27 February 2023: Clinical Research
Comparison of Lumbar Fusion Surgical Outcomes Between Patients with Lumbar Spinal Stenosis ≥80 Versus 65–79 Years Old
Kuan Li1BCDE, Xiao HanDOI: 10.12659/MSM.938837
Med Sci Monit 2023; 29:e938837






Abstract
BACKGROUND: The efficacy of lumbar fusion surgery in patients age 80 years and older with lumbar spinal stenosis (LSS) is still controversial. This retrospective study aimed to evaluate the surgical outcomes of LSS patients ³80 vs 65-79 years.
MATERIAL AND METHODS: The study included 66 patients diagnosed with LSS from 2014 to 2020; 33 patients were ³80 years and 33 patients were 65-79 years. The 2 groups were matched for sex and surgical segment. All patients underwent posterior lumbar decompression, fixation, and fusion surgery. The Numerical Rating Scale (NRS) of leg and back pain, Oswestry Disability Index (ODI), Short-Form Health Survey (SF-36), and radiographic data were collected before surgery and at 3, 6, and 12 months postoperatively.
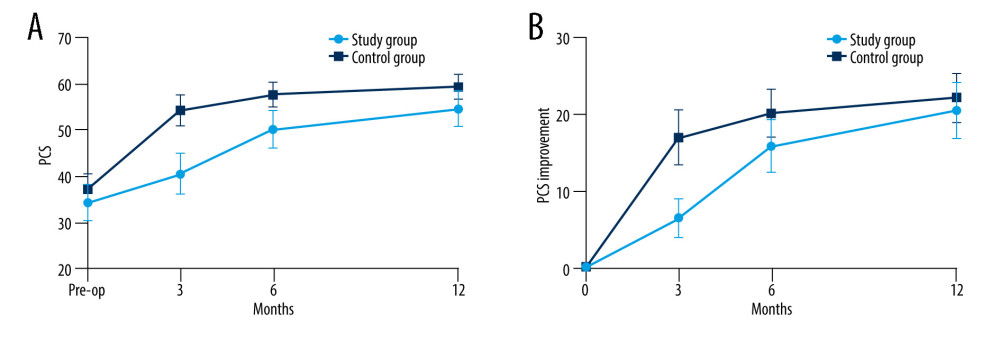
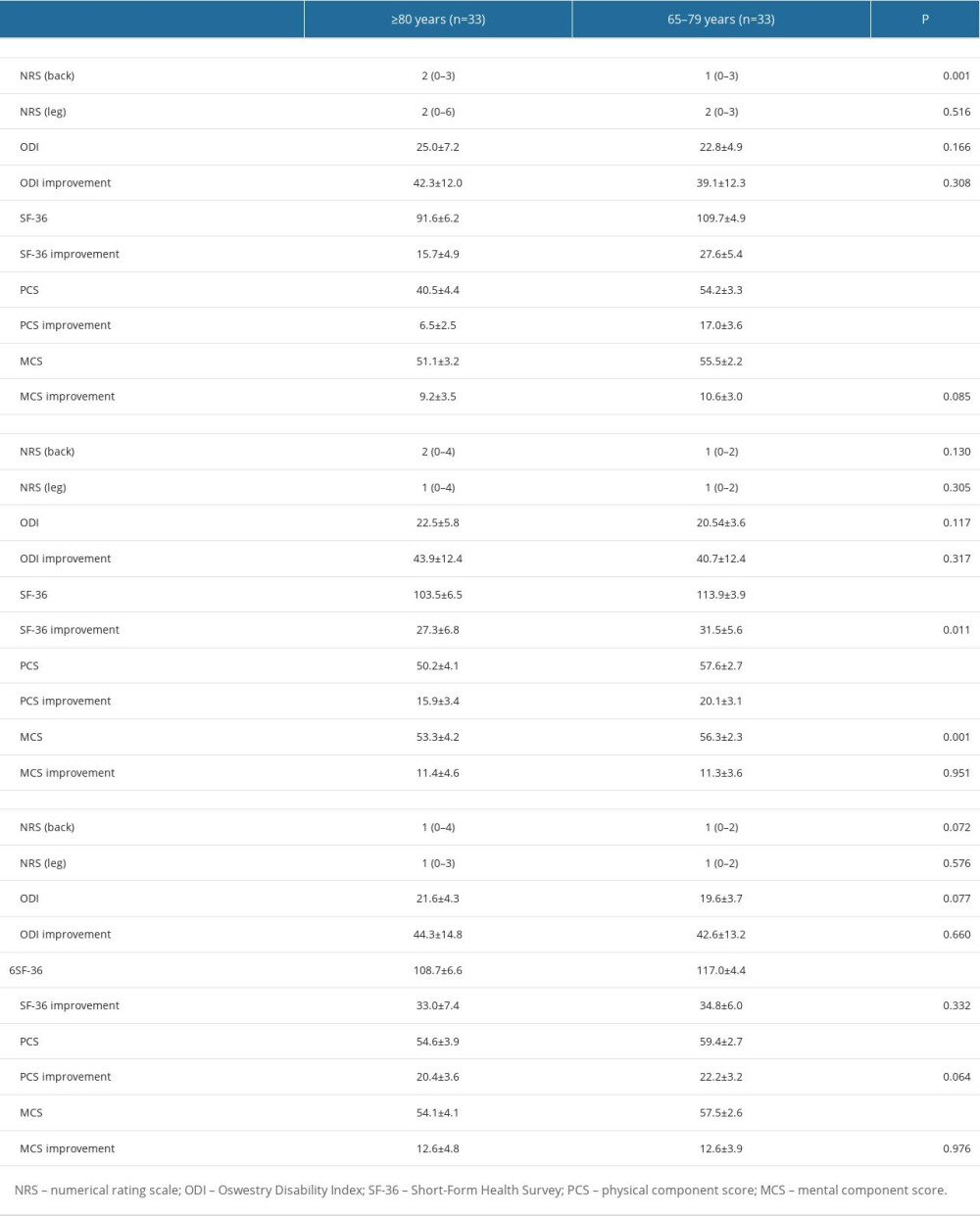
RESULTS: NRS (back) in the ≥80 years group was significantly higher than in the 65-79 years group at 3 months [2 (0-3) vs 1 (0-3), P=0.001]. Improvement of SF-36 (3 months: 15.7±4.9 vs 27.6±5.4, P<0.001; 6 months: 27.3±6.8 vs 31.5±5.6, P=0.011) and Physical Component Score (PCS) (3 months: 6.5±2.5 vs 17.0±3.6, P<0.001; 6 months: 15.9±3.4 vs 20.1±3.1, P<0.001) at 3 and 6 months in the ≥80 years group were significantly smaller than in 65-79 years group. There was a difference of Pfirrmann index of adjacent segment disc between the 2 groups at 12 months [≥80 vs 65-79 years group: 5.5 (4-8) vs 5 (3-8), P=0.003].
CONCLUSIONS: Lumbar fusion surgery in patients ≥80 years with LSS can provide comparable improvements in clinical and radiographic outcomes compared with younger patients. Postoperative physiological function recovery was slower in patients ≥80 years.
Keywords: Spinal Stenosis, Treatment Outcome, Lumbar Vertebrae, Quality of Life, Humans, Aged, 80 and over, Aged, Decompression, Surgical, Spinal Fusion
Background
With the development of society and medical care, the average life expectancy of human beings keeps increasing. By 2050, the population of people aged 80 and over will increase to 379 million around the world [1], with 150 million in China [2]. This will lead to increased incidence and prevalence of age-related diseases, such as lumbar spinal stenosis (LSS).
LSS is a clinical syndrome of neurogenic claudication and radicular pain due to a narrowing of the spinal canal or nerve root impingement [3]. Pain associated with LSS usually presents as radiating buttock or lower-extremity pain, burning or discomfort, often accompanied by low back pain, and impairment of walking, sensory loss, paresthesias, or muscle weakness, seriously affecting the quality of life of patients [3]. The World Health Organization defines elderly people in developing countries as being over 65 years [4], and LSS is the most common indication for spine surgery in people over 65 years of age [5]. Posterior lumbar decompression, fixation, and fusion surgery is still among the most effective methods for treating LSS [6], and the use of this procedure is increasing continuously [7]. Compared with non-surgical treatment, surgery with or without fusion can improve disability over 2 years in adults with symptomatic LSS [3,6]. As the life expectancy of the population increases, more and more elderly patients with LSS will require surgical treatment to improve their quality of life. In the past 10 years, the “safe age” of lumbar spine surgery reported in the literature gradually increased from 65 to 75 years old [8,9]. Nevertheless, the elderly, especially those age 80 years and older, tend to have multiple comorbidities and a high prevalence of osteoporosis, which can have adverse effects on lumbar fusion surgery, including increased complications, poor functional outcomes, and increased mortality [10,11]. The conclusions on the safety and efficacy of lumbar fusion surgery in patients over 80 are still controversial, and the available data are not comprehensive [12]. Therefore, this study aimed to evaluate the lumbar fusion surgical outcomes of patients with LSS ≥80 years vs those 65–79 years.
Material and Methods
STUDY DESIGN AND POPULATION:
This retrospective observational study included patients with a primary diagnosis of LSS who underwent surgery at the Orthopedics Department of our hospital between May 2014 and September 2020. The study was approved by the Ethics Committee of our hospital. The requirement for individual consent was waived by the committee because of the retrospective nature of the study.
The inclusion criteria were: 1) underwent lumbar decompression, fixation, and fusion surgery due to LSS as a primary diagnosis, 2) followed up at 3, 6, and 12 months postoperatively, and 3) age ≥65 years. The exclusion criteria were: 1) lumbar disc herniation, 2) rheumatoid arthritis, 3) fresh vertebral fracture or other acute injuries, 4) degenerative scoliosis of >10° and >3 mm spondylolisthesis or over 15° instability on dynamic lateral radiograph between adjacent lumbar vertebrae [13], or 5) history of lumbar surgery.
The patients were grouped as ≥80 and 65–79 years. The 2 groups were matched for sex and surgical segment. If a patient in the study group had multiple matches, computer software was used to randomly select a patient for the control group.
SURGICAL PROCEDURE AND POSTOPERATIVE REHABILITATION:
In this study, all patients underwent conventional open surgeries. All operations were performed by the same experienced senior chief physician. The surgery was performed in the prone position. The paraspinal muscles were dissected, and the spinous processes, bilateral articular processes, and roots of the transverse processes were exposed. Titanium polyaxial pedicle screws (Legacy, Medtronic, USA) were inserted into the bilateral pedicles. Two titanium rods were properly bent and placed between the nuts to obtain a suitable sagittal curve, and the nuts were tightened to lock the rods. Next, laminectomy and spinal canal decompression were performed. Finally, bilateral modified facet joint fusion was performed, which was an innovative technique of the authors’ team [14,15]. Briefly, a high-speed grinding drill was used to grind the articular surface of bilateral facet joints to create the bone graft bed. This bed was implanted with allogeneic cancellous bone granules and autologous cancellous bone.
The drainage tube was removed when the wound drainage volume was less than 100 mL/day. Then, the physician guided the patient to stand and walk under the protection of personalized lumbar support. All patients were recommended to increase their walking exercise 1 month after surgery. The lumbar support was removed 3 months postoperatively, and standard procedures such as lumbar floating, crouching, bending, and jogging were performed under guidance to strengthen the lumbar back muscles.
DATA COLLECTION:
The demographic and clinical data of patients, including age, sex, body mass index (BMI), surgical segment, operation time, blood loss volume, drainage tube placement time, length of hospital stay, the total cost of hospitalization, and complications, were collected from the medical records. The weighted Charlson Comorbidity Index (CCI) [16] and the American Society of Anesthesiologists’ physical status classification (ASA) [17] were used to assess the preoperative physical condition of these patients.
The Numerical Rating Scale (NRS) for back and leg pain [18], the validated simplified Chinese version of Oswestry Disability Index (ODI) [19], and the validated simplified Chinese version of Short-Form Health Survey (SF-36) [20] were collected before surgery and at 3, 6, and 12 months after surgery. SF-36 was divided into 2 parts for statistical analysis: Physical Component Summary (PCS) and Mental Component Summary (MCS). The improvement value was used as the indexes of clinical outcomes and defined as the change between the score at follow-up and the preoperative score.
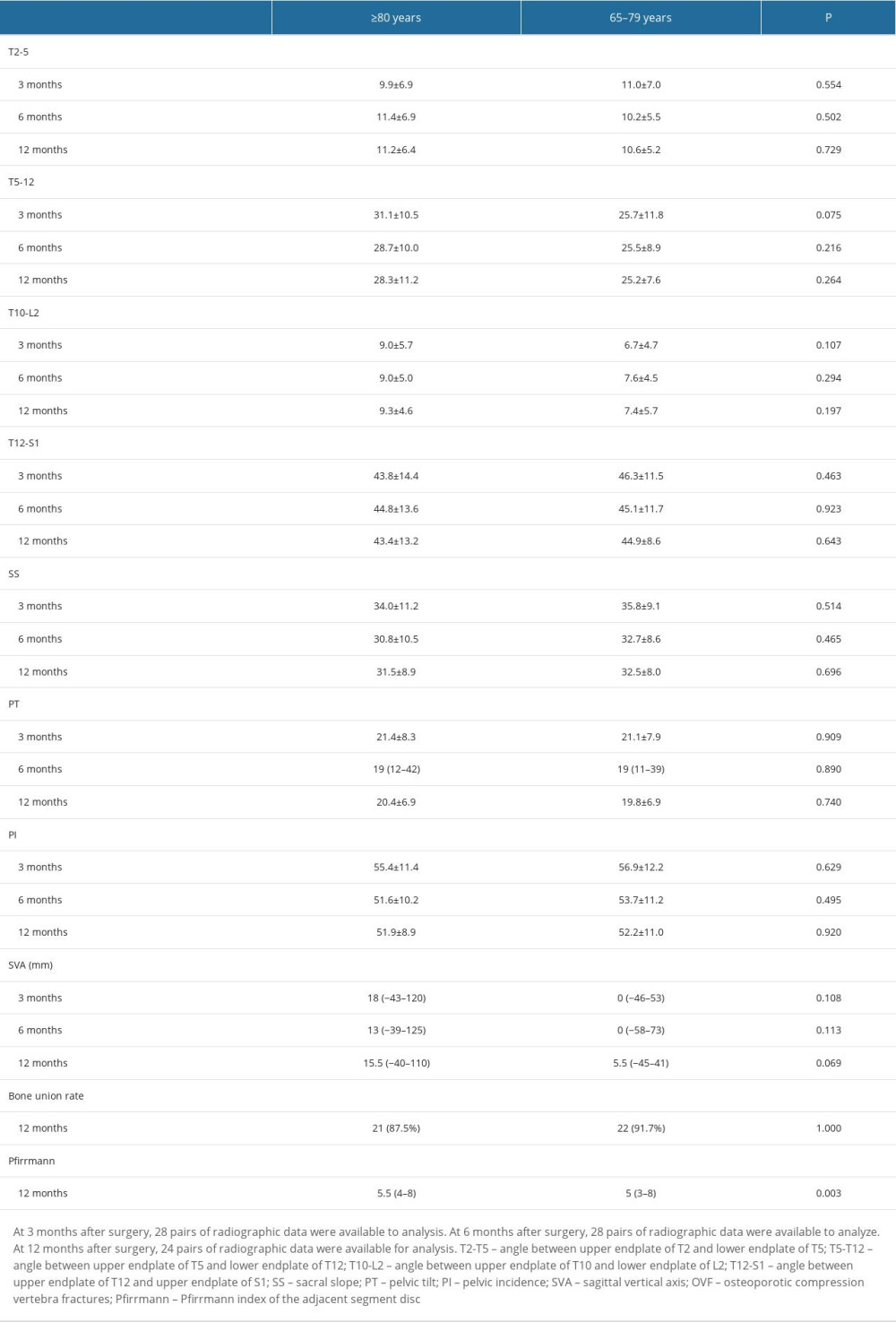
The preoperative radiographic data included all-spine lateral radiograph, extension-flexion lateral radiograph, lumbar magnetic resonance imaging (MRI), and bone density test. An immediate postoperative lumbar lateral radiograph was performed to determine if the screws were positioned correctly. All-spine lateral X-rays were performed at 3, 6, and 12 months. A lumbar MRI was performed at 6 and 12 months. Lumbar computed tomography (CT) was performed at 12 months. Preoperative and postoperative all-spine lateral radiographs were used to evaluate the sagittal parameters and implant-related complications and to record the preoperative osteoporotic compression vertebra fractures (OVF) and the postoperative new-onset OVF. All sagittal spino-pelvic parameters were collected, including sagittal vertical axis (SVA), sacral slope (SS), pelvic tilt (PT), pelvic incidence (PI), upper thoracic kyphosis angle (T2-T5), lower thoracic kyphosis angle (T5-T12), thoracolumbar lordosis angle, and lumbar lordosis angle (LLA) (T12-S1) at each follow-up time point [21]. The bone union status was assessed using the postoperative CT. The Pfirrmann index was used to grade the degree of adjacent disc degeneration from levels 1 to 8 [22]. The middle part of the disc was selected in T2WI sagittal lumbar MRI images to obtain the Pfirrmann index to ensure consistency of grading criteria. For patients without L5/S1 fusion, the Pfirrmann index was defined as the average of the upper and lower adjacent segment discs. For patients with L5/S1 fusion, the Pfirrmann index referred to the upper adjacent segment disc.
STATISTICAL ANALYSIS:
SF-36 (including PCS and MCS) was used as the main outcome. According to previous studies, the relevant parameter values were set at α=0.05 (bilateral) and β=0.10. By using PASS 15.0 (NCSS, USA), the sample size of each group was 10 cases. Assuming that the loss to follow-up rate was 20%, the required sample size was 12 patients in each group. Data were analyzed using SPSS 23.0 (IBM, Armonk, NY, USA). Patients with missing data were excluded. The Shapiro-Wilk normality test was performed to determine the distribution normality of all data. Normally distributed data are presented as means±standard deviation (SD) and analyzed using the independent
Results
CHARACTERISTICS OF THE PATIENTS:
Thirty-three patients with LSS were included in the ≥80 years group. After matching based on sex and surgical segment, 33 patients in the 65–79 years group were included.
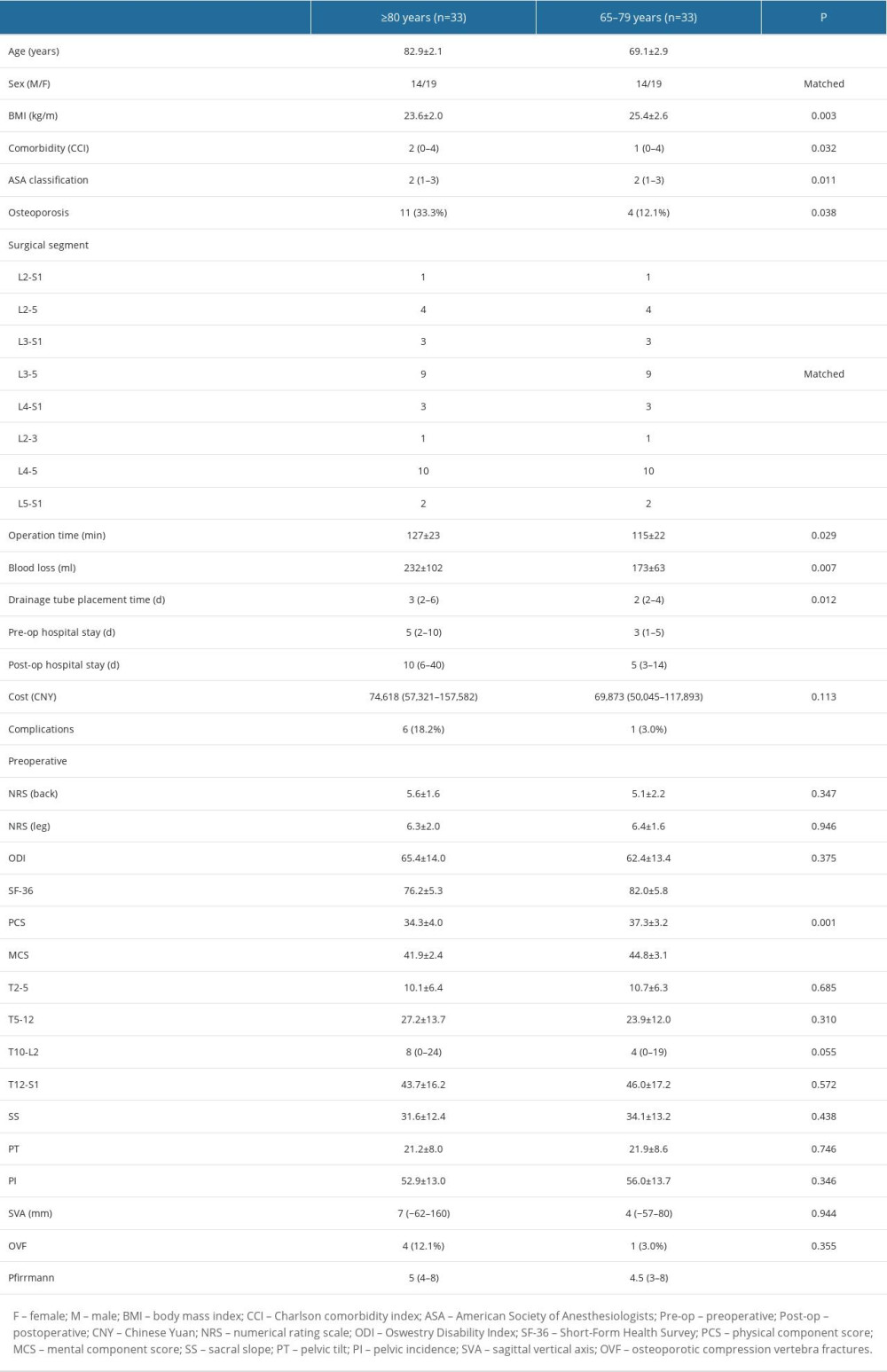
The mean age of the patients in the ≥80 years group was 82.9±2.1 years (range, 80–88 years). The mean age of the patients in the 65–79 years group was 69.1±2.9 years (range, 65–78 years). There were significant differences in BMI, CCI, ASA classification, osteoporosis, operation time, blood loss, drainage tube placement time, pre-operation hospital stay, post-operation hospital stay, SF-36, PCS, MCS, and Pfirrmann index between the 2 groups (all P<0.05) (Table 1).
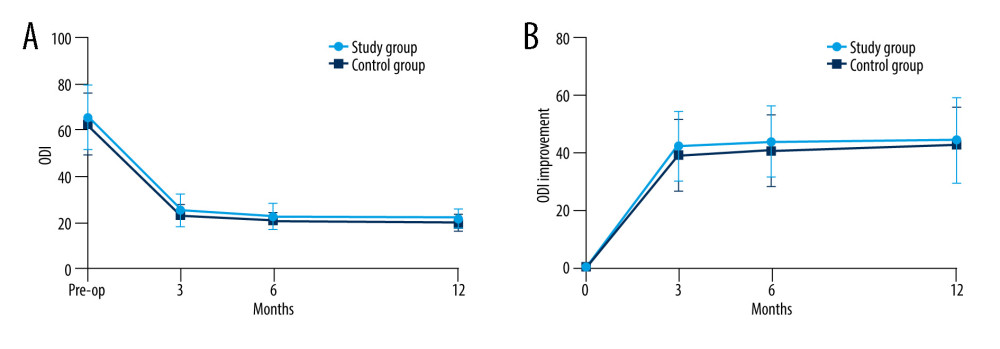
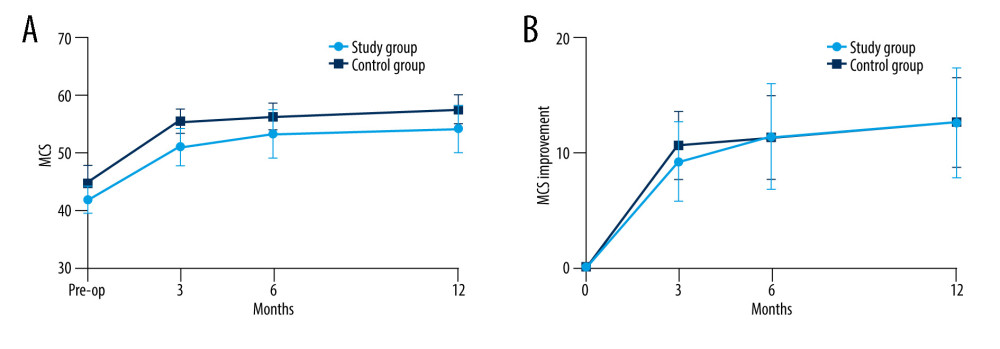
The NRS (back) in the ≥80 years group was significantly higher than in the 65–79 years group at 3 months after the operation: 2 (0–3) vs 1 (0–3), P=0.001. The SF-36 (3 months: 15.7±4.9 vs 27.6±5.4, P<0.001; 6 months: 27.3±6.8 vs 31.5±5.6, P=0.011) and PCS (3 months: 6.5±2.5 vs 17.0±3.6, P<0.001; 6 months: 15.9±3.4 vs 20.1±3.1, P<0.001) improvements at 3 and 6 months postoperatively in the ≥80 years group were significantly smaller than in the 65–79 years group (all P<0.05) (Figure 1). There were no differences in ODI and MCS improvements between the 2 groups (Table 2 and Figures 2, 3).
There were no significant differences in any radiographic outcomes between the 2 groups, except for Pfirrmann index at 12 months (≥80 years group vs 65–79 years group: 5.5 (4–8) vs 5 (3–8), P=0.003) (Table 3).
Postoperative complications occurred in 6 patients in the ≥80 years group (18.2%), including 1 case of wound infection, 2 of poor wound healing, 2 of delirium, and 1 of intermuscular vein thrombosis. One patient in the 65–79 years group (3.0%) had complicated wound incision healing.
Discussion
In a multicenter observational study, Giannadakis et al [23] followed patients who underwent laminectomy or microdecompression; they compared those ≥80 years (n=178) with those 21–79 years (n=1325) and found no differences in ODI and NRS (back and leg) at 1 year after surgery. In another study, the ODI recovered to 27.3 and 23.7, NRS (back) recovered to 3.6 and 3.9, and NRS (leg) recovered to 3.5 and 3.6 (≥80 vs <80 years) at 1 year postoperatively [24]. Similar results were obtained in a single-center retrospective study: patients >80 years (n=38) and <80 years (n=28) underwent lumbar fusion surgery and had comparable clinical outcomes [25]. Likewise, in the present study, there were no differences in the postoperative improvement of ODI. Most previous studies only provided final data at the last follow-up without comparing multiple follow-up results in the short term [24–27]. We found that the improvement of ODI was greater within 3 months after surgery. It stabilized after 6 months after surgery, and the trendof ODI improvement was also similar in the 2 groups. At 12 months after the operation, the ODI of the 2 groups recovered to 21.6±4.3 and 19.6±3.7, and the improvement of ODI was 44.3±14.8 and 42.6±13.2 (≥80 years vs 65–79 years). On the one hand, the pain improvement of patients ≥80 years was not different from those of patients younger than 80 years after surgery. On the other hand, it also showed that the speed of pain recovery in the 2 groups was similar, and most of the pain symptoms were relieved within 3 months after surgery. No study has reported this result yet. In the present study, at 3 months, the NRS (back) in the ≥80 years group was higher than in the 65–79 years group, which might be related to older age and a higher prevalence of osteoporosis [28], but there was no difference in NRS (back and leg) between the 2 groups at 6 months and 12 months after surgery.
LSS seriously affects the patients’ quality of life and, to varying degrees, affects the patients’ physical and mental health [29]. SF-36 is a commonly used health self-assessment questionnaire that can effectively assess patients’ physiological function and psychological status [20]. In a 2-year follow-up of patients ≥80 years vs 65–79 years who underwent posterior lumbar interbody fusion (PLIF), Hayashi et al [10] found that only the body pain (BP) subdomain of SF-36 was significantly improved in the elderly group. Rihn et al [27] reported on patients with lumbar degenerative disease treated surgically or conservatively and found no differences in PCS scores between patients >80 years vs those 65–79 years. However, neither of these 2 studies assessed the dynamic outcomes of SF-36 at multiple follow-up time points after surgery. In the present study, the preoperative baseline PCS and MCS differed between the 2 groups. This difference could be due to the negative impact of more comorbidities on the physical function and self-perception health of the patients in the ≥80 years group. Interestingly, the improvement in MSC was comparable between the 2 groups at all postoperative follow-up time points. In addition, the MCS of both groups was mostly improved at 3 months postoperatively and gradually stabilized during follow-up. Pain was mostly relieved in both groups at 3 months postoperatively, which might have resulted in improved MCS. The improvement of ODI and MCS in the 2 groups had similar trends over time, validating that hypothesis. The PCS of the 65–79 years group was significantly improved 3 months after surgery and stabilized during follow-up. PCS improvement in the ≥80 years group was slower and was comparable to the 65–79 years group until 12 months after surgery. This might be because patients ≥80 years have poorer overall health and take longer to recover after surgery. Surgeons should make patients ≥80 years aware of the slow recovery of function after surgery and help patients establish reasonable expectations that can lead to better surgical satisfaction [30]. The PCS of the ≥80 years group was lower than in the 65–79 years group at 12 months. Older patients usually have a longer disease course, which means the nerve is compressed for longer, leading to less mobility after surgery [31,32]. Therefore, we believe that to avoid long-term nerve compression resulting in poor postoperative physiological recovery, patients with surgical indications should undergo timely surgical treatment, which is also suitable for patients ≥80 years old.
More postoperative complications occurred in the ≥80 years group compared to the 65–79 years group, which was consistent with the results of some other studies [26,33]. Prolonged operation time was associated with a higher risk of complications [34,35]. Prolonged drainage tube placement time may increase the risk of postoperative wound infection or poor wound healing [36]. The present study had similar results. The prevalence of osteoporosis was significantly higher in the ≥80 years group than in the 65–79 years group. Poor bone condition means greater difficulty in screw placement and decompression, which can increase operation time and blood loss, further increasing drainage tube placement time and complication rates. This suggests that surgeons should be alert for postoperative complications in patients ≥80 years.
Sagittal balance is an important radiographic index in lumbar fusion surgery. Sagittal imbalance contributes to low back pain and adjacent segment degeneration (ASD) [37–40]. A meta-analysis demonstrated that the loss of lumbar lordosis was significantly associated with low back pain [38]. He et al [37] suggested that insufficient improvement in PT can lead to unsatisfactory postoperative low back pain relief. Liow et al [39] found that patients with short-segment lumbar fusion surgery with a postoperative SS >30° had a lower incidence of low back pain. The present study showed no significant differences in sagittal parameters.
Lower postoperative bone union rates were reported in patients >80 years compared with younger patients [10,24], which was not entirely consistent with the present study since there was no significant difference (87.5% vs 91.7%), perhaps because of the use of the modified facet joint bone graft fusion that has been used by the authors for many years. The higher bone union rate is one of the advantages of this technique [14,15]. No new-onset OVF occurred in all patients during the 1-year follow-up, which could be due to insufficient follow-up time. In addition, the patients strictly wore lumbar support for 3 months after surgery.
In the present study, none of the patients developed ASD during the 12-month follow-up, which may be related to the short follow-up. The Pfirrmann index of adjacent segmental intervertebral discs in the ≥80 group was higher than in the 65–79 years group at baseline and 12 months indicating that age ≥80 years does not aggravate the progression of ASD in patients with LSS after lumbar fusion surgery in the short term. However, further verification with longer follow-up is required.
This study has some limitations. First, the sample size was small, mainly due to the strict inclusion and exclusion criteria and the nature of a single-center study. Second, the retrospective nature of the study limited the data to those available from the charts. Future studies should further expand the sample size and conduct multicenter studies to validate existing findings. Nonetheless, this study has some strengths. First, the 2 groups were strictly matched by sex and surgical segment. Second, data not available in previous studies were reported here, including drainage tube placement time, sagittal parameters, and Pfirrmann index of adjacent segmental intervertebral discs.
Conclusions
Although recovery of postoperative physiology is slower in patients ≥80 years of age compared with patients aged 65–79 years, lumbar fusion surgery is safe for patients with LSS ≥80 years old. Surgical treatment provides comparable improvements in pain and quality of life in patients over 80 years of age as in younger patients. In view of the poor postoperative physiological function of elderly patients, patients ≥80 years of age should receive timely surgical treatment for better functional recovery.
References
1. Harper S, Economic and social implications of aging societies: Science, 2014; 346(6209); 587-91
2. Fang EF, Scheibye-Knudsen M, Jahn HJ: Ageing Res Rev, 2015; 24(Pt B); 197-205
3. Siebert E, Pruss H, Klingebiel R, Lumbar spinal stenosis: syndrome, diagnostics and treatment: Nat Rev Neurol, 2009; 5(7); 392-403
4. World Health Organization: Ageing and health: A health promotion approach for developing countries, 2003
5. Lurie J, Tomkins-Lane C, Management of lumbar spinal stenosis: BMJ, 2016; 352; h6234
6. Reid PC, Morr S, Kaiser MG, State of the union: A review of lumbar fusion indications and techniques for degenerative spine disease: J Neurosurg Spine, 2019; 31(1); 1-14
7. Deyo RA, Mirza SK, Martin BI, Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults: JAMA, 2010; 303(13); 1259-65
8. Choi JM, Choi MK, Kim SB, Perioperative results and complications after posterior lumbar interbody fusion for spinal stenosis in geriatric patients over than 70 years old: J Korean Neurosurg Soc, 2017; 60(6); 684-90
9. Nagata K, Nakamoto H, Kato S, Minimum clinically important change for outcome scores among patients aged 75 or over undergoing lumbar spine surgery: Eur Spine J, 2021; 30(5); 1226-34
10. Hayashi K, Matsumura A, Konishi S, Clinical outcomes of posterior lumbar interbody fusion for patients 80 years of age and older with lumbar degenerative disease: Minimum 2 years’ follow-up: Global Spine J, 2016; 6(7); 665-72
11. Lagman C, Ugiliweneza B, Boakye M, Spine surgery outcomes in elderly patients versus general adult patients in the United States: A MarketScan analysis: World Neurosurg, 2017; 103; 780-88
12. Liang H, Lu S, Jiang D, Clinical outcomes of lumbar spinal surgery in patients 80 years or older with lumbar stenosis or spondylolisthesis: A systematic review and meta-analysis: Eur Spine J, 2020; 29(9); 2129-42
13. Leone A, Guglielmi G, Cassar-Pullicino VN, Lumbar intervertebral instability: A review: Radiology, 2007; 245(1); 62-77
14. Ren Z, Li Z, Li S, Modified facet joint fusion for lumbar degenerative disease: Case series of a fusion technique, clinical outcomes, and fusion rate in 491 patients: Oper Neurosurg (Hagerstown), 2020; 19(3); 255-63
15. Li Z, Li Z, Chen X, Comparison between modified facet joint fusion and posterolateral fusion for the treatment of lumbar degenerative diseases: A retrospective study: BMC Surg, 2022; 22(1); 29
16. Charlson ME, Pompei P, Ales KL, A new method of classifying prognostic comorbidity in longitudinal studies: development and validation: J Chronic Dis, 1987; 40(5); 373-83
17. Sankar A, Johnson SR, Beattie WS, Reliability of the American Society of Anesthesiologists physical status scale in clinical practice: Br J Anaesth, 2014; 113(3); 424-32
18. Shafshak TS, Elnemr R, The visual analogue scale versus numerical rating scale in measuring pain severity and predicting disability in low back pain: J Clin Rheumatol, 2021; 27(7); 282-85
19. Liu H, Tao H, Luo Z, Validation of the simplified Chinese version of the Oswestry Disability Index: Spine (Phila Pa 1976), 2009; 34(11); 1211-16 discussion 1217
20. Li L, Wang HM, Shen Y, Chinese SF-36 Health Survey: Translation, cultural adaptation, validation, and normalisation: J Epidemiol Community Health, 2003; 57(4); 259-63
21. Schroeder J, Schaar H, Mattes K, Spinal alignment in low back pain patients and age-related side effects: A multivariate cross-sectional analysis of video rasterstereography back shape reconstruction data: Eur Spine J, 2013; 22(9); 1979-85
22. Griffith JF, Wang YX, Antonio GE, Modified Pfirrmann grading system for lumbar intervertebral disc degeneration: Spine (Phila Pa 1976), 2007; 32(24); E708-12
23. Giannadakis C, Solheim O, Jakola AS, Surgery for lumbar spinal stenosis in individuals aged 80 and older: A multicenter observational study: J Am Geriatr Soc, 2016; 64(10); 2011-18
24. Liao JC, Chiu PY, Chen WJ, Surgical outcomes after instrumented lumbar surgery in patients of eighty years of age and older: BMC Musculoskelet Disord, 2016; 17(1); 402
25. Liao JC, Chen WJ, Surgical outcomes in the elderly with degenerative spondylolisthesis: Comparative study between patients over 80 years of age and under 80 years-a gender-, diagnosis-, and surgical method-matched two-cohort analyses: Spine J, 2018; 18(5); 734-39
26. Son HJ, Jo YH, Ahn HS, Outcomes of lumbar spinal fusion in super-elderly patients aged 80 years and over: Comparison with patients aged 65 years and over, and under 80 years: Medicine (Baltimore), 2021; 100(31); e26812
27. Rihn JA, Hilibrand AS, Zhao W, Effectiveness of surgery for lumbar stenosis and degenerative spondylolisthesis in the octogenarian population: analysis of the Spine Patient Outcomes Research Trial (SPORT) data: J Bone Joint Surg Am, 2015; 97(3); 177-85
28. Hikata T, Ishii K, Matsumoto M, Risk factor for poor patient satisfaction after lumbar spine surgery in elderly patients aged over 80 years: Clin Spine Surg, 2021; 34(4); E223-28
29. Yagi M, Suzuki S, Nori S, How decompression surgery improves the lower back pain in patient with lumbar degenerative stenosis: A propensity-score-matched analysis: Spine (Phila Pa 1976), 2022; 47(7); 557-64
30. Witiw CD, Mansouri A, Mathieu F, Exploring the expectation-actuality discrepancy: A systematic review of the impact of preoperative expectations on satisfaction and patient reported outcomes in spinal surgery: Neurosurg Rev, 2018; 41(1); 19-30
31. Hebert JJ, Abraham E, Wedderkopp N, Preoperative factors predict postoperative trajectories of pain and disability following surgery for degenerative lumbar spinal stenosis: Spine (Phila Pa 1976), 2020; 45(21); E1421-30
32. Aimar E, Iess G, Gaetani P, Degenerative lumbar stenosis surgery: predictive factors of clinical outcome-experience with 1001 patients: World Neurosurg, 2021; 147; e306-14
33. Puvanesarajah V, Jain A, Shimer A, Complications and mortality following 1 to 2 level lumbar fusion surgery in patients above 80 years of age: Spine, 2017; 42(6); 437-41
34. Wang M, Widi G, Levi A, The safety profile of lumbar spinal surgery in elderly patients 85 years and older: Neurosurg Focus, 2015; 39(4); E3
35. Watanabe T, Kanayama M, Takahata M, Perioperative complications of spine surgery in patients 80 years of age or older: A multicenter prospective cohort study: J Neurosurg Spine, 2019 [Online ahead of print]
36. Pennington Z, Lubelski D, Molina C, Prolonged post-surgical drain retention increases risk for deep wound infection after spine surgery: World Neurosurg, 2019; 130; e846-53
37. He S, Zhang Y, Ji W, Analysis of spinopelvic sagittal balance and Persistent Low Back Pain (PLBP) for Degenerative Spondylolisthesis (DS) following Posterior Lumbar Interbody Fusion (PLIF): Pain Res Manag, 2020; 2020; 5971937
38. Chun SW, Lim CY, Kim K, The relationships between low back pain and lumbar lordosis: A systematic review and meta-analysis: Spine J, 2017; 17(8); 1180-91
39. Liow MHL, Goh GS, Chua JL, Sagittally balanced degenerative spondylolisthesis patients with increased sacral slope and greater lumbar lordosis experience less back pain after short-segment lumbar fusion surgery: Clin Spine Surg, 2020; 33(5); E231-35
40. Takeda K, Okada E, Shinozaki Y, Risk factors for early-onset radiographical adjacent segment disease in patients with spondylolytic spondylolisthesis after single-level posterior lumbar interbody fusion: Spine J Jul, 2022; 22(7); 1112-18
Figures
In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387