01 March 2023: Clinical Research
Bakri Balloon for Treatment of Postpartum Hemorrhage: A Real-World 2016–2020 Study in 279 Women from a Single Center
Chanyun Xiao1BCEF, Ying Wang1BCEF, Na Zhang1ADEG*, Guo-qiang Sun1ADFDOI: 10.12659/MSM.938823
Med Sci Monit 2023; 29:e938823






Abstract
BACKGROUND: Postpartum hemorrhage (PPH) may be primary or secondary and is defined as the loss of 500 ml or more of blood within the first 24 h after birth. The Bakri balloon tamponade (BBT) is an intrauterine device used as an adjunctive treatment for refractory PPH. The aim of this study was to present the real-world experience from a single center on the effectiveness of the BBT for the treatment of PPH.
MATERIAL AND METHODS: This cohort study of 279 women was conducted in a real-world setting. Patients’ characteristics and clinical outcomes between the BBT Success group and BBT Failure group were analyzed by t test or chi-square test. The primary outcome was the success rate of BBT. The secondary outcomes were the perinatal outcomes.
RESULTS: The success rate of BBT was 88.89% (248/279). A blood transfusion rate of 65.95% (184/279) was observed. After using the BBT, significant differences were observed in intervention (P<0.001), blood loss (P<0.001), indwelling time of BBT (P<0.001), and blood transfusion (P<0.001) between the Success group and Failure group. The Success group showed greater range of descent in blood loss (991.56.15±13.65 mL in Success group vs 816.23±7.57 mL in Failure group). Of the 31 women with BBT failure, 87.10% (27/31) received uterine artery embolization (UAE), 96.77% (30/31) received blood transfusion, and none required a hysterectomy.
CONCLUSIONS: The findings from this study from a single center in China supported those from previous studies showing that the BBT was an effective treatment to control PPH.
Keywords: Postpartum Hemorrhage, Uterine Balloon Tamponade, Postpartum Period, Pregnancy, Humans, Female, Cohort Studies, Aircraft, Balloon Occlusion, China
Background
Postpartum hemorrhage (PPH) is still a leading cause of maternal morbidity and mortality [1], accounting for over 2.5% of maternal deaths worldwide [2]. Various risk factors were reported for PPH, such as cesarean delivery [3] and placenta accreta [4]. Uterine atony, soft-tissues injury associated with the birth canal, and placental factors such as placenta previa are considered as the most common reasons for PPH [5]. A higher prevalence of PPH is reported in undeveloped or low-income countries than in developed or high-income countries [6]. A peripartum hysterectomy may be inevitable in case of severe PPH and showed great harm to the parturient, including loss of fertility, and high morbidity was proved to be closely associated with peripartum hysterectomies [7]. Therefore, it is still essential to explore a safer and more effective method to reduce the application of hysterectomies.
To date, various conservative procedures have been developed to control PPH. The Bakri balloon tamponade (BBT) has been recommended by the American College of Obstetricians and Gynecologists (ACOG) and WHO as a second-line conservative treatment for PPH [8]. The criteria for use of uterine tamponade were: during cesarean section and after intraoperative uterine massage and use of an uterotonic such as oxytocin and carboprost tromethamine, the presence of persistent active uterine bleeding or an amount of bleeding that reached a volume of 500 mL, and the initial treatment of PPH is usually uterotonic drugs such as oxytocin and prostaglandin. Compared with other conserving interventions, such as arterial ligation, uterine artery embolization (UAE), B-lynch compression sutures, and uterine packing, BBT requires minimal local resources and does not entail extensive training or complex equipment; it showed high effectiveness and kept the mother’s ability to bear additional children [9]. The balloon (a maximum volume of 500 mL) was inserted either transvaginally after vaginal delivery or transvaginally/transabdominally after cesarean delivery, and it was removed from the uterine cavity within 24 h. We sutured the uterine incision and carefully avoided puncturing the balloon. Ultrasonography was used to monitor its intrauterine position. A fluid collection bag connected to the BBT was used to monitor bleeding from the uterine cavity. The posterior fornix of the vagina can be packed with gauze to prevent the balloon from falling off. Although the efficacy and effectiveness of BBT has been intensively studied, conflicting evidence has also been reported [10]. Said Ali et al reviewed 28 articles and reported that BBT may be a less effective tool for management of PPH after vaginal or cesarean delivery [8]. The BBT proved an effective adjunct in management of refractory PPH, and postpartum bleeding was controlled without further surgical intervention in 95% of women, even those with uterine atony [11]. Moreover, knowledge about use of the BBT in the Chinese population with postpartum bleeding is limited and there is a lack of information on its effectiveness in real-world settings.
Therefore, the aim of this study was to present the real-world experience from a single center on the effectiveness of the BBT for the treatment of PPH in 279 women.
Material and Methods
ETHICS APPROVAL:
All procedures performed in the study were approved by the Ethics Committee of Maternal and Child Health hospital of Hubei Province (IEM XM073) and conformed to the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Written or orally informed consents were obtained from all patients to participate in the study.
STUDY SUBJECTS:
A real-world database containing electronic health record data was established. A total of 279 eligible puerpera with postpartum bleeding who failed to respond to the first-line conservative management (the routine protocol for PPH) and received BBT (Cook Medical, Spencer, IN, USA) in the cohort study were recruited from January 2016 to December 2020. All eligible women were enrolled in the study if they met the following criteria. Inclusion criteria were: 1) age ≥18 years old; 2) a gestation age of ≥28 weeks; 3) received the BBT; 4) failed first-line conservative management. Exclusion criteria were: 1) those with uterine fibroids; 2) those with malignant tumors; 3) pelvic infections; 4) those with communication disorders; 5) those with abortion; 6) data obvious exceptions in the records.
CLINICAL DATA COLLECTION:
The maternal clinical characteristics of all pregnant women recruited were collected, including weight, gestational age, maternal age, parity, delivery mode (vaginal delivery and cesarean delivery), birth number, repeat cesarean section, gestational diabetes, gestational hypertension, uterine atony, placenta accrete, abnormal coagulation, placenta previa, preeclampsia. postpartum bleeding management and perinatal outcomes, such as balloon placement method, uterine contractions, suture method before using the BBT, lower genital tract trauma, intervention after using the BBT, infused volume, indwelling time, blood loss and transfusion, and perinatal complications. All data in the records were anonymized and de-identified before analysis.
CLINICAL OUTCOME MEASURES:
The primary outcome was the success rate of BBT. If the postpartum bleeding was stopped utilizing only the BBT and no further surgical interventions were involved, “BBT success” was achieved. If the BBT failed to control the bleeding, a UAE, internal iliac artery embolization (IIAE), or hysterectomy was immediately performed.
The secondary outcomes were the perinatal outcomes between the BBT Success group and BBT Failure group, the effect of delivery methods, interventional embolization on postpartum bleeding after using the BBT on perinatal outcomes, such as blood loss, and transfusion.
STATISTICAL ANALYSIS:
All analyses were performed using SPSS version 23.0 (IBM Corp, Armonk, NY). Categorical data were combined to obtain frequencies and percentages, while continuous data are presented as means±standard deviation (SD). Continuous data between 2 groups were analyzed for statistically significant differences using the
Results
BASELINE CHARACTERISTICS AND PRIMARY OUTCOME ANALYSIS:
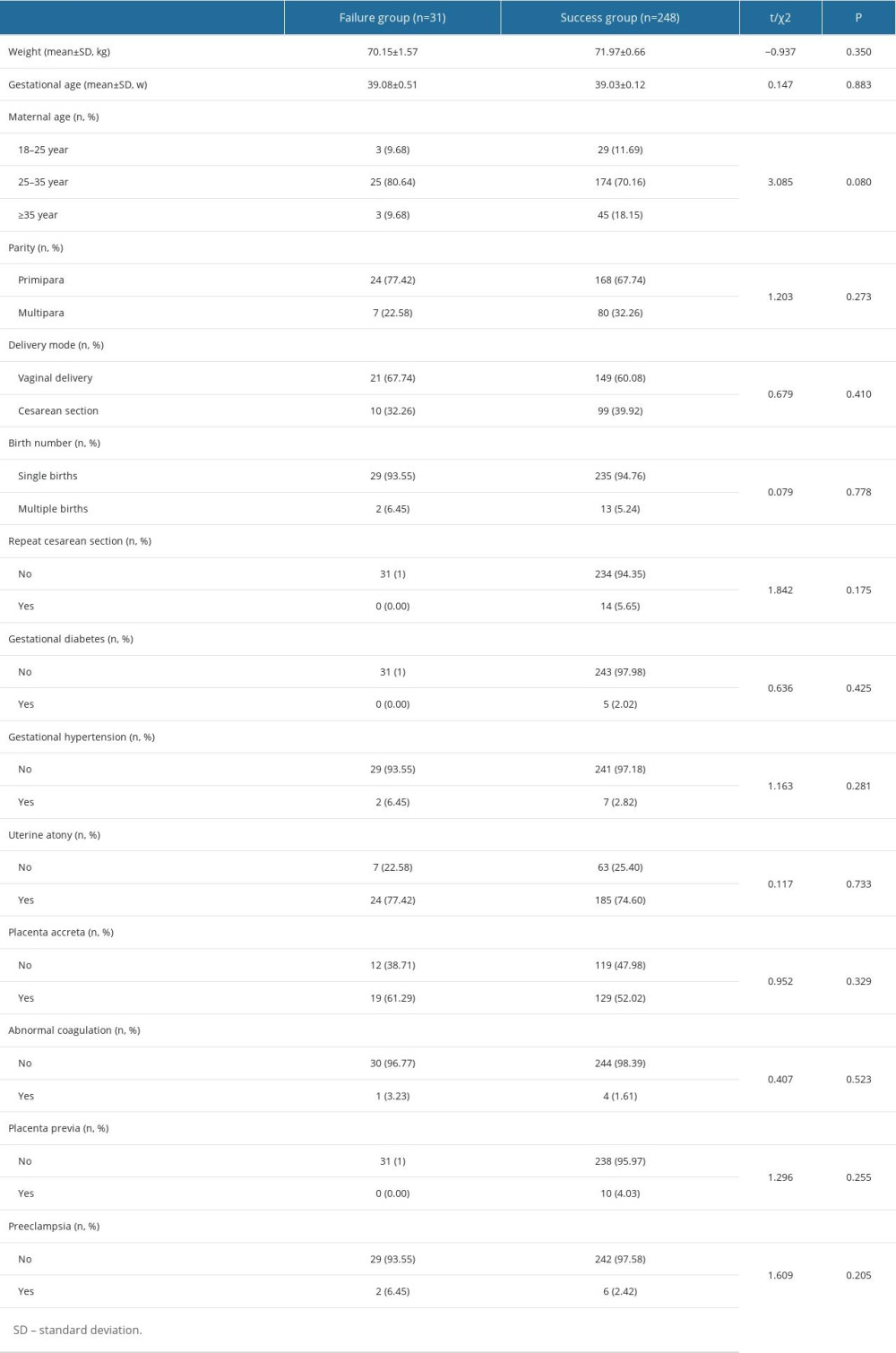
A total of 279 pregnant women using BBT were finally recruited in the study. Analysis of primary outcome revealed that the success rate of BBT was 88.89% (248/279, Table 1). Further analysis of baseline characteristics between the Failure group and Success group demonstrated no significant differences in parameters such as, weight, gestational age, maternal age, parity, delivery mode, and past medical history (all P>0.05).
COMPARISON OF PERINATAL OUTCOMES BETWEEN FAILURE GROUP AND SUCCESS GROUP:
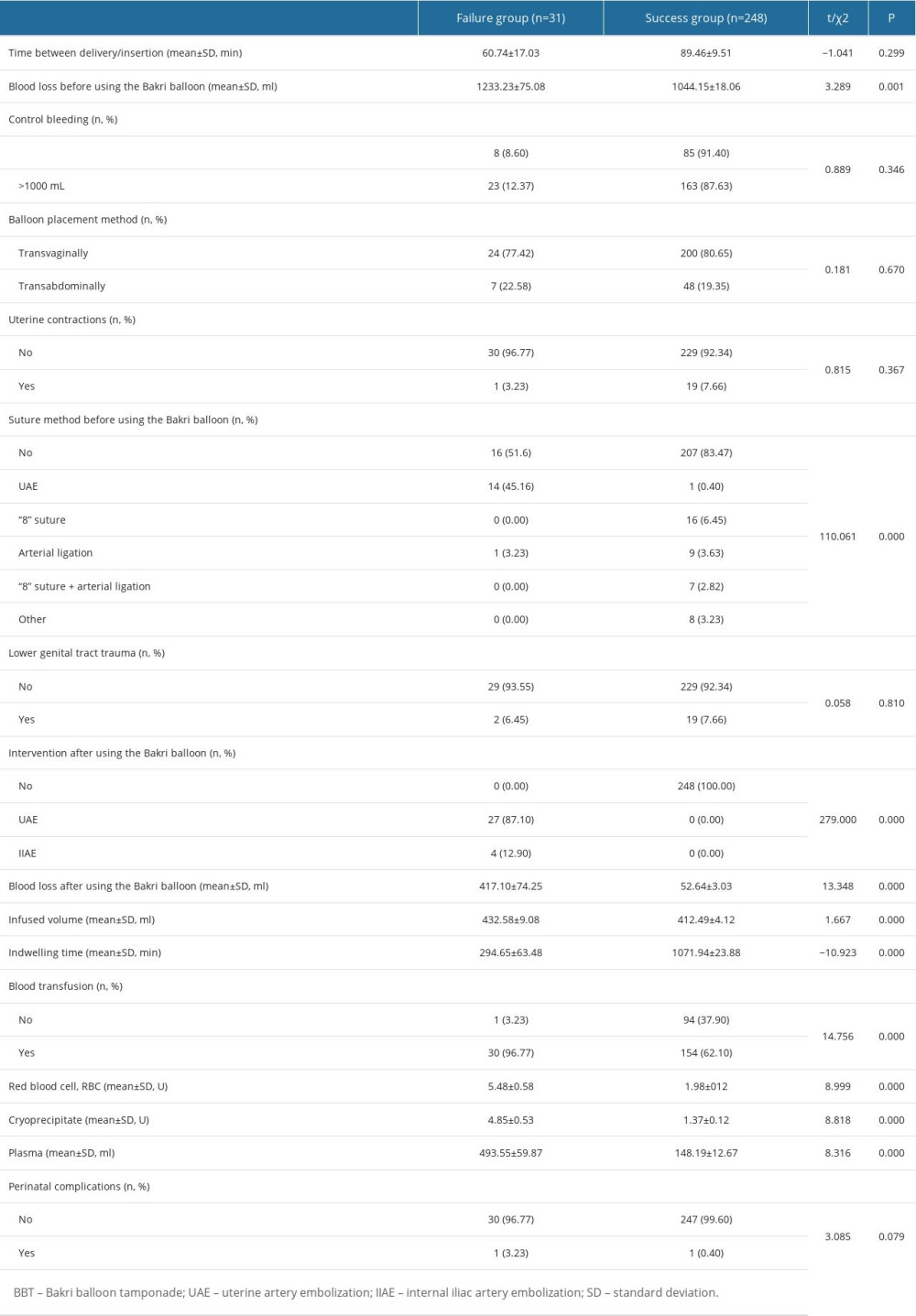
The perinatal outcomes between the Failure group and Success group were compared (Table 2). The time between delivery and BBT insertion was 60.74±17.03 min in the Failure group and 89.46±9.51 min in the Success group. No significant differences were observed in time between delivery/insertion (P=0.300), different balloon placement method (P=0.670), using uterine contractions (P=0.367), or lower genital tract trauma (P=0.810). Between women with blood loss >1000 mL (n=186) and <1000 mL (n=93), BBT showed a similar effectiveness in control of bleeding (P=0.346). A total of 184 (65.95%) women received blood transfusion and no women required a hysterectomy. In the Failure group, the overwhelming majority (30/31; 96.77%) required blood transfusion, and there were 27 women who received UAE accounting for 87.10% (27/31) and 4 women received IIAE, accounting for 12.90% (4/31).
Significant differences were observed in blood loss before using the BBT, different suture method before using the BBT, intervention after using the BBT, blood loss after using the BBT, and indwelling time of BBT, blood transfusion (red blood cell, cryoprecipitate, plasma) between the Failure group and Success group (all
COMPARISON OF PERINATAL COMPLICATIONS BETWEEN FAILURE GROUP AND SUCCESS GROUP:
Analysis of perinatal complications showed postoperative fever in 1 patient in each group (Table 2). The difference showed no significance (P=0.079).
Discussion
LIMITATIONS:
There are several limits in our study. The subjects are all from our single center, and the sample size was relatively small for a cohort study. BBT has been authorized for use in PPH management in China since 2012, and was introduced in our hospital in 2016. However, we believe that our study shows the real-world use status of BBT in women with postpartum bleeding in China. Further research is needed to assess correlations of the efficacy with independent predictors for BBT failure and different delivery modes.
Conclusions
The findings from this study from a single center in China supported those from previous studies, which showed that the BBT was an effective treatment to control PPH. The current research expands the knowledge about women with postpartum bleeding to better guide the clinical use of BBT in real-world settings.
References
1. GBD 2017 Causes of Death Collaborators, Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017: Lancet, 2018; 392(10159); 1736-88
2. AbouZahr C, Global burden of maternal death and disability: Br Med Bull, 2003; 67; 1-11
3. Collins SL, Alemdar B, van Beekhuizen HJ, Evidence-based guidelines for the management of abnormally invasive placenta: Recommendations from the International Society for Abnormally Invasive Placenta: Am J Obstet Gynecol, 2019; 220(6); 511-26
4. Zuckerwise LC, Craig AM, Newton JM, Outcomes following a clinical algorithm allowing for delayed hysterectomy in the management of severe placenta accreta spectrum: Am J Obstet Gynecol, 2020; 222(2); 179e1-e9
5. Evensen A, Anderson JM, Fontaine P, Postpartum hemorrhage: Prevention and treatment: Am Fam Physician, 2017; 95(7); 442-49
6. Mehrabadi A, Hutcheon JA, Lee L, Trends in postpartum hemorrhage from 2000 to 2009: A population-based study: BMC Pregnancy Childbirth, 2012; 12; 108
7. Huque S, Roberts I, Fawole B, Risk factors for peripartum hysterectomy among women with postpartum haemorrhage: Analysis of data from the WOMAN trial: BMC Pregnancy Childbirth, 2018; 18(1); 186
8. Said Ali A, Faraag E, Mohammed M, The safety and effectiveness of Bakri balloon in the management of postpartum hemorrhage: A systematic review: J Matern Fetal Neonatal Med, 2021; 34(2); 300-7
9. Doumouchtsis SK, Papageorghiou AT, Arulkumaran S, Systematic review of conservative management of postpartum hemorrhage: What to do when medical treatment fails: Obstet Gynecol Surv, 2007; 62(8); 540-47
10. Suarez S, Conde-Agudelo A, Borovac-Pinheiro A, Uterine balloon tamponade for the treatment of postpartum hemorrhage: A systematic review and meta-analysis: Am J Obstet Gynecol, 2020; 222(4); 293.e1-e52
11. Brown H, Okeyo S, Mabeya H, The Bakri tamponade balloon as an adjunct treatment for refractory postpartum hemorrhage: Int J Gynaecol Obstet, 2016; 135(3); 276-80
12. Olsen R, Reisner DP, Benedetti TJ, Dunsmoor-Su RF, Bakri balloon effectiveness for postpartum hemorrhage: A “real world experience”: J Maternal Fetal Neonatal Med, 2013; 26(17); 1720-23
13. Dumont A, Bodin C, Hounkpatin B, Uterine balloon tamponade as an adjunct to misoprostol for the treatment of uncontrolled postpartum haemorrhage: A randomised controlled trial in Benin and Mali: BMJ open, 2017; 7(9); e016590
14. Kong CW, To WWK, Intraluminal pressure of uterine balloon tamponade in the management of severe post-partum hemorrhage: J Obstet Gynaecol Res, 2018; 44(5); 914-21
15. Revert M, Rozenberg P, Cottenet J, Quantin C, Intrauterine balloon tamponade for severe postpartum hemorrhage: Obstet Gynecol, 2018; 131(1); 143-49
16. Gauchotte E, De La Torre M, Perdriolle-Galet E, Impact of uterine balloon tamponade on the use of invasive procedures in severe postpartum hemorrhage: Acta Obstet Gynecol Scand, 2017; 96(7); 877-82
17. Laas E, Bui C, Popowski T, Mbaku OM, Rozenberg P, Trends in the rate of invasive procedures after the addition of the intrauterine tamponade test to a protocol for management of severe postpartum hemorrhage: Am J Obstet Gynecol, 2012; 207(4); 281.e1-e7
18. Liu C, Gao J, Liu J, Predictors of failed intrauterine balloon tamponade in the management of severe postpartum hemorrhage: Front Med (Lausanne), 2021; 8; 656422
19. Bakri YN, Amri A, Abdul Jabbar F, Tamponade-balloon for obstetrical bleeding: Int J Gynaecol Obstet, 2001; 74(2); 139-42
20. Bakri YN, Uterine tamponade-drain for hemorrhage secondary to placenta previa-accreta: Int J Gynaecol Obstet, 1992; 37(4); 302-3
21. Vitthala S, Tsoumpou I, Anjum ZK, Aziz NA, Use of Bakri balloon in post-partum haemorrhage: A series of 15 cases: Aust N Z J Obstet Gynaecol, 2009; 49(2); 191-94
22. Pala Ş, Atilgan R, Başpınar M, Comparison of results of Bakri balloon tamponade and caesarean hysterectomy in management of placenta accreta and increta: A retrospective study: J Obstet Gynaecol, 2018; 38(2); 194-99
23. Guo Y, Hua R, Bian S, Intrauterine Bakri balloon and vaginal tamponade combined with abdominal compression for the management of postpartum hemorrhage: J Obstet Gynaecol Can, 2018; 40(5); 561-65
24. Kong MC, To WW, Balloon tamponade for postpartum haemorrhage: Case series and literature review: Hong Kong Med J, 2013; 19(6); 484-90
25. Wang D, Xu S, Qiu X, Early usage of Bakri postpartum balloon in the management of postpartum hemorrhage: A large prospective, observational multicenter clinical study in South China: J Perinat Med, 2018; 46(6); 649-56
26. Jing L, Wei G, Mengfan S, Yanyan H, Effect of site of placentation on pregnancy outcomes in patients with placenta previa: PLoS One, 2018; 13(7); e0200252
27. Baba Y, Matsubara S, Ohkuchi A, Anterior placentation as a risk factor for massive hemorrhage during cesarean section in patients with placenta previa: J Obstet Gynaecol Res, 2014; 40(5); 1243-48
28. Wright CE, Chauhan SP, Abuhamad AZ, Bakri balloon in the management of postpartum hemorrhage: A review: Am J Perinatol, 2014; 31(11); 957-64
29. Soltan MH, Mohamed A, Ibrahim E, El-menia air inflated balloon in controlling atonic post partum hemorrhage: Int J Health Sci (Qassim), 2007; 1(1); 53-59
In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387