15 March 2023: Clinical Research
Alterations in Amygdala/Hippocampal Volume Ratios in Children with Obstructive Sleep Apnea Syndrome Caused by Adenotonsillar Hypertrophy
Yanshan Ma1ABCE, Zheli Niu2ABCE, Lin Ruan2CDF, Sisi Xue3CDF, Nan Li3F, Xiaoguang YaoDOI: 10.12659/MSM.937420
Med Sci Monit 2023; 29:e937420






Abstract
BACKGROUND: Intermittent hypoxemia can cause changes in certain brain structures. However, in pediatric patients with obstructive sleep apnea (OSA) caused by adenotonsillar hypertrophy (ATH), there is only limited information on the effect of ATH-induced OSA on brain structures. This study sought to investigate alterations in amygdala and hippocampal volumes in children with OSA by ATH.
MATERIAL AND METHODS: Magnetic resonance imaging scans were applied in children who had ATH-induced OSA (ATH/OSA) and in healthy children. Amygdala and hippocampus volumes and adenoid sizes were measured on MRI volumetric images. The ratio of adenoid size/nasopharyngeal depth was used to describe the severity of adenoid hypertrophy. The clinical variables of the involved subjects were investigated.
RESULTS: One hundred ATH/OSA children and 100 healthy children without ATH/OSA participated in the study. The ATH/OSA children had higher amygdala volumes and amygdala/hippocampus volume ratios but lower hippocampus volumes than healthy controls, and the amygdala/hippocampus volume ratios were correlated with disease duration and hypoxemia conditions. However, our data showed that amygdala/hippocampus volume ratios were not correlated with the ratios of adenoid size/nasopharyngeal depth in the ATH/OSA children. In addition, the ratio of adenoid size/nasopharyngeal depths in ATH/OSA children was higher than that in healthy children in each subgroup based on the age of participants.
CONCLUSIONS: Compared to healthy controls, amygdala/hippocampus volume ratios are increased in children with ATH/OSA.
Keywords: Adenoids, Adult Children, Amygdala, Hippocampus, Hypertrophy, Sleep Apnea Syndromes, Humans, Child, Sleep apnea, obstructive, Palatine Tonsil, Hypoxia
Background
Prevalence studies have shown that pediatric obstructive sleep apnea (OSA) affects up to 5% of children [1,2]. Adenotonsillar hypertrophy (ATH) is the leading cause of OSA in children. The classic pathologies of OSA include intermittent upper airway obstruction and increased upper airway resistance, which then lead to alveolar hypoventilation, intermittent hypoxemia, and sleep fragmentation with repeated arousals during sleep [3].
Kheirandish-Gozal et al reported that several brain regions of OSA children, including the prefrontal cortex, middle and posterior corpus callosum, thalamus, hippocampus, and cerebellar areas, showed reduced entropy values [4], while Philby et al suggested that pediatric OSA subjects showed gray matter volume reductions in multiple areas compared to healthy controls [3]. Studies on OSA animal models have demonstrated that OSA can induce neuronal cell losses in several brain regions, which then result in changes in cognition and mood functions, especially in pediatric OSA [5]. Children with OSA can display multiple behavioral deficits, such as daytime sleepiness and deficits in memory and attention, which then impair academic and work performance [6,7]. In recent years, changes in behavior and cognition in OSA children have been reported. Cha et al demonstrated lower mean diffusivity of the dentate gyrus in children with OSA, which correlates with a lower verbal learning and memory scores [8]. Other studies have revealed that deficits in cognitive and behavioral abilities could be attributed to alterations of brain structures induced by intermittent hypoxemia [3,4].
Both the amygdala and hippocampus can play a role in the development of behavior and cognitive ability in children. The amygdala is an almond-shaped brain region located in the anterior portion of the temporal lobe. It is clear that the amygdala serves as an important structure related to neuropsychiatric and neurodevelopmental disorders [9], such as depression, social phobia, autism, and schizophrenia. The hippocampus is a complex subcortical structure embedded deep in the temporal lobe and plays a critical role in learning, memory, spatial navigation, and emotional behavior [10,11]. It is vulnerable and can be damaged by a variety of stimuli. Studies have shown that a dysfunctional hippocampus could be related to multiple diseases, including attention-deficit/hyperactivity disorder in children [12]. MacMillan et al suggested that increased amygdala/hippocampal volume ratios were associated with the severity of anxiety in pediatric major depression [13]. Moreover, both the amygdala and hippocampus are oxygen-sensitive organs. In a murine model, Raman et al found that chronic hypoxia could affect hippocampal development [14]. Carry et al found a significant decrease in the cell size and axonal degeneration of corticotropin-releasing factor-positive neurons in the amygdala of rats after undergoing neonatal hypoxia-ischemia [15]. Therefore, hypoxia is potentially associated with changes in the amygdala and hippocampus [16]. However, there is a lack of data on changes in hippocampal and amygdala volumes in children with OSA caused by ATH. Thus, research on the amygdala and hippocampus in children with OSA caused by ATH could provide more information about pathological changes.
In recent years, imaging technologies such as MRI and CT have been widely used in the diagnosis and therapy of pediatric OSA, which can help researchers and clinicians to assess the size of the adenotonsillar, the severity, or the outcome of adenotonsillectomy. In particular, MRI can evaluate the anatomy of the pharynx and brain structure. Therefore, in this study, using MRI scans, we aimed to investigate whether hippocampal and amygdala volumes are affected by ATH-induced OSA in pediatric patients.
Material and Methods
ETHICS CONSIDERATION AND CONSENT TO PARTICIPATE:
The protocol (NO. 20160632) was approved by the Shijiazhuang Hospital of Traditional Chinese Medicine review board. The study adhered to the laws of China, the Declaration of Helsinki version 2008, and the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) statement. An informed consent form was signed by all children’s parents or legal guardians regarding radiology and publications of the study in all formats of the publication house, including the personal data of patients, irrespective of time and language. The clinical trial registration number is ChiCTR2100045287.
SUBJECT COHORT:
Inclusion criteria of ATH/OSA children in this study included: (1) Age 2–16 years; (2) both sexes; (3) Pathology of adenotonsillar hypertrophy; (4) Evidence of OSA according to the Guideline on Diagnosis and Management of Obstructive Sleep Apnea Syndrome in Children by American Academy of Pediatrics (with symptoms, physical examination, imaging, night polysomnography); (5) Polysomnographic criteria: according to the criteria of the American Academy of Sleep Medicine. Apnea was defined as a >90% reduction in airflow for at least the duration of 2 breaths, and hypopnea was defined as a ≥30% reduction of airflow for at least 2 breaths associated with a ≥3% desaturation from pre-event baseline or the event is associated with an arousal. Apnea-hypopnea index (AHI) ≥1; (6) at least 1 month duration of symptoms; and (7) no history of bronchitis, pneumonia, asthma, emphysema, bronchopulmonary dysplasia, tuberculosis, whooping cough, or cancer in airway.
Inclusion criteria of healthy pediatric subjects in this study were: (1) physical examination and the results of routine laboratory tests are within normal limits; (2) no history of acute/chronic tonsillitis, peritonsillar abscess, acute mononucleosis, strep throat, or during the past 6 months; (3) no history of adenotonsillar hypertrophy or tonsilloliths; (4) no history of disease in the nervous system; (5) no history of infection, bronchitis, pneumonia, asthma, emphysema, bronchopulmonary dysplasia, tuberculosis, whooping cough, or cancer in airway; and (6) no obesity history.
Exclusion criteria were: (1) history of otitis media, acute bronchopulmonary disease, systemic inflammation, tuberculosis, infection of upper airway, sinusitis, septal deformity, hypertension, immunodeficiency, hyperthyroidism, neuromuscular disorders, cancer, allergy sinusitis, heart failure, malnutrition, craniofacial syndromes, bronchial asthma, cranial nerve palsies, head injury, laryngopharyngeal reflux, or dental disease during the past 6 months; (2) OSA due to other reasons, such as obesity; or (3) any history of disease in the nervous system.
Sample size was calculated by estimating 30 children (15 children with ATH/OSA and 15 health controls), considering α=0.050 (type I error) and β=0.200 (type II error).
In summary, 100 children with ATH/OSA were enrolled, while 100 age-matched healthy children with no history of ATH and/or OSA were randomly recruited from children admitted to our clinic as the control group.
Demographic characteristics were collected from the recruited subjects, including age, sex, body mass index (BMI), disease duration, history of asthma, history of chronic or allergic rhinitis, and food/drug allergies. The data were recorded by the staff in our hospital and analyzed by the researchers involved in this study. Adenotonsillar sizes were collected by MRI scan examination. The hippocampal and amygdala volumes were accessed by MRI scan. Data on clinical variables, including eosinophil count in peripheral blood and total serum IgE level, were also collected.
An otolaryngologist was introduced to evaluate the size of the tonsillar and adenoid, and the child’s general appearance thorough physical examination, symptoms, medical history, flexible endoscopy, X-ray, and MRI results.
To evaluate tonsillar size, a 5-grade scale (Brodsky Grading Scale) was applied as follows [17]: 0: tonsils within the tonsillar fossa; 1: tonsils just outside of the tonsillar fossa and occupy ≤25% of the oropharyngeal width; 2: tonsils occupy 26–50% of the oropharyngeal width; 3: tonsils occupy 51–75% of the oropharyngeal width; 4: tonsils occupy >75% of the oropharyngeal width.
To evaluate adenoid size, flexible endoscopy examinations were performed, then a 4-grade scale was applied as follows based on the relationship of the adenoids to the adjacent structures in the rear of nasal cavity (both sides) [18]: 1 point: adenoids had no contact with other tissues; 2 points: the torus tubaris was in contact with the adenoids; 3 points: the torus tubaris and vomer were in contact with the adenoids; 4 points: the torus tubaris, vomer and soft palate were in contact with the adenoids. In most cases, there was no difference between the right and left adenoids. In unbalanced cases, the higher score was presented and used for our analysis.
All ATH/OSA children underwent polysomnography. No sleep deprivation or sedation was used. Children were studied in a dedicated, quiet, darkened room with an ambient temperature of 24°C in the company of one of their parents. Analysis of the polysomnogram was performed using standard techniques. The mean oxygen saturation of arterial blood (mean SaO2), minimum oxygen saturation of arterial blood (min Sao2), and AHI were determined.
MRI ASSESSMENT:
MRI was obtained with a 1.5 T device (Signa HD, GE, US) without sedation. The imaging protocol included axial T2-weighted (T2-w1) TSETR4000/TE, 120 ms; 5 mm section thickness; and axial T1-weighted spin echo (T1w SE) images (TR400/TE, 15 ms; acquisition matrix of 278×256, field of view (FOV) of 220×230. All images were available in digital form. MR images were re-evaluated by 2 radiologists. When readings differed, the decision was made on the basis of consensus.
ADENOID SIZE INVESTIGATION:
Using the measuring scale, we determined 2 lines as follows (Fujioka Method) [19]: (1) The distance between the outermost point of convexity of adenoid shadow and spheno/basiocciput (A), and (2) the distance between spheno/basiocciput and posterior end of the hard palate (N). Thereafter, the adenoid size was described as the ratio of the adenoid size/nasopharyngeal depth (A/N).
AMYGDALA AND HIPPOCAMPAL VOLUME:
T1-weighted brain images were used to assess amygdala and hippocampal volumes with a 3D MPRAGE (Magnetization Prepared Rapid Gradient Echo Imaging) protocol. Images were visually inspected by radiologists to ensure the quality of registration and segmentation. Images were assessed on a slice-by-slice basis to obtain optimal contrast to visualize the anatomic landmarks for segmentation. Regions of interest were initially segmented automatically using a proprietary tool and then were adjusted manually. The amygdala and hippocampus were extracted from each participant’s image. Thereafter, the amygdala/hippocampus volume ratios (A/H ratios) were calculated as the total amygdala volume (left and right) divided by the total hippocampus volume.
INTER-RATER AND INTRA-RATER RELIABILITY MEASUREMENT:
To access inter-rater reliability, measurement was performed on MR images of 30 randomly selected cases by 2 raters using the same protocol. The measurements of the structures were used to compute inter-rater reliability using absolute agreement and multiple raters intraclass correlation coefficient (ICC).
To assess intra-rater reliability, measurement was performed on 20 randomly selected MR images using the same protocol with 3-month intervals. Intra-rater reliability test scores were calculated using absolute agreement ICC.
STATISTICAL ANALYSIS:
Statistical analysis was conducted using SPSS 26.0 (IBM SPSS, Armonk, NY, USA) for statistical computing and graphics.
To assess the effect of age on measures of interest, healthy children and children with ATH/OSA were investigated. Nonlinear (quadratic) and linear models were applied to test the effect of age on the values of A/N ratios, while linear models were applied to test the effect of age on the values of A/H ratios. Multiple linear regression was utilized to investigate correlations among clinical variables on the A/H ratios. Pearson’s correlation coefficients were utilized to investigate correlations among clinical variables on the A/H ratios.
The data of the clinical variables and demographic characteristics are expressed as the mean±standard deviation (SD) for continuous variables when the data were normally distributed, as a 95% confidence interval (CI) when the data had a skewed distribution, or counts (percentages) for discrete variables. A two-tailed t test, ANOVA, and chi-square test were used for the statistical analysis.
Results
DEMOGRAPHIC DATA AND CLINICAL VARIABLES:
From 2016–2019, 100 pediatric patients with ATH/OSA and 100 healthy children without ATH were included in this study. The demographic characteristics and clinical variables of all involved participants are presented in Table 1. In the ATH/OSA group, the mean age was 5.74 years old, the mean BMI z score was 0.37, and 68% were male. A total of 7% of study participants had positive food/drug allergies, 14% had clinical features of allergic rhinitis, and 5% had a history of asthma in the ATH/OSA group. The blood eosinophil count and total serum IgE were 289.15±67.10 μL and 251.27±63.21 U/mL, respectively.
In the age- and sex-matched control group, the mean age was 5.95 years old, the mean BMI z score was 0.32, and 65% were male (Table 1). In the control group, 5% of the study participants had a food/drug allergy, while no children had a history of asthma or allergic rhinitis. The blood eosinophil count and total serum IgE were 279.12±51.64 μL and 236.42±66.95 U/mL, respectively.
There was no significant difference between the ATH/OSA children and the healthy children regarding age, sex, BMI z score, history of food/drug allergy, smoking history in family, serum IgE, and eosinophil count in peripheral blood.
PSG parameters of pediatric patients with ATH/OSA are summarized in Table 1. Sleep was characterized by an increased number of arousals and by low sleep efficiency. The mean apnea-hypopnea index (AHI) was 33.25 and was associated with nocturnal hypoxemia (nadir SaO2).
INTER-RATER AND INTRA-RATER RELIABILITY:
The A/N ratios and the volumes of amygdala and hippocampus were used to evaluate inter-rater reliability of 2 raters by calculating the ICCs. Strong ICC results were observed for A/N ratios, amygdala, and hippocampus among raters (A/N ratios: ICC=0.91; amygdala: ICC=0.92; and hippocampus: ICC=0.90). To assess intra-rater reliability, ICCs were calculated at 2 time points (at 3-month intervals). The A/N ratios and the volumes of amygdala and hippocampus at these 2 points were measured. High intra-rater reliability results were observed (A/N ratios: ICC=0.98; amygdala: ICC=0.96; and hippocampus: ICC=0.94). Thus, the measurements were highly replicable.
THE A/N RATIOS OF INVOLVED PEDIATRIC SUBJECTS:
Based on the results of the MRI scan, we calculated the A/N values of each participant. Then, we generated the trend of A/N values based on the ages of participants in each group. As shown in Figure 1A and 1B, in the healthy control group, the A/N values increased from 2–5 years old and reached peak values at approximately 5 years old, from 0.54 to 0.6. Thereafter, the A/N ratios started to decrease to 0.43 at approximately 15 years. In contrast, the A/N ratios did not change with age in ATH/OSA group (Figure 1A, 1C). Moreover, compared to the control group, the A/N ratios were significantly higher in the ATH/OSA participants (Mean (95% CI): 0.85(0.83 to 0.86), vs 0.56 (0.55 to 0.57), P=0.000, Table 1).
THE RELATION BETWEEN ATH/OSA AND AMYGDALA/HIPPOCAMPUS VOLUME RATIOS (A/H RATIOS):
Our results showed that hippocampal volumes in children with ATH/OSA were significantly lower than those in controls (Table 1). However, amygdala volumes and A/H ratios in children with ATH/OSA were both higher than those in controls, as shown in Table 1.
Further analysis explored the correlations between A/H ratios and clinical variables in the ATH/OSA group. The results of multiple linear regression analysis are presented in Table 2, which used the AHI, disease duration, A/N ratios, min SaO2, percent SaO2<90%, and mean SaO2 as the independent variables and A/H ratios as dependent variables among all ATH/OSA children. After controlling for age, sex, and BMI as confounding variables, the data showed that A/H ratios had significant positive correlations with the disease duration (R2=0.183, β=0.109, P=0.012). A longer duration of disease was associated with higher A/H ratios. Moreover, there was a significant positive correlation between the A/H ratios and the hypoxemia variables: AHI (R2=0.219, β=0.501, P=0.000) and percentage of SaO2 <90% (R2=0.085, β=0.286, P=0.005). In contrast, the mean SaO2 showed a significant negative correlation with the A/H ratios (R2=0.203, β=−0.448, P=0.000). However, there was no significant relationship observed between the size of the adenotonsillar (A/N ratios) and the A/H ratios (R2=0.005, β=0.038, P=0.717). In addition, in the control group, A/H ratios showed a statistically significant positive correlation with the ages of healthy children (R2=0.429, β=0.576, P=0.000, Table 3).
Figure 2A–2D presents the correlation between the A/H ratios and AHI, disease duration, percent SaO2 <90%, and mean SaO2 in all ATH/OSA children. The disease duration showed a statistically significant positive correlation with A/H ratios (r=0.406; 95% CI, 0.206 to 0.585; P=0.000, Figure 2A). In contrast, mean SaO2 showed a significant negative correlation with the A/H ratios (r=−0.442; 95% CI, −0.623 to −0.256; P=0.000, Figure 2B). Moreover, the AHI and percentage of SaO2 <90% showed significantly positive correlations with the A/H ratios (r=0.487; 95% CI, 0.298 to 0.619; P=0.000; and r=0.280; 95% CI, 0.061 to 0.485; P=0.005, respectively, Figure 2C, 2D). In addition, in the control group, A/H ratios showed a statistically significant positive correlation with the ages of healthy children (r=0.647; 95% CI, 0.510 to 0.756; P=0.000, Figure 3).
Discussion
In the present study, we assessed the adenotonsillar size, air pathway obstruction, amygdala, and hippocampus volumes of ATH/OSA pediatric patients. The results showed that ATH/OSA pediatric patients had higher amygdala volumes and A/H ratios but lower hippocampus volumes than healthy pediatric patients. Moreover, we found that the A/H ratios of ATH/OSA pediatric patients were correlated with the disease duration of ATH/OSA and hypoxemia conditions.
Recent studies have revealed that OSA can induce hypoxia in patients, which then contributes to histological and pathological changes in multiple organs of humans, including brain tissues. Pathological changes in brain structures could be observed by MRI. Canessa et al investigated the brain structures of pediatric OSA patients and found decreased volumes in multiple regions of the brain (hippocampus, left posterior parietal cortex, and right superior frontal gyrus) in pediatric OSA patients compared with healthy controls [20], which was consistent with our data. Philby et al reported that gray matter volumes of the superior frontal and prefrontal and superior and lateral parietal cortices were clearly decreased in pediatric OSA patients [3]. Kheirandish-Gozal et al suggested that the changes on MRI indicated acute pathological insults by OSA [4], which could then impair mood function and cognitive ability.
OSA can have a direct effect on cognitive ability, including memory, attention, psychomotor speed, executive, verbal, and visual-spatial skills [21]. Wu et al investigated 437 pediatric OSA patients and identified that 33.4% of pediatric OSA patients had attention-deficit hyperactivity disorder [22], in which multiple parameters of cognitive abilities indices, including verbal and visual memory indices, attention index, and speech index, were all significantly decreased in the OSA subjects [23]. Bilyukov et al investigated 30 pediatric congenital heart disease patients and found that these patients combined with OSA had significantly lower intelligence quotient (IQ) levels than patients without OSA [24]. In a study on 79 pediatric OSA patients, Esposito et al found that these pediatric OSA patients had more errors in executive function evaluation and cognitive assessment than healthy controls [25]. In a meta-analysis including 11 papers (2776 patients) by Mauro et al, the data showed that treatment with adenotonsillectomy in ATH/OSA pediatric patients improved behavioral disorders [26]. Therefore, the data demonstrate that the pathology of OSA contributes to changes in behavior and cognitive ability.
In the present study, our data showed that pediatric OSA patients had higher volumes of the amygdala but lower volumes of the hippocampus than healthy controls. The changes in the ratios of the amygdala to the hippocampus may contribute to behavioral changes in children, which has been revealed in recent years. Mert et al found that amygdala volume was associated with children’s levels of anxiety and depression [27]. Additionally, the volume of the hippocampus was related to behavioral change or emotional disturbance. Koolschijn et al suggested that hippocampal volume was inversely related to internalizing behavior problems, including anxious/depressive, withdrawal and somatic symptoms [28]. Moreover, our data showed that the changes in A/H ratios were related to the duration of disease, duration of hypoxia in sleep, and SaO2 levels. We suggest that all 3 variables could be related to hypoxia severity and duration, consistent with studies on animal models that demonstrated pathological changes in brain tissues induced by OSA. Ward et al observed a decline in spatial memory in rat OSA models [29]. Gozal et al demonstrated that intermittent hypoxemia could induce apoptosis of neurons, proliferation of glia, and cytoarchitectural disorganization in the rat hippocampal CA1 region and the frontoparietal cortex [30]. Lloyd et al found that OSA could activate microglia in the brains of rats with OSA, which then induced inflammatory changes in the brain [31]. Furthermore, intermittent hypoxemia could damage hippocampal neurons through regulation of long-term potentiation (LTP), which is a physiological NMDA-dependent mechanism and participates in the biological function of learning and memory [32]. Therefore, the pathological changes in neurons of the brain induced by OSA could eventually impair cognitive ability and mood function in pediatric OSA patients.
In addition, adenotonsillar hypertrophy is considered to involve abnormally large adenoids and tonsils composed of lymphoid cells. Papaioannou et al investigated the size of the adenotonsillar in children aged 0–15.9 years by MRI, and the results showed that adenoid size increased during the first 7–8 years of life and then decreased gradually in children without snoring, whereas the adenoid size was increased but not correlated with age in children with snoring [33]. Ishida et al investigated the size of adenoids and tonsils in Japanese individuals aged 6–20 years, and they found that adenoids and tonsils were smaller in young adults compared to children of preschool age [34]. Our study investigated A/N ratios in all pediatric subjects, and we found a similar trend of A/N ratios, consistent with previous studies. The A/N ratios started to increase from age 2, peaked at age 6, and then started to decrease in the healthy children. In contrast, the A/N ratios did not change with age in the ATH/OSA group.
Conclusions
In summary, our study suggested that ATH pathology could lead to an increase in the A/H ratio, which might result in changes in behavior, mood, or cognitive ability in ATH pediatric patients. Additionally, the A/H ratios were correlated with disease duration and hypoxemia, which indicated that the treatment window should be considered during development of the therapeutic strategy. We also found that the increasing A/N ratios were only identified in the first 5 years of life, and its clinical significance warrants further investigation.
Figures
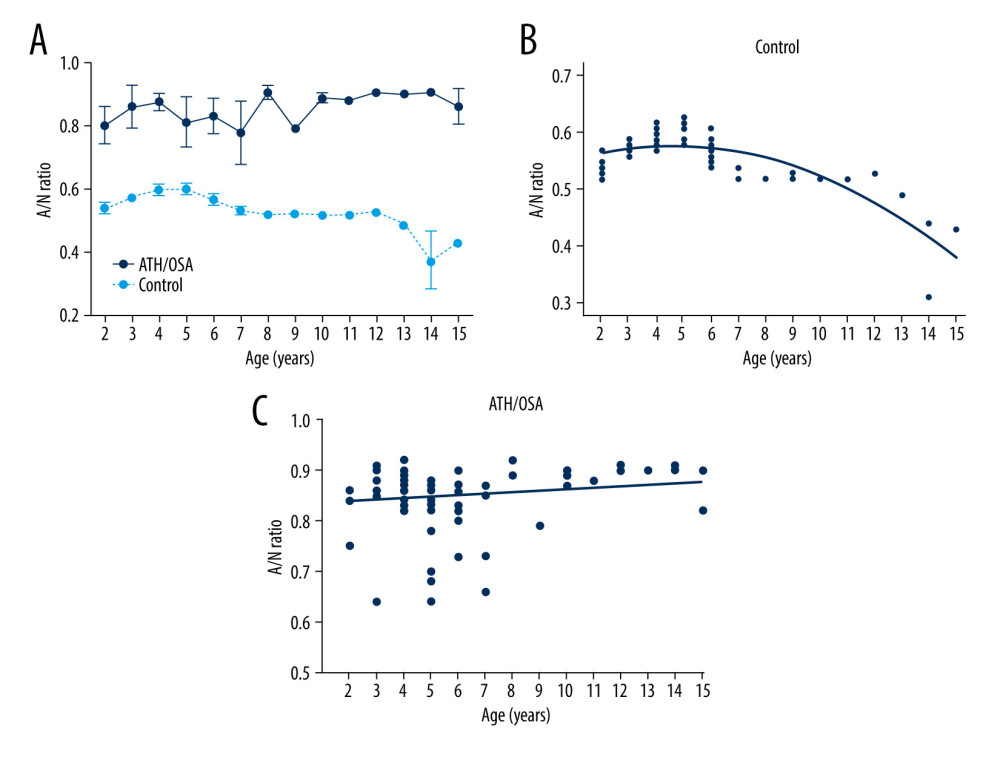 Figure 1. The A/N ratios of involved subjects at different ages. (A) In the control group of healthy children, the data showed that A/N ratios were 0.54 at approximately age 2, increased to 0.60 at approximately age 5, and then started to decrease to 0.43 at approximately age 15. In the ATH/OSA group, A/N ratios were large irrespective of age. Data are presented as the mean±SD. (B) Curve fitting (control group) and (C) line fitting (ATH/OSA group) for the associations of A/N ratios with age. In the control group, R2=0.662 and P=0.00 by ANOVA. In the ATH/OSA group, R2=0.012 and P=0.523, by ANOVA. By SPSS V.26 (IBM SPSS, Armonk, NY, USA).
Figure 1. The A/N ratios of involved subjects at different ages. (A) In the control group of healthy children, the data showed that A/N ratios were 0.54 at approximately age 2, increased to 0.60 at approximately age 5, and then started to decrease to 0.43 at approximately age 15. In the ATH/OSA group, A/N ratios were large irrespective of age. Data are presented as the mean±SD. (B) Curve fitting (control group) and (C) line fitting (ATH/OSA group) for the associations of A/N ratios with age. In the control group, R2=0.662 and P=0.00 by ANOVA. In the ATH/OSA group, R2=0.012 and P=0.523, by ANOVA. By SPSS V.26 (IBM SPSS, Armonk, NY, USA). 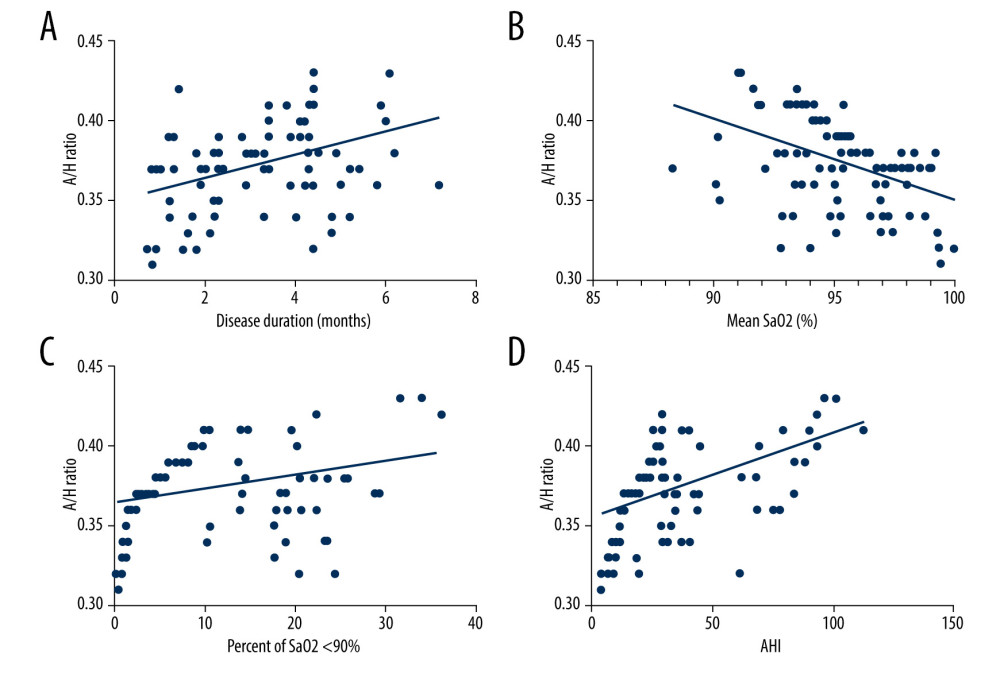 Figure 2. Correlation of amygdala/hippocampus ratios with clinical variables. (A–D) Amygdala/hippocampus ratios were associated with the duration of ATH/OSA disease, mean SaO2, percentage time of SaO2 <90%, and AHI in the ATH/OSA group. Line fitting for the associations of amygdala/hippocampus ratios with disease duration (A), mean SaO2 (B), percentage time of SaO2 <90% (C), and AHI (D). Mean SaO2 – mean oxygen saturation of arterial blood; amygdala/hippocampus ratios – A/H ratios, AHI – apnea-hypopnea index. Created using SPSS V.26 (IBM SPSS, Armonk, NY, USA).
Figure 2. Correlation of amygdala/hippocampus ratios with clinical variables. (A–D) Amygdala/hippocampus ratios were associated with the duration of ATH/OSA disease, mean SaO2, percentage time of SaO2 <90%, and AHI in the ATH/OSA group. Line fitting for the associations of amygdala/hippocampus ratios with disease duration (A), mean SaO2 (B), percentage time of SaO2 <90% (C), and AHI (D). Mean SaO2 – mean oxygen saturation of arterial blood; amygdala/hippocampus ratios – A/H ratios, AHI – apnea-hypopnea index. Created using SPSS V.26 (IBM SPSS, Armonk, NY, USA). 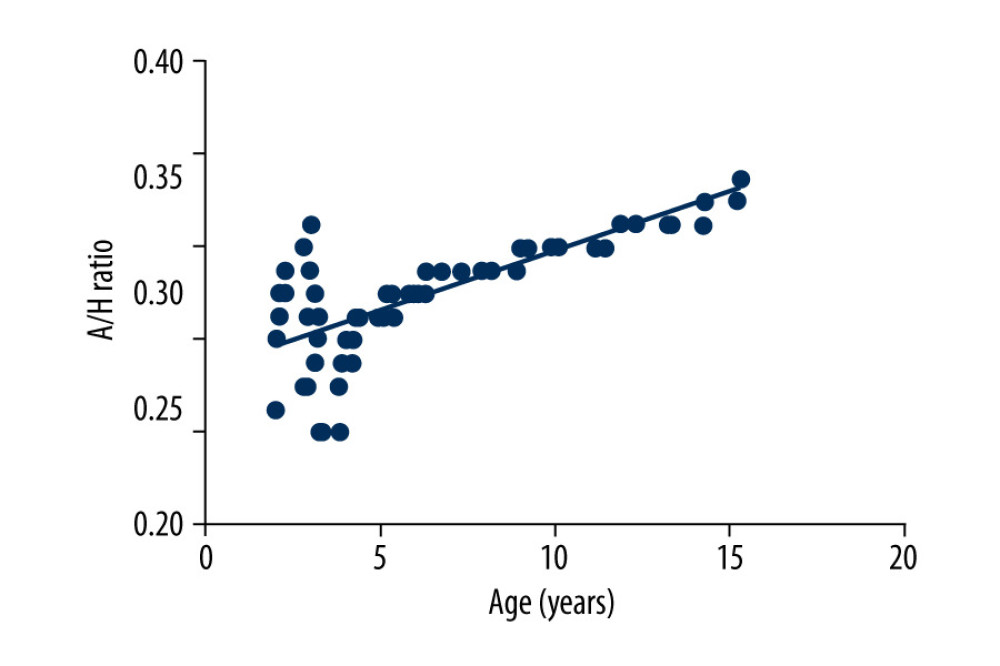 Figure 3. Correlation between the amygdala/hippocampus ratios and age in the control group of healthy children. Created using SPSS V.26 (IBM SPSS, Armonk, NY, USA).
Figure 3. Correlation between the amygdala/hippocampus ratios and age in the control group of healthy children. Created using SPSS V.26 (IBM SPSS, Armonk, NY, USA). Tables
Table 1. Demographic characteristics and clinical variables of subjects.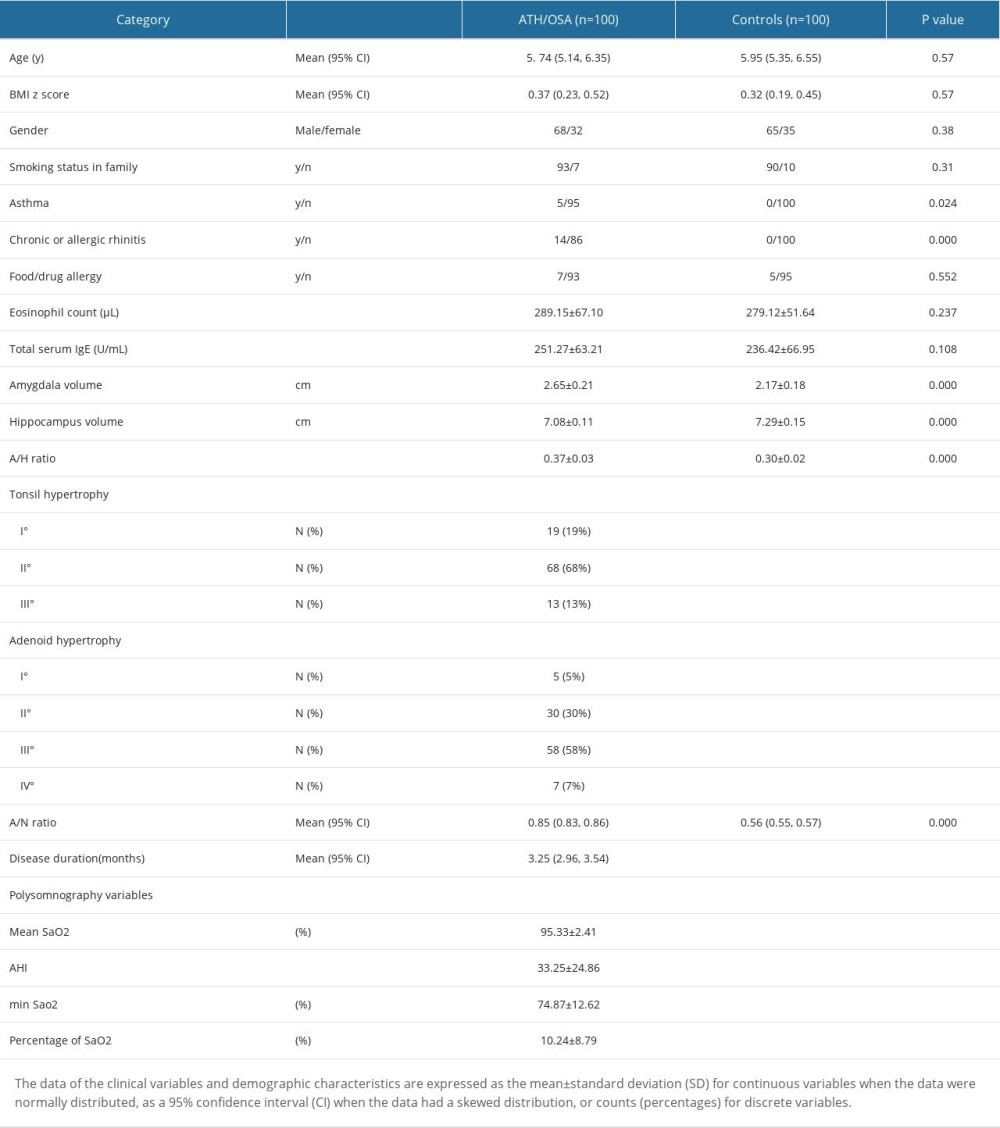 Table 2. Correlation between Amygdala: Hippocampus volume (A/H ratio) and clinical variables of ATH/OSA pediatric patients using multiple linear regression analysis.
Table 2. Correlation between Amygdala: Hippocampus volume (A/H ratio) and clinical variables of ATH/OSA pediatric patients using multiple linear regression analysis.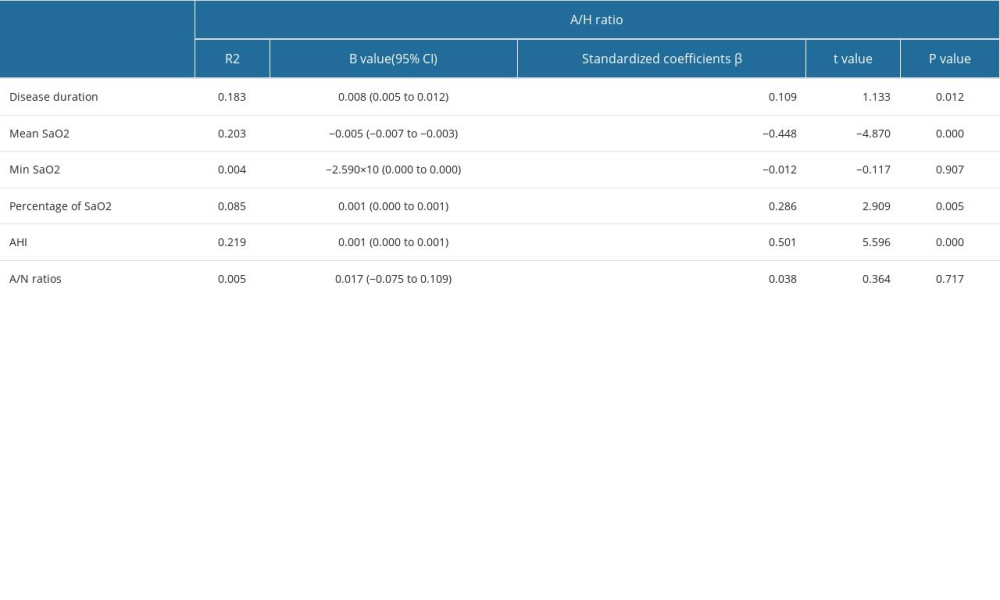 Table 3. Correlation between Amygdala: Hippocampus volume (A/H ratio) and clinical variables of healthy children using multiple linear regression analysis.
Table 3. Correlation between Amygdala: Hippocampus volume (A/H ratio) and clinical variables of healthy children using multiple linear regression analysis.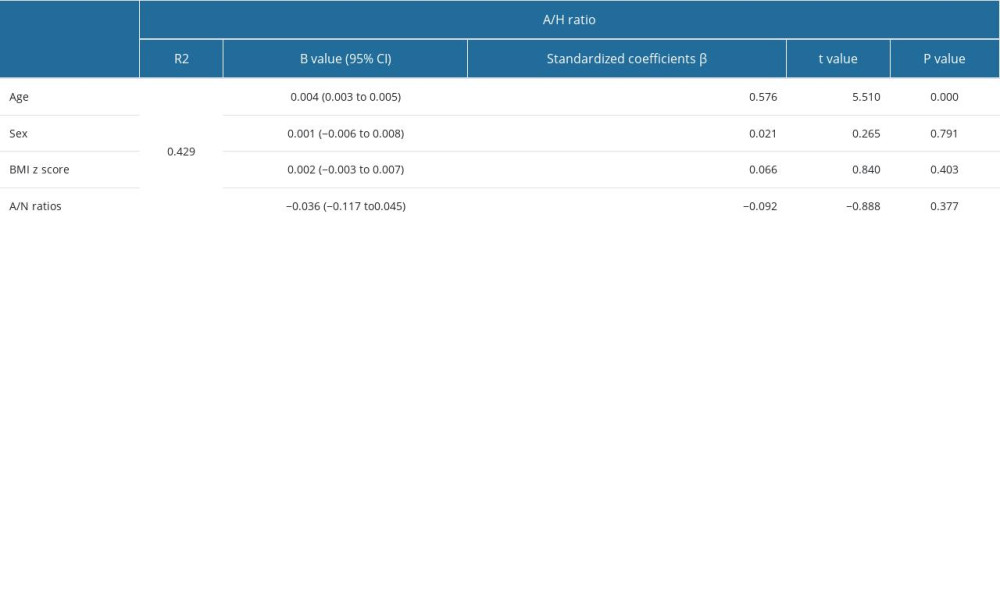
References
1. Bixler EO, Vgontzas AN, Lin HM, Sleep disordered breathing in children in a general population sample: prevalence and risk factors: Sleep, 2009; 32; 731-36
2. Marcus CL, Sleep-disordered breathing in children: Curr Opin Pediatr, 2000; 12; 208-12
3. Philby MF, Macey PM, Ma RA, Reduced regional grey matter volumes in pediatric obstructive sleep apnea: Sci Rep, 2017; 7; 44566
4. Kheirandish-Gozal L, Sahib AK, Macey PM, Regional brain tissue integrity in pediatric obstructive sleep apnea: Neurosci Lett, 2018; 682; 118-23
5. Gozal D, CrossTalk proposal: the intermittent hypoxia attending severe obstructive sleep apnoea does lead to alterations in brain structure and function: J Physiol, 2013; 591; 379-81
6. Hunter SJ, Gozal D, Smith DL, Effect of sleep-disordered breathing severity on cognitive performance measures in a large community cohort of young school-aged children: Am J Respir Crit Care Med, 2016; 194; 739-47
7. O’Brien LM, Mervis CB, Holbrook CR, Neurobehavioral correlates of sleep-disordered breathing in children: J Sleep Res, 2004; 13; 165-72
8. Cha J, Zea-Hernandez JA, Sin S, The effects of obstructive sleep apnea syndrome on the dentate gyrus and learning and memory in children: J Neurosci, 2017; 37; 4280-88
9. Schumann CM, Bauman MD, Amaral DG, Abnormal structure or function of the amygdala is a common component of neurodevelopmental disorders: Neuropsychologia, 2011; 49; 745-59
10. Nalivaeva NN, Turner AJ, Zhuravin IA, Role of prenatal hypoxia in brain development, cognitive functions, and neurodegeneration: Front Neurosci, 2018; 12; 825
11. Anand KS, Dhikav V, Hippocampus in health and disease: An overview: Ann Indian Acad Neurol, 2012; 15; 239-46
12. Plessen KJ, Bansal R, Zhu H, Hippocampus and amygdala morphology in attention-deficit/hyperactivity disorder: Arch Gen Psychiatry, 2006; 63; 795-807
13. MacMillan S, Szeszko PR, Moore GJ, Increased amygdala: hippocampal volume ratios associated with severity of anxiety in pediatric major depression: J Child Adolesc Psychopharmacol, 2003; 13; 65-73
14. Raman L, Kong X, Gilley JA, Kernie SG, Chronic hypoxia impairs murine hippocampal development and depletes the postnatal progenitor pool by attenuating mammalian target of rapamycin signaling: Pediatr Res, 2011; 70; 159-65
15. Carty ML, Wixey JA, Kesby J, Long-term losses of amygdala corticotropin-releasing factor neurons are associated with behavioural outcomes following neonatal hypoxia-ischemia: Behav Brain Res, 2010; 208; 609-18
16. Alchanatis M, Zias N, Deligiorgis N, Sleep apnea-related cognitive deficits and intelligence: an implication of cognitive reserve theory: J Sleep Res, 2005; 14; 69-75
17. Brodsky L, Modern assessment of tonsils and adenoids: Pediatr Clin North Am, 1989; 36; 1551-69
18. Parikh SR, Coronel M, Lee JJ, Brown SM, Validation of a new grading system for endoscopic examination of adenoid hypertrophy: Otolaryngol Head Neck Surg, 2006; 135; 684-87
19. Fujioka M, Young LW, Girdany BR, Radiographic evaluation of adenoidal size in children: adenoidal-nasopharyngeal ratio: Am J Roentgenol, 1979; 133; 401-4
20. Canessa N, Castronovo V, Cappa SF, Obstructive sleep apnea: Brain structural changes and neurocognitive function before and after treatment: Am J Respir Crit Care Med, 2011; 183; 1419-26
21. Bilyukov RG, Nikolov MS, Pencheva VP, Cognitive impairment and affective disorders in patients with obstructive sleep apnea syndrome: Front Psychiatry, 2018; 9; 357
22. Wu J, Gu M, Chen S, Factors related to pediatric obstructive sleep apnea-hypopnea syndrome in children with attention deficit hyperactivity disorder in different age groups: Medicine (Baltimore), 2017; 96; e8281
23. Madaeva I, Berdina O, Polyakov V, Kolesnikov S, Obstructive sleep apnea and hypertension in adolescents: Effect on neurobehavioral and cognitive functioning: Can Respir J, 2016; 2016; 3950914
24. Combs D, Edgin JO, Klewer S, OSA and neurocognitive impairment in children with congenital heart disease: Chest, 2020; 158; 1208-17
25. Esposito M, Antinolfi L, Gallai B, Executive dysfunction in children affected by obstructive sleep apnea syndrome: An observational study: Neuropsychiatr Dis Treat, 2013; 9; 1087-94
26. Di Mauro P, Cocuzza S, Maniaci A, The effect of adenotonsillectomy on children’s behavior and cognitive performance with obstructive sleep apnea syndrome: State of the art: Children (Basel), 2021; 8(10); 921
27. Merz EC, Tottenham N, Noble KG, Socioeconomic status, amygdala volume, and internalizing symptoms in children and adolescents: J Clin Child Adolesc Psychol, 2018; 47; 312-23
28. Koolschijn PC, van IMH, Bakermans-Kranenburg MJ, Crone EA, Hippocampal volume and internalizing behavior problems in adolescence: Eur Neuropsychopharmacol, 2013; 23; 622-28
29. Ward CP, McCoy JG, McKenna JT, Spatial learning and memory deficits following exposure to 24 h of sleep fragmentation or intermittent hypoxia in a rat model of obstructive sleep apnea: Brain Res, 2009; 1294; 128-37
30. Gozal D, Daniel JM, Dohanich GP, Behavioral and anatomical correlates of chronic episodic hypoxia during sleep in the rat: J Neurosci, 2001; 21; 2442-50
31. Lloyd EE, Durgan DJ, Martini SR, Bryan RM, Pathological effects of obstructive apneas during the sleep cycle in an animal model of cerebral small vessel disease: Hypertension, 2015; 66; 913-17
32. Arias-Cavieres A, Khuu MA, Nwakudu CU, A HIF1a-dependent pro-oxidant state disrupts synaptic plasticity and impairs spatial memory in response to intermittent hypoxia: eNeuro, 2020; 7 ENEURO.0024-20.2020
33. Puig F, Rico F, Almendros I, Vibration enhances interleukin-8 release in a cell model of snoring-induced airway inflammation: Sleep, 2005; 28; 1312-16
34. Ishida T, Manabe A, Yang SS, Patterns of adenoid and tonsil growth in Japanese children and adolescents: A longitudinal study: Sci Rep, 2018; 8; 17088
Figures
Figure 1. The A/N ratios of involved subjects at different ages. (A) In the control group of healthy children, the data showed that A/N ratios were 0.54 at approximately age 2, increased to 0.60 at approximately age 5, and then started to decrease to 0.43 at approximately age 15. In the ATH/OSA group, A/N ratios were large irrespective of age. Data are presented as the mean±SD. (B) Curve fitting (control group) and (C) line fitting (ATH/OSA group) for the associations of A/N ratios with age. In the control group, R2=0.662 and P=0.00 by ANOVA. In the ATH/OSA group, R2=0.012 and P=0.523, by ANOVA. By SPSS V.26 (IBM SPSS, Armonk, NY, USA).Figure 2. Correlation of amygdala/hippocampus ratios with clinical variables. (A–D) Amygdala/hippocampus ratios were associated with the duration of ATH/OSA disease, mean SaO2, percentage time of SaO2 <90%, and AHI in the ATH/OSA group. Line fitting for the associations of amygdala/hippocampus ratios with disease duration (A), mean SaO2 (B), percentage time of SaO2 <90% (C), and AHI (D). Mean SaO2 – mean oxygen saturation of arterial blood; amygdala/hippocampus ratios – A/H ratios, AHI – apnea-hypopnea index. Created using SPSS V.26 (IBM SPSS, Armonk, NY, USA).Figure 3. Correlation between the amygdala/hippocampus ratios and age in the control group of healthy children. Created using SPSS V.26 (IBM SPSS, Armonk, NY, USA). Tables
Table 1. Demographic characteristics and clinical variables of subjects.Table 2. Correlation between Amygdala: Hippocampus volume (A/H ratio) and clinical variables of ATH/OSA pediatric patients using multiple linear regression analysis.Table 3. Correlation between Amygdala: Hippocampus volume (A/H ratio) and clinical variables of healthy children using multiple linear regression analysis.Table 1. Demographic characteristics and clinical variables of subjects.Table 2. Correlation between Amygdala: Hippocampus volume (A/H ratio) and clinical variables of ATH/OSA pediatric patients using multiple linear regression analysis.Table 3. Correlation between Amygdala: Hippocampus volume (A/H ratio) and clinical variables of healthy children using multiple linear regression analysis. In Press
Clinical Research
Body Weight and Insulin Resistance Indicators Among ChildrenMed Sci Monit In Press; DOI: 10.12659/MSM.951434
Clinical Research
Comparison of Radiographic Cervical Sagittal Alignment Parameters in Patients With Nonspecific Neck Pain, D...Med Sci Monit In Press; DOI: 10.12659/MSM.952950
Clinical Research
Combined Fibrinogen and Urinary α1-Microglobulin as Predictors of Respiratory Tract Infection in Children w...Med Sci Monit In Press; DOI: 10.12659/MSM.951066
Database Analysis
Evaluation of Salivary Total Oxidant Status (TOS) and Total Antioxidant Status (TAS) in Orthodontic Patient...Med Sci Monit In Press; DOI: 10.12659/MSM.952052
Most Viewed Current Articles
17 Jan 2024 : Review article 14,175,576
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,756,620
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,465,966
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,651
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387