30 September 2022: Clinical Research
Effects of Left Atrial Appendage Closure on Neuroendocrine Function in Patients with Nonvalvular Atrial Fibrillation
Fei Wang1ABE*, Zhong-bao Ruan1BDG, Ge-cai Chen1BC, Jun-guo Zhu1CF, Li Zhu1ADOI: 10.12659/MSM.937586
Med Sci Monit 2022; 28:e937586






Abstract
BACKGROUND: The left atrial appendage (LAA) is an organ with neuroendocrine function. It remains unclear whether left atrial appendage closure (LAAC) has physiological effects on neuroendocrine function in patients with nonvalvular atrial fibrillation (NVAF). In the present study, we aimed to investigate the effects of LAAC on neuroendocrine function in patients with NVAF.
MATERIAL AND METHODS: We enrolled 20 patients with NVAF treated by LAAC in Jiangsu Taizhou People’s Hospital from October 2019 to October 2020. Blood samples were collected 1 day before LAAC and 12 months after LAAC. Plasma concentrations of adrenaline, aldosterone, pro-atrial natriuretic peptide (NT-proANP), and N-terminal pro-B-type natriuretic peptide (NT-proBNP) were measured.
RESULTS: LAAC was successfully performed in all patients, without serious complications. Compared with the preoperative levels, there was no significant difference in the levels of NT-proANP, NT-proBNP, and epinephrine at 12 months after LAAC (P>0.05). However, there was a significant decrease in aldosterone level at 12 months post-procedure (209.04±132.98 pg/ml) compared with pre-procedure baseline (279.08±166.88 pg/ml, P=0.04). There was no correlation between the compression rate of the occlusion and the reduction of aldosterone (Kendall’s Tau-b=0.159, P=0.351).
CONCLUSIONS: LAAC can be safely and effectively performed in NVAF patients, and showed no significant effect on the adrenergic system and natriuretic peptides, but had an influence on the RAAS.
Keywords: Left Atrial Appendage Closure, Nonvalvular Atrial Fibrillation, Neuroendocrine Function, Adrenergic Agents, Aldosterone, Atrial Appendage, Atrial Fibrillation, atrial natriuretic factor, Epinephrine, Humans, Natriuretic Peptide, Brain, Treatment Outcome
Background
Nonvalvular atrial fibrillation (NVAF) is one of the most frequent arrhythmias in clinical practice, accounting for up to 1/3 of patients hospitalized for arrhythmias [1]. The prevalence of NVAF is increased with age, reaching as high as 17.4% in people age ≥85 years [2]. The prevention of thromboembolic complications is an important link in the treatment of NVAF. The left atrial appendage (LAA) is a key source of thrombosis in patients with NVAF. An increasing number of studies have indicated that the morphology of LAA seems to be crucially linked to the risk of stroke, and more than 90% of cases of thrombosis in patients with NVAF are directly linked to the LAA [3,4].
Currently, the oral anticoagulation (OAC) warfarin or novel oral anticoagulants (NOAC) is still a first-line treatment strategy for stroke prevention in NVAF patients [4]. However, the disadvantages and contraindications of OAC or NOAV promote the clinical application of left atrial appendage closure (LAAC). The safety and efficacy of LAAC regarding prevention of ischemic stroke events in patients with NVAF have been confirmed by several studies [6–10]. Under normal physiological conditions, the LAA not only has contractile function, but also can promote the secretion of atrial peptide (ANP), brain natriuretic peptide (BNP), and other neurohormones. However, there are limited data on the effect of LAAC on the neuroendocrine function of the LAA. In the present study, we aimed to explore the effects of LAAC on the neuroendocrine function of patients with NVAF.
Material and Methods
STUDY POPULATION:
From October 2019 to February 2020, 20 NVAF patients were enrolled at Jiangsu Taizhou People’s Hospital to undergo LAAC. All patients were included with the criteria as: age >18 years, NVAF, high risk for stroke (CHA2DS2-VASC score ≥2 for males and ≥3 for females, intolerance to therapy with long-term oral anticoagulants (INR value unstable, contraindications to anticoagulation, oral anticoagulant therapy failure: transient ischemic attack or stroke during anticoagulant therapy). The study was approved by the Ethics Committee of Jiangsu Taizhou People’s Hospital. Written informed consents were obtained from all patients before the procedure.
SPECIMEN COLLECTION AND ASSESSMENT OF NEUROENDOCRINE PROFILE:
Within 4 h of admission (pre-procedure) and 12 months after the LAAC (12 months post-procedure), approximately 10 ml of peripheral blood was drawn into ethylene diamine tetra-acetic acid (EDTA) anticoagulant tubes from each participant as they lay in supine position. All blood samples were collected after patients had fasted for at least 6 h. Plasma concentrations of adrenaline, aldosterone, pro-atrial natriuretic peptide (NT-proANP), and N-terminal pro-B-type natriuretic peptide (NT-proBNP) were measured with an ELISA kit used in strict accordance with the instructions. These assays were intended to assess changes in the adrenergic system, renin-angiotensin-aldosterone system (RAAS), and natriuretic peptides.
LAAC PROCEDURE:
As described previously [10], LAAC was performed in all patients using the WATCHMAN device. Briefly, transthoracic echocardiography (TTE) and cardiac computed tomography angiography (CCTA) were used to evaluate the feasibility of LAAC, with a focus on understanding the morphological structure of the LAA and LAA thrombus evaluation. Next, procedures were carried out using TEE and fluoroscopic guidance. Following a transseptal puncture, a WATCHMAN device of the appropriate size was delivered into the LAA through the delivery sheath. After a tug test, the device was released after confirmation of its proper positioning with minimal (<5 mm) or no residual peri-device leak via imaging.
POSTPROCEDURAL ANTICOAGULATION:
Generally, an anticoagulation regimen combined with antiplatelet therapy (clopidogrel or aspirin) was recommended for 3 months after LAAC. Subsequently, dual antiplatelet therapy (DAT, aspirin plus clopidogrel) was followed for another 3 months. This was followed by lifelong aspirin or clopidogrel if there were no persistent peri-device leaks more than 5 mm or device-related thrombosis detected at the TEE or CCTA follow-up. TEE or CCTA was routinely performed at 3 months, 6 months, and 12 months post-procedure for all patients.
STATISTICAL ANALYSIS:
SPSS 23.0 was used to analyze the experimental data. Continuous variables were described in the form of mean±standard deviation and analyzed using paired sample
Results
BASELINE CHARACTERISTICS:
A total of 20 patients who successfully underwent left atrial appendage occlusion and completed long-term follow-up were enrolled from October 2019 to October 2020. The mean age was 69.35±8.29 years old, including 4 females (25%) and 3 patients (15%) with paroxysmal NVAF. The average CHA2DS2-VASC score was 3.00±1.45 and the HAS-BLED score was 2.52±0.89. Detailed baseline characteristics are described in Table 1.
PROCEDURAL AND POSTPROCEDURAL PROTOCOLS:
LAAC was successfully performed in all patients. The average diameter of the LAA orifice measured by TEE during the operation was 24.34±3.05 mm, and the maximum depth was 25.26±3.06 mm. The size of occluders selected ranged from 21 mm to 33 mm, and the compression rate of the occluder was (18.13±3.54)%. After successful release of the device, mild leaks (<3 mm) were observed in 2 cases and moderate leak (3–5 mm) in 1 case. Pericardial effusion occurred in 1 patient and the condition was improved after a pericardial puncture. The anticoagulant therapy (rivaroxaban, dabigatran, or warfarin) combined with antiplatelet (aspirin or clopidogrel) was followed for 3 months after LAAC, then the combination of aspirin and clopidogrel was used for another 3 months, followed by lifelong aspirin or clopidogrel. The procedural details are shown in Table 2.
:
CTA and TEE were performed in all patients at 12 months post-LAAC. No device displacement or devicerelated thrombi was detected. No significant peri-device leaks (jet width >5 mm) were observed, while clinically acceptable peri-device leakage (2-mm residual shunt) occurred in 1 patient. LVEF at the 12-month follow-up was similar to the baseline levels. However, there was a significant change in left atrial (LA) size at the 12-month follow-up compared with the baseline (48.67±6.61 mm vs 50.42±5.12 mm, t=2.333,
IMPACT OF LAAC ON THE NEUROENDOCRINE SYSTEM:
As shown in Table 3 and Figure 1, compared with preoperative levels, there was no statistically significant difference in NT-proANP, NT-proBNP, or adrenaline levels at 12 months after LAAC (P>0.05). However, there was a significant decrease in aldosterone level at 12 months post-procedure (209.04±132.98 pg/ml) compared with the pre-procedure baseline (279.08±166.88 pg/ml, P=0.04). There was no correlation between the compression rate of the occlusion and the reduction of aldosterone (r=0.177, P=0.408) (Figure 2).
Discussion
Physiologically, the LAA is an organ with neuroendocrine function, which plays a critical role in the maintenance of system homeostasis. As we know, LAA is also a main source of ANP and BNP, which play critical roles in natriuresis [11]. ANP and BNP have been reported to influence the sympathetic nervous system and the RAAS, thus achieving the function of reducing cardiac load [12,13]. The extension of muscle cells of the LAA, oxytocin, and hypoxia are the main factors that stimulate the secretion of ANP and BNP [14,15]. Whether elimination of the LAA from systemic circulation via LAAC has any deleterious effects on the human body remains unknown. There are also few studies exploring whether LAAC reduces the release of natriuretic peptides, thus affecting the expression of hormones involved in sympathetic nerves and RAAS [16,17].
Lakkireddy et al demonstrated that levels of NT-proBNP and NT-proANP immediately increased after LAAC and recovered to the baseline level 3 months after surgery [18]. Another study found that, compared with preoperative levels, there was no significant change in NT-proBNP levels in patients at 1, 3, 6, 12, and 24 months after LAAC [19]. In the present study, compared with preoperative levels, there was no significant change in NT-proANP or NT-proBNP levels at 12 months after LAAC, which was consistent with the report by Herman et al [19].
Some early research found that the levels of epinephrine, norepinephrine, renin, and aldosterone were significantly reduced, which indicated that epicardial LAAC downregulated the adrenergic system and RAAS. No such effects were found after endocardial LAAC [18]. Therefore, the exact effects of LAAC on neuroendocrine function in patients with NVAF remain unclear or are controversial. In this study, compared with the baseline, there was no significant change in the level of adrenaline at 12 months after endocardial LAAC with the WATCHMAN device, which was consistent with the change of NT-proANP and NT-proBNP. However, the level of aldosterone was significantly decreased, which indicated a downregulation of the RAAS after LAAC. We inferred that the long-term pressure effect of the WATCHMAN device on the wall of the LAA could cause pathological changes in the LAA and its surrounding tissues by causing a decrease in aldosterone level, which was similar to the changes in the LAAC after suturing the LAA with the Lariat device [20].
To the best of our knowledge, upregulation of the RAAS has always occurred in patients with AF, which can promote the occurrence of atrial remodeling. LAAC can affect the remodeling of the LA from possible downregulation of the RAAS [21]. In our study, there was not only a significantly change in the level of aldosterone, but also a significantly change in the diameter of left atrial between the baseline (50.42±5.12 mm) and 12 months after LAAC (48.67±6.61 mm,
For reasons of stability, 8–20% device compression after LAAC with the WATCHMAN device should be targeted to obtain complete LAA closure [22]. In this study, the compression ratio of the plugging device ranged from 11% to 24%. Considering that a different compression ratio can cause different pressure on the LAA wall and its surrounding tissues, thus affecting the experimental results, we performed correlation analysis between LAA closure device compression rate and the reduction of aldosterone. The results suggested that there was no correlation between the compression ratio after WATCHMAN occluder implantation and the decline of aldosterone (r=0.177,
Conclusions
LIMITATIONS:
The results of the present study are based on a small sample. Therefore, a larger sample and longer follow-up are required to evaluate the effect of LAAC on neuroendocrine function in patients with NVAF.
Figures
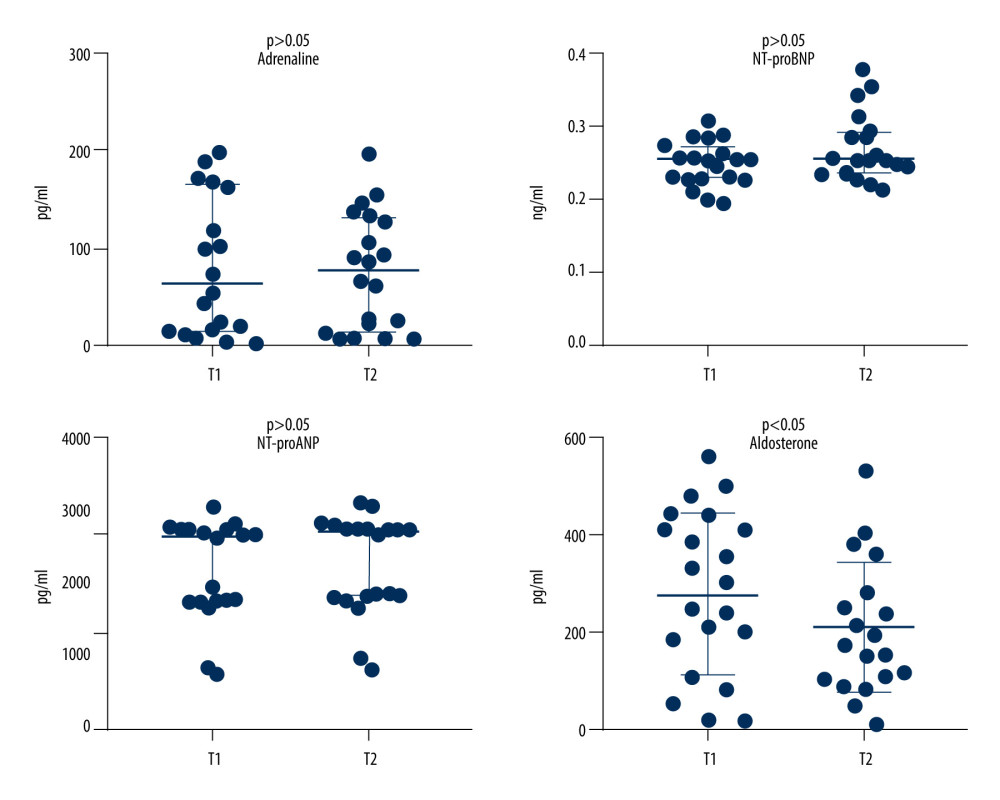 Figure 1. Changes of adrenaline, aldosterone, NT-proANP, and NT-proBNP at 12 months after LAAC compared with the pre-procedure. T1 – pre-procedure; T2 –12 months post-procedure.
Figure 1. Changes of adrenaline, aldosterone, NT-proANP, and NT-proBNP at 12 months after LAAC compared with the pre-procedure. T1 – pre-procedure; T2 –12 months post-procedure. 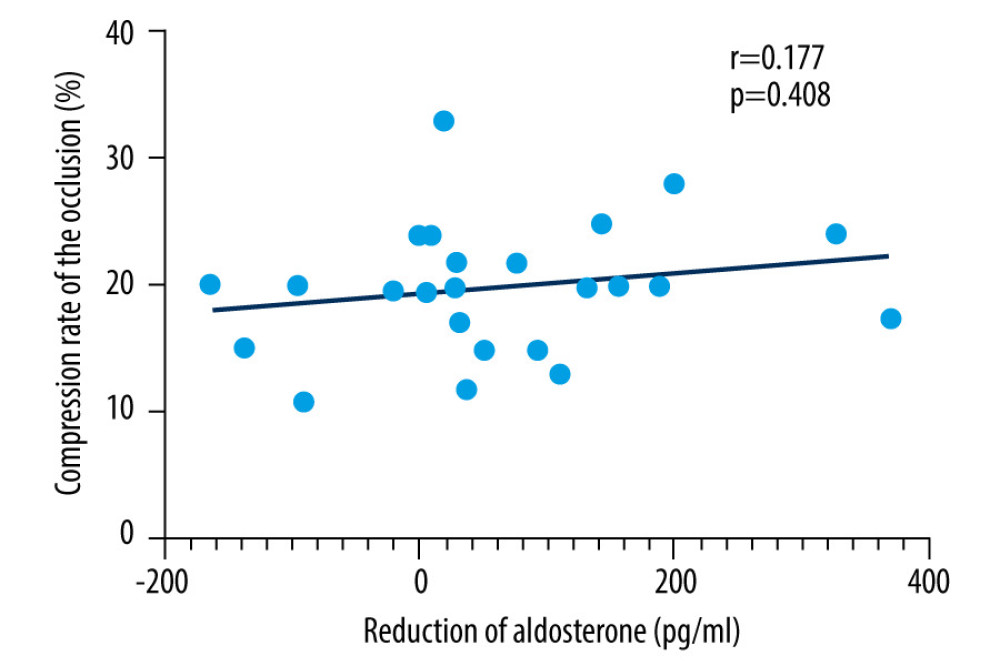 Figure 2. Spearman correlation analysis of the compression rate of the occlusion and the reduction of aldosterone.
Figure 2. Spearman correlation analysis of the compression rate of the occlusion and the reduction of aldosterone. References
1. Camm AJ, Kirchhof P, Lip GYH, Guidelines for the management of atrial: The Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC): Eur Heart J, 2010; 31; 2369-429
2. Schnabel RB, Yin XY, Gona P, Fifty-year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the community: Lancet, 2015; 386; 154-62
3. Ramlawi B, Saleh WKA, Edgerton J, The left atrial appendage: Target for stroke reduction in atrial fibrillation: Methodist Debakey Cardiovasc J, 2015; 11; 100-3
4. Sonaglioni A, Lombardo M, Nicolosi GL, Incremental diagnostic role of left atrial strain analysis in thrombotic risk assessment of nonvalvular atrial fibrillation patients planned for electrical cardioversion: Int J Cardiovasc Imaging, 2021; 37; 1539-50
5. Mumoli N, Amellone C, Antonelli G, Clinical discussions in antithrombotic therapy management in patients with atrial fibrillation: A Delphi Consensus Panel: CJC Open, 2020; 2; 641-51
6. Pacha HM, Al-khadra Y, Soud M, Percutaneous devices for left atrial appendage occlusion: A contemporary review: World J Cardiol, 2019; 11; 57-70
7. Schellinger PD, Tsivgoulis G, Steiner T, Percutaneous left atrial appendage occlusion for the prevention of stroke in patients with atrial fibrillation: Review and critical appraisal: J Stroke, 2018; 20; 281-91
8. Kabra R, Girotra S, Sarrazin MV, Clinical outcomes of mortality, readmissions, and ischemic stroke among medicare patients undergoing left atrial appendage closure via implanted device: AMA Netw Open, 2019; 2; e1914268
9. Parashar A, Tuzcu EM, Kapadia SR, Cardiac plug I and amulet devices: Left atrial appendage closure for stroke prophylaxis in atrial fibrillation: J Atr Fibrillation, 2015; 7; 1236
10. Suradi HS, Hijazi ZM, Left atrial appendage closure: outcomes and challenges: Neth Heart J, 2017; 25; 143-51
11. Wilber DJ, Neurohormonal regulation and the left atrial appendage: J Am Coll Cardiol, 2018; 71; 145-47
12. Phillips KP, Walker DT, Humphries JA, Combined catheter ablation for atrial fibrillation and WATCHMAN(R) left atrial appendage occlusion procedures: Five-year experience: J Arrhythmia, 2016; 32; 119-26
13. Nishikimi T, Maeda N, Matsuoka H, The role of natriuretic peptides in cardioprotection: Cardiovasc Res, 2006; 69; 318-28
14. Pandey KN, Guanylyl cyclase/atrial natriuretic peptide receptor-A: Role in the pathophysiology of cardiovascular regulation: Can J Physiol Pharmacol, 2011; 89; 557-73
15. Haanwinckel MA, Elias LK, Favaretto AL, Oxytocin mediates atrial natriuretic peptide release and natriuresis after volume expansion in the rat: Proc Natl Acad Sci USA, 1995; 92; 7902-6
16. Bartus K, Podolec J, Lee RJ, Atrial natriuretic peptide and brain natriuretic peptide changes after epicardial percutaneous left atrial appendage suture ligation using LARIAT device: J Physiol Pharmacol, 2017; 68; 117-23
17. Majunke N, Sandri M, Adams V, Atrial and brain natriuretic peptide secretion after percutaneous closure of the left atrial appendage with the WATCHMAN device: J Invasive Cardiol, 2015; 27; 448-52
18. Lakkireddy D, Turagam M, Afzal MR, Left atrial appendage closure and systemic homeostasis: J Am Coll Cardiol, 2018; 71; 135-44
19. Herman D, Osmancik P, Neuzil P, The effect of left atrial appendage closure on heart failure biomarkers: A PRAGUE-17 trial subanalysis: J Cardiovasc Electrophysiol, 2021; 32; 2645-54
20. Maybrook R, Pillarisetti J, Yarlagadda V, Electrolyte and hemodynamic changes following percutaneous left atrial appendage ligation with the LARIAT device: J Interv Card Electrophysiol, 2015; 43(3); 245-51
21. Paweł W, Janusz S, Iwona G, Left atrial mechanical remodelling assessed as the velocity of left atrium appendage wall motion during atrial fibrillation is associated with maintenance of sinus rhythm after electrical cardioversion in patients with persistent atrial fibrillation: PLoS One, 2020; 15; e0228239
22. Glikson M, Wolff R, Hindricks G, EHRA/EAPCI expert consensus statement on catheter-based left atrial appendage occlusion – an update: Europace, 2020; 22; 184
Figures
Tables
 Table 1. Baseline characteristics of the included patients.
Table 1. Baseline characteristics of the included patients.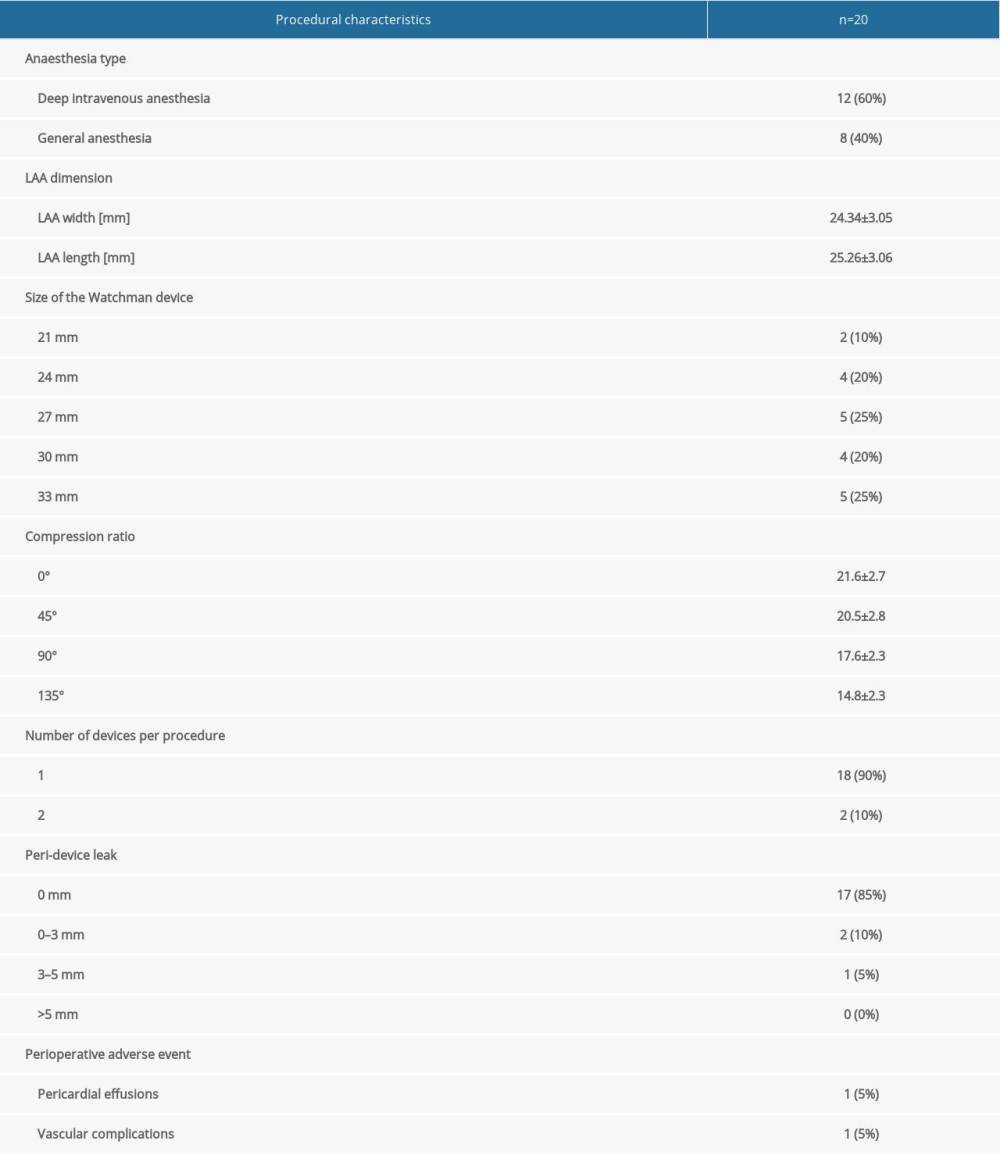 Table 2. Procedural characteristics.
Table 2. Procedural characteristics. Table 3. Impact of LAAC on adrenaline, aldosterone, NT-proANP, and NT-proBNP.Table 1. Baseline characteristics of the included patients.Table 2. Procedural characteristics.Table 3. Impact of LAAC on adrenaline, aldosterone, NT-proANP, and NT-proBNP.
Table 3. Impact of LAAC on adrenaline, aldosterone, NT-proANP, and NT-proBNP.Table 1. Baseline characteristics of the included patients.Table 2. Procedural characteristics.Table 3. Impact of LAAC on adrenaline, aldosterone, NT-proANP, and NT-proBNP. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387