12 November 2021: Clinical Research
A Retrospective Study of the Risk Factors for Postoperative Foot or Ankle Pain in 90 Patients with Varus Osteoarthritis of the Knee who Underwent Total Knee Arthroplasty
Li-Jie Wu1ABCF, Shi-Gang JiangDOI: 10.12659/MSM.932796
Med Sci Monit 2021; 27:e932796






Abstract
BACKGROUND: The reasons for foot and ankle pain following total knee arthroplasty (TKA) for knee varus osteoarthritis are unknown. This retrospective study aimed to investigate the risk factors for postoperative foot and ankle pain in patients with varus osteoarthritis of the knee who underwent TKA.
MATERIAL AND METHODS: We enrolled 90 patients who underwent TKA for varus knee osteoarthritis. The visual analog scale (VAS) was used to evaluate patients’ foot or ankle pain before and after surgery. The correlation between independent variables (eg, age, sex, body mass index [BMI], ankle osteoarthritis, and varus angle) and foot and ankle pain in patients with osteoarthritis of the knee was measured. Moreover, radiological changes were compared between the groups with and without worsened pain.
RESULTS: No significant difference in VAS was found between patients <60 and ≥60 years of age (P>0.05). Male sex and BMI <30 kg/m² were weakly correlated with preoperative foot or ankle pain. However, patients with varus of ≥6° and preexisting ankle osteoarthritis had a higher incidence of foot or ankle pain before surgery. Moreover, no significant differences in radiological changes were found between the groups with and without worsened foot or ankle pain after surgery (P>0.05).
CONCLUSIONS: In male patients with osteoarthritis of the knee, a BMI <30 kg/m², varus of <6°, and no preexisting ankle osteoarthritis were protective factors for foot and ankle pain. TKA corrected knee and ankle malalignment. Therefore, postoperative foot and ankle pain was not associated only with TKA surgery.
Keywords: Age Factors, Arthroplasty, Replacement, Knee, Pain, Aged, 80 and over, Ankle, Body Mass Index, Female, Foot, Humans, Male, Osteoarthritis, Knee, Pain, Postoperative, Patient Acuity, Risk Factors, Sex Factors
Background
Total knee arthroplasty (TKA) is an effective surgical method used to treat advanced osteoarthritis of the knee [1,2]. In most patients, joint function can be reestablished and pain can be alleviated through the correction of lower extremity malalignment [3,4]. TKA surgery can achieve normal alignment of the lower extremity in a 3-dimensional plane, including the axial, sagittal, and coronal planes, by the accurate installation of the prosthesis [5]. However, recent studies have shown that a change in the level of knee alignment affects the foot and ankle joints and induces adverse clinical symptoms, such as foot and ankle pain [6,7].
In orthopedic medicine, foot and ankle pain are common clinical symptoms that can influence movement and affect patient quality of life [8–10]. The pain can be further divided into ankle pain, forefoot pain, hindfoot pain, and multiple pain [11]. The common etiologies of foot and ankle pain including ligament injury [12], peroneal tendon disorders [12], neural causes [8], and bony causes [13]. The uncommon causes of foot and ankle pain are infectious tenosynovitis of the tibialis anterior tendon [14], transient osteoporosis [15], and complex regional pain syndrome [16]. In recent years, foot or ankle pain following TKA has received increasing attention from orthopedic specialists worldwide [6,7,17,18]. We hypothesized that, in addition to changes in the lower extremity’s mechanical axis after TKA, patient age, sex, body mass index (BMI), genu varus severity, and the presence of preoperative ankle osteoarthritis might also be associated with postoperative foot and ankle pain.
However, the related risk factors of foot and ankle pain following TKA are still not elucidated. Furthermore, there is no consensus concerning the prevention of foot and ankle pain following TKA. It is essential to estimate the related risk indicators of foot and ankle pain following TKA in patients with osteoarthritis of the knee to help with diagnosis, decision making, and pain control. Therefore, this retrospective study aimed to investigate the risk factors for postoperative foot or ankle pain in 90 patients with varus osteoarthritis of the knee who underwent TKA.
Material and Methods
ETHICS APPROVAL:
Ethics approval for the study was obtained from the Ethics Committee of the Third Hospital of Hebei Medical University. Consent was obtained from all patients.
INCLUSION AND EXCLUSION CRITERIA:
From January 2017 and October 2019, a total of 90 consecutive patients who received TKA surgery in the Third Hospital of Hebei Medical University were retrospectively studied. The inclusion criteria were as follows: (1) radiological findings suggested varus osteoarthritis of the knee; (2) patient was symptomatic due to osteoarthritis of the knee; (3) full-length standing anteroposterior radiographs of bilateral lower extremities were performed before and after surgery; (4) unilateral TKA was performed. The exclusion criteria were as follows: (1) radiological findings were unclear or the patients did not have full-length preoperative or postoperative standing anteroposterior images; (2) patient had undergone previous ankle surgery or had a medical history of ankle injury; (3) patient had received revision TKA, uni-compartmental knee arthroplasty, or other knee surgeries [18].
PAIN EVALUATION:
All patients’ visual analog scale (VAS) scores were evaluated before surgery and 1, 3, 6, and 12 months after surgery. A previous study categorized foot and ankle pain into ankle pain, forefoot pain, hindfoot pain, and multiple pain [11]. In this study, we used the term “foot and ankle pain” for any of these types of pain. When there were definite focal tenderness and VAS score ≥1, pain was considered to exist. For instance, hindfoot pain was considered when pain beyond the calcaneus (Achilles insertion sites, plantar fascia, and subtalar joint) with a VAS score of 4. Forefoot pain was considered when there was tenderness about the toes (metatarsal, tarsal bones, and metatarsophalangeal joint) with a VAS score of 3. Ankle pain was considered when there was medial joint line tenderness with a VAS score of 1.
RADIOGRAPHIC ASSESSMENT:
All patients received the same surgical strategies performed by our corresponding author. Two trained surgeons, who were blinded to the purpose of the study, independently measured the selected angles from the picture archiving and communication system (Beijing Tianjian Yuanda Technology Co., Ltd., China). The 2 surgeons independently performed the quality evaluation and data extraction. If the measured results were consistent, the data were considered valid. However, if the measurement results were inconsistent, the 2 surgeons needed to remeasure the data until a consensus was reached [18].
The center of the femoral head was determined using the Moses circles method [19]. The femur and tibia mechanical axes were defined as a line from the center of the femoral head to the center of the knee and a line from the center of the tibial plateau to the center of the ankle, respectively. Normal alignment of the lower limb was considered when the mechanical axis passed through the hip, knee, and ankle midpoints in a straight line. The midpoint of the knee was represented by the center of the femoral condyle at the top of the intercondylar notch. The center of the ankle was defined as the midpoint of the talus joint surface [20]. The hip-knee-ankle angle (HKA) (Figure 1A), lateral tibial angle (LTA) (Figure 1B), medial angle of the proximal tibia (MAPT) (Figure 1C), tibia anterior surface angle (TASA) (Figure 2A), tibia talar surface angle (TTSA) (Figure 2B), talar tilt angle (TTA) (Figure 2C), the angle between the ground and the upper surface of talus (GS) (Figure 2D), medial ankle joint space (MAJS) (Figure 2E), and medial ankle clear space (MACS) (Figure 2F) were measured.
Varus deformity severity was estimated by the HKA, with an HKA of ≥3° considered varus knee deformity [21–23]. The HKA was calculated using the angle between the mechanical axes of the tibia and femur. The tibiotalar joint alignment was assessed with the TTSA [22,23] and was measured through the angle between the talus upper surface and tibia anatomical axis. Moreover, the TTA, GS, MAJS, and MACS were used to evaluate the ankle changes before and after surgery.
GROUPING DESIGN:
Subgroups were determined using the following demographic and radiographic factors: age at surgery (<60 years, ≥60 years), sex (female, male), BMI (BMI <25 kg/m2, BMI 25–30 kg/m2, BMI ≥30 kg/m2), varus (<6°, 6–10°, ≥10°), and preexisting ankle osteoarthritis (yes or no). Subsequently, the preoperative foot or ankle pain of patients with osteoarthritis of the knee was compared within each of 5 groups. Following TKA, the groups with and without worsened foot or ankle pain were established to investigate the correlation between ankle radiological changes and foot or ankle pain. Changes before and after surgery were calculated as follows: Δ radiological changes=preoperative angle–postoperative angle. For example, Δ HKA=preoperatively HKA–postoperative HKA. All data, including age, sex, BMI, varus angle, and whether patients had preexisting ankle osteoarthritis, were collected from clinical records and radiograph findings (Table 1).
STATISTICAL ANALYSIS:
The chi-squared test was used for comparison between groups. Logistic regression analysis was used to determine the connection between ankle pain following TKA and the independent variables. Changes in HKA, LTA, MPTA, TASA, TTSA, TTA, GS, MAJS, and MACS were compared using a paired
Results
Ninety patients were included, with 16 men and 74 women aged 66.3±6.3 years (range, 51 to 82 years). Mean BMI values of 27.7±3.2 kg/m2 (range, 18.99 to 37.04 kg/m2) were obtained. The mean follow-up duration was 23 months.
The chi-squared test results revealed no significant difference between patients <60 years and ≥60 years (
There were no significant differences in TASA, TTSA, and MACS before and after surgery (
Discussion
The present findings indicated that knee preoperative malalignment was corrected significantly, whereby the MAJS and MACS were improved on the operated side following TKA. An essential finding in the current study was that various risk factors, including female sex, high BMI, varus of ≥6°, and preexisting ankle osteoarthritis, increased the incidence of foot and ankle pain in patients with osteoarthritis of the knee. Several previous studies have described the association between knee and ankle malalignment after TKA [2,6,11,17,18,24–26]. Nonetheless, few authors have investigated the risk factors associated with foot or ankle pain in patients with osteoarthritis of the knee, to the best of our knowledge. Misdiagnosis and mistreatment of foot or ankle pain can lead to serious complications and impair physical function. Accordingly, understanding the relationships between risk factors and foot and ankle pain is essential to prevent postoperative surgical complications. We hypothesized that risk factors, including surgical age, sex, BMI, varus severity, and preexisting ankle osteoarthritis, might be associated with foot and ankle pain following TKA. Herein, we retrospectively studied 90 patients to evaluate the risk indicators of foot or ankle pain following TKA in patients with osteoarthritis of the knee to help with diagnosis, decision making, and pain control.
In this study, we found that age did not significantly influence foot or ankle pain in patients with osteoarthritis of the knee (Table 1). To date, it has not been established whether age is a risk factor for foot or ankle pain after TKA. As a risk factor of advanced knee osteoarthritis, age could affect patient satisfaction with TKA, according to previous studies [27,28]. The patient-reported dissatisfaction rate of TKA has ranged from 11% to 25% in past decades [29,30]. At present, the relationship between age and pain is controversial. Numerous authors believe that elderly patients have a high pain threshold, especially women [31,32]. Moreover, elderly patients are believed to be less susceptible to the experience of pain because the somatosensory pain system and immune system change with age [33]. Lautenbacher et al [34] suggested that aging can reduce pain sensitivity for lower pain intensities. However, Molton et al [35] reported that age could bring various pains, such as musculoskeletal, chronic joint, osteoarthritic back, and peripheral neuropathic pain. Therefore, in our view, clinicians should fully consider the risk factors of foot and ankle pain in patients with osteoarthritis. Mullaji et al [24] reported that age is not a risk factor for postoperative limb mechanical axis malalignment, suggesting that age is not associated with postoperative foot and ankle pain. In the present study, elderly patients had a higher incidence of foot or ankle pain in osteoarthritis of the knee (
Regarding patient sex, we found that women were more likely to have a foot or ankle pain than were men (35.85% vs 8.11%,
Obesity is considered a global public health crisis [41–43]. China has the largest affected population globally, with approximately 46% of adults and 15% of children with overweight or obesity [43]. Obesity is also a demographic factor that is increasingly common in patients undergoing TKA [44]. No significant difference was found between the BMI <24 kg/m2 group and the 24≤ BMI <30 kg/m2 group (
Preexisting ankle osteoarthritis is frequently found on X-ray fluoroscopic for some patients with knee osteoarthritis who are symptomatic. However, ankle osteoarthritis prevalence is lower than that of knee osteoarthritis. In the present study, 17 of 90 (19%) patients had both knee and ankle osteoarthritis (Table 1), a finding that was similar to that of 4, who reported that one-third of patients experienced both knee and ankle osteoarthritis. Numerous authors have reported that osteoarthritis of the knee is a common factor inducing pain and disability in the elderly population [53,54]. However, studies evaluating the correlation between foot and ankle pain and preexisting ankle osteoarthritis are scarce. In the present study, the preexisting ankle osteoarthritis group had a higher level of foot or ankle pain than did the group without preexisting ankle osteoarthritis (
The severity of preoperative knee deformity in relation to the ankle and foot stability after TKA has received increasing attention. Numerous reasons for foot or ankle pain following TKA have been reported, including overcorrecting the tilt of the distal tibia plafond and ankle alignment [25], residual varus in the knee [2], and unbalanced lower extremities with genu varum [11]. Nevertheless, retrospective studies of the influence of varus angle on foot and ankle pain after TKA are extremely uncommon. In the present study, the varus of ≥6° group had a higher incidence of foot or ankle pain than did the varus of <6° group (
The issues concerning preoperative and postoperative radiological factor changes and whether TKA can cause foot or ankle pain are hot topics in orthopedic medicine. We found that HKA was significantly improved after surgery, compared with before surgery (
Although the risk factors for foot or ankle pain following TKA were evaluated objectively, comprehensively, and scientifically in this study, the study still has many limitations. First, this was a was a single-center retrospective study with a small sample size, and the proportion of men and women in the study participants was not equal. These factors may have led to bias in the study results. Therefore, multi-center randomized controlled trials with a similar sex ratio and a larger sample size should be conducted. Second, the results may not be applicable to other populations, owing to racial differences. Third, the participants in this study were patients with osteoarthritis of the knee with genu varus. Consequently, the results may not be applicable to genu valgus. Finally, individuals differ in their sensitivity to pain, while VAS scores are primarily based on individual subjective feelings. Therefore, there may be errors in the VAS score.
Conclusions
The findings of this study showed that in male patients with osteoarthritis of the knee, a BMI <30 kg/m2, varus of <6°, and no preexisting ankle osteoarthritis were protective factors for foot and ankle pain. TKA corrected knee and ankle malalignment. Therefore, postoperative foot or ankle pain was not associated only with TKA surgery.
Figures
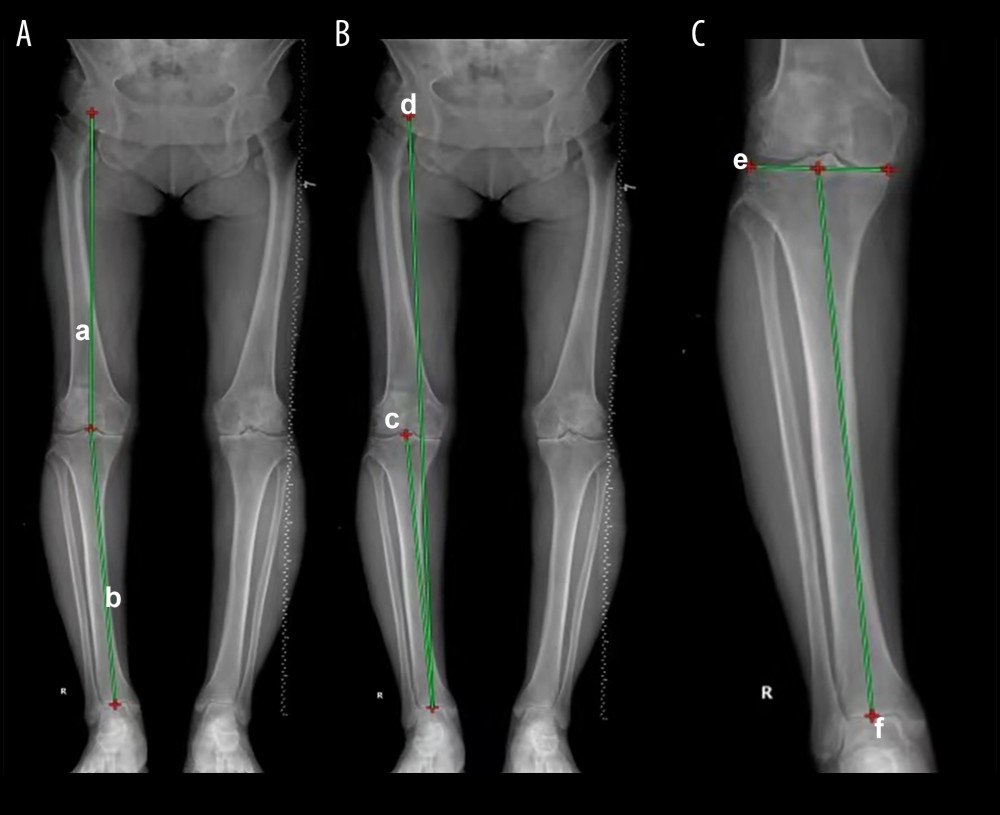 Figure 1. Measurement of hip-knee-ankle angle (HKA) and ankle parameters based on full-leg standing anteroposterior radiographs. HKA was defined as the medial angle between (a) and (b) (A). Lateral tibial angle was defined as the medial angle between (c) and (d) (B). Medial angle of the proximal tibia was defined as the lateral angle between (d) and (f) (C).
Figure 1. Measurement of hip-knee-ankle angle (HKA) and ankle parameters based on full-leg standing anteroposterior radiographs. HKA was defined as the medial angle between (a) and (b) (A). Lateral tibial angle was defined as the medial angle between (c) and (d) (B). Medial angle of the proximal tibia was defined as the lateral angle between (d) and (f) (C). 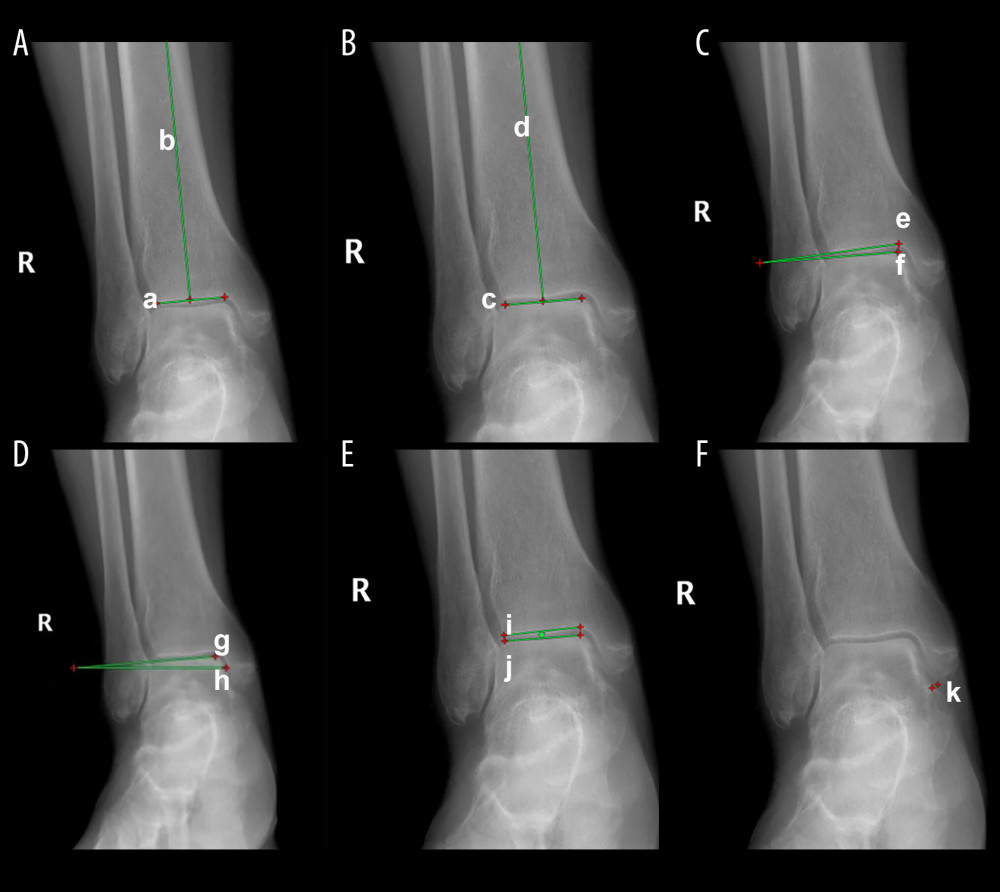 Figure 2. The tibia anterior surface angle was defined as the angle between (a) and (b) (A). The tibia talar surface angle was formed by the angles between (c) and (d) (B). Angle between the ground and the upper surface of talus was defined as the angle between (e) and (f) (C). The talar tilt angle was defined as the angles between (g) and (h) (D). The medial ankle joint space was defined as the medial angles between (i) and (j) (E). Moreover, medial ankle clear space was defined as the line k from the medial malleolus to the lateral malleolus (F).
Figure 2. The tibia anterior surface angle was defined as the angle between (a) and (b) (A). The tibia talar surface angle was formed by the angles between (c) and (d) (B). Angle between the ground and the upper surface of talus was defined as the angle between (e) and (f) (C). The talar tilt angle was defined as the angles between (g) and (h) (D). The medial ankle joint space was defined as the medial angles between (i) and (j) (E). Moreover, medial ankle clear space was defined as the line k from the medial malleolus to the lateral malleolus (F). Tables
Table 1. Incidence of foot or ankle pain and associated risk factors were evaluated before surgery.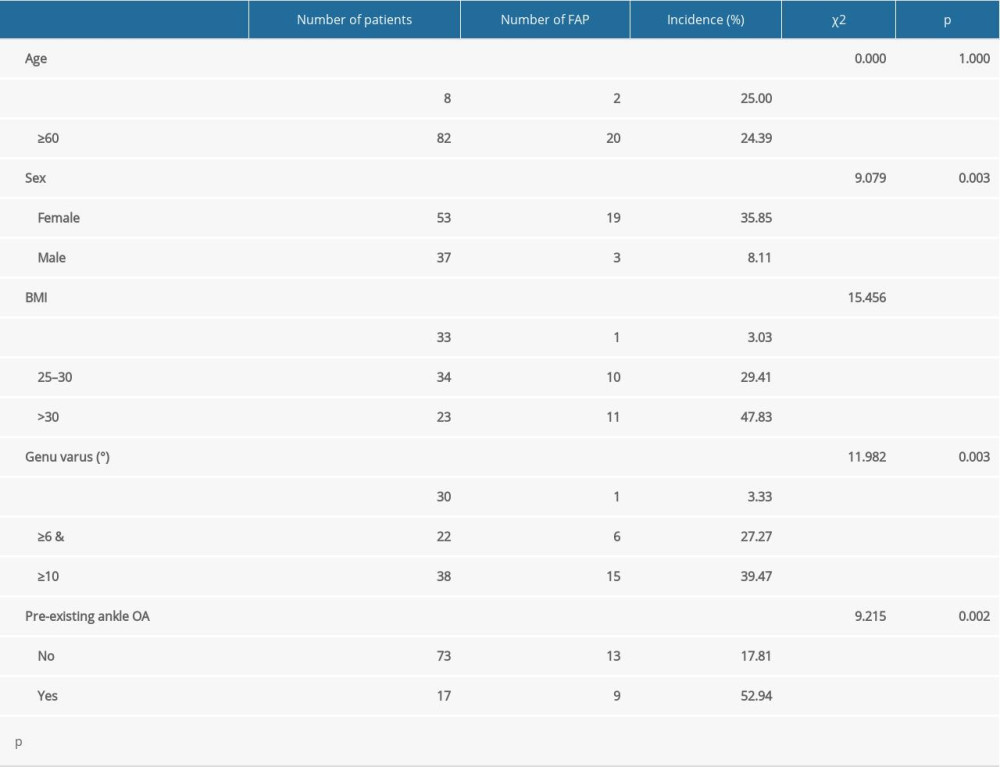 Table 2. The logistic regression analysis of foot or ankle pain and its potential explanatory variables.
Table 2. The logistic regression analysis of foot or ankle pain and its potential explanatory variables.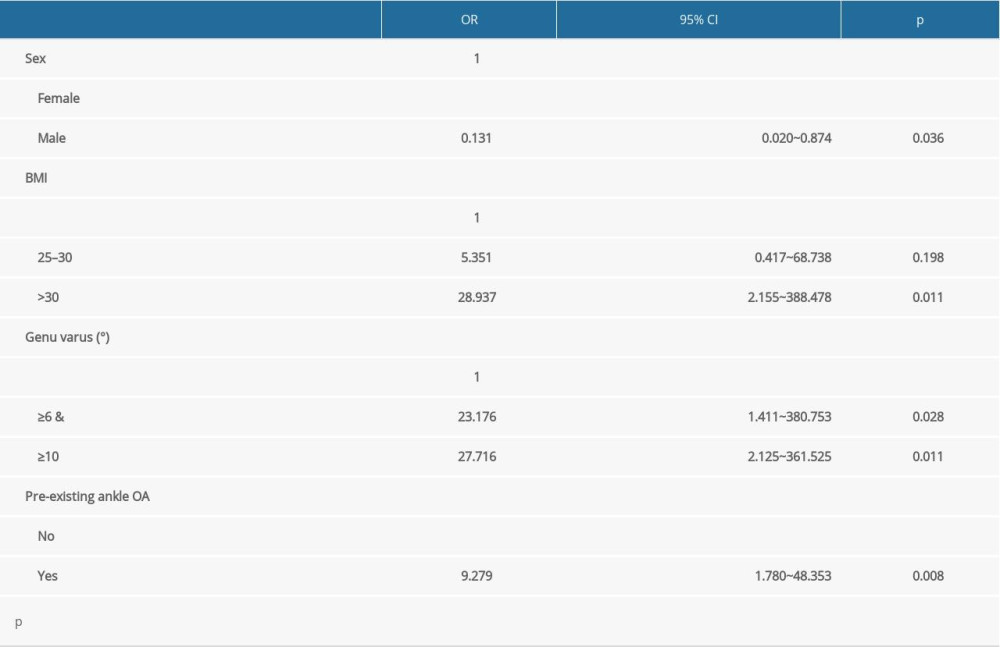 Table 3. Lower limb alignments on the operated side were compared before and after total knee arthroplasty using full-length standing anteroposterior radiographs.
Table 3. Lower limb alignments on the operated side were compared before and after total knee arthroplasty using full-length standing anteroposterior radiographs.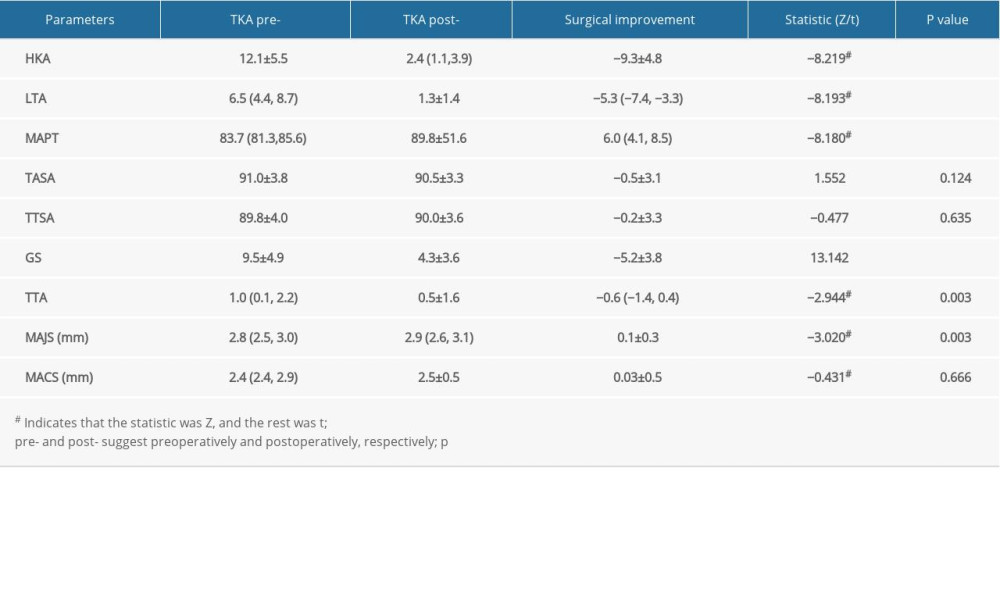 Table 4. The Δ radiological factors changes were compared in the groups with and without worsened foot or ankle pain.
Table 4. The Δ radiological factors changes were compared in the groups with and without worsened foot or ankle pain.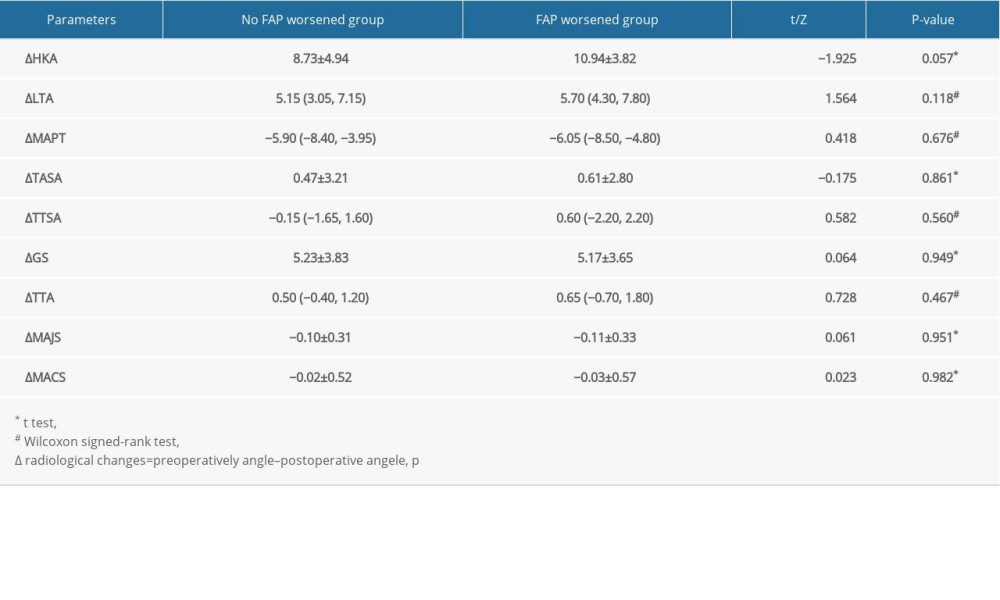
References
1. Ha CW, Park YB, Underestimation and undertreatment of osteoporosis in patients awaiting primary total knee arthroplasty: Arch Orthop Trauma Surg, 2020; 140(8); 1109-14
2. Kim CW, Gwak HC, Kim JH, Radiologic factors affecting ankle pain before and after total knee arthroplasty for the varus osteoarthritic knee: J Foot Ankle Surg, 2018; 57(5); 865-69
3. Kim SJ, MacDonald M, Hernandez J, Wixson RL, Computer assisted navigation in total knee arthroplasty: Improved coronal alignment: J Arthroplasty, 2005; 20(7 Suppl 3); 123-31
4. Tew M, Waugh W, Tibiofemoral alignment and the results of knee replacement: J Bone Joint Surg Br, 1985; 67(4); 551-56
5. Keene G, Simpson D, Kalairajah Y, Limb alignment in computer-assisted minimally-invasive unicompartmental knee replacement: J Bone Joint Surg Br, 2006; 88(1); 44-48
6. Norton AA, Callaghan JJ, Amendola A, Correlation of knee and hindfoot deformities in advanced knee OA: Compensatory hindfoot alignment and where it occurs: Clin Orthop Relat Res, 2015; 473(1); 166-74
7. Okamoto Y, Otsuki S, Jotoku T, Clinical usefulness of hindfoot assessment for total knee arthroplasty: Persistent post-operative hindfoot pain and alignment in preexisting severe knee deformity: Knee Surg Sports Traumatol Arthrosc, 2017; 25(8); 2632-39
8. Sidon E, Rogero R, McDonald E, Prevalence of neuropathic pain symptoms in foot and ankle patients: Foot Ankle Int, 2019; 40(6); 629-33
9. Nakamura Y, Uchiyama S, Kamimura M, Bone alterations are associated with ankle osteoarthritis joint pain: Sci Rep, 2016; 6; 18717
10. Murray C, Marshall M, Rathod T, Population prevalence and distribution of ankle pain and symptomatic radiographic ankle osteoarthritis in community dwelling older adults: A systematic review and cross-sectional study: PLoS One, 2018; 13(4); e0193662
11. Bae JY, Seo DK, Cho HK, Lee SK, Effect of lower-extremity angular imbalance on foot and ankle pain in patients with genu varus deformity: J Foot Ankle Surg, 2020; 59(4); 743-47
12. Choudhary S, McNally E, Review of common and unusual causes of lateral ankle pain: Skeletal Radiol, 2011; 40(11); 1399-413
13. Yamamoto N, Tsukada S, Kawai J, Calcaneal insufficiency fractures following total knee arthroplasty: Classification and clinical findings: Injury, 2019; 50(12); 2339-45
14. Frenkel O, Young male with severe ankle pain: Ann Emerg Med, 2017; 70(2); e27-28
15. Limaye R, Tripathy SK, Pathare S, Saeed K, Idiopathic transient osteoporosis of the talus: A cause for unexplained foot and ankle pain: J Foot Ankle Surg, 2012; 51(5); 632-35
16. Soylev GO, Boya H, A rare complication of total knee arthroplasty: Type l complex regional pain syndrome of the foot and ankle: Acta Orthop Traumatol Turc, 2016; 50(5); 592-95
17. Lee JH, Jeong BO, Radiologic changes of ankle joint after total knee arthroplasty: Foot Ankle Int, 2012; 33(12); 1087-92
18. Gao F, Ma J, Sun W, Radiographic assessment of knee-ankle alignment after total knee arthroplasty for varus and valgus knee osteoarthritis: Knee, 2017; 24(1); 107-15
19. Bargren JH, Blaha JD, Freeman MA, Alignment in total knee arthroplasty. Correlated biomechanical and clinical observations: Clin Orthop Relat Res, 1983; 173; 178-83
20. Jeffery RS, Morris RW, Denham RA, Coronal alignment after total knee replacement: J Bone Joint Surg Br, 1991; 73(5); 709-14
21. Rames RD, Mathison M, Meyer Z, No impact of under-correction and joint line obliquity on clinical outcomes of total knee arthroplasty for the varus knee: Knee Surg Sports Traumatol Arthrosc, 2018; 26(5); 1506-14
22. Valderrabano V, Horisberger M, Russell I, Etiology of ankle osteoarthritis: Clin Orthop Relat Res, 2009; 467(7); 1800-6
23. Gao F, Ma J, Sun W, Guo W, The influence of knee malalignment on the ankle alignment in varus and valgus gonarthrosis based on radiographic measurement: Eur J Radiol, 2016; 85(1); 228-32
24. Mullaji AB, Shetty GM, Lingaraju AP, Bhayde S, Which factors increase risk of malalignment of the hip-knee-ankle axis in TKA?: Clin Orthop Relat R, 2013; 471(1); 134-41
25. Gursu S, Sofu H, Verdonk P, Sahin V, Effects of total knee arthroplasty on ankle alignment in patients with varus gonarthrosis: Do we sacrifice ankle to the knee?: Knee Surg Sports Traumatol Arthrosc, 2016; 24(8); 2470-75
26. Chang CB, Jeong JH, Chang MJ, Concomitant ankle osteoarthritis is related to increased ankle pain and a worse clinical outcome following total knee arthroplasty: J Bone Joint Surg Am, 2018; 100(9); 735-41
27. Kamenaga T, Muratsu H, Kanda Y, The influence of postoperative knee stability on patient satisfaction in cruciate-retaining total knee arthroplasty: J Arthroplasty, 2018; 33(8); 2475-79
28. Lange JK, Lee YY, Spiro SK, Haas SB, Satisfaction rates and quality of life changes following total knee arthroplasty in age-differentiated cohorts: J Arthroplasty, 2018; 33(5); 1373-78
29. Bourne RB, Chesworth BM, Davis AM, Patient satisfaction after total knee arthroplasty: Who is satisfied and who is not?: Clin Orthop Relat Res, 2010; 468(1); 57-63
30. Franklin PD, Lewallen D, Bozic K, Implementation of patient-reported outcome measures in U.S. Total joint replacement registries: Rationale, status, and plans: J Bone Joint Surg Am, 2014; 96(Suppl 1); 104-9
31. Lautenbacher S, Kunz M, Strate P, Age effects on pain thresholds, temporal summation and spatial summation of heat and pressure pain: Pain, 2005; 115(3); 410-18
32. Lautenbacher S, Experimental approaches in the study of pain in the elderly: Pain Med, 2012; 13(Suppl 2); S44-50
33. Paladini A, Fusco M, Coaccioli S, Chronic pain in the elderly: The case for new therapeutic strategies: Pain Physician, 2015; 18(5); E863-76
34. Lautenbacher S, Peters JH, Heesen M, Age changes in pain perception: A systematic-review and meta-analysis of age effects on pain and tolerance thresholds: Neurosci Biobehav Rev, 2017; 75; 104-13
35. Molton IR, Terrill AL, Overview of persistent pain in older adults: Am Psychol, 2014; 69(2); 197-207
36. Xie K, Han X, Jiang X, The effect of varus knee deformities on the ankle alignment in patients with knee osteoarthritis: J Orthop Surg Res, 2019; 14(1); 134
37. Felson DT, Zhang Y, Hannan MT, The incidence and natural history of knee osteoarthritis in the elderly. The Framingham Osteoarthritis Study: Arthritis Rheum, 1995; 38(10); 1500-5
38. Zhang Y, Xu L, Nevitt MC, Comparison of the prevalence of knee osteoarthritis between the elderly Chinese population in Beijing and whites in the United States: The Beijing Osteoarthritis Study: Arthritis Rheum, 2001; 44(9); 2065-71
39. Atik OS, Gunal I, Korkusuz F, Burden of osteoporosis: Clin Orthop Relat Res, 2006; 443; 19-24
40. Payer J, Killinger Z, Sulkova I, Celec P, Preferences of patients receiving bisphosphonates – how to influence the therapeutic adherence: Biomed Pharmacother, 2008; 62(2); 122-24
41. Wang Y, Lobstein T, Worldwide trends in childhood overweight and obesity: Int J Pediatr Obes, 2006; 1(1); 11-25
42. Ng M, Fleming T, Robinson M, Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013: Lancet, 2014; 384(9945); 766-81
43. Wang Y, Wang L, Qu W, New national data show alarming increase in obesity and noncommunicable chronic diseases in China: Eur J Clin Nutr, 2017; 71(1); 149-50
44. Gonzalez Della Valle A, Chiu YL, Ma Y, The metabolic syndrome in patients undergoing knee and hip arthroplasty: trends and in-hospital outcomes in the United States: J Arthroplasty, 2012; 27(10); 1743-1749.e1
45. Estes CS, Schmidt KJ, McLemore R, Effect of body mass index on limb alignment after total knee arthroplasty: J Arthroplasty, 2013; 28(8 Suppl); 101-5
46. Butterworth PA, Menz HB, Urquhart DM, Fat mass is associated with foot pain in men: The Geelong Osteoporosis study: J Rheumatol, 2016; 43(1); 138-43
47. Krushell RJ, Fingeroth RJ, Primary Total knee arthroplasty in morbidly obese patients: A 5- to 14-year follow-up study: J Arthroplasty, 2007; 22(6 Suppl 2); 77-80
48. Dewan A, Bertolusso R, Karastinos A, Implant durability and knee function after total knee arthroplasty in the morbidly obese patient: J Arthroplasty, 2009; 24(6 Suppl); 89-94
49. Samson AJ, Mercer GE, Campbell DG, Total knee replacement in the morbidly obese: A literature review: ANZ J Surg, 2010; 80(9); 595-99
50. Ritter MA, Davis KE, Meding JB, The effect of alignment and BMI on failure of total knee replacement: J Bone Joint Surg Am, 2011; 93a(17); 1588-96
51. Berend ME, Ritter MA, Meding JB, Tibial component failure mechanisms in total knee arthroplasty: Clin Orthop Relat Res, 2004; 428; 26-34
52. Tallroth K, Harilainen A, Kerttula L, Sayed R, Ankle osteoarthritis is associated with knee osteoarthritis. Conclusions based on mechanical axis radiographs: Arch Orthop Traum Surg, 2008; 128(6); 555-60
53. Corti MC, Rigon C, Epidemiology of osteoarthritis: prevalence, risk factors and functional impact: Aging Clin Exp Res, 2003; 15(5); 359-63
54. Felson DT, Lawrence RC, Dieppe PA, Osteoarthritis: New insights. Part 1: The disease and its risk factors: Ann Intern Med, 2000; 133(8); 635-46
55. Cho WS, Cho HS, Byun SE, Changes in hindfoot alignment after total knee arthroplasty in knee osteoarthritic patients with varus deformity: Knee Surg Sports Traumatol Arthrosc, 2017; 25(11); 3596-604
Figures
Figure 1. Measurement of hip-knee-ankle angle (HKA) and ankle parameters based on full-leg standing anteroposterior radiographs. HKA was defined as the medial angle between (a) and (b) (A). Lateral tibial angle was defined as the medial angle between (c) and (d) (B). Medial angle of the proximal tibia was defined as the lateral angle between (d) and (f) (C).Figure 2. The tibia anterior surface angle was defined as the angle between (a) and (b) (A). The tibia talar surface angle was formed by the angles between (c) and (d) (B). Angle between the ground and the upper surface of talus was defined as the angle between (e) and (f) (C). The talar tilt angle was defined as the angles between (g) and (h) (D). The medial ankle joint space was defined as the medial angles between (i) and (j) (E). Moreover, medial ankle clear space was defined as the line k from the medial malleolus to the lateral malleolus (F). Tables
Table 1. Incidence of foot or ankle pain and associated risk factors were evaluated before surgery.Table 2. The logistic regression analysis of foot or ankle pain and its potential explanatory variables.Table 3. Lower limb alignments on the operated side were compared before and after total knee arthroplasty using full-length standing anteroposterior radiographs.Table 4. The Δ radiological factors changes were compared in the groups with and without worsened foot or ankle pain.Table 1. Incidence of foot or ankle pain and associated risk factors were evaluated before surgery.Table 2. The logistic regression analysis of foot or ankle pain and its potential explanatory variables.Table 3. Lower limb alignments on the operated side were compared before and after total knee arthroplasty using full-length standing anteroposterior radiographs.Table 4. The Δ radiological factors changes were compared in the groups with and without worsened foot or ankle pain. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387