EBenign neoplasms of the orbit: Klin Monbl Augenheilkde, 2019; 236(7); 929-47 [in German]
21. Batinac T, Zamolo G, Ruzić A, Persić V, Apoptosis in skin cancer development and regression: Coll Antropol, 2007; 31(Suppl 1); 23-28
22. Gallaher JA, Brown JS, Anderson ARA, The impact of proliferation-migration tradeoffs on phenotypic evolution in cancer: Sci Rep, 2019; 9(1); 2425
23. Zhang X, Liu X, Zhou D, Zheng G, Targeting anti-apoptotic BCL-2 family proteins for cancer treatment: Future Med Chem, 2020; 12(7); 563-65
24. Knight T, Luedtke D, Edwards H, A delicate balance – The BCL-2 family and its role in apoptosis, oncogenesis, and cancer therapeutics: Biochem Pharmacol, 2019; 162; 250-61
25. Siqueira EC, Souza FT, Diniz MG, Hsp27 (HSPB1) differential expression in normal salivary glands and pleomorphic adenomas and association with an increased Bcl2/Bax ratio: Tumour Biol, 2015; 36(1); 213-17
26. Ferreira JC, Morais MO, Elias MR, Pleomorphic adenoma of oral minor salivary glands. An investigation of its neoplastic potential based on apoptosis, mucosecretory activity and cellular proliferation: Arch Oral Biol, 2014; 59(6); 578-85
27. Ashkenazi A, Fairbrother WJ, Leverson JD, Souers AJ, From basic apoptosis discoveries to advanced selective BCL-2 family inhibitors: Nat Rev Drug Discov, 2017; 16(4); 273-84
Figures
Figure 1. (A) Normal lacrimal glands are mainly composed of acinars and ducts. The acinars are composed of serous glandular cells, the ductal epithelial cells are neatly arranged to form lumens of various sizes, with scattered lymphocytes and blood vessels (HE staining×200). (B) The tumor tissues are a mixture of glandular epithelium, myoepithelial cells, and interstitium. The envelope structure of the tumor margin is loose, as indicated by the arrow. The remaining normal lacrimal gland tissues are visible on the right (HE staining ×100). (C) Some glandular epithelial and myoepithelial cells grew outwards and invaded the outside of the capsule with clusters in a “sprouting” manner, as indicated by the arrow (HE staining ×100). (D) the edge of the tumor envelope is roughly even, glandular epithelium, myoepithelial cells, and lymphocytes are scattered in the envelope, as indicated by the arrow (HE staining ×100).Figure 2. The positive expression products of bcl-2 are brown-yellow particles, mainly located in the cytoplasm of glandular epithelial and myoepithelial cells, as indicated by the arrow. The expression of bcl-2 in the experimental group (A) was 14928.76 pixels and 3975.40 pixels in the control group (B) (immunohistochemical staining×400).Figure 3. The positive expression products of bax are brown-yellow particles, mainly located in the cytoplasm of glandular epithelial and myoepithelial cells, as indicated by the arrow. The expression of bax in the experimental group (A) was 8364.82 pixels and 5149.36 pixels in the control group (B) (immunohistochemical staining ×400). Tables
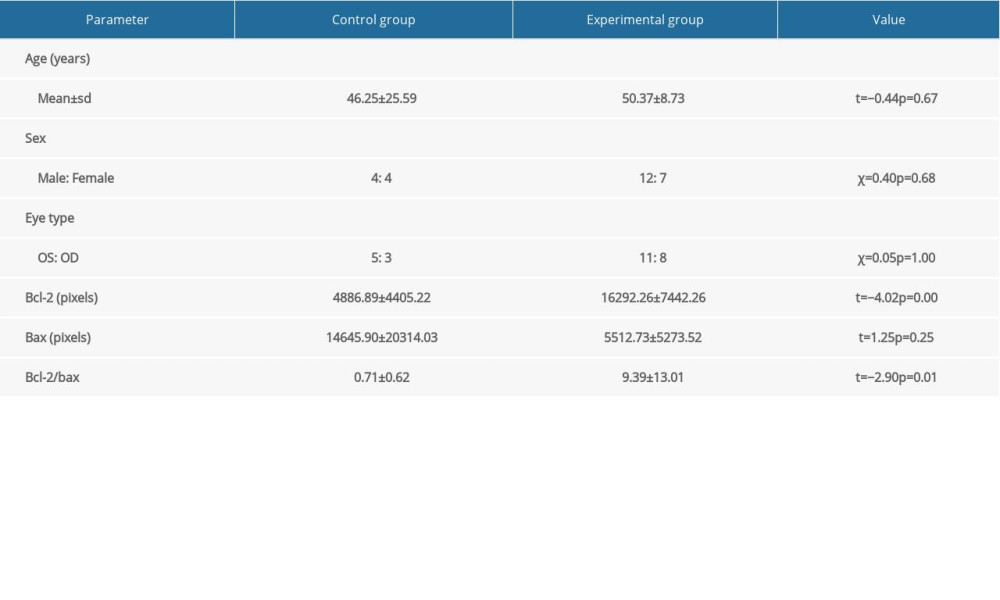 Table 1. Characteristics of patients and summary of the experimental and control groups. P value refers to comparisons between 2 groups. OS means oculus sinister, and OD means oculus dexter.Table 1. Characteristics of patients and summary of the experimental and control groups. P value refers to comparisons between 2 groups. OS means oculus sinister, and OD means oculus dexter.
Table 1. Characteristics of patients and summary of the experimental and control groups. P value refers to comparisons between 2 groups. OS means oculus sinister, and OD means oculus dexter.Table 1. Characteristics of patients and summary of the experimental and control groups. P value refers to comparisons between 2 groups. OS means oculus sinister, and OD means oculus dexter. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387