22 August 2021: Clinical Research
Association Between Blood Pressure Control and Arterial Stiffness in Middle-Aged and Elderly Chinese Patients with Hypertension
Geyue Qu1ABCDEF*, Zhongying Zhang1AEF, Hong Zhu1BCDDOI: 10.12659/MSM.931414
Med Sci Monit 2021; 27:e931414






Abstract
BACKGROUND: The severity of arterial stiffness can be evaluated by pulse wave velocity (PWV). This study investigated the association between blood pressure (BP) control and arterial stiffness in middle-aged and elderly Chinese patients with hypertension.
MATERIAL AND METHODS: Three hundred and twelve hypertensive patients were divided according to whether their hypertension was well-controlled or uncontrolled and stratified according to age. Arterial stiffness was evaluated by brachial-ankle pulse wave velocity (baPWV). The effect of BP control on arterial stiffness and its severity was assessed by multivariate linear and logistic regression analyses.
RESULTS: Moderate and severe arterial stiffness was detected significantly more often in patients with uncontrolled hypertension than in those with well-controlled hypertension, regardless of age. BaPWV increased by 8.467 cm/s in the study population overall for every 1-mmHg increment in systolic BP and by 8.584, 8.616, and 8.199 cm/s, respectively, in patients aged 45-65, 65-80, and ≥80 years. Regardless of age, the risk of arterial stiffness was 5.93 times higher (95% confidence interval 2.78-12.64) and the risk of a one-grade increase in the severity of arterial stiffness was 4.01 times higher (95% confidence interval 2.51-6.42) in patients with uncontrolled hypertension than in those with well-controlled hypertension.
CONCLUSIONS: This study found a positive relationship between baPWV and BP and identified uncontrolled BP as a risk factor for arterial stiffness and its severity. Management of BP within a reasonable range may help to ameliorate arterial stiffness.
Keywords: Blood Pressure, essential hypertension, Vascular Stiffness, Aged, 80 and over, Arteries, Hypertension, Public Health Surveillance, Severity of Illness Index, Surveys and Questionnaires
Background
Arterial stiffness (AS) is an early functional vascular lesion [1] that has been confirmed to be a risk factor for cardiovascular events and is an important characteristic in the development of essential hypertension. Deaths associated with elevated systolic blood pressure (BP) increased between 1990 and 2015 [2], and the morbidity of hypertension increases with age [3,4]. The morbidity rate of hypertension is twice as high in the elderly than it is in their younger counterparts [5], and two-thirds of people over the age of 65 years have hypertension. The vascular walls of the elderly are less elastic and more vulnerable to the effect of high BP [6]. A multicenter cohort study [7] showed that pulse wave velocity increased with age in hypertensive patients, especially after the age of 50 years. Therefore, more attention should be focused on arterial function in middle-aged and elderly patients with hypertension. Brachial-ankle pulse wave velocity (baPWV) is widely used to evaluate AS and its severity [8,9]. In this study, baPWV was used to investigate the association between BP control and AS in middle-aged and elderly hypertensive Chinese patients to increase awareness of the importance of BP control in older patients.
Material and Methods
STUDY POPULATION:
The study population consisted of 312 hypertensive Chinese patients aged 45–97 years who were hospitalized in the Geriatrics Department at the Xuanwu Hospital of Capital Medical University, Beijing, between January 2018 and October 2019 and in whom there had been no change in antihypertensive therapy for at least 2 weeks. Patients with coronary heart disease, dyslipidemia, diabetes mellitus, and/or stroke were included. None of the subjects had secondary hypertension, acute cardiovascular disease, atrial fibrillation, acute cerebrovascular disease, cancer, infection, thyroid dysfunction, hepatic disease, end-stage kidney disease (stage ≥4), acute kidney injury, aortic aneurysm, an ankle/brachial pressure index ≤0.9 or >1.4, or previous endovascular and/or surgical treatment for peripheral arterial disease.
This study was approved by the Ethics Committee of Xuanwu Hospital of Capital Medical University and was conducted in accordance with the principles of the Declaration of Helsinki. Informed consent was obtained from each patient before data collection.
DATA COLLECTION:
The study data included clinical examinations, questionnaire assessments, laboratory tests, and baPWV measurements for all patients. All BP and baPWV data were collected on the same day.
CLINICAL EXAMINATIONS:
Clinical measurements followed the standard recommended procedures. Height and weight were measured for each subject, and body mass index was calculated as weight in kilograms divided by the square of height in meters.
After a 15-minrest, subjects were asked to sit at a table with their upper arms exposed and placed at the heart level. BP was measured twice by an experienced physician using a clinically validated electronic sphygmomanometer (HBP-1400; Omron, Dalian, China). No cigarette, coffee, tea, or alcohol consumption was allowed for 30 min before the measurements were recorded. The average reading was analyzed. Hypertension was defined as a sitting systolic BP ≥140 mmHg and/or a diastolic BP ≥90 mmHg on more than 3 consecutive occasions on different days or as the use of antihypertensive medication. Patients aged 45–65 years were considered to be middle-aged and those older than 65 years were deemed to be elderly.
According to the major guidelines for hypertension [10–12], we defined the following target BP values for antihypertensive therapy: <130/80 mmHg in the group aged 45–65 years;<140/90 mmHg in the group aged 65–80 years; <150/90 mmHg in the group aged ≥80 years; <140/80 mmHg in the group aged45–65 years with chronic kidney disease; and <140/90 mmHg in the group aged ≥65 years with diabetes or chronic kidney disease.
QUESTIONNAIRE ASSESSMENTS:
Standardized questionnaires, including basic information (eg, name, sex, age), lifestyle habits (eg, smoking status, alcohol consumption), medical history (coronary heart disease, diabetes mellitus, dyslipidemia, and stroke), medications (antihypertensive, antidiabetic, and antihyperlipidemic agents), were completed by doctors. Smoking was defined as a self-reported history of smoking for ≥1 year. Drinking was defined as a self-reported history of alcohol consumption for ≥1 year.
LABORATORY TESTS:
Venous blood samples were collected from the forearm after overnight fasting and sent to the clinical laboratory department at Xuanwu Hospital within 30 min, where they were tested for fasting blood glucose (FBG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), triglycerides, uric acid, homocysteine, serum creatinine, and hemoglobin using an auto-analyzer (Hitachi 7600; Tokyo, Japan). The estimated glomerular filtration rate was calculated using the Chronic Kidney Disease Epidemiology Collaboration method [13].
BAPWV MEASUREMENTS:
BaPWV was measured using an oscillometer-based device (BP-203RPE III; Colin-Omron, Co., Ltd., Tokyo, Japan) after at least 5 min of rest in the supine position. Coffee, tea, cigarette, and alcohol consumption was not allowed for 30 min before the test. Trained technicians and physicians placed pressure cuffs on both arms and ankles. The lower edge of the arm cuff was positioned 2–3 cm above the cubital fossa transverse striation, and the lower edge of the ankle cuff was positioned 1–2 cm above the medial malleolus. The heart monitor was placed on the left edge of the sternum, and the electrodes for the electrocardiogram were placed directly. Bilateral baPWV readings were taken simultaneously, and the maximum readings for the right and left baPWV were used for the analysis.
BaPWV was used to assess arterial stiffness in this study because of the known positive relationship between these 2 parameters. According to a previous report [14], AS was classified as mild if baPWV was ≥1400 cm/s, moderate if baPWV was ≥1700 cm/s, and severe if baPWV was ≥2000 cm/s.
STATISTICAL ANALYSIS:
All data were confirmed to be normally distributed. Continuous variables are presented as the mean±standard deviation and were compared between 2 groups using the
Results
PATIENT CHARACTERISTICS:
The mean age of the 312 study participants was 68.3±12.6 years (range 45–97), and 197 (63.1%) were male. The patient demographic and clinical characteristics stratified by BP are shown in Table 1. The subjects were divided into 2 groups according to whether their BP met the target; 169 patients (54.2%) had well-controlled hypertension (mean age 69.6±12.0 years [range 45–93]), whereas 143 (45.8%) had uncontrolled hypertension (mean age 66.7±13.1years [range 45–97]). Systolic and diastolic BP values were higher in patients with uncontrolled hypertension than in those with well-controlled hypertension. Furthermore, there were statistically significant between-group differences in systolic and diastolic BP, age, FBG, LDL-C, and triglyceride levels and in the proportions of patients who smoked, consumed alcohol, and took antihypertensive medication (P<0.05).
When subjects were divided into age groups, namely, 45–65 years (n=129), 65–80 years (n=111), and ≥80 years (n=72), systolic BP was observed to increase and the diastolic BP decreased with age (P<0.05; Table 2).
DISTRIBUTION OF BAPWV AND AS DETECTION RATES:
The distribution of baPWV and the frequency of AS detection for both the study population overall and by age subgroup are shown in Table 3. The mean baPWV was 1779.2±404.8 cm/s, and the AS detection rate was 79.5%. The baPWV values and AS detection rates were significantly higher in patients with uncontrolled hypertension than in those with well-controlled hypertension in all age groups (P<0.05) and increased with age.
DISTRIBUTION OF DEGREES OF AS:
The distribution of the severity of AS in the study population overall and the age subgroups (excluding patients without AS) is shown in Table 4. In the study population overall, the detection rates for mild, moderate, and severe AS were 33.0%, 19.2%, and 27.2%, respectively. The detection rates for moderate and severe AS were significantly higher in patients with uncontrolled hypertension than in those with well-controlled hypertension, regardless of age (P<0.05).
MULTIVARIATE LINEAR REGRESSION ANALYSIS OF SYSTOLIC BP AND BAPWV:
The results of the multivariate linear regression analysis for systolic BP and baPWV in the study population overall and in the age subgroups are shown in Table 5. With baPWV as the dependent variable and systolic BP as the independent variable, after adjusting for age, sex, FBG, LDL-C, triglycerides, smoking, alcohol consumption, and antihypertensive medication, multivariate linear regression analysis of data for the study population overall showed a positive linear relationship between systolic BP and baPWV (t=7.862, P<0.05) and an increase in baPWV by 8.467cm/s for every 1-mmHg increment in systolic BP. Furthermore, a positive linear relationship was observed between systolic BP and baPWV in patients aged 45–65 years, 65–80 years, and ≥80 years (t=6.254, t=4.307, and t=3.260, respectively; P<0.05); the baPWV increased by 8.584, 8.616, and 8.199 cm/s, respectively, for each 1-mmHg increment in systolic BP.
BINARY AND ORDINAL LOGISTIC REGRESSION ANALYSIS OF BP CONTROL AND AS OR ITS SEVERITY:
The results of the binary and ordinal logistic regression analyses of BP control and AS and its severity in the study population overall are shown in Table 6. With baPWV as the dependent variable (<1400 cm/s, 0; ≥1400 cm/s, 1), and BP control as the independent variable (well-controlled BP, 0; uncontrolled BP, 1), after adjusting for age, sex, FBG, triglycerides, LDL-C, smoking, alcohol consumption, and antihypertensive medication, binary logistic regression analysis showed that the risk of AS in patients with uncontrolled hypertension was 5.93 times higher (95%CI, 2.78–12.64) than that in patients with well-controlled hypertension. In the study population overall, with baPWV as the dependent variable (mild AS, 1; moderate AS, 2; severe AS, 3) and BP control as the independent variable (well-controlled BP, 0; uncontrolled BP, 1), after adjusting for the above-mentioned factors, binary logistic regression analysis showed that the risk of a one-grade increase in the severity of AS in patients with uncontrolled hypertension was 4.01 times higher (95%CI, 2.51–6.42) than that in patients with well-controlled hypertension.
Discussion
Previous studies [15] found that age and BP are the 2 most important factors influencing PWV. In this study, both the baPWV value and the AS detection rate (baPWV ≥1400 cm/s) increased from middle-age through to old age, indicating that AS is part of the aging process in patients with hypertension. In this study, the baPWV value was high in hypertensive patients, reaching 1779.2±404.8cm/s in the study population overall and 1528.9±249.8, 1859.2±362.0, and 2104.0±414.2cm/s in patients aged 45–65, 65–80 and ≥80 years, respectively. Although the samples were different, a study by Ueki et al [16] showed the same trend. However, baPWV was significantly higher in our study than in a previous study by Yiming et al in younger hypertensive patients [17]. The rate of detection of AS in middle-aged and elderly patients with hypertension was high, at 79.5%, and the detection rates for mild, moderate, and severe AS were 33.0%, 19.2%, and 27.2%, respectively. BaPWV is a classical clinical indicator of AS that has been shown to be closely related to cardiovascular events [18] and is an independent risk factor for cardiovascular disease [19]. Niiranen et al [20] showed that the risk of cardiovascular events was greater in individuals with high PWV than in those with low PWV, regardless of whether they were hypertensive. Therefore, patients with high PWV, particularly those who are hypertensive and middle-aged or elderly, should be managed carefully.
In a study that included 1079 patients [21], the mean PWV was 6.85±1.66 m/s in the normotensive control group and 8.04±1.8 m/s in the hypertensive group, and it increased linearly with age. In that study, the mean PWV was significantly higher in patients over 50 years of age than in younger patients (8.35 m/s vs 5.92 m/s, P<0.001); moreover, the rate of increase in PWV per decade was significantly higher in the hypertensive group than in the normotensive group (0.93 m/s vs 0.44 m/s, P<0.001). A large-scale longitudinal study that followed up 577 Chinese patients from 2008 to 2014 [22] found that the PWV was more rapid in hypertensive subjects than in normotensive subjects and that subjects who were normotensive at baseline and subsequently became hypertensive during follow-up had a more rapid PWV than those who remained normotensive. The results of that study are consistent with our present findings that PWV increases with age and BP. In our study, middle-aged and elderly patients with hypertension were prone to developing a high baPWV and severe AS. Therefore, these patients should be considered as a high-risk group. Regular monitoring of AS in patients with hypertension from middle-age onwards and timely detection of changes in AS could delay or prevent cardiovascular disease.
The EVOPIU study [23], in which subjects were followed up for 4 years, showed that carotid-femoral PWV was higher in the hypertensive group with poor BP control than in the normotensive group and the hypertensive group with good BP control and that the PWV increased with age. Moreover, a survey of the offspring of the original participants in the Framingham study [20] found that a high PWV was significantly more common in subjects with uncontrolled hypertension than in those with well-controlled hypertension (90% vs 60%). In our study of a middle-aged and elderly hypertensive population, the mean baPWV value and the AS detection rate were significantly higher in patients with uncontrolled hypertension (1860.4±404.2 cm/s and 90.9%, respectively) than in those with well-controlled hypertension (1710.4±393.6 cm/s and 69.8%). Furthermore, the moderate and severe AS detection rates were both significantly higher in patients with uncontrolled hypertension (27.3% and 32.2%, respectively) than in those with well-controlled hypertension (12.4% and 23.1%).
The findings outlined above indicate that fluctuation of BP accelerates progression of AS in patients with hypertension. A cross-sectional study in a rural adult population in China [24] showed that baPWV was more closely correlated with BP (including systolic BP, diastolic BP, mean arterial pressure, and pulse pressure) than age (Spearman correlation coefficient, P<0.001). In this study, even in the same age group, baPWV, detection rate of AS, and the incidence of moderate or severe AS were high in patients with uncontrolled hypertension, indicating that AS development could be avoided by well-controlled BP regardless of age. Furthermore, multivariate linear regression analysis revealed a positive linear relationship between systolic BP and baPWV in the study population overall and the different age groups. In the study population overall, baPWV increased by 8.467 cm/s with each 1-mmHg increment in systolic BP and by 8.584, 8.616, and 8.199 cm/s in patients aged 45–65, 65–80, and ≥80 years, respectively. After adjusting for other confounding factors, logistic regression analysis showed that uncontrolled BP was a risk factor for AS and its severity. The risk of AS was 5.93 times higher (95%CI 2.78–12.64) and the risk of a one-grade increase in the severity of AS was 4.01 times higher (95% CI 2.51–6.42) in patients with uncontrolled hypertension than in those with well-controlled hypertension. Our study shows that well-controlled BP could reduce the risk and severity of AS in middle-aged and elderly patients with hypertension. Therefore, antihypertensive therapy should focus on the target BP; and standard treatment is the key to reducing cardiovascular events, which has similarly been confirmed by previous studies. A meta-analysis [25] showed that BP <150/90 mmHg in hypertensive patients aged 60 years or older could significantly improve health status.
This study confirmed the effect of BP on baPWV. Therefore, we should be concerned with not only BP but also baPWV in hypertensive patients. The recommendations for target BP in the current guidelines in elderly patients with hypertension are not consistent [26]. The 2019 Chinese guideline for the management of hypertension in the elderly [11] indicates that BP should be decreased to 140/90 mmHg in patients aged over 65 years and initially to 150/90 mmHg and subsequently to 140/90 mmHg, if possible, in patients over 80 years of age. Meanwhile, the 2018 European Guidelines for Hypertension [12] recommend a target BP range of 130–140/70–80 mmHg in patients over the age of 65 years, but do not set a specific target for those over 80 years, and emphasize only a lower limit of 130/70 mmHg in patients over 65 years. However, the SPRINT study [27], which included patients aged 75 years or older, found that compared with a systolic BP of 140 mmHg, a value <120 mmHg could significantly reduce fatal and nonfatal major cardiovascular events and mortality from any cause without increasing the total incidence of serious adverse events. BaPWV can be used in patients with hypertension to predict the risk of cardiovascular disease and as an indicator of target organ damage and BP control during long-term antihypertensive treatment [28]. As required by the European Guidelines for Hypertension, antihypertensive therapy should not only meet the BP target but also reduce the severity of AS, and improvement in PWV should be evaluated simultaneously while controlling BP. At present, there is still a lack of consensus regarding antihypertensive targets in the elderly. Therefore, further large-scale and multiregional studies are needed to define antihypertensive treatment targets that can delay or ameliorate AS.
AS is a manifestation of arterial dysfunction, and its pathological mechanism includes collagen deposition, fracture or degradation of elastic fibers, necrosis and calcification in the middle arterial layer, and collagen cross-linking, which results in excessive vascular fibrosis and reduced elasticity [1]. Aging causes degenerative changes in the vessel wall, leading to the above changes in vascular structure [29], vascular endothelial dysfunction, decreased release of vasodilators (nitric oxide and prostacyclin), and increased release of vasoconstrictors (endothelin and thromboxane), which further promote AS. The same changes occur in AS caused by hypertension; however, the exact mechanism has not been fully elucidated, which is not only shown on the hemodynamic changes. Activation of the renin-angiotensin-aldosterone system, oxidative stress, and other factors can similarly cause excessive arterial fibrosis and deposition of extracellular matrix, leading to AS. It has been reported that hypertension and AS cause and affect each other and that stiffness of the vascular wall and stenosis of the vascular lumen caused by AS are risk factors for high BP [20]. However, the temporal relationship between arterial stiffness and BP remains controversial. The Bogalusa Heart Study [30] reported that elevated BP preceded increased arterial stiffness during young adulthood. In contrast, a study by Wu et al [31] found that arterial stiffness can precede elevated BP. The reasons may be that the subjects in the latter study were older and the follow-up time was shorter. In addition, BP hemodynamics changed with aging, which might change the temporal relationship between arterial stiffness and BP.
This study has several limitations. First, all study participants were Chinese, and the sample size was small. Therefore, its results require confirmation in a large multicenter study. Second, BP was measured in the ward. Therefore, the possibility that white-coat and masked hypertension may have resulted in the overestimation or underestimation of BP and affected our results cannot be excluded. Third, although relevant confounding factors were adjusted for as far as possible when evaluating the relationship between BP and baPWV, we did not adjust for changes in environment, physical exercise, or dietary habits. Fourth, we used baPWV rather than the criterion standard of carotid-femoral PWV to evaluate AS, which may have caused some errors.
Conclusions
In this study, we observed a high rate of AS and a positive relationship between baPWV and BP in middle-aged and elderly Chinese patients with hypertension and identified uncontrolled BP to be a risk factor for AS and its severity. Therefore, we should both actively monitor the degree of AS and prescribe antihypertensive therapy. Standard treatment with a target BP is the key to reducing cardiovascular events in middle-aged and elderly patients with hypertension.
Tables
Table 1. Patient characteristics*.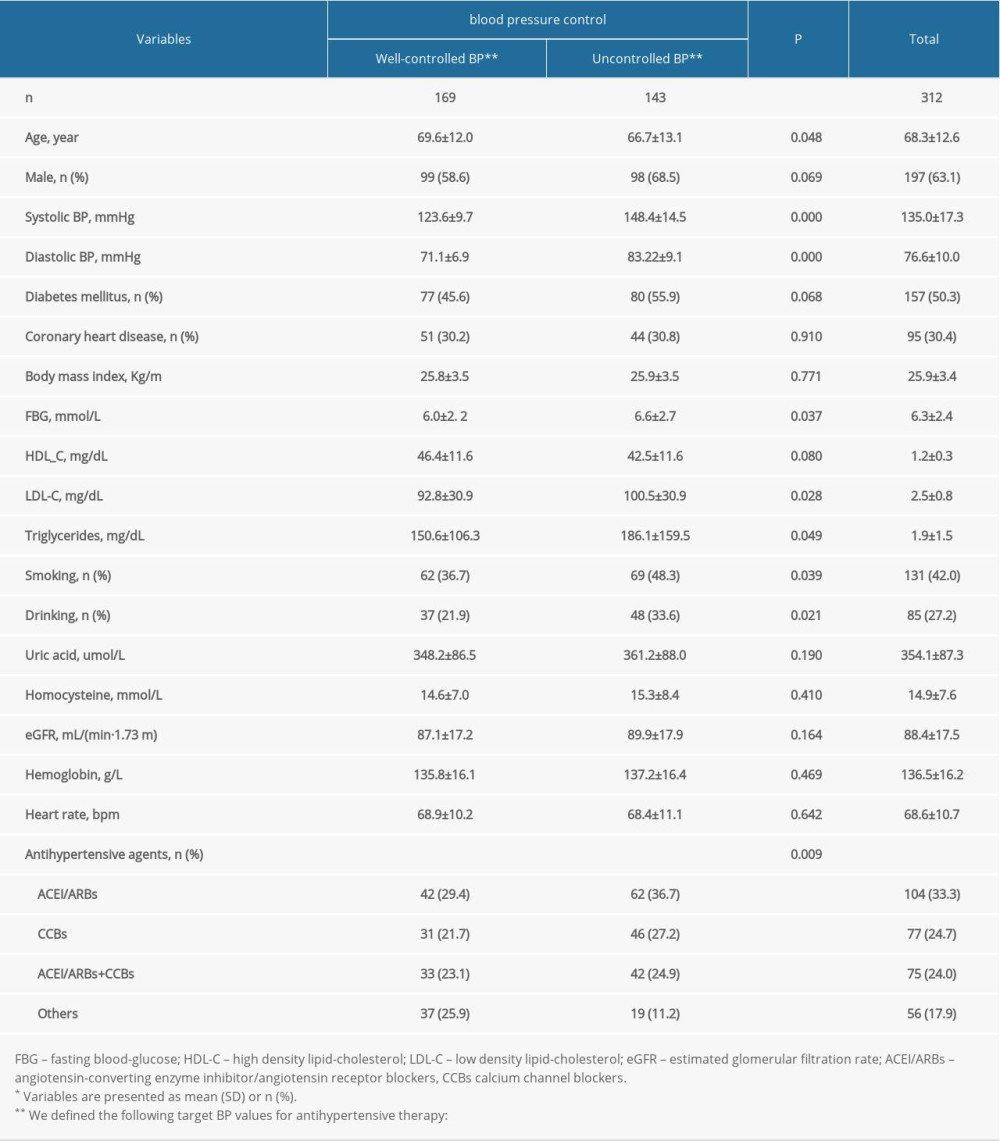 Table 2. Characteristics of total subjects* according to different age groups.
Table 2. Characteristics of total subjects* according to different age groups.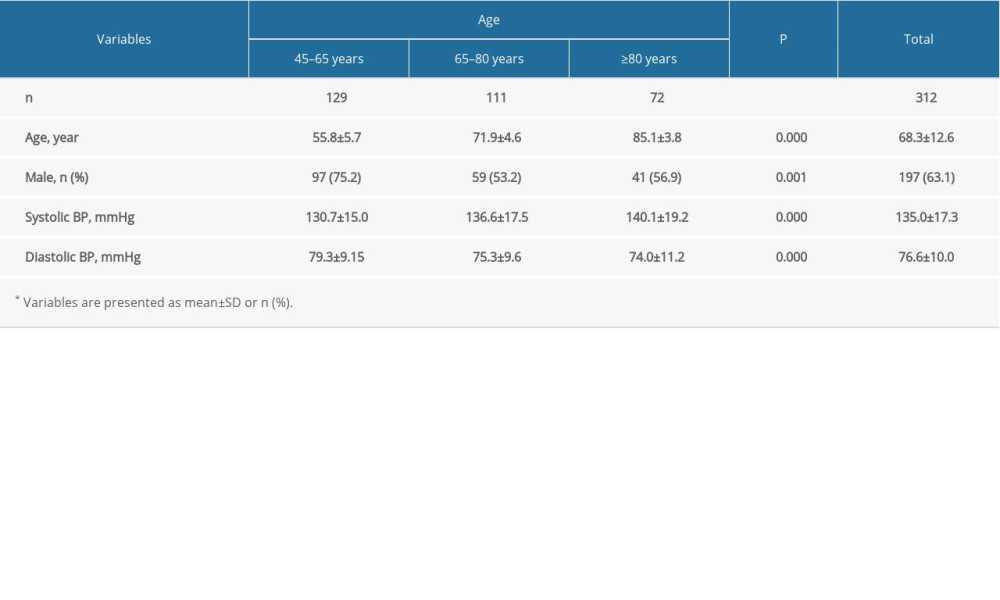 Table 3. Distribution of baPWV and AS detection rates for both the study population overall and by age subgroup*.
Table 3. Distribution of baPWV and AS detection rates for both the study population overall and by age subgroup*.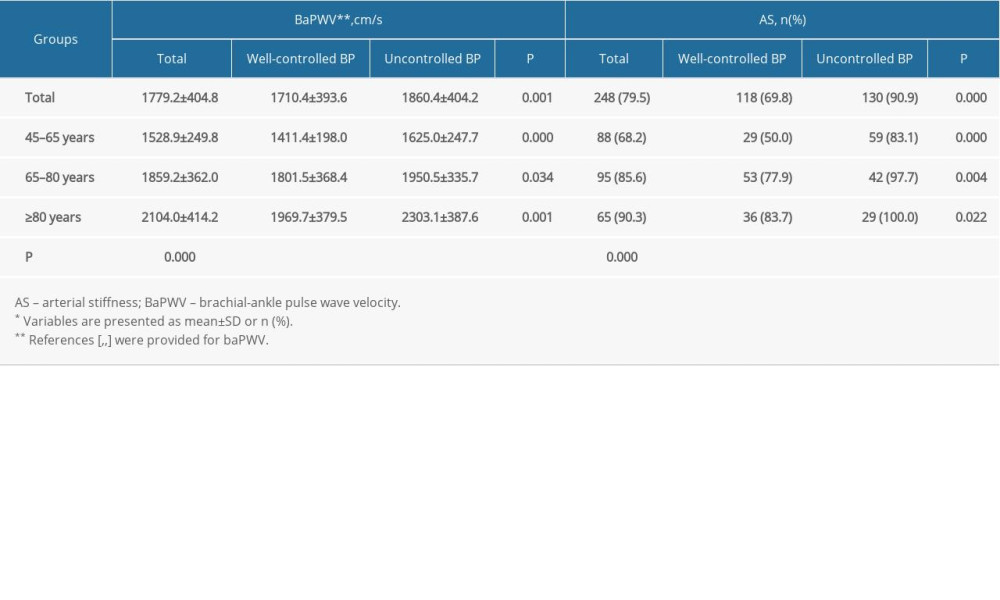 Table 4. Distribution of degrees of AS in the study population overall and the age subgroups*.
Table 4. Distribution of degrees of AS in the study population overall and the age subgroups*.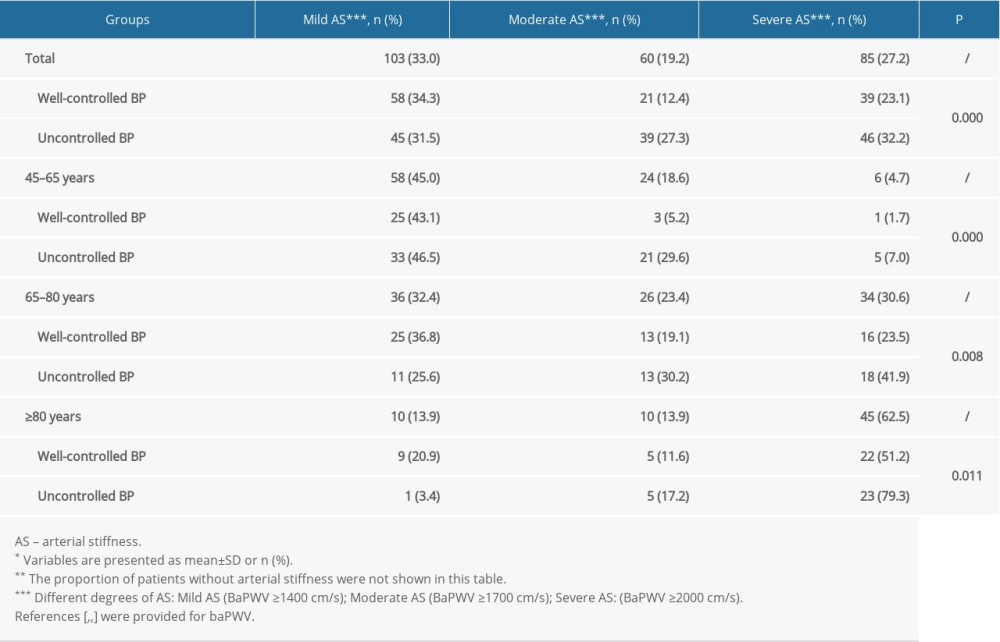 Table 5. Multivariate linear regression analysis of systolic BP and baPWV in the study population overall and the age subgroups*.
Table 5. Multivariate linear regression analysis of systolic BP and baPWV in the study population overall and the age subgroups*.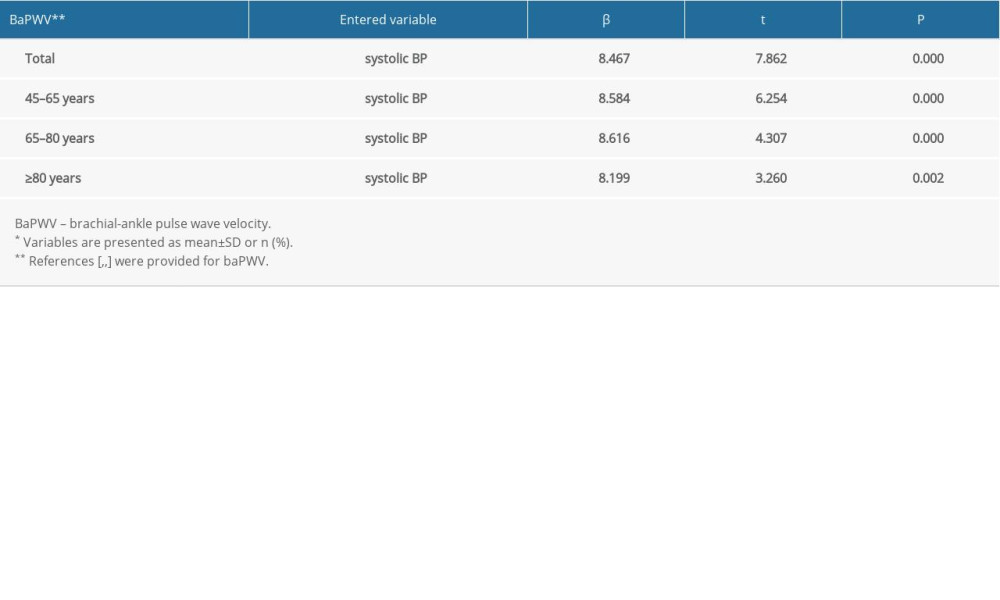 Table 6. Binary and ordinal logistic regression analysis of BP control and AS and its severity in the study population overall*.
Table 6. Binary and ordinal logistic regression analysis of BP control and AS and its severity in the study population overall*.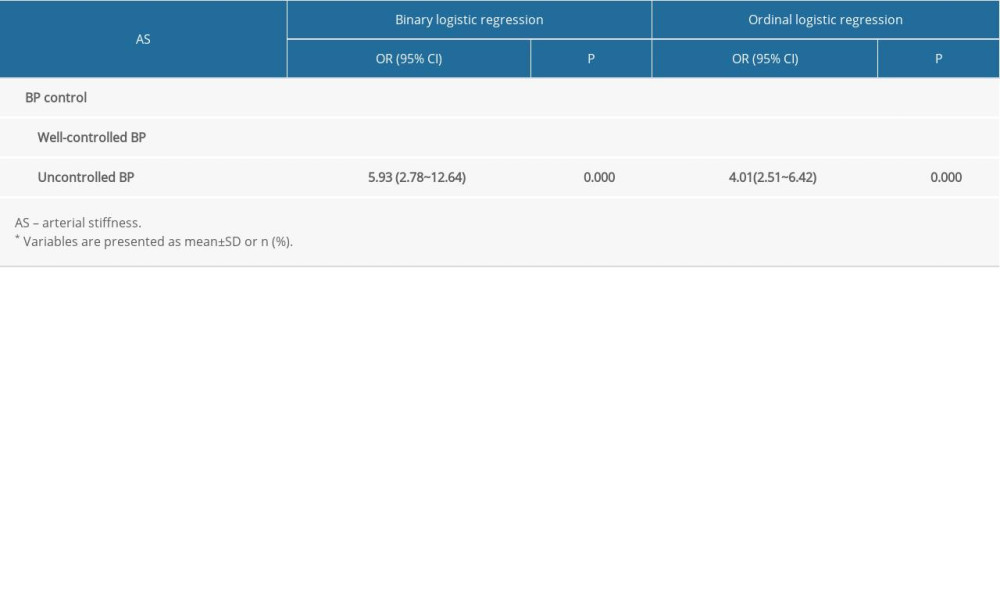
References
1. Townsend RR, Wilkinson LB, Schiffrin EL, Recommendations for improving and standardizing vascular research on arterial stiffness: A Scientific Statement from the American Heart Association: Hypertension, 2015; 66; 698-722
2. Forouzanfar MH, Liu P, Roth GA, global burden of hypertension and systolic blood pressure of at least 110 to 115 mmHg, 1990–2015: JAMA, 2017; 317; 165-82
3. Zheng Ml, Xu Xp, Wang Xb, Age, arterial stiffness, and components of blood pressure in Chinese adults: Medicine (Baltimore), 2014; 93; e262
4. Levine DA, Lewis CE, Williams OD, Geographic and demographic variability in 20-year hypertension incidence: The CARDIA study: Hypertension, 2011; 57; 39-47
5. Ferreira I, van de Laar RJ, Prins MH, Carotid stiffness in young adults: A life-course analysis of its early determinants: The Amsterdam Growth and Health Longitudinal Study: Hypertension, 2012; 59; 54-61
6. Kobalava DZ, Shavarova KE, Clinical features of arterial hypertension in the elderly and senile age and the rationale for using the combination of amlodipine/indapamide-retard: Kardiologiia, 2017; 57; 60-70
7. Diaz A, Tringler M, Wray S, The effects of age on pulse wave velocity in untreated hypertension: J Clin Hypertens (Greenwich), 2018; 20; 258-65
8. Jannasz I, Sondej T, Targowski TPulse wave velocity – a useful tool in assessing the stiffness of the arteries: Pol Merkur Lekarski, 2019; 46; 257-62 [in Polish]
9. Munakata M, Brachial-ankle pulse wave velocity in the measurement of arterial stiffness: Recent evidence and clinical applications: Curr Hypertens Rev, 2014; 10; 49-57
10. Liu L-S2010 Chinese guidelines for the management of hypertension: Zhonghua Xin Xue Guan Bing Za Zhi, 2011; 39(7); 579-615 [in Chinese]
11. 2019 Chinese guideline for the management of hypertension in the elderly: Chin J Cardiovasc Med, 2019; 24; 1-23 [in Chinese]
12. Williams B, Mancia G, Spiering W, 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: J Hypertens, 2018; 36; 1953-2041
13. Levey AS, Stevens LA, Schmid CH, A new equation to estimate glomerular filtration rate: Ann Intern Med, 2009; 150; 604-12
14. Huang Jh, Chen Zk, Yuan Jh, Association between body mass index (BMI) and brachial-ankle pulse wave velocity (baPWV) in males with hypertension: A community-based cross-section study in North China: Med Sci Monit, 2019; 25; 5241-57
15. Mitchell GF, Arterial stiffness and hypertension: Hypertension, 2014; 64; 13-18
16. Ueki Y, Miura T, Minamisawa M, The usefulness of brachial-ankle pulse wave velocity in predicting long-term cardiovascular events in younger patients: Heart Vessel, 2017; 32; 660-67
17. Yiming G, Zhou Xh, Lv Wk, Reference values of brachial-ankle pulse wave velocity according to age and blood pressure in a central Asia population: PLoS One, 2017; 12; e0171737
18. Ben-Shlomo Y, Spears M, Boustred C, Aortic pulse wave velocity improves cardiovascular event prediction: An individual participant meta-analysis of prospective observational data from 17,635 subjects: J Am Coll Cardiol, 2014; 63; 636-46
19. Tomiyama H, Matsumoto C, Shiina K, Yamashina A, Brachial-Ankle PWV: Current status and future directions as a useful marker in the management of cardiovascular disease and/or cardiovascular risk factors: J Atheroscler Thromb, 2016; 23; 128-46
20. Niiranen TJ, Kalesan B, Hamburg NM, Relative contributions of arterial stiffness and hypertension to cardiovascular disease: The Framingham Heart Study: J Am Heart Assoc, 2016; 5; e004271
21. Diaz A, Tringler M, Wray S, The effects of age on pulse wave velocity in untreated hypertension: J Clin Hypertens (Greenwich), 2018; 20; 258-65
22. Lin LY, Liao YC, Lin HF, Determinants of arterial stiffness progression in a Han-Chinese population in Taiwan: A 4-year longitudinal follow-up: BMC Cardiovasc Disord, 2015; 15; 100
23. de Mendonça GS, de Souza DF, de Alvarenga Cunha Brunelli AC, Arterial stiffness in elderly patients with normotension and hypertension in Brazil: J Clin Hypertens, 2018; 20; 1285-93
24. Xu Yx, Wu Yq, Li J, The predictive value of brachial-ankle pulse wave velocity in coronary atherosclerosis and peripheral artery diseases in urban Chinese patients: Hypertens Res, 2008; 31; 1079-85
25. Weiss J, Freeman M, Low A, Benefits and harms of intensive blood pressure treatment in adults aged 60 years or older: A systematic review and meta-analysis: Ann Intern Med, 2017; 166; 419-29
26. Kjeldsen S, Feldman RD, Lisheng L, Updated national and international hypertension guidelines: A review of current recommendations: Drugs, 2014; 74; 2033-51
27. Williamson JD, Supiano MA, Applegate WB, Intensive vs standard blood pressure control and cardiovascular disease outcomes in adults aged ≥75 years: A randomized clinical trial: JAMA, 2016; 315; 2673-82
28. Chobanian AV, Bakris GL, Black HR, Seventh report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure: Hypertension, 2003; 42; 1206-52
29. Spronck B, Heusinkveld MHG, Donders WP, A constitutive modeling interpretation of the relationship among carotid artery stiffness, blood pressure, and age in hypertensive subjects: Am J Physiol Heart Circ Physiol, 2015; 308; H568-82
30. Chen W, Li S, Fernandez C, Temporal relationship between elevated blood pressure and arterial stiffening among middle-aged black and white adults: The Bogalusa Heart Study: Am J Epidemiol, 2016; 183; 599-608
31. Wu S, Jin C, Li S, Aging, arterial stiffness, and blood pressure association in Chinese adults: Hypertension, 2019; 73; 893-99
Tables
Table 1. Patient characteristics*.Table 2. Characteristics of total subjects* according to different age groups.Table 3. Distribution of baPWV and AS detection rates for both the study population overall and by age subgroup*.Table 4. Distribution of degrees of AS in the study population overall and the age subgroups*.Table 5. Multivariate linear regression analysis of systolic BP and baPWV in the study population overall and the age subgroups*.Table 6. Binary and ordinal logistic regression analysis of BP control and AS and its severity in the study population overall*. In Press
Clinical Research
Body Weight and Insulin Resistance Indicators Among ChildrenMed Sci Monit In Press; DOI: 10.12659/MSM.951434
Clinical Research
Comparison of Radiographic Cervical Sagittal Alignment Parameters in Patients With Nonspecific Neck Pain, D...Med Sci Monit In Press; DOI: 10.12659/MSM.952950
Clinical Research
Combined Fibrinogen and Urinary α1-Microglobulin as Predictors of Respiratory Tract Infection in Children w...Med Sci Monit In Press; DOI: 10.12659/MSM.951066
Database Analysis
Evaluation of Salivary Total Oxidant Status (TOS) and Total Antioxidant Status (TAS) in Orthodontic Patient...Med Sci Monit In Press; DOI: 10.12659/MSM.952052
Most Viewed Current Articles
17 Jan 2024 : Review article 14,175,576
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,756,620
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,465,966
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,651
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387