17 December 2022: Database Analysis
Correlation of Patellofemoral Chondromalacia and Body Mass Index (BMI) in Relation to Sex and Age Analysis of 1.5T and 3.0T Magnetic Resonance (MR) Images Using the Outerbridge Scale
Dominik Sieroń1ABCDEF*, Izabella Jabłońska2ABCEF, Paweł NiemiecDOI: 10.12659/MSM.937246
Med Sci Monit 2022; 28:e937246






Abstract
BACKGROUND: BACKGROUND Cartilage disease (chondromalacia) is most commonly found in the patellofemoral joint. Non-invasive magnetic resonance imaging methods are used to assess the severity of chondromalacia. The available literature lacks papers describing the predilection of chondromalacia changes to BMI assessed on the basis of geometric data that can be assessed by 1.5T and 3.0T MRI. The aim of this study was to assess the relationship between the severity of chondromalacia of the patellofemoral joint and age, sex, and BMI assessed on the 1.5T and 3.0T MRI scanners. MATERIAL AND METHODS The study involved 324 patients, including 159 (49%) women and 165 (51%) men, aged 8-87 years (mean age: 45.1±20.9). The studied group had a BMI in the range of 14.3-47.3 (M: 27.7±5.02). A 1.5T and 3.0T MRI scanner were used in the study. To assess the cartilage of the patellofemoral joint, Outerbridge scales were used. RESULTS The age of the patients showed a significant correlation (Spearman’s rank, P<0.0001) with Outterbridge grade for each surface of patellofemoral joint. Higher correlation between BMI and Outerbridge grade was noted in the patella (rho=0.4139) than in the femur (rho=0.2890). There were no significant differences between women and men in the Outerbridge assessment of the knee joint (P>0.05). Significant more degeneration was found at the 1.5T scanner compared to the 3.0T MRI (P<0.0025). CONCLUSIONS The severity of chondromalacia significantly depends on age and BMI level. There is a stronger correlation between the degree of chondromalacia and BMI in women than in men.
MATERIAL AND METHODS:
RESULTS:
CONCLUSIONS:
Keywords: Aging, Body Mass Index, Cartilage Diseases, Chondromalacia Patellae, Magnetic Resonance Imaging, patellofemoral joint, Male, Humans, Female, young adult, Adult, Middle Aged, Aged, Patella, Knee Joint, Magnetic Resonance Spectroscopy
Background
The knee joint consists of the femorotibial joint and the patellofemoral joint. Increasing interest among clinicians has focused on the patellofemoral joint as a source of anterior compartment knee pain [1].
Osteoarthritis of the patellofemoral joint is a common disease of aging (>55 years of age). The condition occurs in women (17.1–34.0%) and men (18.5–19.0%) [2,3]. The literature indicates a predominance of women over men with chondromalacia of the patellofemoral joint due to an increased Q-angle (a line through the center of the patella to the anterior superior iliac spine and another line from the tibial tubercle through the center of the patella) and not necessarily explaining this difference with hormonal reasons [4]. Patients report discomfort in the anterior part of the knee when kneeling, squatting, sitting for a long period of time, and walking downhill or climbing stairs. Accompanying crepitations and a perceived morning stiffness is experienced in the patella region [5]. Factors that accelerate the development of chondromalacia of the patellofemoral joint are described in the literature [4]: trauma, quadriceps insufficiency, femoral condyle deformities are the most commonly mentioned [6–8].
Obesity is one of the factors that develops degenerative changes in cartilage on the background of mechanical load, but also on the metabolic basis [9]. Studies have shown that the infrapatellar fat pad releases inflammatory mediators and contributes to the development of osteoarthritis [10,11].
Chondromalacia of the patella covers a wide spectrum of severity. MRI with the Outerbridge scale is used as diagnostic method allowing non-invasive visualization of cartilage, which has a high sensitivity (84–87%) for chondromalacia changes of the knee joint [12–14]. A uniform and optimal pulse sequence for MRI cartilage imaging has still not been developed. Fat-suppressed fast-spin-echo proton-density and gradient-echo imaging is considered to be the most effective sequences for cartilage evaluation [15].
The purpose of this study was to examine the relationship between the degree of chondromalacia of the patellofemoral joint and BMI according to age category and sex. An additional aim was to note differences in cartilage assessment by MRI with the 1.5T and 3T.
Material and Methods
STUDY DESIGN:
All patients signed a general consent allowing us to use their anonymized medical date for research purposes. The local IRB waived ethics approval due to the retrospective study design using irreversible anonymization. In the current observational cross-sectional study, we analyzed the effect of BMI, including demographic variables (age, sex of subjects), on the severity of patellofemoral joint chondromalacia in a group of patients undergoing evaluation of knee joint lesions in 2018–2019. Patients were recruited from municipal and clinical hospitals and private facilities in Zamość, Elbląg, Jelenia Góra, Bielsko-Biała (Poland) and University Institute of Diagnostic, Pediatric and Interventional Radiology Tiefenau Hospital, Bern, Switzerland. The examination was performed according to Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines. The evaluation included the anterior compartment of the patellofemoral joint.
INCLUSION AND EXCLUSION CRITERIA:
The analyzed group of patients was referred by Orthopedists, Surgeon or Rehabilitation Specialist with concerns of pain or suspicion of arthrosis or post-traumatic lesions. Due to pain concerns, individuals reported on their own request for examination in the scope of private services. The study group consisted of 324 patients divided into 2 groups depending on sex: 159 (47.1%) women and 165 (52.9%) men. A total of 155 (47.8%) patients, including 70 (45.2%) women and 85 (54.8%) men, were examined on the 1.5T unit, while 169 (52.2%) patients, including 89 (52.7%) women and 80 (47.3%) men, were examined on the 3. 0T unit. Four age classes were defined for the study: 94 participants were <30 years, 61 participants were 30–45 years, 78 participants were 46–60 years, and 91 participants were >60 years. This study included 2 groups: 1.5T and 3.0T, with no control group. The 1.5T and 3.0T MRI exams were not performed on the same study participants. This study did not include inter-rater reliability analysis.
Exclusion criteria were previous surgery and chronic post-traumatic changes.
EVALUATION OF CARTILAGE CHONDROMALACIA:
To evaluate cartilage chondromalacia, we employed the 4-level Outerbridge classification (Table 1) using fat saturated proton-density sequences, a modified classification for arthroscopic cartilage evaluation [16–19].
IMAGE ACQUISITION:
The study was evaluated on iMac pro (Apple, Cupertino, USA) using the FDA-approved OsiriX MD software (version 11.0, Pixmeo SARL, Bernex, Switzerland). All MRI studies were irreversibly anonymized. MRI were performed on a 3.0T scanner (Ingenia 3.0T, Philips, Amsterdam, Netherlands) or on a 1.5T GE scanner (SIGNA, GE, Milwaukee, USA) GE instrument at different facilities located in clinical hospitals and private facilities in Zamość, Elbląg, Jelenia Góra, and Bielsko-Biała. The MRI protocols were standardized in all MR laboratories. Studies with differing protocols were excluded.
The following diagnostic sequence protocol was used in the study: axial, sagittal, and coronal PD FS; sagittal and coronal T1 (all with a slice thickness of 3 mm); and 3D high-resolution PD FS with a slice thickness from 0.8 to 1 mm. The same protocol was used in each diagnostic facility. Sequence parameters were in accordance with the European Society of Sport Traumatology, Knee Surgery & Arthroscopy (ESSKA) (Table 2) [20]. All images were assessed by an experienced musculoskeletal radiologist.
STATISTICAL ANALYSIS:
Chi-square (χ2) test of independence was used to analyze the difference of chondromalacia in the various age, sex, and MRI unit groups. We assessed the correlation between age subgroups and Outerbridge scale chondromalacia lesion scores, the C contingency coefficient was calculated, and the R-Spearman rank correlation was checked.
Subsequently, the correlation between BMI level and Outerbridge chondromalacia lesion scores was tested with Kruskal-Wallis, ANOVA, and post hoc analysis (Conover test), trend for mean values (Me) of BMI level in each Outerbridge scale grade, Jonckheere-Terpstra trend test, and the R-Spearman rank correlation (RHO). The above analysis was performed for the whole group, 1.5T and 3.0T, for women and men, and separately for 1.5T and 3.0T. The continuity coefficient was used as a measure of the relationship between age subgroup and Outerbridge scale grade. The use of the χ2 test provided the basis for the calculation of the C coefficient. Our table had dimensions of 4×4, and in this case Cmax=0.866. It was assumed that both 1.5T MRI and 3.0T MRI groups were homogeneous in terms of age, sex, and BMI based on the test χ2 (
Results
AGE:
Age was significantly correlated with the Outterbridge grade (Spearman rank correlation, P<0.0001). The femur and the patella reached correlation coefficients of rho=0.7128 and rho=0.6875, respectively (Table 3; Figure 1).
SEX:
There were no significant differences between women and men in the Outerbridge assessment for each knee joint compartment in each age subgroup (test χ2,
WOMEN: For women, age was correlated (Spearman rank cor-relation, P<0.0001) with Outerbridge grade for the femur (rho=0.7434) and patella (rho=0.7434) (Figure 2).
MEN: For men, age was correlated (Spearman rank correlation, P<0.0001) with Outterbridge grade for the femur (rho=0.6740) and patella (rho=0.6837) (Figure 3).
TYPE OF SCANNERS (1.5 T VS 3.0 T):
Significant differences were found between the scanner type (1.5T vs 3.0T) in the Outerbridge assessment for femur (χ2, P=0.0023) and patella (χ2, P=0.0064). For the 1.5T scanner, the Outerbridge scale grades in the femur and patella were on average M: 1.684; SD, 1.386 and M: 1.955; SD 1,350, respectively. For the 3.0T scanner, lower Outerbridge grade resulted for femur and patella: M: 1.024; SD 1.277 and M: 1.574; SD 1.511. The MR images for patella and femur for each Outerbridge scale depending on the scanner are shown in Figures 4 and 5.
Only for Patella, there was a statistically significant difference in the Outerbridge grade between the male and female subjects obtained on 1.5T (
BMI:
The average BMI for the entire study group was 27.7; SD: 5.02. The highest values of BMI were noted in patients diagnosed with Outterbridge grade III for femur and Outerbridge grade IV for patella. For the individual parameters of the Outerbridge scale, the mean BMI is presented in the Table 4.
FEMUR: A significant correlation was found between BMI level and Outerbridge parameter score for both scanners (rho=0.3996, P=0.0001) (Figure 6A).
There was a statistically significant difference in BMI level according to Outerbridge parameter score (
For femur, there were significant statistical differences between the Outerbridge subgroups (1 and 2 versus 3 and 4) in the BMI level (
The Outerbridge parameter grade 0 showed a statistically significant lower mean (Me) BMI level compared to grades I, II, and III (
PATELLA: There was a statistically significant positive correlation between BMI level and Outerbridge parameter grade for this location (rho=0.4139, P=0.0001) (Figure 6B).
Parameters Outerbridge grades differed significantly by BMI levels (
The Outerbridge subgroups (I and II versus III and IV) differed significantly by BMI level for patella (
The Outerbridge parameter grade 0 showed a statistically significant lower mean (Me) BMI level compared to grades I, II, III, and IV (
Discussion
There was a significant positive correlation between the Outerbridge chondromalacia grade and BMI and age. Differences between the 1.5T and 3.0T were found in Outerbridge chondromalacia grades and individual age subcategories. Differences between men and women were noted on 1.5T and 3.0T in the assessment of patella articular surface cartilage.
MRI is becoming a more common imaging modality for degenerative changes. Researchers in new publications use MRI more frequently to evaluate OA and infer its greater diagnostic sensitivity [21,22]. Our observations suggest that 1.5T and 3.0T are both accurate forms of assessment of chondromalacia of the patellofemoral joint. A study comparing the efficacy of MRI in assessing knee cartilage to an arthroscopic method showed moderate sensitivity of MRI – patella (76.4%) and femur (88.2%) – suggesting careful clinical evaluation of patients with suspected knee cartilage disorders [23]. Despite the clear findings of significant deterioration of knee joint function with the development of advanced chondromalacia in patients evaluated by arthroscopy, MRI images do not differ between early and advanced stages of chondromalacia in joint functional outcomes [24].
The association of higher Outerbridge chondromalacia grades and BMI appears stronger in women. In women, the correlation coefficients between the Outterbridge grade for femur and BMI was 0.5971 for 1.5T scanner and 0.4065 for 3.0T scanner. In men, the correlation coefficients between the Outerbridge grade for femur and BMI was lower than in women: 0.3517 for 1.5T scanner and 0.2676 for 3.0T scanner. Additionally, in the Outerbridge assessment for patella, the relationship with BMI in women was higher than in men: 1.5T (0.5810 vs 0.4010) and for 3.0T (0.3988 vs 0.3563). An explanation for this phenomenon can be the higher body fat ratio in women than men [25] and the associated higher levels of inflammatory mediators, which have detrimental effects on knee cartilage structures [26]. It is claimed that increasing body weight significantly decreases patellofemoral cartilage volume in women more than in men [27]. One study has shown an association between abnormal trochlear (femur) morphology and patellar cartilage damage (lateral part) particularly in women [28]. In our study population, a significant increase in the severity of femur cartilage lesions with age was noted. Additionally, differences in patella cartilage scores between men and women were found, along with a stronger correlation between chondromalacia and BMI in women. It seems that women are more prone to risk factors for chondromalacia of the patellofemoral joint than are men.
It was assumed that both groups (1.5T and 3.0T) are homogeneous due to the lack of significant differences in terms of age, sex, and BMI (
The main drawback of our study is the lack of evaluation of the same group of subjects with both 1.5T and 3.0T devices. In addition, the lack of a control group of healthy subjects with no knee joint problems made it impossible to observe the association of chondromalacia lesions with the clinical status in different Outerbridge grades. Future studies should distinguish between isolated chondromalacia of the patellofemoral joint and those with concomitant femorotibial joint lesions to comprehensively evaluate risk factors for the disease.
Conclusions
Evaluation of chondromalacia of the patellofemoral joint cartilage by 1.5T and 3.0T is an effective form of lesion classification using Outerbridge grades.
A positive correlation between the degree of chondromalacia of the patellofemoral joint with BMI and age was found, especially in women.
Figures
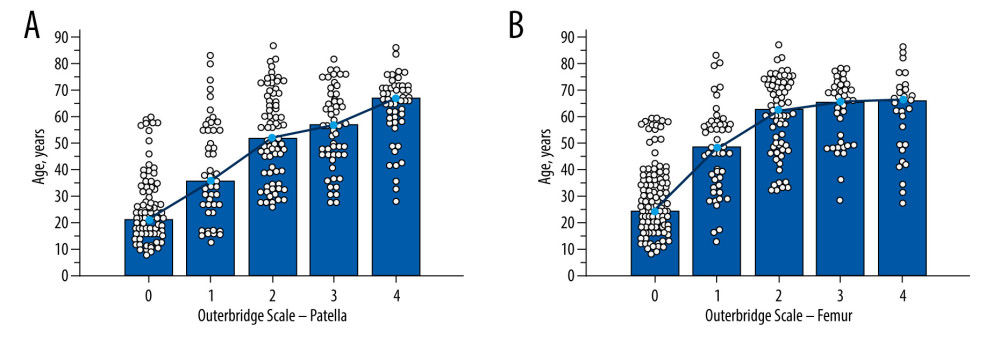 Figure 1. Relationship between the Outerbridge scale and age for patella (A) and femur (B).
Figure 1. Relationship between the Outerbridge scale and age for patella (A) and femur (B). 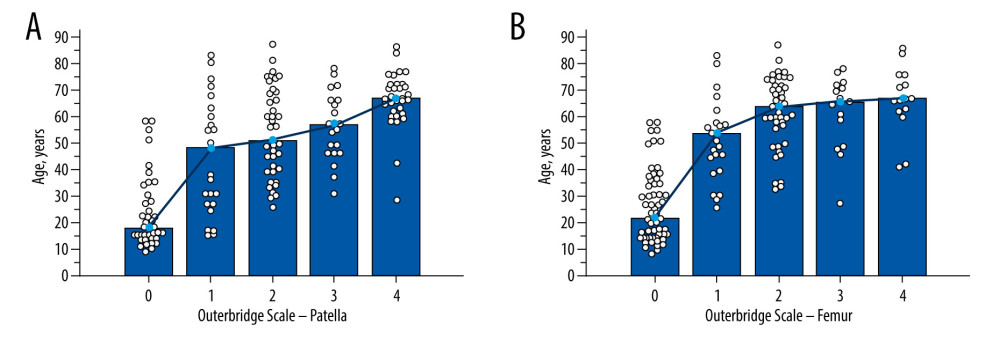 Figure 2. Relationship between the Outterbridge scale and age for patella (A) and femur (B) in females.
Figure 2. Relationship between the Outterbridge scale and age for patella (A) and femur (B) in females. 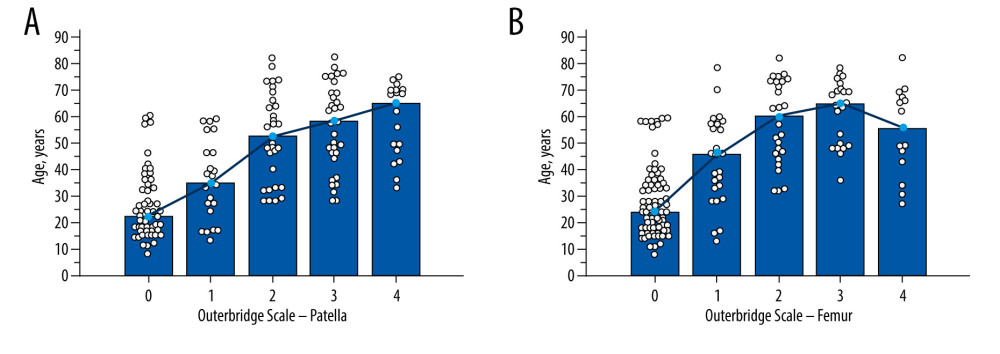 Figure 3. Relationship between the Outerbridge scale and age for patella (A) and femur (B) in males.
Figure 3. Relationship between the Outerbridge scale and age for patella (A) and femur (B) in males. 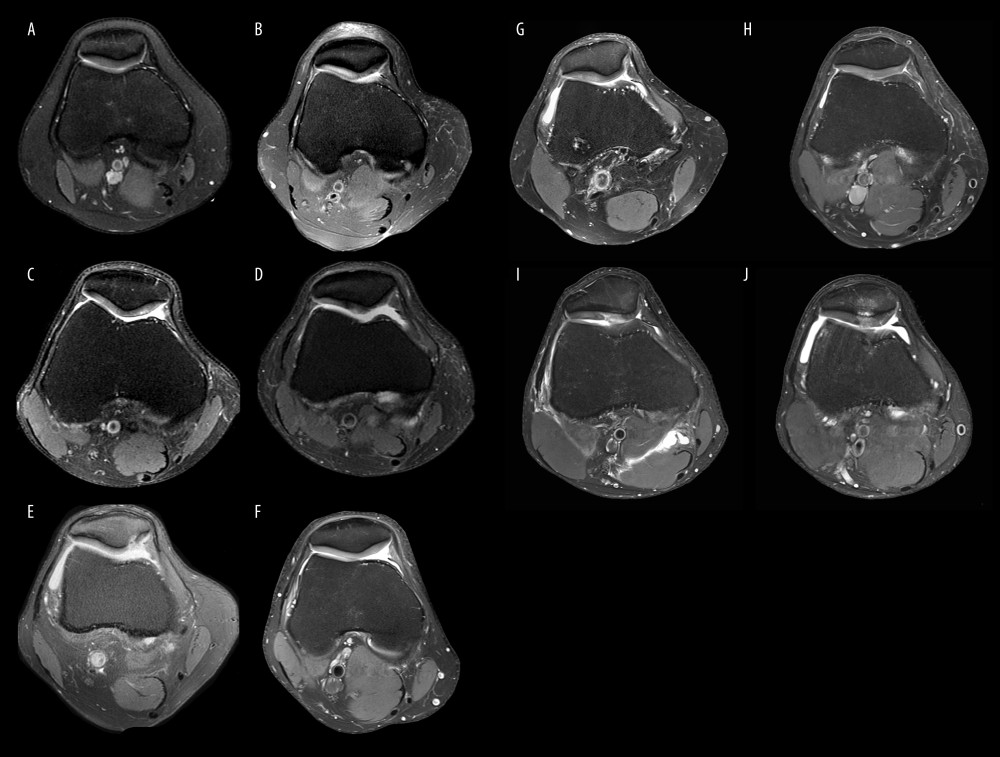 Figure 4. (A–J) Axial PD-weighted images with patellar chondromalacia (white arrows) with different Outterbridge classifications 0/1/2/3/4 (A/B/C/D/E).
Figure 4. (A–J) Axial PD-weighted images with patellar chondromalacia (white arrows) with different Outterbridge classifications 0/1/2/3/4 (A/B/C/D/E). 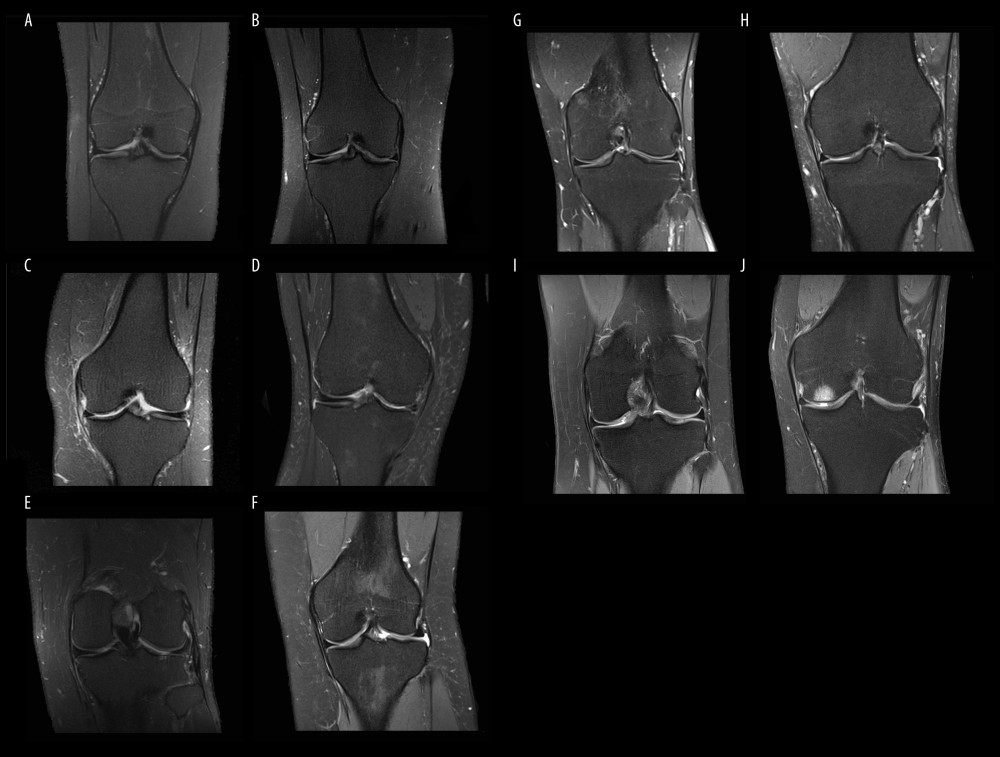 Figure 5. (A–J) Coronal PD-weighted images with femoral chondromalacia (white arrows) with different Outterbridge classifications 0/1/2/3/4 (A/B/C/D/E).
Figure 5. (A–J) Coronal PD-weighted images with femoral chondromalacia (white arrows) with different Outterbridge classifications 0/1/2/3/4 (A/B/C/D/E). 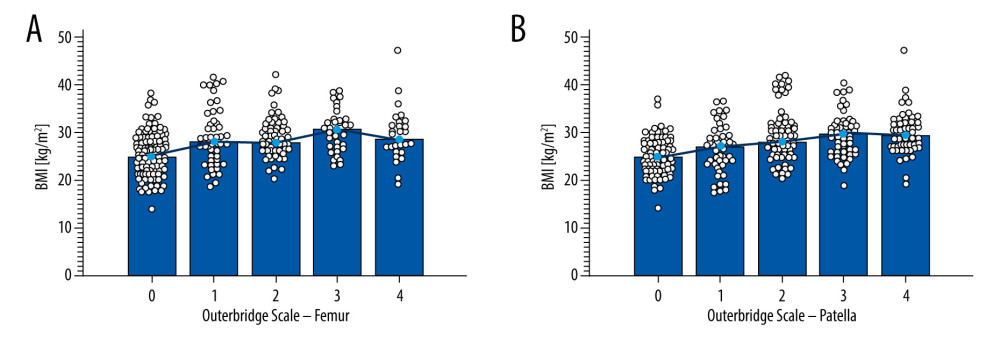 Figure 6. Relationship between BMI and Outerbridge grades using both scanners (1.5T and 3.0T) in study group for femur (A) and patella (B).
Figure 6. Relationship between BMI and Outerbridge grades using both scanners (1.5T and 3.0T) in study group for femur (A) and patella (B). References
1. Zheng W, Li H, Hu K, Chondromalacia patellae: Current options and emerging cell therapies: Stem Cell Res Ther, 2021; 12; 412
2. Davies A, Vince A, Shepstone L, Donell S, Glasgow M, The radiologic prevalence of patellofemoral osteoarthritis: Clin Orthop Relat Res, 2002; 402; 206-12
3. Drexler M, Dwyer T, Marmor M, The treatment of acquired patella baja with proximalize the tibial tuberosity: Knee Surg Sports Traumatol Arthrosc, 2012; 21; 2578-83
4. Habusta SF, Coffey R, Ponnarasu S, Chondromalacia patella. [Updated 2022 May 12]: StatPearls [Internet], 2022, Treasure Island (FL), StatPearls Publishing
5. Bei M, Tian F, Xiao Y, Raloxifene retards cartilage degradation and improves subchondral bone micro-architecture in ovariectomized rats with patella baja-induced – patellofemoral joint osteoarthritis: Osteoarthr Cartil, 2020; 28; 344-55
6. Watts N, Belmont P, Orr J, Incidence and risk factors for chronic anterior knee pain: J Knee Surg, 2015; 29; 248-53
7. Damgacı L, Özer H, Duran S, Patella–patellar tendon angle and lateral patella–tilt angle decrease patients with chondromalacia patella: Knee Surg Sports Traumatol Arthrosc, 2020; 28; 2715-21
8. Chan V, Moran D, Mwangi I, Eustace S, Prevalence and clinical significance of chondromalacia isolated to the anterior margin of the lateral femoral condyle as a component of patellofemoral disease: Observations at MR imaging: Skeletal Radiol, 2013; 42; 1127-33
9. Clockaerts S, Bastiaansen-Jenniskens Y, Runhaar J, The infrapatellar fat pad should be considered as an active osteoarthritic joint tissue: A narrative review: Osteoarthr Cartil, 2010; 18; 876-82
10. Masaki T, Takahashi K, Hashimoto S, Volume change in infrapatellar fat pad is associated not with obesity but with cartilage degeneration: J Orthop, 2019; 37; 593-600
11. Kok H, Donnellan J, Ryan D, Torreggiani W, Correlation between subcutaneous knee fat thickness and chondromalacia patellae on magnetic resonance imaging of the knee: Can Assoc Radiol J, 2013; 64; 182-86
12. Tuna B, Semiz-Oysu A, Pekar B, The association of patellofemoral joint morphology with chondromalacia patella: A quantitative MRI analysis: Clin Imaging, 2014; 38; 495-98
13. Pihlajamäki H, Kuikka P, Leppänen V, Reliability of clinical findings and magnetic resonance imaging for the diagnosis of chondromalacia patellae: J Bone Joint Surg Am, 2010; 92; 927-34
14. Harris J, Brophy R, Jia G, Sensitivity of magnetic resonance imaging for detection of patellofemoral articular cartilage defects: Arthroscopy, 2012; 28; 1728-37
15. Khanna AJ, Cosgarea AJ, Mont M, Magnetic resonance imaging of the knee: J Bone Jt Surg, 2001; 83; 128-41
16. Park C, Song K, Kim J, Lee S, Retrospective evaluation of outcomes of bone peg fixation for osteochondral lesion of the talus: Bone Joint J, 2020; 102-B; 1349-53
17. Slimi F, Zribi W, Trigui M, The effectiveness of platelet-rich plasma gel on full-thickness cartilage defect repair in a rabbit model: Bone Joint Res, 2021; 10; 192-202
18. Elder S, Clune J, Walker J, Gloth P, Suitability of EGCG as a means of stabilizing a porcine osteochondral xenograft: J Funct Biomater, 2017; 8; 43
19. Eldridge S, Barawi A, Wang H, Agrin induces long-term osteochondral regeneration by supporting repair morphogenesis: Sci Transl Med, 2020; 12; eaax9086
20. Kassarjian A, Fritz L, Afonso P: Guidelines for MR imaging of sports injuries, 2016, European Society of Skeletal Radiology Sports Sub-committee Available from: https://essr.org/content-essr/uploads/2016/10/ESSR-MRI-Protocols-Knee.pdf
21. Kobayashi S, Pappas E, Fransen M, The prevalence of patellofemoral osteoarthritis: A systematic review and meta-analysis: Osteoarthr Cartil, 2016; 24; 1697-707
22. Hunter D, Zhang W, Conaghan P, Responsiveness and reliability of MRI in knee osteoarthritis: A meta-analysis of published evidence: Osteoarthr Cartil, 2011; 19; 589-605
23. Danieli M, Guerreiro J, Queiroz A, Diagnosis and classification of chondral knee injuries: comparison between magnetic resonance imaging and arthroscopy: Knee Surg Sports Traumatol Arthrosc, 2015; 24; 1627-33
24. Aysin I, Askin A, Dirim Mete B, Investigation of the relationship between anterior knee pain and chondromalacia patellae and patellofemoral malalignment: Eurasian J Med, 2018; 50; 28-33
25. Wu B, O’Sullivan A, Sex differences in energy metabolism need to be considered with lifestyle modifications in humans: J Nutr Metab, 2011; 2011; 391809
26. Stannus O, Jones G, Cicuttini F, Circulating levels of IL-6 and TNF-α are associated with knee radiographic osteoarthritis and knee cartilage loss in older adults: Osteoarthr Cartil, 2010; 18; 1441-47
27. Teichtahl A, Wang Y, Wluka A, The longitudinal relationship between body composition and patella cartilage in healthy adults: Obesity, 2008; 16; 421-27
28. Duran S, Cavusoglu M, Kocadal O, Sakman B, Association between trochlear morphology and chondromalacia patella: an MRI study: Clin Imaging, 2017; 41; 7-10
Figures
Figure 1. Relationship between the Outerbridge scale and age for patella (A) and femur (B).Figure 2. Relationship between the Outterbridge scale and age for patella (A) and femur (B) in females.Figure 3. Relationship between the Outerbridge scale and age for patella (A) and femur (B) in males.Figure 4. (A–J) Axial PD-weighted images with patellar chondromalacia (white arrows) with different Outterbridge classifications 0/1/2/3/4 (A/B/C/D/E).Figure 5. (A–J) Coronal PD-weighted images with femoral chondromalacia (white arrows) with different Outterbridge classifications 0/1/2/3/4 (A/B/C/D/E).Figure 6. Relationship between BMI and Outerbridge grades using both scanners (1.5T and 3.0T) in study group for femur (A) and patella (B). Tables
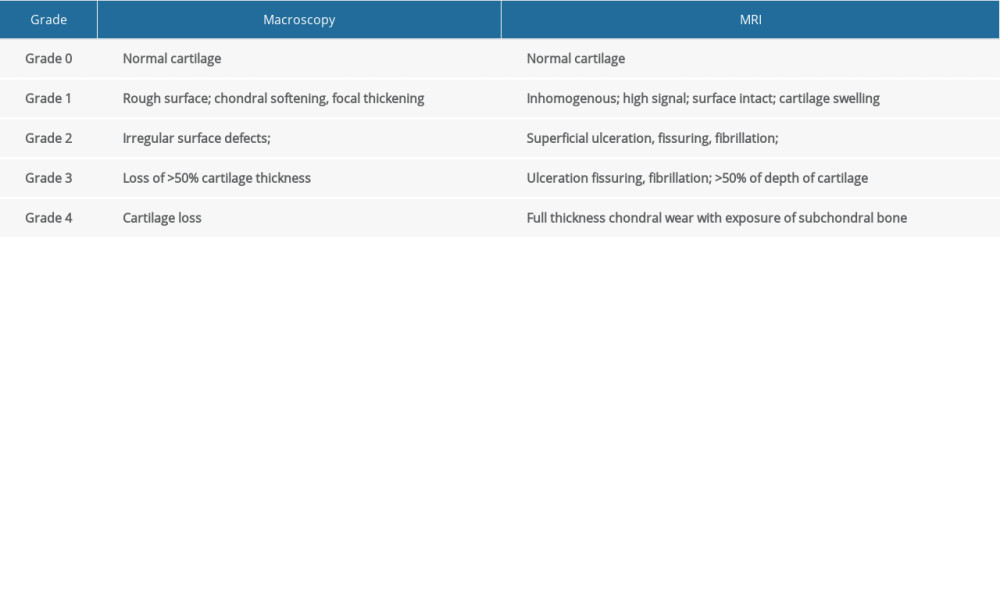 Table 1. Outerbridge classification.
Table 1. Outerbridge classification. Table 2. Sequences parameters.
Table 2. Sequences parameters.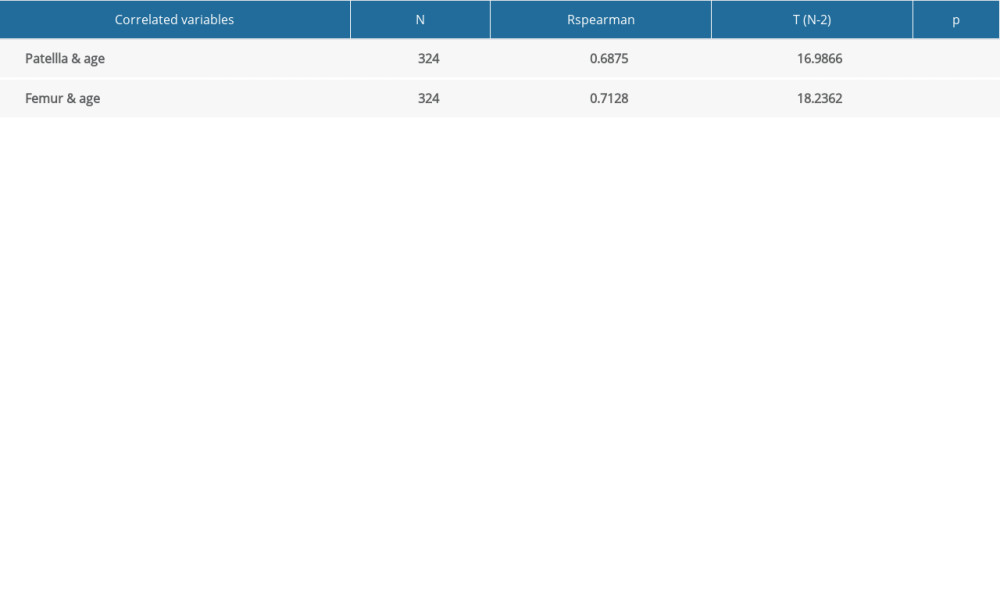 Table 3. Relationship between the Outerbridge scale and age for the patellofemoral joint.
Table 3. Relationship between the Outerbridge scale and age for the patellofemoral joint.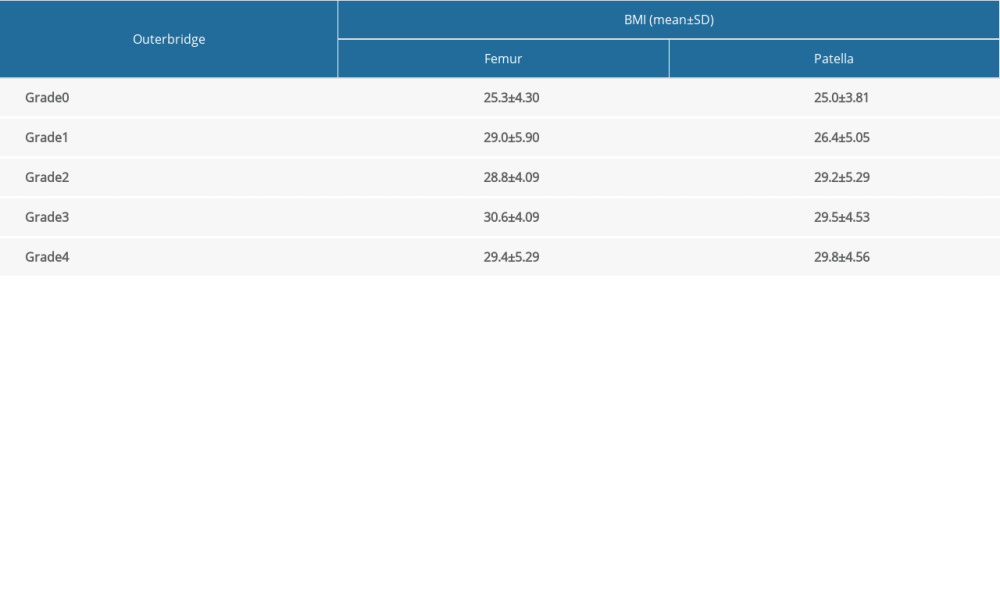 Table 4. BMI for Outerbridge scale.Table 1. Outerbridge classification.Table 2. Sequences parameters.Table 3. Relationship between the Outerbridge scale and age for the patellofemoral joint.Table 4. BMI for Outerbridge scale.
Table 4. BMI for Outerbridge scale.Table 1. Outerbridge classification.Table 2. Sequences parameters.Table 3. Relationship between the Outerbridge scale and age for the patellofemoral joint.Table 4. BMI for Outerbridge scale. In Press
Meta-Analysis
Effectiveness of Cardiac Telerehabilitation in Improving Functional Capacity, Quality Of Life and Cardiovas...Med Sci Monit In Press; DOI: 10.12659/MSM.953366
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,468
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,759,966
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,248
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,898
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387