24 August 2021: Clinical Research
Whole-Process Digitalization-Assisted Immediate Implant Placement and Immediate Restoration in the Aesthetic Zone: A Prospective Study
Xiaomei Han12ABCDEFG, Change Qi2C, Pengnv Guo2C, Shuying Zhang2B, Yali Xu2B, Guanghui Lv2A, Ying Li1AE*, Changyi LiDOI: 10.12659/MSM.931544
Med Sci Monit 2021; 27:e931544






Abstract
BACKGROUND: This study explored the clinical effects of whole-process digitalization (WD)-assisted immediate implant placement (IIP) and immediate restoration (IR) in the aesthetic zone and clarified the clinical procedures.
MATERIAL AND METHODS: Patients who received maxillary aesthetic region IIP and IR treatment were randomly distributed into WD-assisted and conventional groups. Postoperative assessment included implant accuracy, marginal bone loss, aesthetic evaluation, and patient satisfaction evaluation. The aesthetic evaluation included visual analog score (VAS), pink aesthetic score (PES), and white aesthetic score (WES). Numerical data, measurement data, and grade data were analyzed by χ² test, t test, and Mann-Whitney U test.
RESULTS: The WD-assisted group exhibited decreased implant accuracy, including coronal deviation, apical deviation, angular deviation, and depth deviation, compared with the conventional group (P<0.05). The marginal bone loss in both the mesiodistal direction and the buccolingual direction were significantly lower in the WD-assisted group than in the conventional group (P<0.05). The VAS, PES, and WES were all significantly higher in the WD-assisted group than in the conventional group at 3, 6, and 12 months after surgery (P<0.05). Patients in the WD-assisted group also reported a higher satisfaction level than those in the conventional group (P<0.05).
CONCLUSIONS: WD-assisted IIP and IR treatment in the aesthetic zone increased implant accuracy, decreased marginal bone loss, improved aesthetic effect, and increased patient satisfaction compared with conventional treatment. Therefore, WD-assisted IIP and IR treatment constitutes a promising approach in clinical oral implantology.
Keywords: Dental Implants, Dental Impression Technique, Dental Restoration, Temporary, Immediate Dental Implant Loading, Prospective Studies, Dentistry, Dental Implantation, Esthetics, Dental, Imaging, Three-Dimensional, Maxilla, Patient Satisfaction, Radiography, Surgery, Computer-Assisted, Time Factors
Background
Dental implantology is gaining increased popularity owing to developments in biomechanics, material science, mechanical design, and manufacturing technology during the past decades. It has become a routine method for the restoration of clinical dentition defects [1]. The conventional delayed placement method requires 3–6 months for healing before starting the restoration process [2–4]. Recently, treatment based on immediate implant placement (IIP) and immediate restoration (IR) has become popular in clinical dental implantation because it can effectively shorten the surgical procedure, reduce the number of visits, and achieve better outcomes [5].
At present, implant placement during IIP and IR treatment depends on preoperative X-ray or cone-beam computed tomography (CBCT) assessment, including bone height at the implant area and position of the lower alveolar nerve and maxillary sinus. Moreover, the traditional surgical method during implant insertion is based on a surgical guide and the doctor’s experience [6]. Due to deviation in the thickness of the surgical guide and variation in surgeon experience, the traditional method can result in an inconsistent angle or depth compared with the original design [7,8]. Such issues not only affect the function and stability of the implant, but also seriously affect the aesthetic outcome of the final restoration [7,9]. Therefore, increasing the accuracy and reducing the error of the implant angle and depth during IIP and IR are urgent goals.
In recent years, the application of digital technology in a variety of medical disciplines and for treatment of various diseases has gradually increased [10]. Through computer analysis and digitization, 2-dimensional images or data can be converted into 3-dimensional (3D) stereo images, and subsequent data analysis can enable accurate diagnosis, simulation, and surgical guidance [11]. Digital technology has been extensively applied in the treatment of oral diseases. In 2011, the first 3D printing-assisted transplantation of an artificial mandible was conducted in the Netherlands. The postoperative reestablishment of the patient’s language expression and masticatory function was better with the computer-assisted transplantation than the conventional method [12]. Additionally, several digital technologies have been used in oral implantology, such as 3D reconstruction, 3D printing [13], and digital impression. These successful examples indicate that digital technology can assist in oral implantology by providing 3D, intuitive, and accurate information of implant angle and depth. However, high-quality prospective clinical studies with large samples to compare clinical outcomes between digital medicine technology-assisted implantation and conventional implantation are still scarce. Previous studies related to digital technology-assisted implantation in the aesthetic zone were restricted to case reports [14] or only used digital impressions in the overall treatment [15]. Those studies compared the digital technology-assisted implantation with conventional implantation, but mainly focused on implant accuracy and aesthetic evaluation. They lacked evaluation of marginal loss and patient satisfaction, which the present study includes. In addition, the specific operation procedures of digital technology-assisted implantation are still unclear.
Briefly, in this prospective study, patients who received maxillary aesthetic region IIP and IR treatment were randomly divided into a conventional group and a whole-process digitalization (WD)-assisted group. The parameters related to implant accuracy, marginal bone loss, aesthetic parameters, and patients’ satisfaction were also assessed. Our study aimed to provide experimental evidence for the clinical application of WD-assisted implantation and to clarify surgical procedures.
Material and Methods
OVERALL STUDY DESIGN:
Sixty outpatients with failing teeth in the maxillary anterior aesthetic region who received IIP and IR treatment were randomly assigned to either the conventional group or the WD-assisted group. The parameters related to implant accuracy, including coronal deviation, apical deviation, angular deviation, and depth deviation (Figure 1), were evaluated. Aesthetic parameters, including visual analog score (VAS), pink aesthetic score (PES), and white aesthetic score (WES), were also recorded at 3, 6, and 12 months after surgery. In addition, marginal bone loss and patients’ satisfaction were also assessed.
PATIENT RECRUITMENT AND ALLOCATION:
The study enrolled 60 patients who received IIP and IR treatment at the Department of Oral Implantology, Affiliated Hospital of Chifeng University, Chifeng, Inner Mongolia. Random and single blind design was used to divide the patients into either the conventional group or the WD-assisted group (n=30 for each group). The conventional group received conventional IIP and IR treatments, while the WD-assisted group received WD-assisted IIP and IP treatment. A total of 52 and 50 implants were done in the conventional and WD-assisted groups, respectively. The surgery and evaluation procedures were independently conducted by different observers, who were blinded to each other.
SAMPLE SIZE CALCULATION:
Sample size calculation was done with statistical software (PASS®, version15.0, NCSS Inc., Kaysville, UT, USA). The calculation formula was based on the means and 95% study power, with the significance level (α) set at 0.05. The results of a previous study comparing accuracy deviation between designed and actual implant position, including coronal deviation, apical deviation, and angular deviation with computer-assisted surgery and free-hand implantation, were utilized for the sample calculation [16]. Based on the outcomes of the studies for 3D deviation at coronal (1.18±0.72 mm and 2.07±0.51 mm), apical (1.43±0.74 mm and 2.89±1.02 mm), and angular (4.21±1.91 mm and 8.84±4.64 mm) parameters and depth (0.54±0.29 mm and 0.78±0.33 mm), the required minimum sample size for the above-mentioned 4 parameters were 14, 11, 16, and 45 implants, respectively. Since aesthetic evaluation indexes (VAS, PES and WES), marginal bone loss, and patients’ satisfaction were novel parameters in our study that have not been studied before, the power calculation for these was only indirectly possible.
Inclusion criteria [17] for the current study were as follows: (1) implant site in the aesthetic area of the maxillary anterior teeth; (2) usable bone height of more than 3 mm in the extraction socket, without obvious soft or hard tissue defects; (3) no obvious inflammation at the periapical area of the implant site; (4) bone type from I to III in the Zarb bone density classification system; (5) stable centric occlusion, with normal overbite and overjet; and (6) good compliance by patient.
The exclusion criteria were as follows: (1) acute periodontal or periapical inflammation at the implant site; (2) soft tissue cellulitis around the diseased tooth; (3) nonideal root position and angle, with significant changes needed for the implant angle; (4) presence of systemic disease that would interfere with wound healing; (5) thin gingival biological type of periodontal biological tissue; (6) presence of poor oral habits such as smoking and grinding teeth that could not be corrected; and (7) implants torque below 35 N·cm and above 45 N·cm.
ETHICS APPROVAL:
All procedures involving human participants were in accordance with the ethical standards of the National Science and Technology Ethics Committee and with the 1964 Declaration of Helsinki and its later amendments. The study design was approved by the Clinical Scientific Research and Experimental Ethics Committee, Affiliated Hospital of Chifeng University (No. fsyy202014). All patients provided signed informed consent and consented to the study procedure.
WD-ASSISTED IIP AND IP TREATMENT:
For the WD-assisted group, patients received WD-assisted IIP and IP treatment, including preoperative preparation, IIP and IR treatment, soft tissue molding, and final restoration.
Preoperative preparation included examination and recording. Before surgery, clinical photographs (Figure 2A, 2B) were taken by digital camera (Canon®, EOS 70D, Canon, Inc., Tokyo, Japan). The CBCT images were obtained with a CBCT scanner (MORITA®, 3D Accuitomo 170, MORITA, Inc., Tokyo, Japan), with the patient holding their mouth open (Figure 2C). Then, a polyether impression-molded super-hard plaster model was made.
Next, the digital model and restoration design were established. We performed extraoral scanning of the super-hard plaster model with a digital dental scanner (Aidite®, A-ISPro, Aidite Co. Ltd., Qinhuangdao, PR China). The surface morphology of both the soft and hard tissues was then obtained for construction of the digital model and to confirm the occlusal relationship (Figure 2D). Afterward, the shape of the cervical margin of the restoration was designed with implant guide design software (3 Shape DentalSystem®, version 1.5.1.3, 3 Shape, Inc., Copenhagen, Denmark) according to the root shape of the contralateral homonymous teeth or the residual natural teeth. This step was intended to ensure that the cervical margin contour of the restoration would be consistent with the original natural teeth. According to the relationship between the normal dental arch radian and overjet, the 3D reconstruction of the restoration was performed according to the red and white aesthetics principles. Finally, we imported the patient’s facial photograph to confirm the effects of reconstructed restoration.
The next step was to design the implant position and construct the whole-process guide plate. Implant guide design software (3 Shape DentalSystem®, version 1.5.1.3) was used to register the CBCT data and model scan data. The data for the reconstructed restoration were transferred. According to the restoration-oriented implant design, the implant screw hole was designed to pierce through the lingual fossa of the crown. Then, the integrated image of the abutment crown restoration with screw retention was realized (Figure 2E, 2F). In addition, the whole-process guide plate was designed according to the information from the implant. Afterward, the guide plate was fabricated and the metal guide ring was installed into it.
The temporary implant-supported prostheses were designed according to the implant position data from the whole-process guide plate. The shape of the temporary crown was designed according to the aesthetic effect and occlusal relationship. The shape of the cervical margin was consistent with that of the natural tooth or the contralateral homonymous tooth, ensuring that the temporary restoration would seal the extraction socket after surgery. When 2 or more temporary crowns were made, the gingival embrasure was appropriately enlarged to provide space for postoperative soft tissue growth. The temporary crown (polymethyl methacrylate) was processed by cutting (Aidite®, cameoAV – D5, Aidite Co., Ltd.) and was bonded to the temporary abutment (OSSTEM®, Temporary Abutment, OSSTEM, Inc., Seoul, Korea).
During the IIP and IR operation, the root was extracted minimally without a flap to ensure the integrity of the alveolar bone wall. The implant cavity was prepared with the assistance of a guide plate, and the implant (OSSTEM®, Implant TSIII, OSSTEM Inc.) was inserted. The insertion torque was between 35 and 45 N∙cm. The implant and the labial bone wall had a gap of more than 2 mm, and the implant was placed with collagen bone (Geistlich®, Bio-oss Collagen, Geistlich, Inc., Bern, Switzerland). The temporary crown-abutment was placed in position. The restorations were adjusted to avoid centric, protrusive, and lateral occlusal interference. CBCT was done to check the implant position and orientation (Figure 3).
For soft tissue molding, the intactness of the temporary restoration was examined 4 months after surgery. The soft tissue, including the color, texture, and stability of the cervical margin position, were assessed. Moreover, whether a triangular gap was present between the gingival papilla was also examined. Afterward, the temporary crown was removed within 1 month and the cervical margin shape of the restoration was adjusted with resin for soft tissue molding. The soft tissue was re-examined 6 months after surgery. When the soft tissue shape was satisfactory and the position was stable, final restoration was undertaken (Figure 4).
For final restoration, the 3D position of the implant and the soft tissue cuff shape around the implant were recorded by a modified digital impression technique. First, the morphology of both soft and hard tissues in the mouth including the temporary crown was scanned (3 Shape DentalSystem®, Trios3, 3 Shape Inc., Copenhagen, Denmark). Second, the temporary restoration was removed and the scanning rod was put in. Third, the implant position in the mouth was scanned. Afterward, both the supragingival and subgingival shapes of the temporary restoration were scanned extra-orally. The 3 sets of data were registered through the clinical crown. Finally, the soft tissue cuff shape was generated based on the subgingival morphology of the temporary restoration. In this way, the 3D position of the implant and the soft tissue cuff shape around the implant were recorded accurately (Figure 5). The integrated zirconia base crown and inner crown were designed on the digital model. After the resin model was manufactured by 3D printing machine (Aidite®, AC-3, Aidite Co., Ltd.) and the porcelain veneer was completed on model, the final restoration was inserted into the mouth (Figure 6).
CONVENTIONAL IIP AND IP TREATMENT:
For the conventional group, patients received conventional IIP and IP treatment.
Before surgery, intraoral and facial digital photographs and a CBCT (same equipment as for the WD-assisted group) image were obtained. The alginate impression was prepared and a super-hard plaster model was poured. The artificial teeth were arranged according to the ideal arch curve, occlusal relationship, and overlay coverage. For comparison with the WD-assisted group, a model-scanning step was added to obtain data to match with the postoperative data. After the model was scanned extra-orally, the ideal positions of the implant and screw-retained temporary restoration were designed according to the restoration-oriented principle.
A simple surgical guide plate was made using the following process. A 2-mm-thick plastic film was formed on the plaster model with aligned artificial teeth by using a vacuum molding machine (Jintai®JT-18, Jintai Co., Ltd., Shanghai, P. R. China) to form the guide plate. The implant site guide plate was fenestrated along the lingual edge ridge of the restoration to reserve operation space for preparing the hole.
IIP in the conventional group was performed using a simple surgical guide plate. A minimally invasive tooth extraction method was employed as in the WD-assisted group. The implant cavity was prepared with the aid of a simple surgical guide plate. Implantation and bone grafting procedures were the same as those in the WD-assisted group. A polyether impression was made during the operation and a super-hard plaster model poured. Later, the model was sent to the technician’s room for temporary abutment selection and temporary restoration fabrication. The temporary restoration was composed of titanium temporary abutment and a plastic temporary crown, which were cemented to form an integral whole before being sent back to the dentist. Within 24 h after surgery, the integrated abutment-temporary crown restoration was put into the mouth with occlusion adjustment performed. Afterwards, the CBCT image was taken as in the WD-assisted group.
Soft tissue molding was similar to that in the WD-assisted group.
For final restoration, conventional impression technology was used to make a polyether impression and a super-hard model was poured. Then, the model was sent to the technician’s room for designing and making an all-ceramic restoration, which was put into the mouth using the same procedure as in the WD-assisted group.
IMPLANT ACCURACY:
The postoperative CBCT data of the 2 study groups were imported into STL file editing software (Materialise mimics®, version 20.0, Materialise, Inc., Leuven, Belgium) for comparison with the preoperative data. The deviation parameters of the implant, including coronal deviation, apical deviation, angular deviation, and depth deviation, were measured.
MARGINAL BONE LOSS:
The 3D model data conversion software Geomagic Wrap® (version 2017, Geomagic, Inc., Morrisville, NC, USA) was used to measure the bone height (BH) in the mesiodistal and buccolingual directions of each implant according to the CBCT images. BH values taken immediately after the operation (BH1) and 6 months after the operation (BH2) were recorded respectively. The measurements were repeated 3 times. Marginal bone loss (X) was calculated using the following equation: X=BH1–BH2.
AESTHETIC EVALUATION: The aesthetic evaluation was performed at 3, 6, and 12 months after surgery. Aesthetic parameters included VAS, PES [18], and WES [19]. VAS, PES, and WES evaluation were performed by 2 independent senior dentists and the measurement was repeated 3 times for each experiment.
For the VAS score, a 10-cm-long line was drawn on a paper, with 0 on the left end and 10 on the right end. Patients were asked to consider the degree of aesthetic effects and mark a value from 0 to 10 along the line. The marked value was recorded as the VAS value, which was based on 7 items, including tooth shape, tooth color, frontal view width ratio of the upper anterior teeth, central incisor width-length ratio, pronunciation test, smile curve, and overall satisfaction. The higher the value, the higher the degree of patient satisfaction.
The PES score was evaluated based on 5 items as follows: mesial gingival papilla, 0 points (missing), 1 point (incomplete), or 2 points (complete); distal gingival papilla, 0 points (missing), 1 point (incomplete), or 2 points (complete); the highest position of the gingival margin, 0 points (deviation ≥1 mm), 1 point (deviation ≤1 mm), or 2 points (same); gingival margin curve, 0 points (obviously inconsistent), 1 point (slightly inconsistent), or 2 points (coordinated); convexity/soft tissue color and texture, 0 points (noncoordinated in 2 or 3 aspects), 1 point (noncoordinated in 1 aspect), or 2 points (coordinated in 3 aspects). The total PES score was 10, and a higher score indicated better pink aesthetic effects.
The WES score was evaluated using the following 5 items: shape, volume, color, surface characteristics, and translucency of the crown. The scoring method was based on a comparison with the healthy teeth: 0 points (significant difference), 1 point (slight difference), and 2 points (no difference). The total WES score was 10, with a higher score indicating better white aesthetic effects.
PATIENT SATISFACTION:
Patient satisfaction was recorded at the end of follow-up and including 3 levels: satisfied, moderate, and unsatisfied. Patients were asked to freely score their degree of satisfaction with the treatment.
STATISTICAL ANALYSIS:
Statistical analysis was performed using statistics software (SPSS®, version 22.0, IBM, Inc., Chicago, IL, USA). Numerical data are presented as frequency (percentile) and were analyzed by χ2 test. The measurement data are presented as mean±standard deviation (SD). Independent
Results
CLINICAL CHARACTERISTICS OF THE STUDY SAMPLE:
A total of 60 patients were enrolled in the study and randomly distributed to the conventional group (n=30) or the WD-assisted group (n=30). The clinical characteristics of the study sample are presented in Table 1. There were no statistical differences for sex (P=0.79), age (P=0.26), body mass index (P=0.18), or restoration type (P=0.80) between the 2 study groups.
WD EFFECTIVELY IMPROVES THE ACCURACY OF IMPLANTATION:
The deviation values of actual implant position compared with the preoperative design position are displayed in Table 2 and Figure 7. In the analyses of the implant accuracy parameters, the WD-assisted group exhibited significantly lower coronal deviation (0.74±0.21 mm vs 0.87±0.39 mm, P=0.04) and apical deviation (0.81±0.16 mm vs 0.93±0.25 mm, P=0.01), compared with those of the conventional group. The WD-assisted group also displayed significantly lower angular deviation (2.17±0.92 mm vs 2.98±1.93 mm, P=0.01) and depth deviation (0.39±0.12 mm vs 0.48±0.20 mm, P=0.01) than those of the conventional group. These results indicate that the WD method could substantially improve implant accuracy.
WD DECREASED MARGINAL BONE LOSS:
The marginal bone loss values at 6 months after surgery compared with the postoperative baseline levels are displayed in Table 3. Both the mesiodistal and the buccolingual direction marginal bone loss values of the WD-assisted group were significantly lower than those of the conventional group (P<0.05).
WD INCREASED THE AESTHETIC EFFECTS:
At 3, 6, and 12 months after surgery, VAS, PES, and WES scores were used to evaluate the aesthetic effects between the 2 groups. As shown in Tables 4–6, gradual increases for all 3 scores were observed over the 1-year period for both groups. Notably, VAS, PES, and WES scores in the WD-assisted group were higher than those in the conventional group at all 3 postoperative time points (P<0.05). These results indicate that WD-assisted IIP and IR better promoted aesthetic effects, compared with the conventional IIP and IR method.
WD INCREASED PATIENT SATISFACTION:
Finally, a satisfaction survey was performed at 12 months after surgery to explore patients’ degree of satisfaction with conventional and WD-assisted IIP and IR treatments. As shown in Table 7, all patients in the WD-assisted group were satisfied with the WD-assisted IIP and IR treatment. However, only 66.7% of the patients in the conventional group were satisfied with the conventional IIP and IR treatment, with 26.6% of patients expressing dissatisfaction with the treatment. These results show that patients were more satisfied with the WD-assisted IIP and IR treatment, which had better treatment effects and preferable aesthetic effect.
Discussion
Traditional implant surgery requires patients to wait for more than 3 months after tooth extraction [20]. In addition, after the implant is inserted, another 3 months is required to achieve osseointegration before the restorative step. The long duration of treatment always brings serious aesthetic obstacles for patients, especially in the aesthetic zone [20]. The development of IIP and IR treatment has provided a solution to problems caused by delayed implant treatment. However, it is essential to act prudently when performing the IIP and IR treatment. For example, the IIP and IR treatment is not appropriate for patients with a thin gingiva biological type or a defect of the lateral labial plate. It has been reported that after IIP and IR treatment, the gingiva on the labial side may recede with inaccurate implantation and even cause exposure of the cervical margin of the implant, which will seriously affect the aesthetic effect and implant stability [21–23]. To solve such problems, digital-based IIP and IR treatment has attracted a large amount of attention. With the development of computer-aided design (CAD) and computer-aided manufacturing (CAM) technology, the application of digital technology in clinical practice continues to expand. In the field of dental implantation, CAD technology can accurately reconstruct 3D models of patients and enables dentists to design implants in 2 or 3 dimensions. Recently introduced intraoral scanners could provide additional support in the near future.
Digital technology offers good clinical accuracy and excellent patient feedback compared with conventional methods [24]. Additionally, 3D scanners are easily linkable with 3D printers or millers [25], thus allowing a completely digital workflow for various purposes. CAD/CAM prosthodontic materials show excellent mechanical properties [26] and good clinical durability [27]. With the assistance of digital technology, implant surgery can avoid important anatomical structures and allow adjustments to meet the requirements of bone mass and later restoration [28].
Gherlone et al [29] compared conventional impressions and digital impressions in 25 patients and found that the latter reduced the time needed to take impressions. Furthermore, the digital impressions could be repeated when necessary. Schepke et al [30] conducted a questionnaire survey of patients who underwent digital impressions and traditional impressions. Results showed that patients preferred digital impressions owing to their higher convenience and comfort. Mangano et al [31] reported that when taking optical impressions with intraoral scanning, it is difficult to detect deep marginal lines on prepared teeth or when bleeding occurs. However, these problems only exist for natural teeth and are not valid for dental implants, for which using scan bodies (coupled with CAD-related calculations) resolves all the problems. Owing to manufacturing errors, irregular extraction socket shape, and problems arising from free-hand surgery, conventional surgical procedures can lead to poor restoration shape, mechanical complications, poor self-cleaning ability, and other issues [32]. Vercruyssen et al [33] reported that the digital guide plate technology helped to determine the optimal 3D position of the implant in the software and helped control implant position precisely. In our study, with the development of CAM technology, the implant can be accurately implemented in surgery by constructing the 3D whole-process guide plate. Additionally, during final restoration, by using digital impression/printing technology, the contour of the perforating gingiva was accurately reproduced. Finally, the WD-assisted implantation exhibited significantly improved implant accuracy, including reduced coronal deviation, apical deviation, angular deviation, and depth deviation. WD-assisted implantation also significantly decreased marginal bone loss after operation. Compared with conventional implantation, WD-assisted implantation was not only more accurate, but also preserved the peri-implant bone tissue. Therefore, WD-assisted IIP and IR treatment is worth greater application in clinical practice. In short, the WD-assisted IIP and IR in the aesthetic zone are more efficient, accurate, and comfortable for patients, compared with the conventional method.
Marginal bone loss is an important index of implant healing. Marginal bone loss and soft tissue atrophy at the implant margin will cause implant failure and damage the aesthetic effect of the implant [34]. Immediate implants are performed immediately after tooth extraction. Researchers have concluded that immediate implantation is the best method to prevent marginal bone loss after tooth extraction, compared with traditional delayed implantation [35]. However, due to the difficulty of the operation, immediate implantation may not achieve the desired aesthetic effect. Our results showed that WD-assisted IIP and IR performed in the aesthetic zone can effectively promote aesthetic effects and decrease marginal bone loss compared with conventional treatment.
In addition, with the continuous improvement of people’s living standards, the evaluation of oral implants cannot be limited to the evaluation of implant stability and function. The aesthetic evaluation has increasingly become an important consideration. Relevant research shows that implant accuracy has a major impact on aesthetic effects because deviation in implant accuracy affects the subsequent aesthetic effects of restorations due to the impaired soft tissue shaping [36]. The current study evaluated the aesthetic effects using 3 indexes: VAS, PES, and WES. Our results showed that VAS, PES, and WES scores in the WD-assisted group were all significantly higher compared with the conventional group. With the aid of digitalization, an accurate 3D position of an implant can be achieved. Thus, not only can better aesthetics be achieved, but also peri-implant periodontal tissue tension can be reduced, which is conducive to oral cleaning to maintain excellent periodontal health.
A limitation of the present study is the lack of a cost assessment, which is of great significance. WD-assisted IIP and IR usually cost substantially more for the patient compared with the conventional method. The increased cost arises from the initial investment for technology purchase, training for the clinical team, and additional charges for the digital workflow in the clinic [37]. However, overall treatment cost could be reduced in cases in which WD-assisted implant placement prevents the need for bone augmentation surgery [9]. In the future, we intend to explore the cost-benefit ratio for patients who receive IIP and IR treatment [9]. Another limitation of the present work is that due to the limited number of patients, a multivariate analysis could not be performed to evaluate additional parameters, such as probing depth, clinical attachment level, and sulcus bleeding index. We intend to carry out relevant research in the future.
The present study has the advantage of evaluating the effects of the WD-assisted IIP and IR in the aesthetic zone from various aspects, including implant accuracy, marginal bone loss, aesthetic effects, and patient satisfaction level. Existing research only reports some of the above-mentioned parameters together [16,38]. The present work provides a multidimensional evaluation between conventional and WD-assisted IIP and IR treatment. Our study provides a basis for future research on WD-assisted IIP and IR in the aesthetic zone.
Conclusions
The findings of this prospective study revealed that the WD-assisted IIP and IR treatment exhibited higher accuracy of implants, less marginal bone loss, preferable aesthetic effects, and improved patient satisfaction level, compared with the conventional IIP and IP treatment. The present study further clarified the operation process of WD-assisted IIP and IR treatment, which deserves further clinical application.
Figures
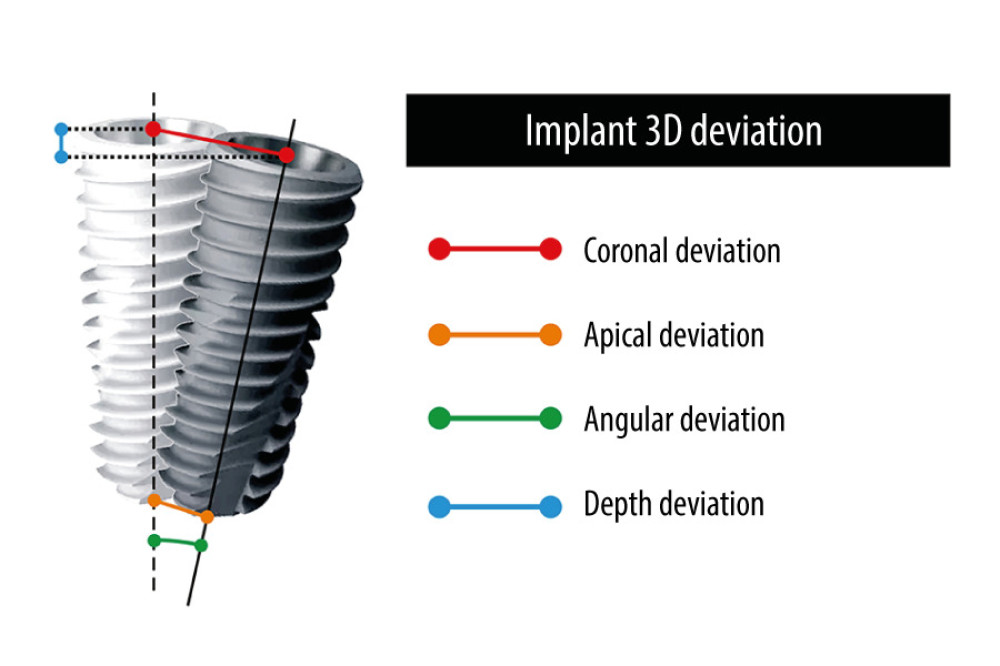 Figure 1. The accuracy evaluation analyzed by the implant 3-dimensional deviation between the designed and the actual implant position including coronal deviation, apical deviation, angular deviation, and depth deviation from the axis.
Figure 1. The accuracy evaluation analyzed by the implant 3-dimensional deviation between the designed and the actual implant position including coronal deviation, apical deviation, angular deviation, and depth deviation from the axis. 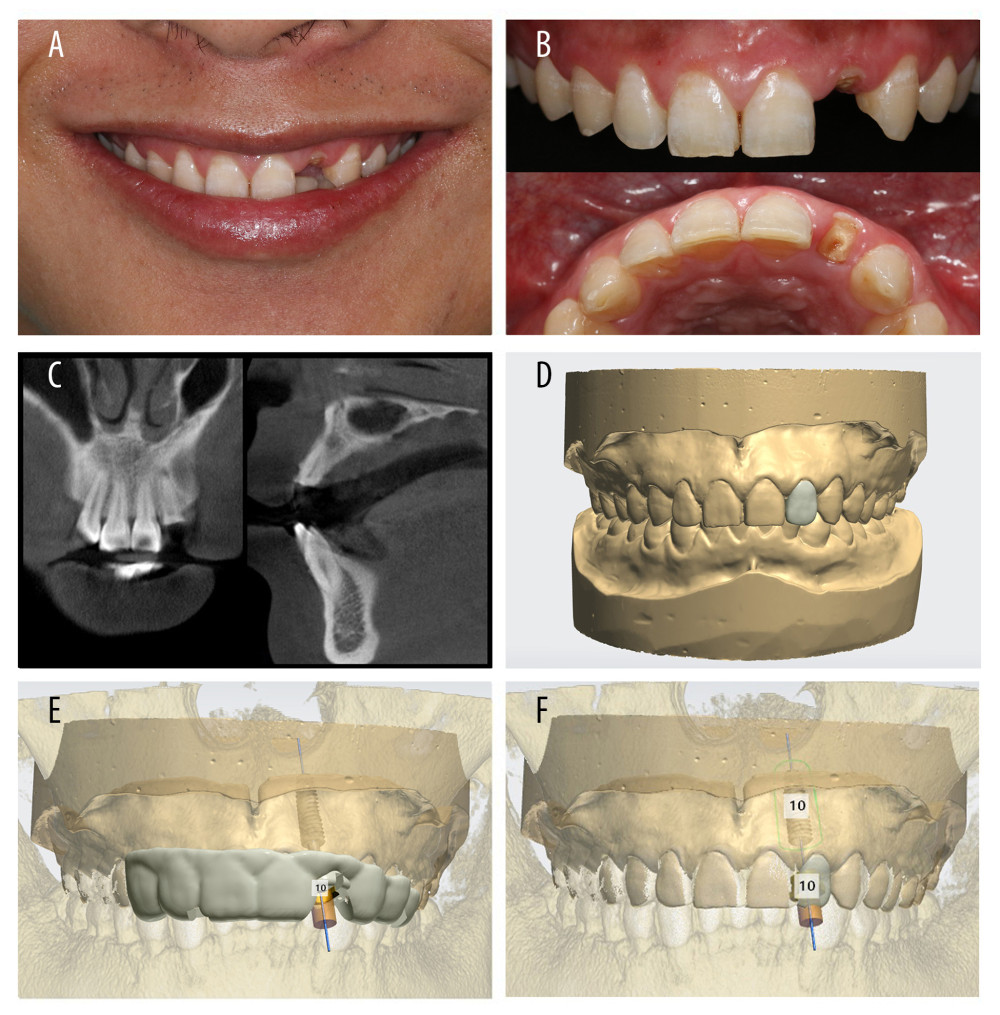 Figure 2. Preoperative preparation. (A) Preoperative photograph of patient with open mouth. (B) Preoperative intraoral image of patient. (C) Preoperative cone-beam computed tomography. (D) Construction of the digital model and design restoration. (E) Design of the implant position and guide plate for 3-dimensional printing. (F) Design of the temporary restoration.
Figure 2. Preoperative preparation. (A) Preoperative photograph of patient with open mouth. (B) Preoperative intraoral image of patient. (C) Preoperative cone-beam computed tomography. (D) Construction of the digital model and design restoration. (E) Design of the implant position and guide plate for 3-dimensional printing. (F) Design of the temporary restoration. 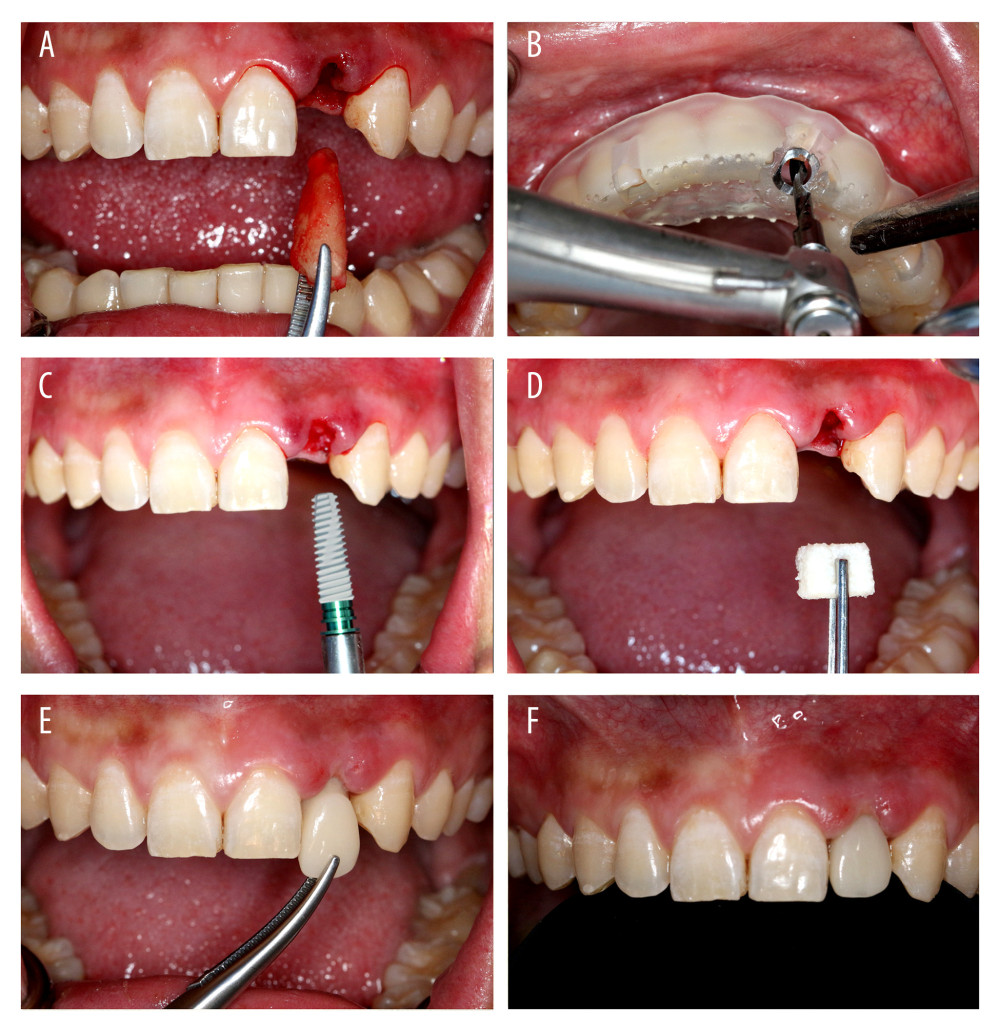 Figure 3. Immediate implant placement and immediate restoration. (A) Minimally invasive extraction without flaps. (B) Three-dimensional guide-assisted preparation of holes. (C) Implantation. (D) Implantation of collagen. (E) Insertion of temporary restorations. (F) Immediate restoration completed.
Figure 3. Immediate implant placement and immediate restoration. (A) Minimally invasive extraction without flaps. (B) Three-dimensional guide-assisted preparation of holes. (C) Implantation. (D) Implantation of collagen. (E) Insertion of temporary restorations. (F) Immediate restoration completed.  Figure 4. Intraoral image of soft tissue molding.
Figure 4. Intraoral image of soft tissue molding. 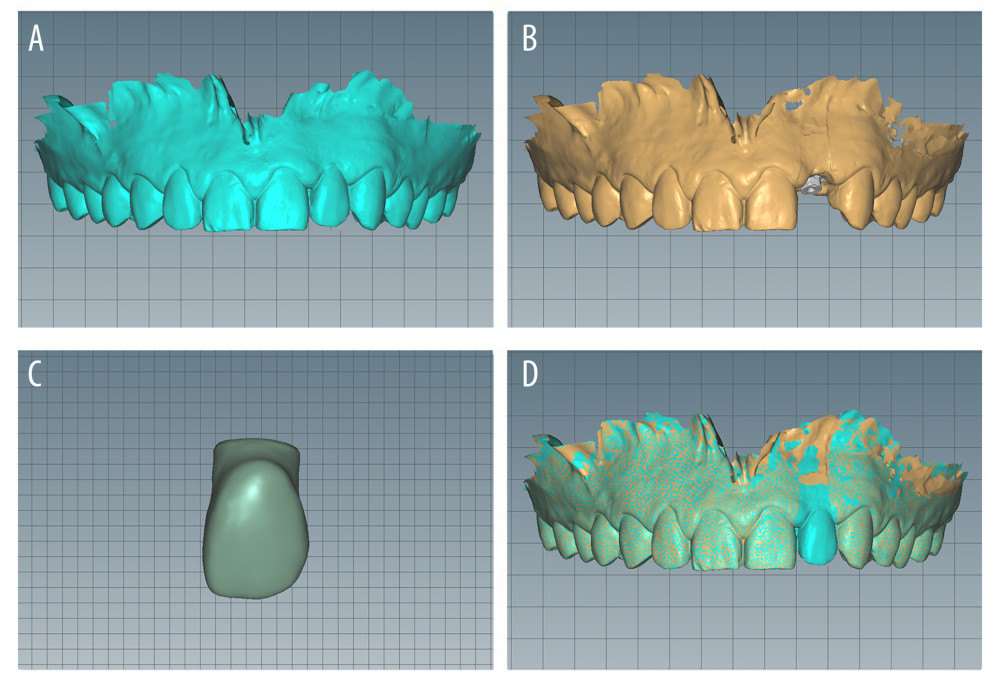 Figure 5. Obtaining the digital impression. (A) Intraoral scanning of the soft and hard tissues and the temporary crown. (B) Intraoral scanning of the implant position. (C) Extraoral scanning of the supragingival and subgingival shapes of the temporary restoration. (D) Generation of the soft tissue cuff shape based on the subgingival morphology of the temporary restoration
Figure 5. Obtaining the digital impression. (A) Intraoral scanning of the soft and hard tissues and the temporary crown. (B) Intraoral scanning of the implant position. (C) Extraoral scanning of the supragingival and subgingival shapes of the temporary restoration. (D) Generation of the soft tissue cuff shape based on the subgingival morphology of the temporary restoration 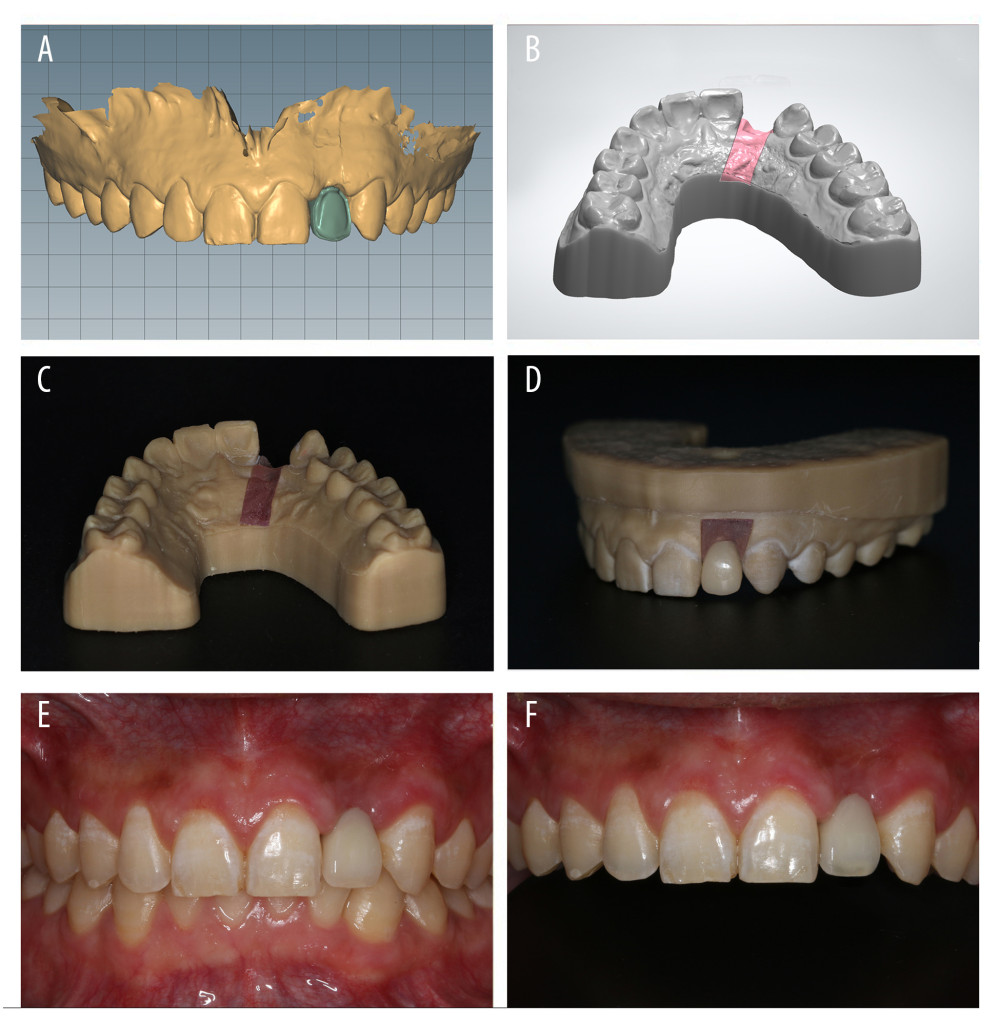 Figure 6. Final restoration. (A) Design of the inner crowns of restoration. (B) Digital impression of the model. (C) Three-dimensional printing of the manufactured model. (D) Final restoration on the model. (E) Front view of the intraoral image at the occlusal position. (F) Front view of the intraoral image at the occlusal position with a black background.
Figure 6. Final restoration. (A) Design of the inner crowns of restoration. (B) Digital impression of the model. (C) Three-dimensional printing of the manufactured model. (D) Final restoration on the model. (E) Front view of the intraoral image at the occlusal position. (F) Front view of the intraoral image at the occlusal position with a black background. 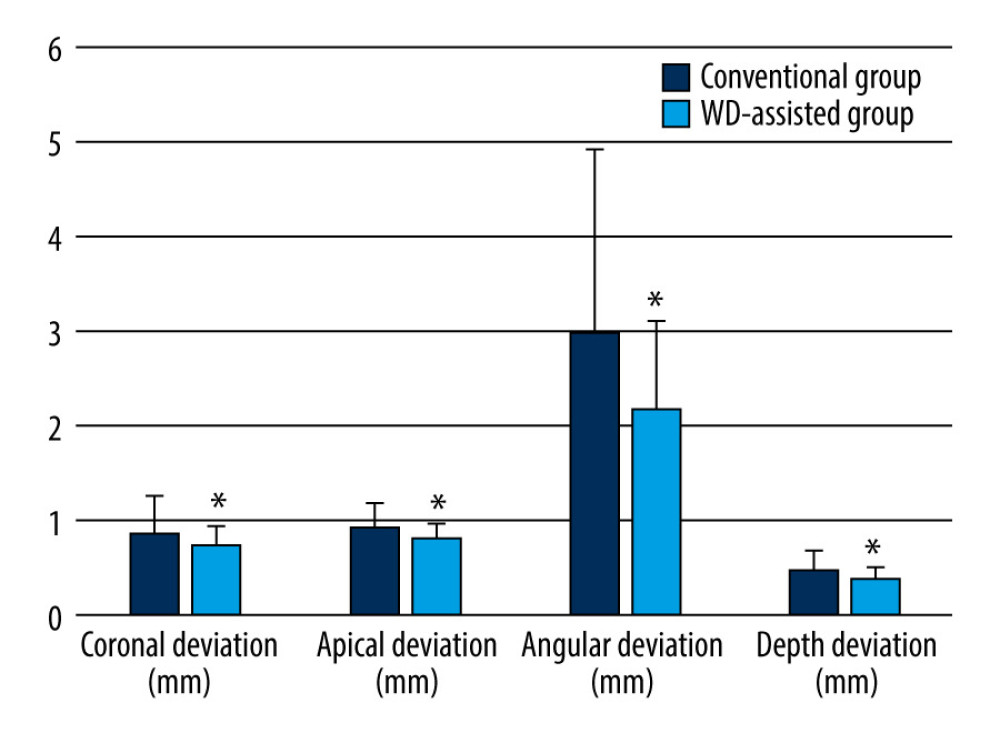 Figure 7. Accuracy evaluation between whole-process digitalization-assisted group and the conventional group.
Figure 7. Accuracy evaluation between whole-process digitalization-assisted group and the conventional group. Tables
Table 1. Clinical characteristics of the study sample. Table 2. The accuracy of implant between the 2 study groups.
Table 2. The accuracy of implant between the 2 study groups.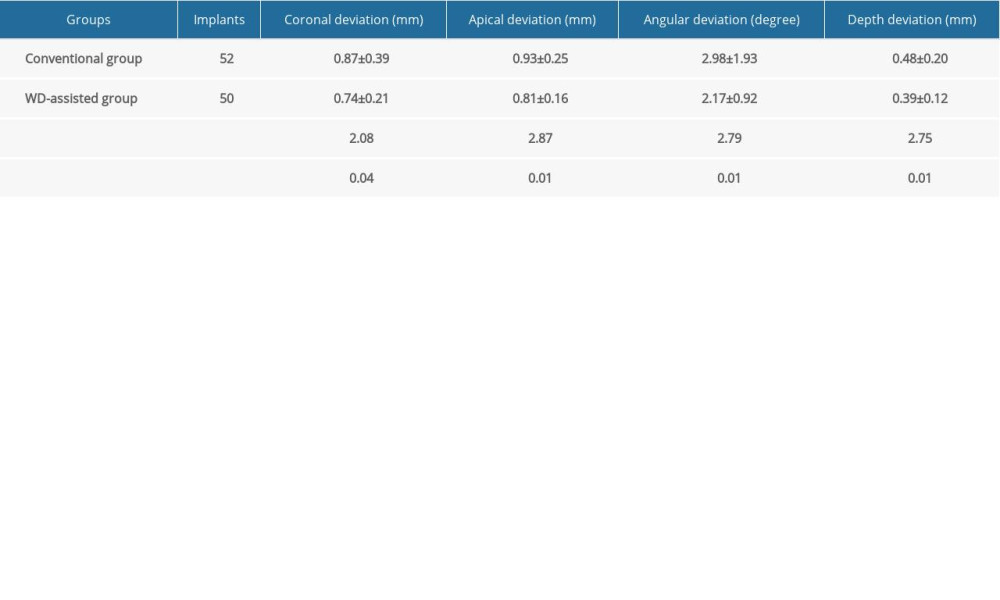 Table 3. Marginal bone loss between the 2 study groups.
Table 3. Marginal bone loss between the 2 study groups.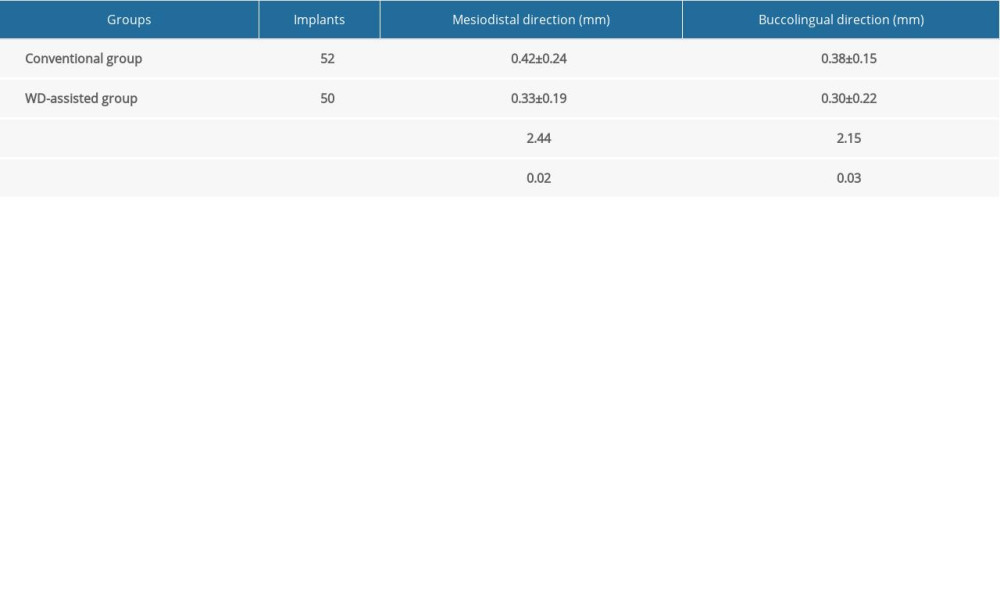 Table 4. Visual analog scores between the 2 study groups.
Table 4. Visual analog scores between the 2 study groups. Table 5. Pink aesthetic scores between the 2 study groups.
Table 5. Pink aesthetic scores between the 2 study groups.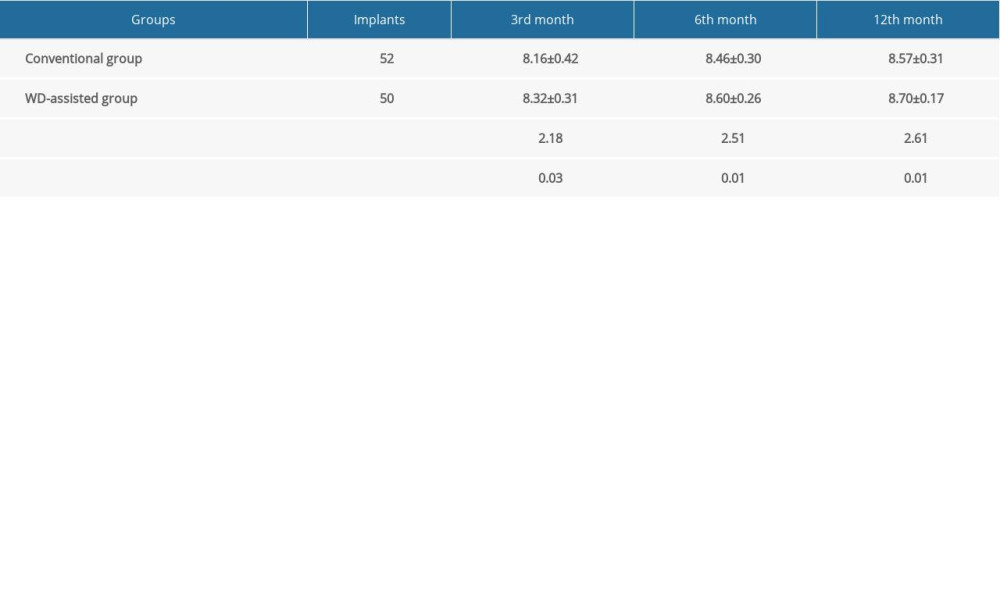 Table 6. White aesthetic scores between the 2 study groups.
Table 6. White aesthetic scores between the 2 study groups.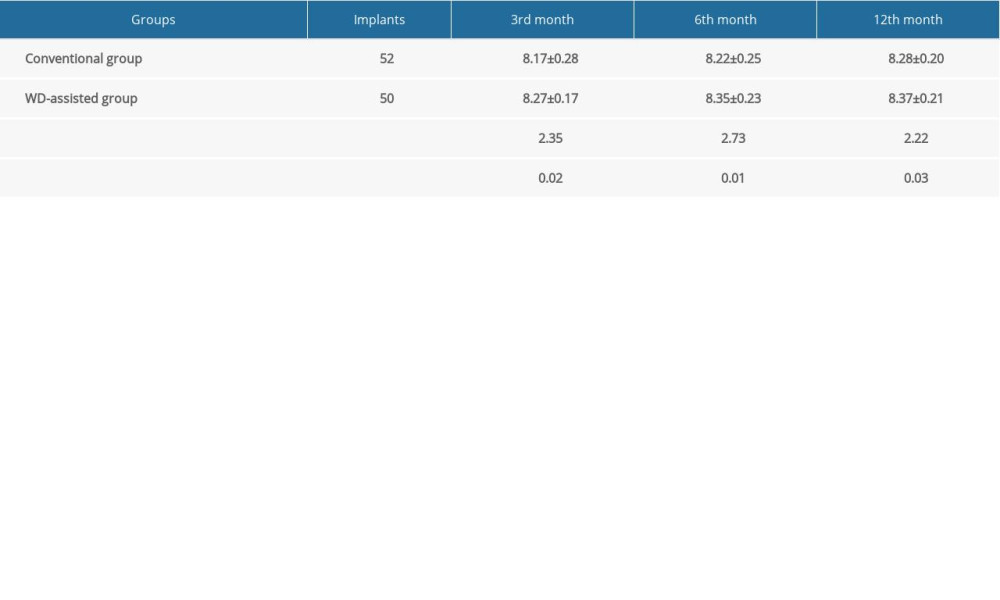 Table 7. Satisfaction survey at 12 months after surgery.
Table 7. Satisfaction survey at 12 months after surgery.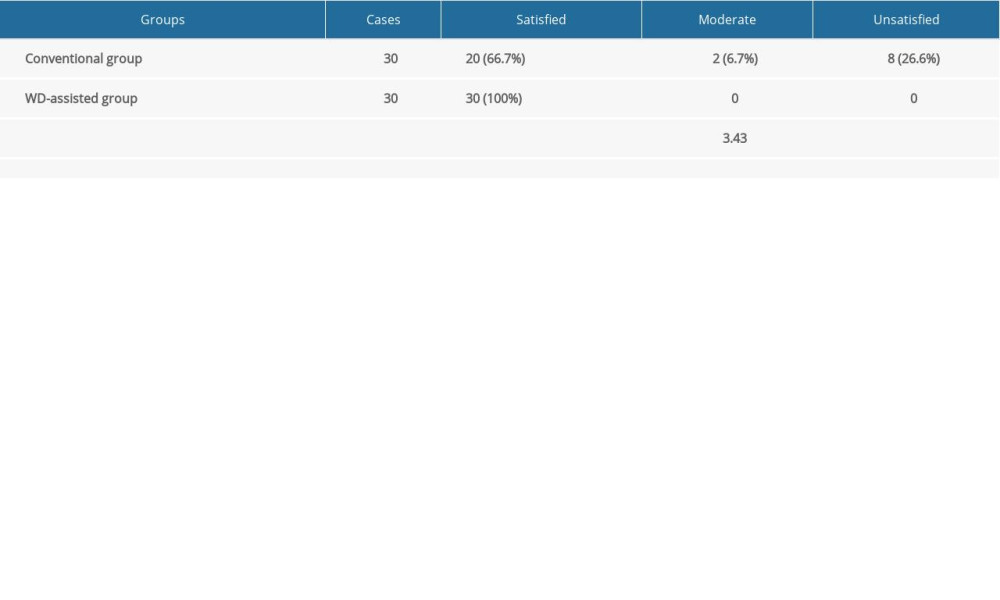
References
1. Sakkas A, Wilde F, Heufelder M, Autogenous bone grafts in oral implantology – is it still a “gold standard”? A consecutive review of 279 patients with 456 clinical procedures: Int J Implant Dent, 2017; 3; 1-17
2. Branemark PI, Hansson BO, Adell R, Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period: Scand J Plast Reconstr Surg, 1977; 16; 1-132
3. Buser D, Mericske-Stern R, Bernard JP, Long-term evaluation of non-submerged ITI implants. Part 1: 8-year life table analysis of a prospective multicenter study with 2359 implants: Clin Oral Implants Res, 1997; 8; 161-72
4. Szmukler-Moncler S, Piattelli A, Favero GA, Dubruille JH, Considerations preliminary to the application of early and immediate loading protocols in dental implantology: Clin Oral Implants Res, 2000; 11; 12-25
5. Becker W, Goldstein M, Immediate implant placement: treatment planning and surgical steps for successful outcome: Periodontol 2000, 2008; 47; 79-89
6. Geng W, Liu CY, Su YC, Accuracy of different types of computer-aided design/computer-aided manufacturing surgical guides for dental implant placement: Int J Clin Exp Med, 2015; 8; 8442-49
7. Wilk BL, Intraoral digital impressioning for dental implant restorations versus traditional implant impression techniques: Compend Contin Educ Dent, 2015; 36; 529-33
8. Patel K, Foschi F, Pop I, Patel S, Mannocci F, The use of intentional replantation to repair an external cervical resorptive lesion not amenable to conventional surgical repair: Prim Dent J, 2016; 5; 78-83
9. Marco C, Carlo M, Eitan M, Clinical applications and effectiveness of guided implant surgery: A critical review based on randomized controlled trials: BMC Oral Health, 2017; 17; 150
10. Egilman AC, Ross JS, Digital medicine systems: An evergreening strategy or an advance in medication management?: BMJ Evid Based Med, 2019; 24; 203-4
11. Pomero V, Mitton D, Laporte S, Fast accurate stereoradiographic 3D-reconstruction of the spine using a combined geometric and statistic model: Clin Biomech, 2004; 19; 240-47
12. Nickels L, World’s first patient-specific jaw implant: Metal Powder Report, 2012; 67; 12-14
13. Nyberg EL, Farris AL, Hung BP, 3D-printing technologies for craniofacial rehabilitation, reconstruction, and regeneration: Ann Biomed Eng, 2017; 45; 45-57
14. Arcuri C, Barlattani JRA, Mazzetti V, Immediate restoration of a single upper central integrating digital workflow and a novel dental implant: A case report: J Biol Regul Homeost Agents, 2019; 33; 171-77
15. Jiang X, Lin Y, Cui HY, Di P, Immediate loading of multiple splinted implants via complete digital workflow: A pilot clinical study with 1-year follow-up: Clin Implant Dent Relat Res, 2019; 33; 171-73
16. Shen P, Zhao J, Fan L, Accuracy evaluation of computer-designed surgical guide template in oral implantology: J Craniomaxillofac Surg, 2015; 43; 2189-94
17. Tymstra N, Raghoebar GM, Vissink A, Meijer HA, Dental implant treatment for two adjacent missing teeth in the maxillary aesthetic zone: A comparative pilot study and test of principle: Clin Oral Implants Res, 2011; 22; 207-13
18. Fürhauser R, Florescu D, Benesch T, Evaluation of soft tissue around single-tooth implant crowns: The pink esthetic score: Clin Oral Implants Res, 2005; 16; 639-44
19. Belser UC, Grütter L, Vailati F, Outcome evaluation of early placed maxillary anterior single-tooth implants using objective esthetic criteria: A cross-sectional, retrospective study in 45 patients with a 2- to 4-year follow-up using pink and white esthetic scores: J Periodontol, 2009; 80; 140-51
20. Lin Y, Current dental implant design and its clinical importance: West China J Stomatol, 2017; 35; 18-28
21. Slagter KWA PhD completed 1 Immediate dental implant placement in the aesthetic zone: Ned Tijdschr Tandheelkd, 2016; 123; 264-65 [in Dutch]
22. Cosyn J, Eghbali A, Hermans A, A 5-year prospective study on single immediate implants in the aesthetic zone: J Clin Periodontol, 2016; 43; 702-9
23. Graauwmans FEJ, Staas TA, Groenendijk E, Meijer GJImmediate front implant placements 2 Objective and subjective aesthetic treatment results: Ned Tijdschr Tandheelkd, 2015; 122; 193-98 [in Dutch]
24. Sfondrini MF, Gandini P, Malfatto M, Computerized casts for orthodontic purpose using powder-free intraoral scanners: Accuracy, execution time, and patient feedback: Biomed Res Int, 2018; 2018; 4103232
25. Luo D, Li T, Wang H, Chen Y, Three-dimensional printing of personalized nasal stents for patients with cleft lip: Cleft Palate Craniofac J, 2018; 56; 521-24
26. Colombo M, Poggio C, Lasagna A, Vickers micro-hardness of new restorative CAD/CAM dental materials: Evaluation and comparison after exposure to acidic drink: Materials (Basel), 2019; 12; 1246
27. Pyo SW, Kim DJ, Han JS, Yeo IL, Ceramic materials and technologies applied to digital works in implant-supported restorative dentistry: Materials (Basel), 2020; 13; 1964
28. Finelle G, Lee SL, Guided immediate implant placement with wound closure by computer-aided design/computer-assisted manufacture sealing socket abutment: Case report: Int J Oral Maxillofac Implants, 2017; 32; e63-67
29. Gherlone E, Capparé P, Vinci R, Conventional versus digital impressions for “All-on-Four” restorations: Int J Oral Maxillofac Implants, 2016; 31; 324-30
30. Schepke U, Meijer HJ, Kerdijk W, Cune MS, Digital versus analog complete-arch impressions for single-unit premolar implant crowns: Operating time and patient preference: J Prosthet Dent, 2015; 114; 403-6
31. Mangano F, Gandolfi A, Luongo G, Logozzo S, Intraoral scanners in dentistry: A review of the current literature: BMC Oral Health, 2017; 17; 149
32. Schlund M, Raoul G, Ferr J, Nicot R, Mandibular osteomyelitis following implant placement: J Oral Maxillofac Surg, 2017; 75; 2560-67
33. Vercruyssen M, Laleman I, Jacobs R, Quirynen M, Computer-supported implant planning and guided surgery: A narrative review: Clin Oral Implants Res, 2015; 26; 69-76
34. Galindo-Moreno P, León-Cano A, Ortega-Oller I, Marginal bone loss as success criterion in implant dentistry: beyond 2 mm: Clin Oral Implants Res, 2014; 26; e28-34
35. Sanda M, Fueki K, Bari PR, Baba K, Comparison of immediate and conventional loading protocols with respect to marginal bone loss around implants supporting mandibular overdentures: A systematic review and meta-analysis: Jpn Dent Sci Rev, 2019; 55; 20-25
36. Singer LD, The importance of immediate bone block autograft to successfully restore the function and aesthetic of the anterior alveolar process and teeth: J Oral Implantol, 2015; 41; 684-91
37. Laleman I, Bernard L, Vercruyssen M, Guided implant surgery in the edentulous maxilla: A systematic review: Int J Oral Maxillofac Implants, 2016; 31; s103-17
38. Palita S, Keskanya S, Nikos M, Atiphan P, The accuracy of single-tooth implants placed using fully digital-guided surgery and freehand implant surgery: J Clin Periodontol, 2019; 46; 949-57
Figures
Figure 1. The accuracy evaluation analyzed by the implant 3-dimensional deviation between the designed and the actual implant position including coronal deviation, apical deviation, angular deviation, and depth deviation from the axis.Figure 2. Preoperative preparation. (A) Preoperative photograph of patient with open mouth. (B) Preoperative intraoral image of patient. (C) Preoperative cone-beam computed tomography. (D) Construction of the digital model and design restoration. (E) Design of the implant position and guide plate for 3-dimensional printing. (F) Design of the temporary restoration.Figure 3. Immediate implant placement and immediate restoration. (A) Minimally invasive extraction without flaps. (B) Three-dimensional guide-assisted preparation of holes. (C) Implantation. (D) Implantation of collagen. (E) Insertion of temporary restorations. (F) Immediate restoration completed.Figure 4. Intraoral image of soft tissue molding.Figure 5. Obtaining the digital impression. (A) Intraoral scanning of the soft and hard tissues and the temporary crown. (B) Intraoral scanning of the implant position. (C) Extraoral scanning of the supragingival and subgingival shapes of the temporary restoration. (D) Generation of the soft tissue cuff shape based on the subgingival morphology of the temporary restorationFigure 6. Final restoration. (A) Design of the inner crowns of restoration. (B) Digital impression of the model. (C) Three-dimensional printing of the manufactured model. (D) Final restoration on the model. (E) Front view of the intraoral image at the occlusal position. (F) Front view of the intraoral image at the occlusal position with a black background.Figure 7. Accuracy evaluation between whole-process digitalization-assisted group and the conventional group. Tables
Table 1. Clinical characteristics of the study sample.Table 2. The accuracy of implant between the 2 study groups.Table 3. Marginal bone loss between the 2 study groups.Table 4. Visual analog scores between the 2 study groups.Table 5. Pink aesthetic scores between the 2 study groups.Table 6. White aesthetic scores between the 2 study groups.Table 7. Satisfaction survey at 12 months after surgery.Table 1. Clinical characteristics of the study sample.Table 2. The accuracy of implant between the 2 study groups.Table 3. Marginal bone loss between the 2 study groups.Table 4. Visual analog scores between the 2 study groups.Table 5. Pink aesthetic scores between the 2 study groups.Table 6. White aesthetic scores between the 2 study groups.Table 7. Satisfaction survey at 12 months after surgery. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387