11 February 2021: Clinical Research
Effect of I Therapy on Complete Blood Count in Patients with Differentiated Thyroid Cancer
Zhongying Rui1CDEF, Ruixin Wu1BCD, Wei Zheng1ADG*, Xuan Wang1BDF, Zhaowei Meng1AF, Jian Tan1AFDOI: 10.12659/MSM.929590
Med Sci Monit 2021; 27:e929590






Abstract
BACKGROUND: The aim of this study was to investigate the effects of ¹³¹I therapy on complete blood count (CBC) in patients with differentiated thyroid cancer (DTC).
MATERIAL AND METHODS: We analyzed CBC in 542 patients with DTC who were grouped according to treatment cycles and cumulative dose and then subdivided by sex and age. The effects of ¹³¹I therapy among the different groups and subgroups were analyzed.
RESULTS: After sorting patients by treatment cycles and doses, ¹³¹I therapy was found to have different effects on CBC depending on patient sex and age. The effect on white blood cell (WBC) counts persisted longer in women, while increases in hemoglobin (Hb) were more significant in men. The influence on red blood cell (RBC) counts was short-lived in patients aged 45 to 54 years. Monocyte counts were significantly decreased only in patients aged 55 years and older who had undergone 3 or 4 treatment cycles. In men, CBC was more affected by cumulative dose. ¹³¹I therapy only influenced platelet and monocyte counts in patients aged 55 years or older. Hb was significantly decreased and increased in the high- and low-dose groups, respectively. No significant complications were observed during follow-up.
CONCLUSIONS: ¹³¹I therapy had a greater impact on WBC counts in women, while changes in RBC counts and Hb were more obvious in men. During ¹³¹I therapy, clinicians should pay attention to different CBC indicators based on a patient’s sex and age, but risks associated with an altered CBC are unlikely to outweigh the benefits of 131I. The results of the present study may help alleviate the concerns of a large proportion of patients with DTC and their families about the effects of ¹³¹I therapy on CBC.
Keywords: ABO Blood-Group System, Dose Fractionation, Iodine, Adolescent, Age Factors, Bone Marrow, Dose-Response Relationship, Radiation, Follow-Up Studies, Hemoglobins, Iodine Radioisotopes, Leukocyte Count, Radiopharmaceuticals, Radiotherapy Dosage, Reference Values, Risk Factors, Sex Factors, Time Factors, young adult
Background
The incidence of thyroid cancer has rapidly increased worldwide in recent decades [1–4]. Differentiated thyroid cancer (DTC), which includes papillary and follicular cancer, comprises the vast majority (>90%) of all thyroid cancers [5]. 131I therapy is a conventional method of treating DTC after thyroidectomy that can successfully ablate remnant or recurrent thyroid carcinoma cells in both primary and metastatic lesions [5, 6]. Although 131I is widely accepted to be safe, it still has adverse effects that negatively affect patient quality of life, although they are rarely life-threatening [7]. They include transient neck pain and edema, gastritis, radiation thyroiditis [7], salivary gland dysfunction [8], and nasolacrimal obstruction [9]. Knowledge about the adverse effects of 131I is essential for both considering preventative measures before and managing complications after treatment.
131I therapy also leads to bone marrow toxicity and can cause bone marrow dysfunction [10]. Some studies have shown that both a single dose and multiple doses of 131I therapy can change complete blood count (CBC) [11,12]. However, the influence of 131I therapy on CBC in patients with DTC is debatable. A large proportion of patients with DTC are concerned about the effects of bone marrow toxicity. However, few studies have investigated the influences of cumulative doses and treatment cycles of 131I and analyzed the influence of age and sex on CBC. Therefore, we evaluated the effects of 131I therapy on CBC in patients grouped by treatment cycles and cumulative doses, with a focus on sex and age.
Material and Methods
PATIENTS:
We reviewed the clinical records of patients with DTC who were treated in the Nuclear Medicine Department of Tianjin Medical University General Hospital between January 2009 and June 2018. All patients underwent total thyroidectomy and dissection of central lymph nodes and lymph nodes on the affected side and then were given at least 1 cycle of postoperative 131I therapy in our department. To avoid the influence of confounding factors, patients were excluded from the study if they: (1) had taken any medications known to affect CBC; (2) were known to have any baseline hematologic diseases or any abnormalities in CBC prior to initial 131I therapy; (3) received external beam radiation therapy and/or chemotherapy before or during the treatments; (4) had postoperative blood loss that impacted CBC; or (5) received more than 4 cycles of 131I therapy, because the size of our cohort was limited.
METHODS:
All patients underwent traditional thyroid hormone withdrawal preparation before 131I therapy. Briefly, they were instructed to follow a low-iodine diet 1 month before, during, and 1 month after 131I therapy. Patients were taken off levothyroxine 2 to 4 weeks before starting 131I therapy. 131I was taken orally. With respect to the dose, 3700 MBq was recommended for patients receiving it as remnant ablative therapy, 3700 to 5550 MBq for patients with cervical lymph node metastasis (LNM) and/or extra-thyroid extension (adjuvant therapy), and 5550 to 7400 MBq generally was recommended for distant metastasis (therapeutic therapy). Diagnostic 131I whole-body scintigraphy (Dx-WBS) was performed 2 to 7 days later with a dual-detector single-photon emission computed tomography/computed tomography (SPECT/CT) machine with high-energy collimators. Otherwise, neck and chest CT or 18F-fluorodeoxyglucose positron emission tomography/CT (18F-FDG PET/CT) was used to evaluate the patients’ physical condition and detect potential metastases. Whole-body radioactivity after 131I therapy was monitored once daily during hospitalization. Patients were advised to limit close contact with relatives for at least 7 days after hospital discharge. A therapeutic and follow-up recommendation was given to each patient. According to the 2015 American Thyroid Association (ATA) [13], based on the results of serological examination (sTg and stimulated thyroglobulin antibodies [sTgAb]) and imaging such as neck ultrasound, Dx-WBS, chest CT, and PET/CT, treatment responses were divided by efficacy into 4 categories: excellent response (ER), indeterminate response (IDR), biochemical incomplete response, and structural incomplete response. Approximately 4 to 6 months after each 131I treatment, the patients returned to the outpatient department for evaluation. If their treatment response was not ER or IDR and their lesions had adequately absorbed the 131I, continued 131I therapy for 4 to 6 months was considered, following Chinese guidelines [14], after the initial course. The cumulative dose was the sum of each 131I dose. The charts for all patients were reviewed and analyzed retrospectively.
An automated CBC was obtained within 3 days before 131I therapy and retesting was delayed for 4 to 6 months after each treatment so that the results would not reflect the transient influence of 131I on bone marrow. All serum blood tests were performed in the hematology laboratory of Tianjin Medical University General Hospital using an automated CBC analyzer (Sysmex xn-2000, Sysmex Corporation, Kobe, Japan).
The normal ranges for hemoglobin (Hb) are 130 to 175 g/dL and 115 to 150 g/L in men and women, respectively. The normal ranges for red blood cells (RBCs) are 4.3 to 5.8×1012 cells/L and 3.8 to 5.1×1012 cells/L in men and women, respectively. For both sexes, the normal ranges for white blood cells (WBCs), platelets (PLTs), neutrophils, lymphocytes, and monocytes are 3.5 to 9.5×109 cells/L, 125 to 350×109 cells/L, 1.8 to 6.3×109 cells/L, 1.1 to 3.2×109 cells/L, and 0.12 to 0.80×109 cells/L, respectively.
ETHICS APPROVAL:
The ethical, methodological, and protocol aspects of this investigation were approved by the Institutional Review Board and Ethics Committee of Tianjin Medical University General Hospital. All methods used in the current study were carried out in accordance with the relevant guidelines and regulations. (Ethical. No. IRB2020-WZ-165).
STATISTICAL ANALYSIS:
Quantitative data are expressed as means±standard deviations (SDs). Normal distribution of quantitative data was tested with a Q-Q plot. Quantitative data with normal distribution were analyzed with a paired
Results
PATIENT GROUPS:
The present study enrolled 542 patients with a mean age of 46.64±12.77 (range: 14 to 78) years. The patients included 152 men with a mean age of 45.98±13.12 years (range: 19 to 78 years) and 390 women with a mean age of 46.91±12.63 years (range: 14 to 76 years). The patients were divided into 4 groups according to treatment cycles (1; n=416, 2; n=83, 3; n=23, and 4; n=20) and 3 groups according to cumulative dose (low-dose; ≤5550 MBq, n=417) (medium-dose; 5551 to 11 100 MBq, n=92) (high-dose; >11 100 MBq, n=33). The patient groups were then subdivided into subgroups according to sex (male and female) and age (<45 years, 45 to 54 years, and ≥55 years).
BASELINE PATIENT CHARACTERISTICS:
Baseline characteristics for and groupings of the patients are summarized in Table 1. Univariate analysis showed that thyroid stimulating hormone (TSH) status did not influence CBC (P>0.05). Before 131I therapy, there were no significant differences in CBC among the different treatment cycle groups or the different cumulative dose groups.
:
CBC data before and after 131I therapy are shown in Table 2. The mean CBC remained within the normal reference range during treatment. There were significant fluctuations in the mean levels of WBCs, RBCs, Hb, PLTs, lymphocytes, and monocytes.
There were significant decreases in WBC and PLT counts after the first (
WBC counts were significantly decreased in the low- and medium-dose groups (
:
Table 3 shows the influence of the number of treatment cycles and cumulative 131I dose on CBC in different sex.
Men had significantly decreased WBC counts after the second cycle (
In men, there were significant decreases in lymphocyte counts in the low- and medium-dose groups (all
:
Table 4 shows the influence of the number of treatment cycles and cumulative 131I dosage on CBC in patients of different ages.
In patients younger than age 45 years, WBC counts were significantly decreased after the first 2 cycles (
In patients younger than age 45 years, WBC counts were significantly decreased in the low- and medium-dose groups (
Patients treated with 4 cycles of 131I were analyzed independently. In this group, there were significant fluctuations in lymphocyte and monocyte counts (P=0.032 and P=0.002, respectively). Lymphocyte counts consistently declined from the first to the third 131I cycle and then increased after the fourth cycle (Figure 1). The only statistically significant decrease compared with the baseline lymphocyte value occurred after the third 131I cycle (1.44±0.43 vs 1.90±0.63, P=0.001). Monocyte counts decreased after the first cycle and then gradually increased after the third cycle (Figure 2). There were no statistically significant differences between any post-treatment and baseline values. However, the final 2 post-treatment values were higher than the value after the first cycle (0.30±0.10 and 0.31±0.09 vs 0.22±0.05, all P=0.001). Data from patients who received >11 000 MBq of 131I were analyzed independently and they revealed a significant fluctuation only in monocyte counts (P=0.027). As shown in Figure 3, monocyte counts decreased after patients had received ≤5550 MBq of 131I and then gradually increased after >5550 MBq had been received. However, there were no statistically significant differences between the post-treatment and baseline values. Finally, it was noteworthy that monocyte counts were higher in patients who received >11 100 MBq of 131I than in those who received ≤5550 MBq (0.30±0.09 vs 0.22±0.05, P=0.003) (Figure 3).
Discussion
Thyroid cancer is becoming prevalent worldwide. Most patients with DTC have an excellent prognosis; 5- and 10-year relative survival rates are between 90% and 95% [15]. However, recurrence occurs in 5% to 20% of patients [16]. 131I therapy is standard for ablation of remnant thyroid tissue and iodine-avid metastases after surgery in patients with intermediate- and high-risk DTC [5]. Thereafter, appropriate TSH suppression therapy should be given routinely. As a systemic treatment, 131I has the major advantage of reducing the risk of local recurrence as well as distant metastasis [17]. It can also serve as a diagnostic tool, enabling visualization of normal and carcinomatous thyroid tissue by means of whole-body scintigraphy [6]. However, 131I therapy can cause long-term or temporary adverse effects such as pulmonary fibrosis and myelosuppression [7,10,18,19]. Hematological toxicity is a common adverse effect of 131I therapy [7]. A study [20] showed that the kinetics of 131I incorporation induced DNA double-strand breaks in blood lymphocytes during radioiodine therapy as a function of the dose absorbed by the blood. However, a study by Zhang et al [21] showed that 131I therapy can contribute to the recovery of patients with DTC by restoring the balance of T helper 17, T cytotoxic 17, and regulatory T cells. In the present study, we documented the effects of 131I therapy on CBC in patients with DTC. We were able to make this clinical observation because of the relatively large number of patients with DTC treated at our institution who undergo regular hematologic monitoring.
A study by Molinaro et al [22] showed a statistically significant decline in total WBC and PLT counts 1 year after treatment compared with baseline CBC before 131I therapy. A study by Padovani et al [23] showed a statistically significant decrease in Hb and PLT count 1 year after treatment in 50 patients who received ≥9250 MBq of 131I. A clinical study by Hu et al [11] also showed that administration of approximately 3700 MBq of 131I was associated with significant declines in WBC, PLT, and lymphocyte counts that persisted for at least 6 months after ablation. Tofani et al [24] showed that 10 patients (group A) who underwent whole-body scintigraphy with 185 MBq of 131I only had a reduction in natural killer cells on Days 7 and 15. Meanwhile, another 10 patients (group B) received 3700 MBq of 131I and showed a delayed reduction in total lymphocyte counts on Days 15, 30, and 60. Our study had a similar conclusion, in that the mean levels of WBCs, PLTs, lymphocytes, and monocytes declined over the course of 131I treatment. In contrast, we found significant increases in RBC counts and Hb. However, the studies by the other investigators that were discussed previously only assessed the effect of a single 131I cycle on CBC. Prinsen et al [10] showed that PLT and WBC counts were transiently decreased after repeated 131I therapy in a population with DTC that had abnormal CBCs. Keldse et al [12] showed, in 24 patients, that compared with pretreatment levels, the median WBC count declined to 78% and the median PLT count declined to 69% after 4 treatment cycles. The study by Prinsen et al [10] demonstrated that post-treatment PLT and WBC counts were transiently decreased compared with pretreatment values in the general population with DTC and that cumulative 131I dose was independently associated with thrombocytopenia. Probst et al [25] reported on a case of severe myelosuppression requiring hospitalization and transfusion support in an otherwise well young woman who had received 6475 MBq of 131I for low-volume micronodular lung disease 1 month before and had a cumulative lifetime dosage of 21 275 MBq. Our study showed that the number of treatment cycles and cumulative doses were associated with significant declines in WBC, PLT, lymphocyte, and monocyte counts as well as significant increases in RBC counts and Hb. However, none of the patients required hospitalization because of myelosuppression.
In the present study, the post-treatment data showed slightly increased RBC counts and Hb levels compared with the pretreatment data. A possible explanation for this phenomenon could be that thyroid hormones have important effects on RBCs in humans [26]. Meanwhile, some studies have reported that low-dose radiation can have a hermetic effect on the hematopoietic system. Total-body low-dose radiation can modulate the capacity of bone marrow cells to differentiate into dendritic cells [27]. Vrndic et al [28] concluded that 131I led to a reduction in all peripheral blood cells (PBCs) and that the decrease in B cells was directly correlated with PBC apoptosis. Radiation damage to B cells also has been shown to lead to elimination of the cells by apoptosis.
In the present study, significant sex-based differences were found in WBC counts, PLT counts, Hb, and monocyte counts in patients who underwent different numbers of treatment cycles. We found that the influences of the number of treatment cycles on WBC counts persisted longer in women than in men. Furthermore, the number of treatment cycles had an effect only on PLT and monocyte counts only in women. In men, the increase in Hb was more significant. Significant sex-based differences were found in WBC, PLT, and RBC counts, and Hb in the groups that received different cumulative doses. The influence of cumulative dose on WBC and PLT counts was only seen in women. In men, the increases in RBC counts in the medium-dose group and in Hb in the low- and high-dose groups were more significant in men than in women. However, our findings were different than those from the study by Prinsen et al [10]. This may be because the patients were from different regions or because the follow-up times in the studies differed. Further research will be needed to understand the influence of sex on hematological characteristics in patients who receive 131I. Therefore, during the course of 131I therapy, clinicians should anticipate decreased levels of WBCs, PLTs, and monocytes in women and increased levels of RBCs and Hb in men.
Because it represents the median age of most large cohorts upon which staging systems are based, an age cutoff of 45 years for DTC has been used in most major thyroid cancer staging systems for many years. The TNM (tumor, node, metastasis) staging system for thyroid cancer, for example, has been in existence for 55 years (AJCC 8th Edition). In our study, we divided patients with DTC into 3 subgroups according to age (<45, 45 to 54, and ≥55 years). After not only accounting for different numbers of treatment cycles but also different cumulative doses, we found that the duration of increased RBC counts was minimal in patients aged 45 to 54 years, decreases in PLT and monocyte counts were seen only in patients older than age 55 years, and the decrease in lymphocyte counts was minimal in patients younger than age 45 years. These findings were similar to those of Prinsen et al [10]. It is possible that slower metabolism associated with increased age allows the radiopharmaceutical to remain in the body longer. Therefore, during the course of 131I therapy, clinicians should pay more attention to elderly patients who receive ≥11 100 MBq of 131I.
A previous study showed that TSH administration increased the expression of the proatherogenic monocyte gene [29]. Van der Weerd et al [30] showed that TSH acts as a previously unrecognized growth factor for developing T cells, with potential clinical use for enhancing thymic output, and thereby, the functional T-cell repertoire in the periphery. Our univariate analysis showed that TSH status had no influence on CBC. Further research is needed to clarify these data, perhaps by simply increasing the sample size.
This analysis has some limitations. First, the present study was cross-sectional. Second, because of the short follow-up time, the cohort of patients who received ≥11 100 MBq of 131I was small. Thus, future prospective studies are needed with larger cohorts and longer follow-up.
Conclusions
The number of treatment cycles and the cumulative dose of 131I therapy influenced CBC but the indictors were still within the normal range. Different numbers of treatment cycles and the cumulative dose of 131I therapy had differential impacts on CBC depending upon patient sex and age. During treatment, clinicians should pay attention to different CBC indicators in patients with DTC according to their sex and age. Because the benefits of 131I therapy in intermediate- and high-risk patients with DTC outweigh the potential hematological risks, there is no need to reduce the number of treatment cycles or the cumulative dosage of 131I. The results from the present study could help alleviate the concerns that a large proportion of patients with DTC and their families have about the effects of 131I therapy on CBC. 131I therapy also can lead to a downward trend in counts of some cells. Therefore, in patients who have decreased counts before 131I therapy, we suggest that the treatment be delayed until the counts have returned to normal.
Figures
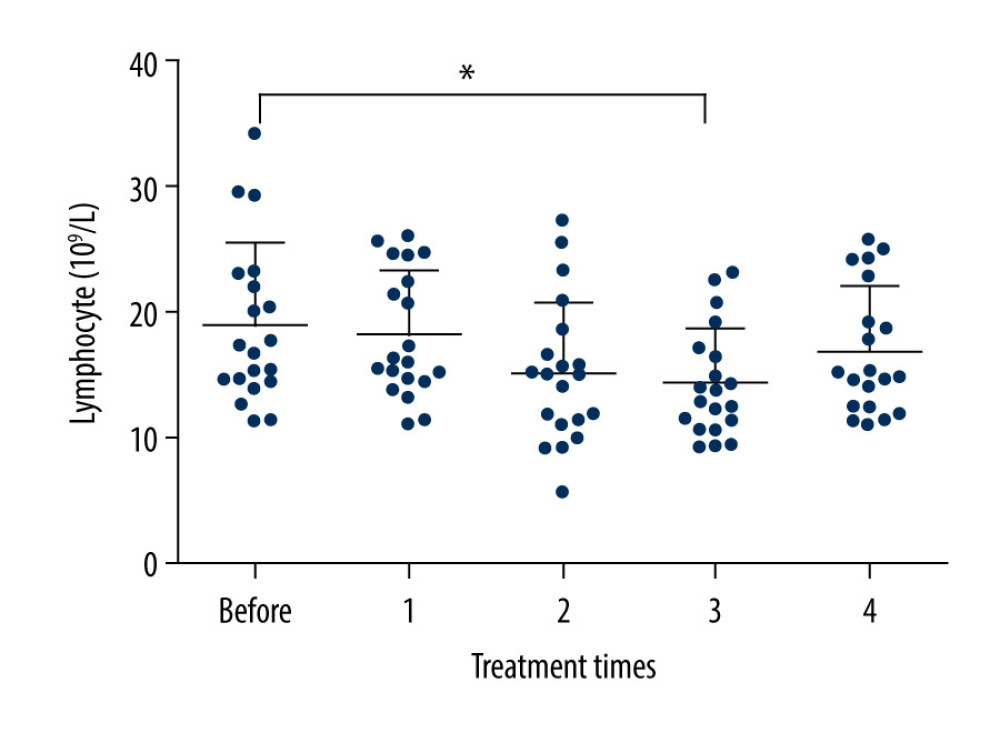 Figure 1. Changes in lymphocyte counts after 131I treatment cycles. The counts consistently declined from the first to the third 131I cycles and then increased after the fourth 131I therapy. The decrease that was statistically significant compared with the baseline lymphocyte count occurred after the third 131I cycle (1.44±0.43 vs 1.90±0.63, P=0.001).
Figure 1. Changes in lymphocyte counts after 131I treatment cycles. The counts consistently declined from the first to the third 131I cycles and then increased after the fourth 131I therapy. The decrease that was statistically significant compared with the baseline lymphocyte count occurred after the third 131I cycle (1.44±0.43 vs 1.90±0.63, P=0.001). 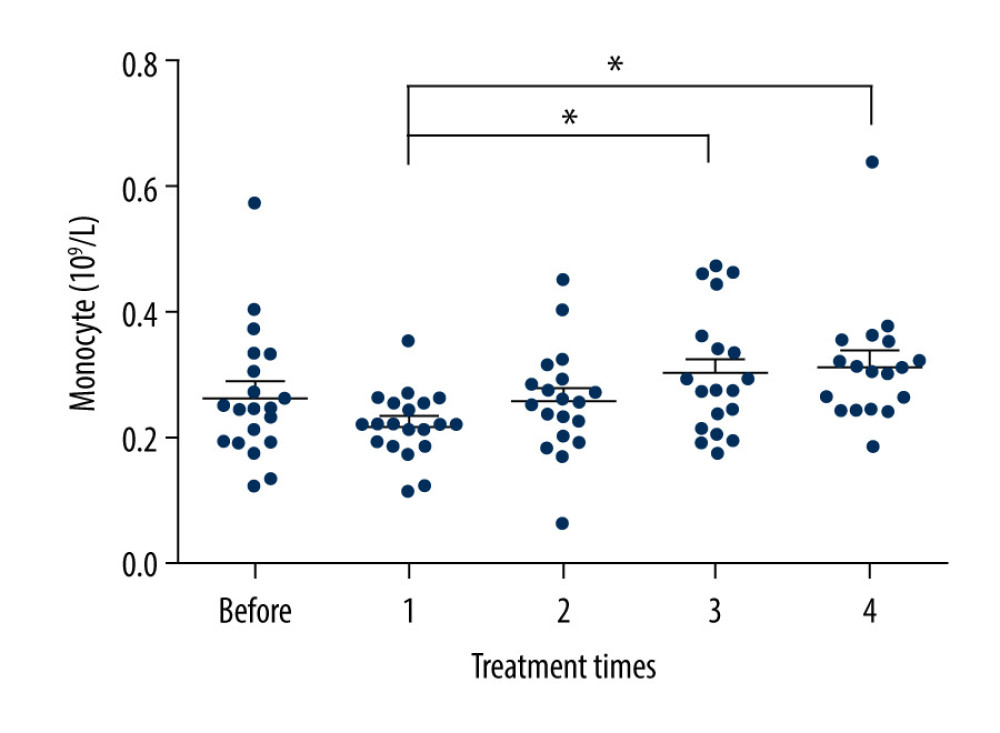 Figure 2. Changes in monocyte counts after 131I treatment cycles. The number of monocytes decreased after the first treatment and then gradually increased after the last 3 treatments. While the differences between post-treatment and baseline values were not significant, the last 2 post-treatment values were higher than the value after the first treatment (0.30±0.10 and 0.31±0.09 vs 0.22±0.05, both P=0.001).
Figure 2. Changes in monocyte counts after 131I treatment cycles. The number of monocytes decreased after the first treatment and then gradually increased after the last 3 treatments. While the differences between post-treatment and baseline values were not significant, the last 2 post-treatment values were higher than the value after the first treatment (0.30±0.10 and 0.31±0.09 vs 0.22±0.05, both P=0.001). 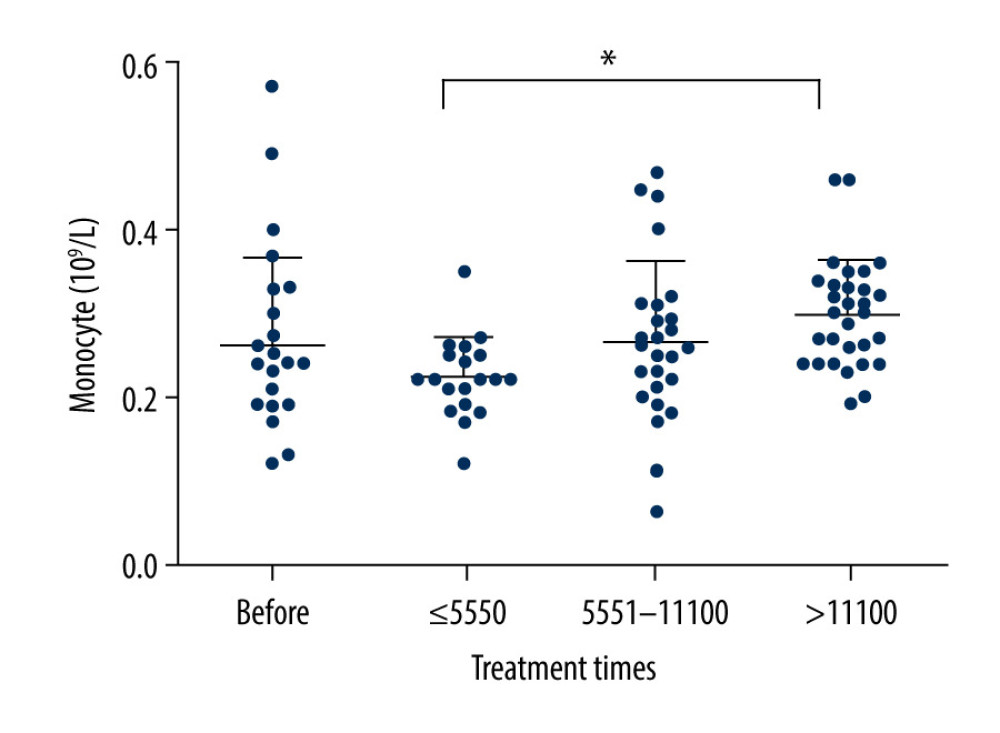 Figure 3. Changes in monocyte counts after cumulative doses of 131I therapy. The number of monocytes decreased when patients had received ≤5550 MBq of 131I and then gradually increased after patients had received >5550 MBq of 131I. While there were no statistically significant differences between post-treatment and baseline values, patients who received >11 100 MBq of 131I had higher monocyte counts than those who received ≤5550 MBq of 131I (0.30±0.09 vs 0.22±0.05, P=0.003).
Figure 3. Changes in monocyte counts after cumulative doses of 131I therapy. The number of monocytes decreased when patients had received ≤5550 MBq of 131I and then gradually increased after patients had received >5550 MBq of 131I. While there were no statistically significant differences between post-treatment and baseline values, patients who received >11 100 MBq of 131I had higher monocyte counts than those who received ≤5550 MBq of 131I (0.30±0.09 vs 0.22±0.05, P=0.003). Tables
Table 1. Patient groupings.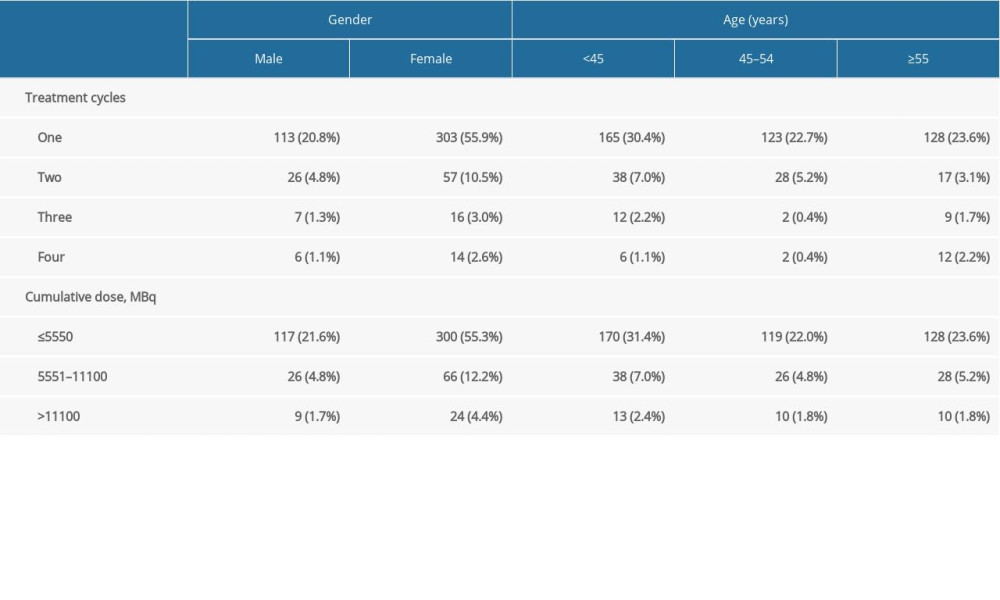 Table 2. CBC data before and after 131I therapy according to the number of treatment cycles and cumulative dose.
Table 2. CBC data before and after 131I therapy according to the number of treatment cycles and cumulative dose.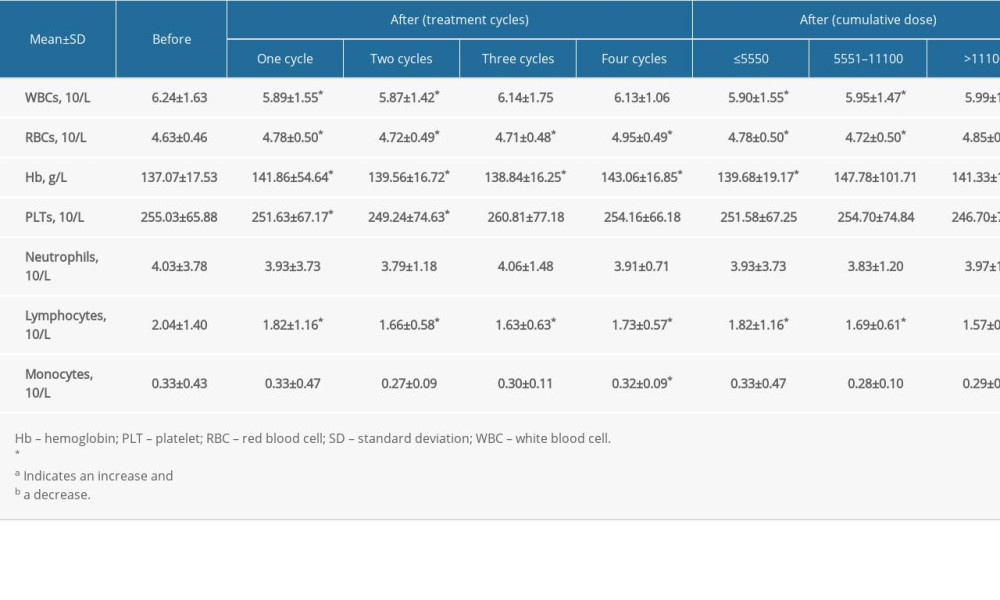 Table 3. CBC data before and after 131I therapy by gender and according to the number of treatment cycles and cumulative dose.
Table 3. CBC data before and after 131I therapy by gender and according to the number of treatment cycles and cumulative dose.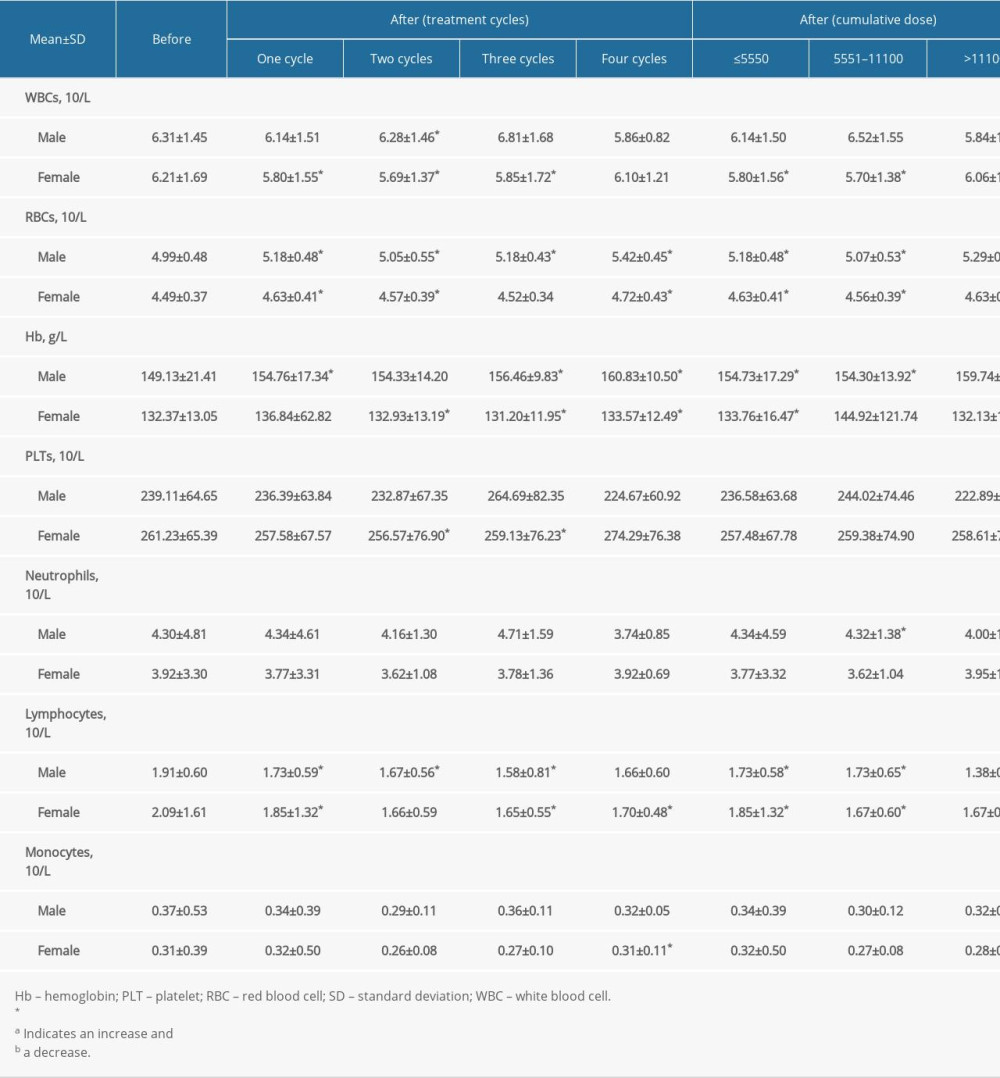 Table 4. CBC data before and after 131I therapy by age group and according to the number of treatment cycles and cumulative dose.
Table 4. CBC data before and after 131I therapy by age group and according to the number of treatment cycles and cumulative dose.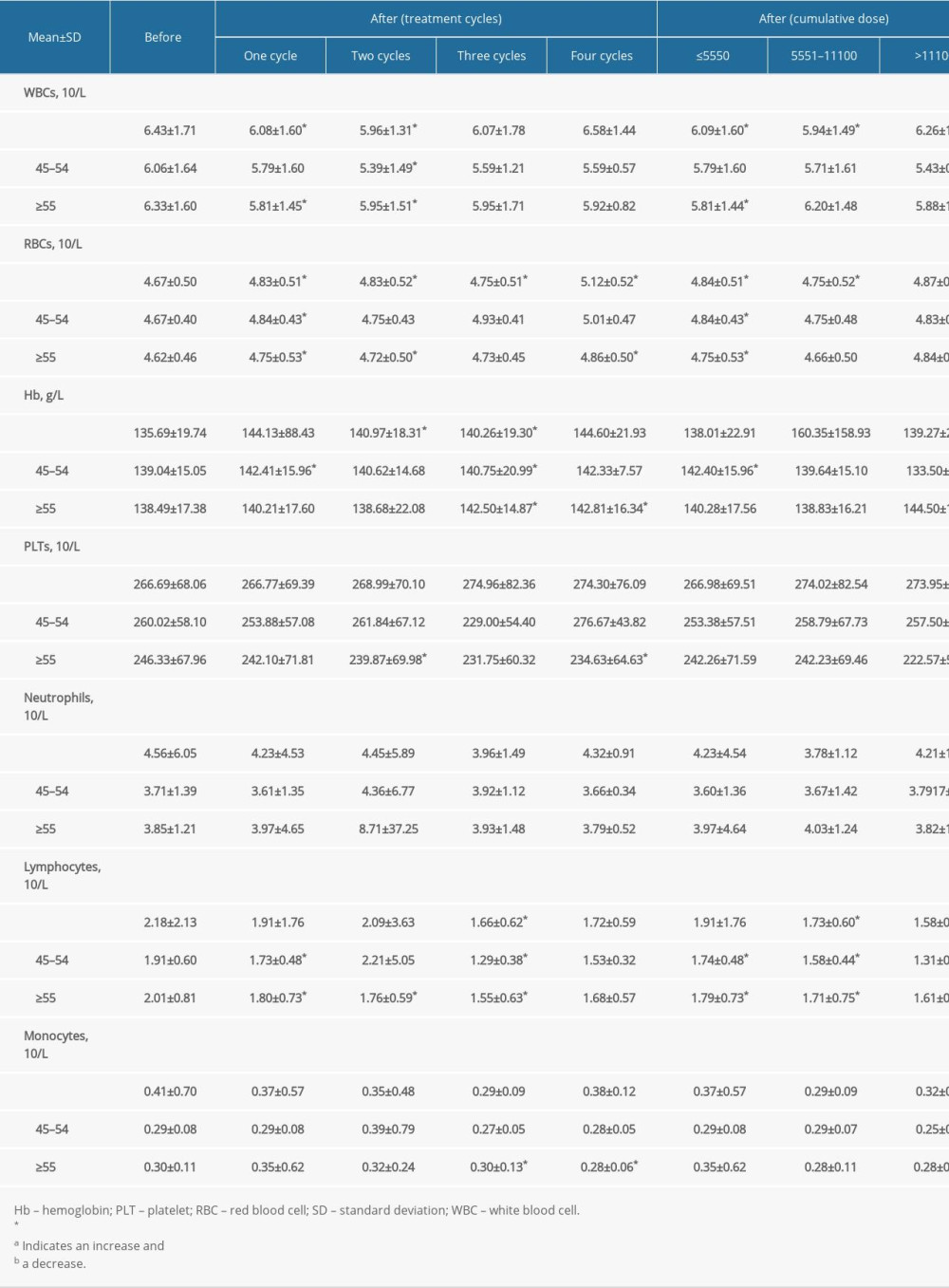
References
1. Davies L, Welch HG, Increasing incidence of thyroid cancer in the United States, 1973–2002: JAMA, 2006; 295; 2164-67
2. Filetti S, Durante C, Hartl D, Thyroid cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up: Ann Oncol, 2019; 30; 1856-83
3. Siegel RL, Miller KD, Jemal A, Cancer statistics, 2018: Cancer J Clin, 2018; 68; 7-30
4. Yang L, Zheng RS, Wang NAnalysis of incidence and mortality of thyroid cancer in China, 2013: Zhonghua Zhong Liu Za Zhi, 2017; 39(11); 862-67 [in Chinese]
5. Haugen BR, Alexander EK, Bible KC, 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer: Thyroid, 2016; 26; 1-133
6. Winkens T, Pachmann K, Freesmeyer M, The influence of radioiodine therapy on the number of circulating epithelial cells (CEC) in patients with differentiated thyroid carcinoma – a pilot study: Exp Clin Endocrinol Diabetes, 2014; 122; 246-53
7. Fard-Esfahani A, Emami-Ardekani A, Fallahi B, Adverse effects of radioactive iodine-131 treatment for differentiated thyroid carcinoma: Nucl Med Commun, 2014; 35; 808-17
8. Upadhyaya A, Meng Z, Wang P, Effects of first radioiodine ablation on functions of salivary glands in patients with differentiated thyroid cancer: Medicine (Baltimore), 2017; 96; e7164
9. Kloos RT, Duvuuri V, Jhiang SM, Nasolacrimal drainage system obstruction from radioactive iodine therapy for thyroid carcinoma: J Clin Endocrinol Metab, 2002; 87; 5817-20
10. Prinsen HT, Klein HE, Brouwers AH, Bone marrow function after (131)I therapy in patients with differentiated thyroid carcinoma: J Clin Endocrinol Metab, 2015; 100; 3911-17
11. Hu T, Meng Z, Zhang G, Influence of the first radioactive iodine ablation on peripheral complete blood count in patients with differentiated thyroid cancer: Medicine (Baltimore), 2016; 95; e4451
12. Keldse N, Mortense BT, Hanse HS, Haematological effects from radioiodinne treatment of thyroid carcinoma: Acta Oncol, 1990; 29; 1035-39
13. Haugen BR, Alexander EK, Bible KC, 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer: Thyroid, 2016; 26(1); 1-133
14. Nuclear Medicine Society of Chinese Medical Association, 131I Guidelines for the treatment of differentiated thyroid cancer (2014 edition): Kaku Igaku, 2014; 034(004); 264-78
15. Davies L, Welch HG, Current thyroid cancer trends in the United States: JAMA Otolaryngol Head Neck Surg, 2014; 140; 317-22
16. Evans C, Tennant S, Perros P, Serum thyroglobulin in the monitoring of differentiated thyroid cancer: Scand J Clin Lab Invest Suppl, 2016; 245; S119-23
17. Sawka AM, Thephamongkhol K, Brouwers M, Clinical review 170: A systematic review and metaanalysis of the effectiveness of radioactive iodine remnant ablation for well-differentiated thyroid cancer: J Clin Endocrinol Metab, 2004; 89; 3668-76
18. Sweeney D, Johnston G, Radioiodine treatment of thyroid cancer general considerations – II side effects of radioiodine therapy for thyroid cancer: Thyroid Cancer, 2000, Totowa, NJ, Humana Press
19. Lee SL, Complications of radioactive iodine treatment of thyroid carcinoma: J Natl Compr Canc Netw, 2010; 8; 1277-86
20. Eberlein U, Scherthan H, Bluemel C, DNA Damage in peripheral blood lymphocytes of thyroid cancer patients after radioiodine therapy: J Nucl Med, 2016; 57(2); 173-79
21. Zhang L, Chen J, Xu C, Effects of iodine-131 radiotherapy on Th17/Tc17 and Treg/Th17 cells of patients with differentiated thyroid carcinoma: Exp Ther Med, 2018; 15(3); 2661-66
22. Molinaro E, Leboeuf R, Shue B, Mild decreases in white blood cell and platelet counts are present one year after radioactive iodine remnant ablation: Thyroid, 2009; 19(10); 1035-41
23. Padovani RP, Tuttle RM, Grewal R, Complete blood counts are frequently abnormal 1 year after dosimetry-guided radioactive iodine therapy for metastatic thyroid cancer: Endocr Pract, 2014; 20; 213-20
24. Tofani A, Sciuto R, Cioffi R, Radioiodine-induced changes in lymphocyte subsets in patients with differentiated thyroid carcinoma: Eur J Nucl Med, 1999; 26; 824-29
25. Probst S, Abikhzer G, Chausse G, I-131 Radiation-induced myelosuppression in differentiated thyroid cancer therapy: Mol Imaging Radionucl Ther, 2018; 27; 84-87
26. Golde DW, Bersch N, Chopra IJ, Thyroid hormones stimulate erythropoiesis in vitro: Br J Haemato, 1977; 37; 173-77
27. Chun SH, Park G, Han YK, Effect of low dose radiation on differentiation of bone marrow cells into dendritic cells: Dose Response, 2012; 11; 374-84
28. Vrndic OB, Djurdjevic PM, Jovanovic DD, Blood cells in thyroid cancer patients: A possible influence of apoptosis: Open Med (Wars), 2016; 11; 87-92
29. Gagnon A, Lochnan HA, Tran CS, Thyroid-stimulating hormone acutely increases monocyte gene expression in vivo: Neuro Endocrinol Lett, 2016; 37; 121-23
30. Weerd K, Hagen PM, Schrijver B, Thyrotropin acts as a T-cell developmental factor in mice and humans: Thyroid, 2014; 24; 1051-61
Figures
Figure 1. Changes in lymphocyte counts after 131I treatment cycles. The counts consistently declined from the first to the third 131I cycles and then increased after the fourth 131I therapy. The decrease that was statistically significant compared with the baseline lymphocyte count occurred after the third 131I cycle (1.44±0.43 vs 1.90±0.63, P=0.001).Figure 2. Changes in monocyte counts after 131I treatment cycles. The number of monocytes decreased after the first treatment and then gradually increased after the last 3 treatments. While the differences between post-treatment and baseline values were not significant, the last 2 post-treatment values were higher than the value after the first treatment (0.30±0.10 and 0.31±0.09 vs 0.22±0.05, both P=0.001).Figure 3. Changes in monocyte counts after cumulative doses of 131I therapy. The number of monocytes decreased when patients had received ≤5550 MBq of 131I and then gradually increased after patients had received >5550 MBq of 131I. While there were no statistically significant differences between post-treatment and baseline values, patients who received >11 100 MBq of 131I had higher monocyte counts than those who received ≤5550 MBq of 131I (0.30±0.09 vs 0.22±0.05, P=0.003). Tables
Table 1. Patient groupings.Table 2. CBC data before and after 131I therapy according to the number of treatment cycles and cumulative dose.Table 3. CBC data before and after 131I therapy by gender and according to the number of treatment cycles and cumulative dose.Table 4. CBC data before and after 131I therapy by age group and according to the number of treatment cycles and cumulative dose.Table 1. Patient groupings.Table 2. CBC data before and after 131I therapy according to the number of treatment cycles and cumulative dose.Table 3. CBC data before and after 131I therapy by gender and according to the number of treatment cycles and cumulative dose.Table 4. CBC data before and after 131I therapy by age group and according to the number of treatment cycles and cumulative dose. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387