06 December 2022: Clinical Research
Surgical Outcomes of Regional Versus General Anesthesia in 203 Patients with Upper- and Lower-Extremity Amputation: A Retrospective Study from a Single Center in Turkey
Nurettin KurtDOI: 10.12659/MSM.938603
Med Sci Monit 2022; 28:e938603






Abstract
BACKGROUND: This retrospective study from a single center in Turkey aimed to compare the surgical results of regional anesthesia and general anesthesia in 203 patients with upper- and lower-extremity amputations.
MATERIAL AND METHODS: The study population consisted of patients who underwent extremity amputation between 2017 and 2021. Patients’ demographic data, comorbidities, American Society of Anesthesiology (ASA) scores, amputated extremities, causes and extents of amputations, length of hospital stay, associated mortality/morbidity, and postoperative 90-day mortality data were comparatively analyzed between the groups created according to the anesthesia methods used in amputations.
RESULTS: The study consisted of 203 patients, of whom 80.8% were male. The most commonly used anesthesia method was peripheral nerve blocks (32.5%), followed by spinal anesthesia (31.5%), general anesthesia (31.0%), epidural anesthesia (2.0%), combined spinal-epidural anesthesia (1.5%), and sedo-analgesia (1.5%). Of the amputations performed, 37.0% were upper-extremity and 63.0% were lower-extremity. Peripheral nerve blocks were used most frequently in upper-extremity amputations (71.5%), and spinal anesthesia was used most frequently in lower-extremity amputations (48.9%). The mean length of hospital stay of the patients who underwent surgery under regional anesthesia methods was shorter than that of those who underwent general anesthesia (8.7±7.4 days vs 15.0±20.6 days). The mortality rate was 0.5% in the first 24 h, 0.5% in the next 48 h, and 4.9% in total.
CONCLUSIONS: The study findings demonstrated that performing extremity amputations under regional anesthesia techniques, particularly peripheral nerve blocks, reduces mortality/morbidity, the need for postoperative intensive care, mean length of stay in hospital, and hospital costs.
Keywords: Amputation, Nerve Block, Humans, Male, United States, Female, Turkey, Anesthesia, General, Lower Extremity, Treatment Outcome
Background
Extremity amputation is a life-changing event that causes significant loss of function. It is estimated that 41 000 people lived with major upper-extremity amputations in 2005 [1]. More than 150 000 people undergo lower-extremity amputation surgery in the United States each year [2]. Extremity amputations are one of the oldest commonly used types of surgery. Extremity amputations lead to both psychological and physical disabilities in patients. The surgical techniques, anesthesia methods used in amputations, and the timing of amputation affect the related mortality and morbidity rates [3]. Traffic accidents, diabetes mellitus (DM), atherosclerosis, hypertension (HT), and peripheral vascular diseases are among the diseases that lead to performance of extremity amputations. Traumatic amputations are the most common type of amputation, and complications related to diabetes mellitus (DM) are the most common cause of non-traumatic amputations [4,5].
Various anesthesia methods are used within the scope of current clinical practices, including general anesthesia (GA), epidural anesthesia (EA), spinal anesthesia (SA), combined spinal-epidural (CSE) anesthesia, peripheral nerve blocks (PNB), and sedoanalgesia [6]. Among these methods, regional anesthesia techniques are increasingly used in recent years. Regional anesthesia techniques used in extremity surgeries have advantages such as early mobilization, shorter hospital stay, postoperative analgesic effect, lower thromboembolism risk, less transfusion need, and lower costs. Regional anesthesia techniques positively affect perioperative and postoperative mortality and morbidity rates related to extremity amputations, particularly in elderly patients [7].
A thorough review of the literature indicated that the studies on this subject were explicitly directed at anesthesia methods, the causes of amputation, or morbidity and mortality rates and complications. Therefore, there is a need for studies that evaluate amputations in detail. To this end, this study has been designed to fill the gap in that respect and was conducted with 203 cases as the largest case series to date that evaluates multiple parameters at once.
Based on these, this retrospective study from a single center in Turkey aimed to compare all aspects of the surgical results of regional anesthesia and general anesthesia in 203 patients with upper- and lower-extremity amputations.
Material and Methods
RESEARCH DESIGN:
This study is a retrospective review of patients who underwent upper- and/or lower-extremity amputation surgery in a single center within 5 years (2017–2022). The protocol of this retrospective study was approved by Van Yuzuncu Yil University Faculty of Medicine Clinical Research Ethics Committee in advance (Approval No. 2022/04-12, Approval Date: 15.04.2022). The study population consisted of patients who underwent upper- and/or lower-extremity amputation using any of the general or regional anesthesia methods between 2017 and 2021 in Van Yuzuncu Yil University Medical Faculty Hospital. Detailed informed written consent was obtained from all patients before the operation.
The data of the patients were obtained from the hospital information management system and the patient follow-up forms for each patient. These patient records were reviewed and analyzed by the author. Cases whose data were fully obtained and who underwent surgery under either general anesthesia or regional anesthesia techniques were included in the study. The patients whose data could not be accessed or were missing, who underwent local anesthesia, or who undergwent revision surgery were not included in the study. In the end, a total of 203 patients aged 18–100 years and whose informed consent was obtained were included in the study sample.
Demographic factors, American Society of Anesthesiologists (ASA) scores, and medical comorbidities, including diabetes mellitus (DM), hypertension (HT), coronary artery disease (CAD), chronic kidney failure (CRF), respiratory system diseases (RSD), central nervous system diseases (CNSD), renal transplantation, and smoking were recorded. The patients’ need for postoperative intensive care unit (ICU), discharge times, 90-day mortality, and transfusion needs of blood products were also analyzed.
The study population was divided into 2 groups according to the anesthesia technique: general and regional anesthesia. Regional anesthesia techniques included spinal, epidural, combined spinal-epidural anesthesia, and peripheral nerve blocks. General anesthesia consisted of endotracheal intubation with a combination of inhalational/intravenous anesthetics for the maintenance of anesthesia. The patients were also divided into 2 groups as upper- and lower-extremity amputations according to the extremity amputation performed.
Patients’ demographic data, comorbidities, and American Society of Anesthesiology (ASA) scores, amputated extremities, causes and extents of amputations, associated complications, length of hospital stay, and postoperative 90-day mortality data were comparatively analyzed between the groups created according to the anesthesia methods used in upper- and lower-extremity amputations.
STATISTICAL ANALYSIS:
The descriptive statistics obtained from the collected research data were expressed as mean with standard deviation, median with minimum and maximum, frequency, and percentage values. The SPSS 28.0 (SPSS for Windows, version 28.0, IBM Corp., Armonk, NY, USA, 2021) software package was used in the statistical analyses.
Results
There were 206 patients who underwent upper- and/or lower-extremity amputations in the Van Yuzuncu Yil University Medical Faculty Hospital between 2017 and 2021. Three of these patients were excluded from the study because of missing data. Of the 203 patients included in the study, 164 (80.8%) were male and 39 (19.2%) were female. The mean age of the patients was 50.2±20.9 (min. 18, max. 97) years. Glasgow Coma Scale (GCS) score was 8 in 1 patient, 13 in 3, and 15 in the remaining patients. In terms of ASA scores, 82, 30, 80, and 11 patients were classified as ASA-I, ASA-II, ASA-III, and ASA-IV, respectively (Table 1).
Of the 119 (58.6%) patients who had comorbidities, 80 (39.4%) had endocrine diseases, 78 (38.4%) had cardiovascular diseases, 24 (11.8%) had respiratory system diseases, and 13 (6.4%) had chronic kidney failure. In addition, 2 patients were kidney transplant patients.
Furthermore, there were 39 (19.2%) smokers and 84 (41.4%) patients without a history of comorbidity. There were 129 (63.5) patients with 1 comorbidity, 39 (19.2%) with 2 comorbidities, 22 (10.8%) with 3 comorbidities, 11 (5.4%) with 4 comorbidities, and 2 (1%) with 5 comorbidities (Table 2).
Complications related to diabetes mellitus, which were observed in 74 (36.5%) patients, were the most common cause of amputation, followed by crush injuries, firearm-mine injuries, peripheral vascular diseases, occupational accidents, osteomyelitis-infectious causes, traffic accidents, malignancies, Buerger’s disease, and frostbites-burns, which were observed in 43 (21.2%), 24 (11.8%), 22 (10.8%), 15 (7.4%), 10 (4.9%), 9 (4.4%), 6 (2.9%), 4 (1.9%), and 2 (1.0%) patients, respectively. A total of 208 extremity amputations, 5 of which were bilateral, were performed in 203 patients included in the study. Among these amputations, 93 (44.8%) were major extremity amputations, including amputations of the knee, hip, elbow, and shoulder, and 115 (55.2%) were minor extremity amputations, including amputations of the finger, toe, and wrist. A total of 208 extremity amputations, 5 of which were bilateral, were performed in 203 patients. Of the amputations performed, 77 (37.0%) were upper-extremity, and 131 (63.0%) were lower-extremity. In upper-extremity amputations, regional anesthesia was used with 74.0% and general anesthesia with 26.0%. Peripheral nerve blocks were the most used regional anesthesia method in upper-extremity amputations. Regional anesthesia was used with 64.3% and general anesthesia with 35.7% of lower-extremity amputations. The most used regional anesthesia method in lower-extremity amputations was spinal anesthesia. Additionally, 107 (48.0%), 91 (40.8%), and 5 (2.2%) amputations were performed on the right extremity, left extremity, and bilaterally, respectively (Table 3).
Regional methods were the most commonly used anesthesia methods applied to the patients included in this study. Among all patients, regional anesthesia methods were used in 137 (67.5%) patients and general anesthesia in 66 (32.5%) patients. The most commonly applied regional anesthesia methods were peripheral nerve blocks and spinal anesthesia, which were applied to 32.5% and 31.5% of the patients, respectively.
Postoperatively, 174 (85.7%) patients received treatment in the postoperative ward and 28 (13.8%) in the intensive care unit. Of the 28 patients who needed intensive care, 20 (71.4%) were operated on under general anesthesia. Of the operated patients, 112 (55.2%) were operated on under elective conditions and 91 (44.8%) under emergency conditions. The hospital stay of the patients ranged from 1 to 90 days. The mean hospital stay was 8.7±7.4 days in patients who were operated on under regional anesthesia techniques and 15.0±20.6 days in patients who received general anesthesia (Table 4).
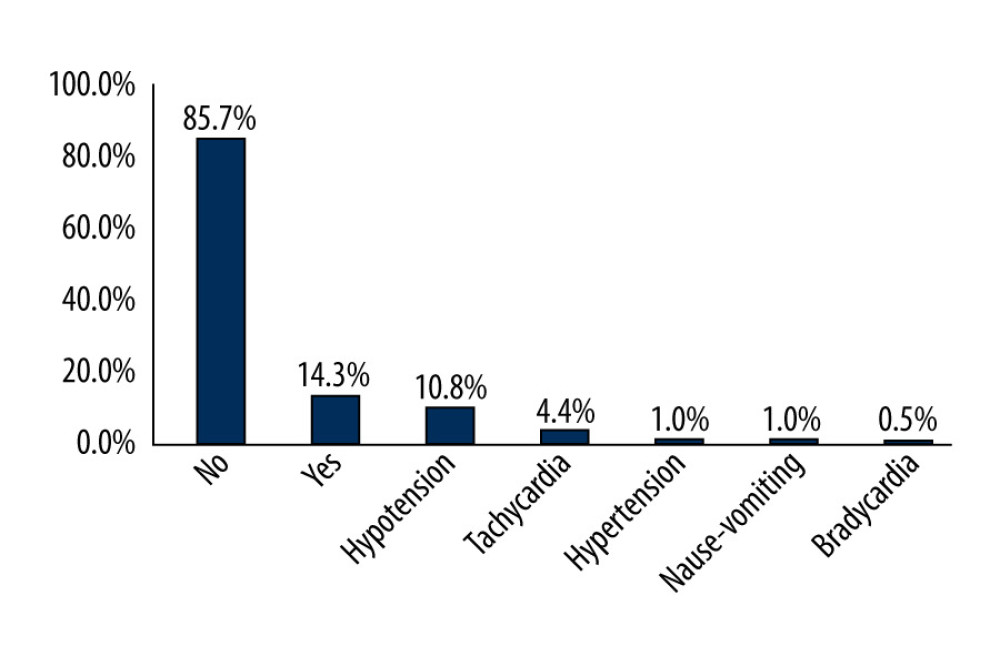
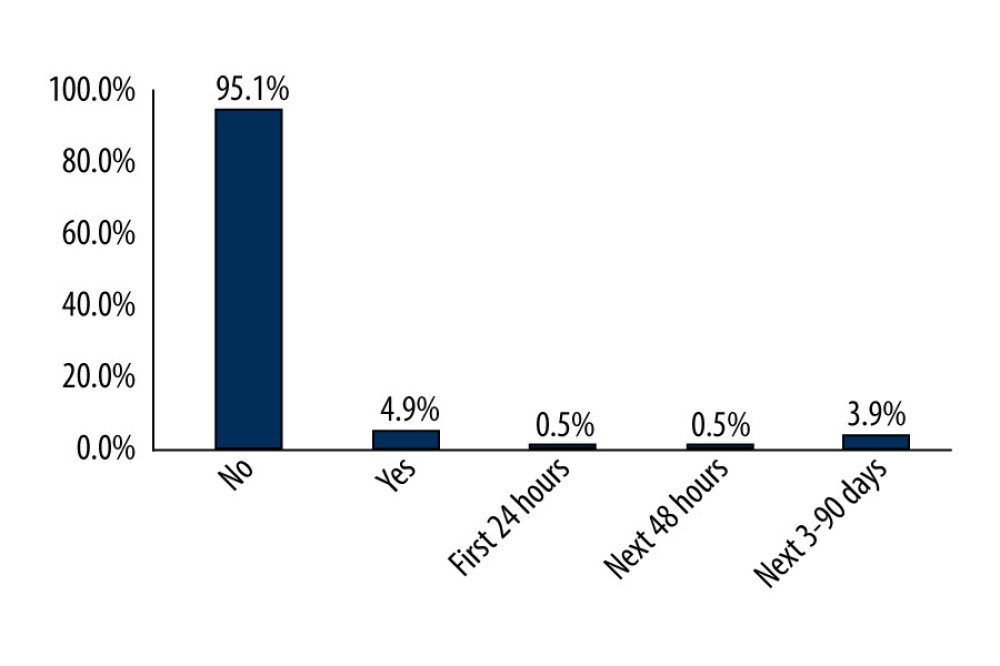
The most common complications were hypotension and tachycardia, which were observed in 10.8% and 4.4% of the patients, respectively (Figure 1). Among these patients, 77.3% who developed hypotension and 66.7% who developed tachycardia were operated on under general anesthesia. There was 1 (0.5%) death in the first 24 h, 1 (0.5%) in the next 48 h, and 10 (4.9%) in total. Of the 10 mortalities, 6 (60%) occurred in patients in whom general anesthesia was used as the method of anesthesia (Figure 2).
Discussion
There are many studies on extremity amputations in the literature. However, these studies were generally designed in a narrow framework directed at the indications, extent, or frequency of amputations or the anesthesia methods used in these amputations. In this context, the present study was designed to address many aspects of the subject, including patients’ demographic data, causes and levels of extremity amputations, comorbidities, postoperative mortality, length of hospital stay, and the advantages of the particular anesthesia techniques used.
In the current study, upper- and lower-extremity amputations were considered together. A total of 208 extremity amputations, 5 of which were bilateral, were performed in 203 patients. Of these 208 amputations, 77 (37.0%) were performed on the upper extremity and 131 (63.0%) on the lower extremity. Regional anesthesia techniques were used at a rate of 74.0% in upper-extremity amputations, 64.3% in lower-extremity amputations, and 67.5% in total amputations. Among all patients, when lower- and upper-extremity amputations were evaluated separately, regional anesthesia techniques were by far the most used methods in anesthesia management. Considering the postoperative processes of the patients, patients who were operated on under regional anesthesia techniques needed shorter intensive care unit stay and shorter hospital stays. In addition, mortality rates were lower in patients who were operated on under regional anesthesia compared to general anesthesia (40% vs 60%).
In a study [8] conducted with 34 patients, Ekere determined that the male-female ratio of the cohort was 2.1: 1 and that one-third of the patients were aged 20–40 years. In the study of Tükenmez et al, [9] conducted with 62 patients, the male-female ratio was 2.5: 1. Similarly, the male-female ratio was high in this study. Additionally, the mean age of the study group was 50.2±20.9 (min. 18, max. 97) years.
Extremity amputations are performed due to trauma, complications of DM, vascular pathologies, firearm injuries, tumors, infections, and frostbites-burns [10]. The most common causes of trauma-related extremity amputations are occupational accidents, traffic accidents, crush injuries, and firearm and mine injuries. Amputation is preferred rather than repair in injuries with severe damage to tissue and bone integrity [11]. As demonstrated in other studies, complications of DM are the leading cause of non-traumatic amputations. DM leads to a number of complications, including peripheral vascular diseases and peripheral neuropathies. These complications inevitably result in amputation [12].
In a study by Masood et al [13] with 53 patients, the leading causes of amputation were DM complications and trauma, which were observed in 54.7% and 45.3% of the patients, respectively. In another study conducted with 162 amputation patients by Chalya et al, [14] DM complications were observed in 41.9%, trauma in 38.4%, and vascular diseases in 8.6% of the patients. In the study by Kidmas et al [15] of 83 amputation cases, the most common causes of amputation were trauma (29.9%), DM complications (26.4%), and malignancies (23%). In comparison, the most common non-traumatic causes of amputations performed within the scope of the lower- and upper-extremity surgeries analyzed in this study were DM complications and peripheral vascular diseases, which were observed in 74 (36.5%) and 22 (10.8%) patients, respectively. Additionally, among the causes of amputation secondary to trauma were crush injuries, firearm-mine injuries, and occupational accidents, which were observed in 43 (21.2%), 24 (11.8%), and 15 (7.4%) patients, respectively. Hence, crush and firearm-mine injuries, in particular, were more common among the causes of amputations analyzed in this study compared to other studies available in the literature. The higher frequency of amputations in the event of crush and firearm-mine injuries might be attributed to the deterioration of tissue integrity in these injuries, which rendered reimplantation almost impossible. In addition, the fact that the province of Van, where the study was conducted, is located at a crossing point of illegal immigrants on the eastern border of Turkey might also have influced the study results.
In a study conducted by Bakis et al [16] with 372 patients, comorbidities were detected in 70% of the patients, including HT in 48.1%, DM in 12.6%, hyperlipidemia in 6.7%, and coronary artery disease (CAD) in 2.6%. In another study conducted by Aulivola et al [17] on 788 patients, 80.6% of the patients had DM, 68.5% had HT, and 60.9% had CAD. In comparison, comorbidities were detected in 58.6% of the patients included in this study, including endocrine diseases in 39.4%, cardiovascular diseases in 38.4%, respiratory system diseases in 11.8%, and chronic renal failure in 6.4%.
Regional anesthesia techniques have significant advantages over general anesthesia, such as early mobilization, postoperative analgesic effect, lower thromboembolism risk, less transfusion need, and the fact that the patient can stay awake during the surgery [18]. Among the regional anesthesia techniques, it is known that peripheral nerve blocks affect hemodynamic functions less than central nerve blocks and cause fewer complications. The success and use of peripheral nerve blocks have increased with the introduction of ultrasonography, particularly in elderly and high-risk patients [7,19]. A retrospective study by Cho et al [20] on the anesthesia techniques used in 7613 amputation cases reported that general anesthesia was used in 39.3% of the cases, neuraxial blocks in 37.3%, and peripheral nerve blocks in 23.3%. Similarly, in the study conducted by Chery et al [21] with 407 patients who underwent lower-extremity amputations, it was reported that general anesthesia was used in 259 (63.6%) patients and regional anesthesia techniques were used in 148 (36.4%) patients. Accordingly, regional anesthesia was used in 137 (67.5%), and general anesthesia in 66 (32.5%) patients. When extremity amputations were evaluated separately, regional anesthesia techniques were used in 64.3% of lower-extremity amputations and 74.0% of upper-extremity amputations. Peripheral nerve blocks, which were used in 32.5% of the patients, were the most used method among both the regional and all anesthesia methods.
Accordingly, the use of peripheral nerve blocks was more common among the amputations performed within the scope of the lower- and upper-extremity surgeries analyzed in this study compared to most of the studies available in the literature. Peripheral nerve blocks provide hemodynamic stability, reducing complications and mortality rates. Moreover, the need for postoperative intensive care was less in patients who underwent regional anesthesia. In addition, the mean length of stay in the hospital was also shorter in patients who were operated on with regional anesthesia techniques compared to those who were operated on with general anesthesia. Hence, it can be speculated that patients who were operated on with regional anesthesia techniques are more likely to return to everyday life in a shorter time, thereby preventing loss of labor and costs.
A detailed preoperative evaluation is needed to determine the extent of amputation in extremity amputations and to create the most appropriate functional stump for prosthesis applications. Clinical examination and Doppler ultrasonography are commonly used to determine the extent of amputation. In addition, imaging methods such as angiography and magnetic resonance imaging are also used, along with a detailed physical examination in cases when deemed necessary [9,22].
The extent of amputation in patients who were scheduled to have elective surgery was decided by cardiovascular surgeons in this study. Essoh et al [23] reported that 46.9%, 16.2%, 11.9%, and 11.2% of the 156 extremity amputation cases included in their study were amputated from below the knee, toes, above the knee, and below the elbow, respectively. In a large-scale study conducted with 7613 cases by Cho et al [20], it was reported that 62.9% of the cases were amputated from the fingers and toes, 18.2% from the upper arm, forearm, and lower leg, 12.1% from the hand and foot, and 6.5% from the thigh. In comparison, 30.2%, 25.0%, 25.4%, and 14.4% of the cases included in this study were amputated from the upper-extremity finger, below the knee, lower-extremity, and over the knee, respectively. Shoulder and hip amputations, which are considered major amputations, were performed in 3 cases each. The relevant studies available in the literature revealed different results in terms of the rates of amputated extremities and the causes of amputations. The discrepancies between these studies might be attributed to the differences between the geographical, socio-cultural, and economic characteristics of the populations on whom these studies were conducted.
Ekere [8] reported the mortality rate in 34 amputation cases as 16.7%. Similarly, Tükenmez et al [9] reported the mortality rate in 62 amputation cases as 15%. In contrast, the mortality rate in the patients included in this study was 4.9%. General anesthesia was used in 6 (60%) of 10 cases who were exitus, spinal anesthesia in 3 (30%), and peripheral nerve block in 1 (10%). General anesthesia was used in 71.4% of the 28 cases who needed postoperative care in the intensive care unit, whereas spinal anesthesia was used in 21.4%, and peripheral nerve blocks were used in only 7.1%. The fact that the mortality rate found in this study is lower than the mortality rates reported in relevant studies available in the literature might be attributed to the use of regional anesthesia techniques. In summary, regional anesthesia techniques reduced the need for intensive care along with mortality and morbidity rates.
There are some limitations of the presentstudy. This was a retrospective study. Accordingly, the data of the patients could only be obtained from the patient follow-up forms and the hospital information management system, which may have led to deficiencies in the data. The study’s retrospective design also prevented a detailed analysis of the types of complications that caused amputations. If a detailed analysis is to be made on this subject, prospective studies are needed.
Conclusions
Anesthesia management is of critical importance given the urgency of extremity amputation surgeries and associated comorbidities. The findings of this study demonstrated that performing extremity amputations under regional anesthesia techniques, especially peripheral nerve blocks, reduced mortality and morbidity rates, the need for postoperative intensive care, mean length of stay in the hospital, and hospital costs.
References
1. Fitzgibbons P, Medvedev G, Functional and clinical outcomes of upper extremity amputation: J Am Acad Orthop Surg, 2015; 23(12); 751-60
2. Molina CS, Faulk J, Lower extremity amputation. 2022: StatPearls [Internet] Jan, 2022, Treasure Island (FL), StatPearls Publishing
3. Tan WS, Arulselvan P, Ng SF, Improvement of diabetic wound healing by topical application of Vicenin-2 hydrocolloid film on Sprague Dawley rats: BMC Complement Altern Med, 2019; 19(1); 20
4. Aksoy M, Ince I, Ahiskalioğlu A, Alt ve üst ekstremite cerrahilerinde anestezi deneyimlerimiz: Son alti yilin retrospektif analizi: Journal of Anesthesia-JARSS, 2014; 22(2); 99-104 [in Turkish]
5. Lin JH, Jeon SY, Romano PS, Humphries MD, Rates and timing of subsequent amputation after initial minor amputation: J Vasc Surg, 2020; 72(1); 268-75
6. O’Donnell BD, Iohom G, Regional anesthesia techniques for ambulatory orthopedic surgery: Curr Opin Anaesthesiol, 2008; 21; 723-28
7. Memtsoudis SG, Sun X, Chiu YL, Perioperative comparative effectiveness of anesthetic technique in orthopedic patients: Anesthesiology, 2013; 118; 1046-58
8. Ekere AU, The scope of extremity amputations in a private hospital in the south-south region of Nigeria: Niger J Med, 2003; 12(4); 225-28
9. Tükenmez M, Çekin T, Karataş C, Diyabetik ayakta alt ekstremite amputasyonlari: Cumhuriyet Medical Journal, 2005; 3; 100-4 [in Turkish]
10. Azar FM, Beaty JH, Canale ST, Campbell’s operative orthopaedics: Amputations of the lower extremity, 2017; 1; 674-85, Philadelphia, Elsevier
11. Parker K, Kirby RL, Adderson J, Thompson K, Ambulation of people with lower-limb amputations: Relationship between capacity and performance measures: Arch Phys Med Rehabil, 2010; 91(4); 543-49
12. Al-Maskar F, El-Sadig M, Prevalence of risk factors for diabetic foot complications: BMC Fam Pract, 2007; 8; 59
13. Masood J, Irfan A, Ghulam M, Current indications for major lower limb amputations at Civil Hospital, Karachi: Pak J Surg, 2008; 24; 228-31
14. Chalya PL, Mabula JB, Dass RM, Major limb amputations: A tertiary hospital experience in northwestern Tanzania: J Orthop Surg Res, 2012; 7(1); 18
15. Kidmas AT, Nwadiaro CH, Igun GO, Lower limb amputation in Jos, Nigeria: East Afr Med J, 2004; 81(8); 427-29
16. Bakis M, Sari S, Cillimoglu AÖ, The effect of anesthesia type on the postoperative complications of major lower extremity surgery: Dicle Tip Dergisi, 2014; 41(1); 191-94
17. Aulivola B, Hile CN, Hamdan AD, Major lower extremity amputation: Outcome of a modern series: Arch Surg, 2004; 139(4); 395-99
18. Borck M, Wandrey JD, Höft M, Local infiltration analgesia versus peripheral nerve block anaesthesia in total knee arthroplasty: A pharmaco-economic comparison: BMC Anesthesiol, 2022; 22(1); 80
19. Offierski C, Peripheral nerve blocks for distal extremity surgery: Clin Plast Surg, 2013; 40; 551-55
20. Cho HS, Kim S, Kim CS, Effects of different anesthetic techniques on the incidence of phantom limb pain after limb amputation: A population-based retrospective cohort study: Korean J Pain, 2020; 33(3); 267-74
21. Chery J, Semaan E, Darji S, Impact of regional versus general anesthesia on the clinical outcomes of patients undergoing major lower extremity amputation: Ann Vasc Surg, 2014; 28(5); 1149-56
22. Pinzur MS, Stuck RM, Sage R, Hunt N, Rabinovich Z, Syme ankle disarticulation in-patients with diabetes: J Bone Joint Surg Am, 2003; 85-A(9); 1667-72
23. Essoh JB, Bamba I, Dje VB, Limb amputations in adults in an Ivorian Teaching Hospital: Niger J Ortho & Trauma, 2007; 6(2); 61-63
Tables
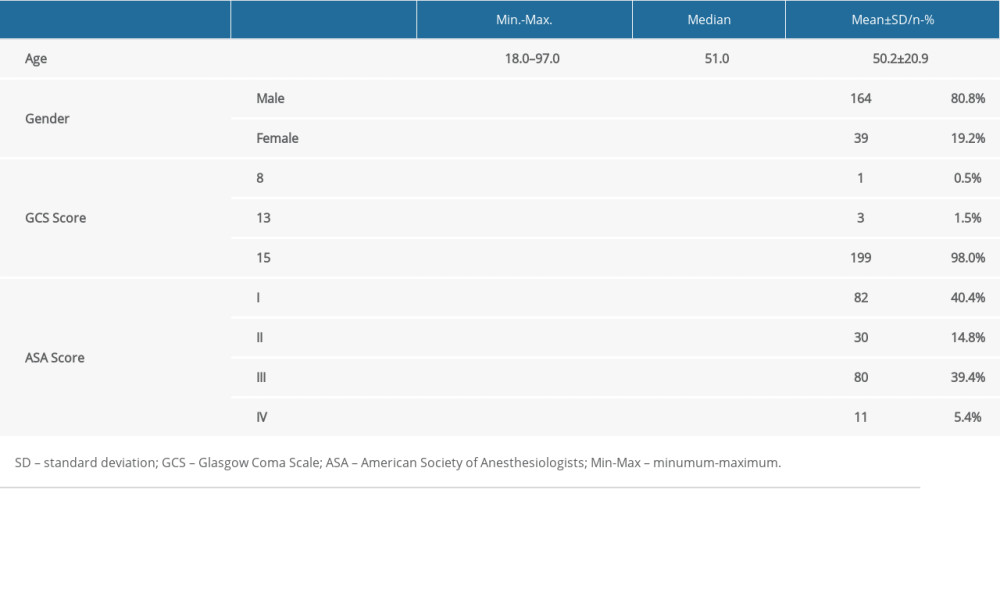 Table 1. Demographic characteristics of the patients.
Table 1. Demographic characteristics of the patients. Table 2. Distribution of patients by comorbidities.
Table 2. Distribution of patients by comorbidities.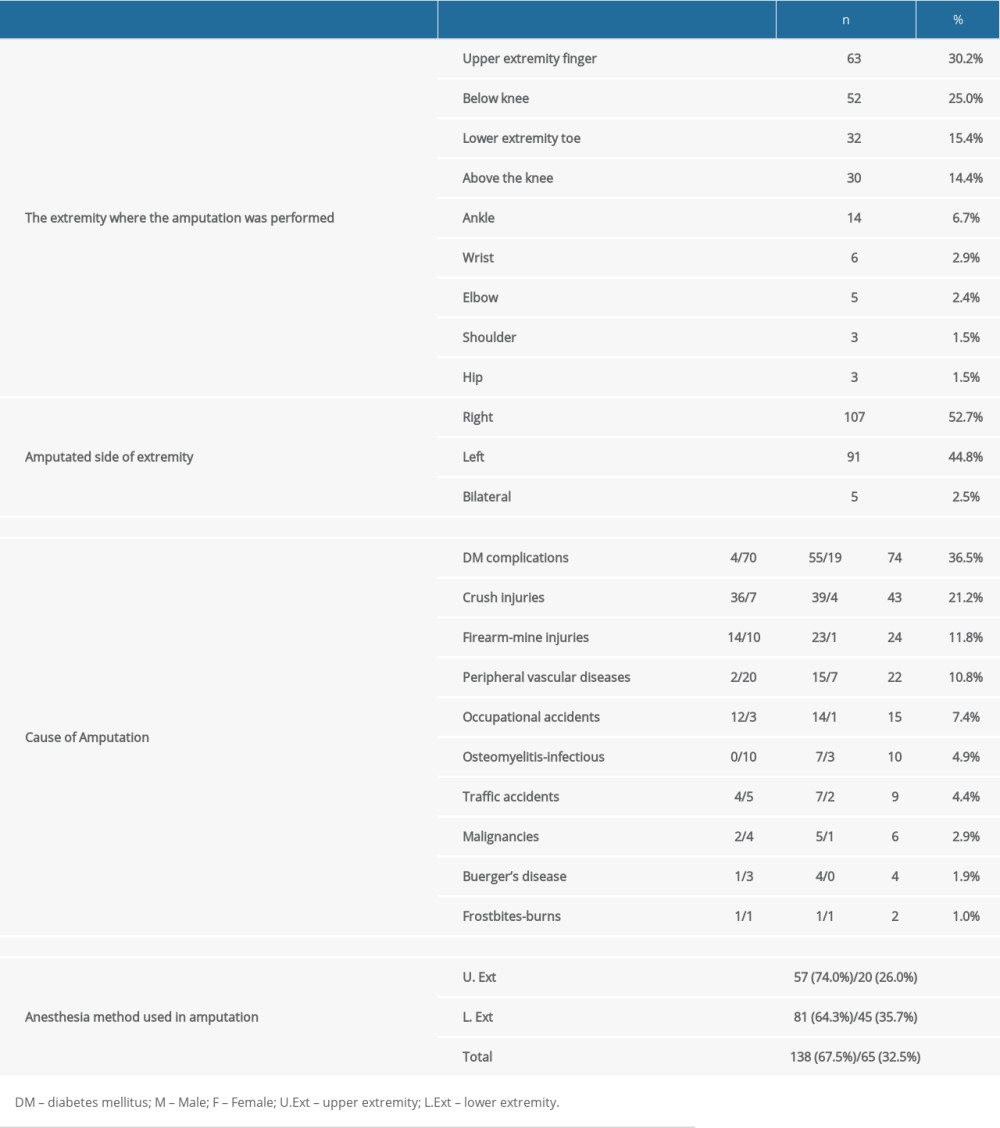 Table 3. The extremity where the amputation was performed and causes of the amputation.
Table 3. The extremity where the amputation was performed and causes of the amputation. Table 4. Anesthesia methods applied to patients and surgery data.Table 1. Demographic characteristics of the patients.Table 2. Distribution of patients by comorbidities.Table 3. The extremity where the amputation was performed and causes of the amputation.Table 4. Anesthesia methods applied to patients and surgery data.
Table 4. Anesthesia methods applied to patients and surgery data.Table 1. Demographic characteristics of the patients.Table 2. Distribution of patients by comorbidities.Table 3. The extremity where the amputation was performed and causes of the amputation.Table 4. Anesthesia methods applied to patients and surgery data. In Press
Meta-Analysis
Effectiveness of Cardiac Telerehabilitation in Improving Functional Capacity, Quality Of Life and Cardiovas...Med Sci Monit In Press; DOI: 10.12659/MSM.953366
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,468
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,759,966
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,248
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,898
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387