01 May 2023: Clinical Research
Evaluation of Preoperative Magnetic Resonance Imaging Parameters with Arthroscopic Validation of Subscapularis Tendon Abnormalities in 187 Patients at a Single Center in Turkey
Gokhan IlyasDOI: 10.12659/MSM.939772
Med Sci Monit 2023; 29:e939772






Abstract
BACKGROUND: This study from a single center in Turkey aimed to evaluate preoperative magnetic resonance imaging (MRI) parameters with arthroscopic validation of subscapularis (SS) tendon abnormalities in 187 patients.
MATERIAL AND METHODS: Preoperative MRI scans of 187 patients who had undergone arthroscopic shoulder surgery by the senior author (all in lateral decubitus position) were evaluated by 3 researchers. Patients with arthroscopically proven SS tendon rupture (n=69) and without rupture (n=118) were divided into 2 groups and compared with various distances and angles. The following parameters were measured: coracohumeral distance (CHD), coracoid morphology, coraco-glenoid angle (CGA), coracoid angle (CA), coraco-humeral angle (CHA), coracoid overlap (CO), coracoid body-glenoid angle (CBGA), coracoid tip-glenoid angle (CTGA), coracoid tip-body angle (CTBA), coraco-scapular angle (CSA), lesser tuberosity angle (LTA), and lesser tuberosity height (LTH).
RESULTS: CHD, CHA, CA, and LTA values decreased in the SS tendon rupture group; coracoid type grade and CO increased (all P<0.001, excluding LTA [P=0.022]). The cut-off values of these measurements were CHD=7.25 mm, CHA=107.25°, CA=111.5°, LTA=31.7°, and CO=16.5 mm. The differences in CGA and CBGA values were not statistically significant (P=0.11, 0.441, respectively). CTGA, CTBA, LTH, and CSA measurements were not included in the intergroup comparisons due to insufficient inter-observer reliability (κ=0.478, 0.239, 0.496, 0.309, respectively). Power (1- b) in post hoc analysis was calculated as 0.941.
CONCLUSIONS: SS tendon rupture was associated with a reduction in the parameters of CHD, CHA, CA, and LTA and an increase in CO on MRI.
Keywords: rotator cuff, Rotator Cuff Injuries, Arthroscopy, Shoulder, Magnetic Resonance Imaging, Humans, Turkey, Reproducibility of Results, Retrospective Studies, Tendon Injuries, Shoulder Joint, Rupture
Background
It is known that the accuracy of magnetic resonance imaging (MRI) is poorer in the diagnosis of subscapularis (SS) tendon tears than in the diagnosis of supraspinatus (SSP), infraspinatus (ISP), and teres minor tears [1]. Bigliani et al found that acromial morphology is a risk factor for rotator cuff injury [2]. Gerber et al defined the sub-coracoid space and coracoid overlap index [3,4]. It is now known that the coraco-humeral distance is involved in the etiology of SS rupture, and studies showing this relationship have been published [5,6]. The usability of many parameters in the preliminary diagnosis of SS rupture has been evaluated by researchers. These include coraco-humeral distance (the shortest distance between the coracoid process and the tuberculum minus on axial views) [5–14], coracoid morphology (type A: flat coracoid, type B: osteophyte at the tip of the coracoid, type C: hooked coracoid) [12,13,15], coracoid angle (the angle between the long axes of the proximal and distal segments of the coracoid process on T1-weighted oblique sagittal views) [15], coraco-glenoid angle (the angle between a line running from the most distal part of the coracoid process to the anterior glenoid corner and a line running along the plane of the glenoid surface on axial views) [7,14], coraco-humeral angle (the angle between lines drawn tangentially from the tip of the coracoid process to the medial and lateral aspects of the humeral head on axial views) [7,14], coracoid overlap (the distance between the most distal part of the coracoid process and the glenoid on axial views) [8,14], coracoid body-glenoid angle (the angle between a line running along the plane of the glenoid surface and the coracoid body on axial views) [16], coracoid tip-glenoid angle (the angle between a line running along the plane of the glenoid surface and the coracoid tip on axial views) [16], coracoid tip-body angle (the angle between the coracoid body and the coracoid tip on axial views) [16], coraco-scapular angle (the angle between the base of the coracoid and the scapular line on axial views, it was defined as the coracoid angle in the original study) [17], coraco-lesser tuberosity angle (it was not included in the study because it was calculated from radiography) [18], lesser tuberosity angle (the angle between the vertical line that equally divides the line connecting the anterior and posterior cartilage of the humeral head and the most prominent part of the lesser tuberosity on axial views) [18], and lesser tuberosity height (the distance between the line from the margin of the anterior cartilage to the baseline of the bicipital groove and the parallel line passing the most prominent edge of the tuberculum minus on axial views) [14,18]. However, some findings, such as long head of biceps tendon tear or malposition and the comma sign, have been implicated as predictive findings of SS rupture on MRI [19,20]. It is known that SS tendon abnormalities can be associated with the chronicity of SSP tendon tears, and injury to the SSP can cause edema in the lesser tuberosity [21].
Although many studies have been conducted to strengthen the diagnosis of SS tendon ruptures, the false negativity of imaging methods should not be ignored. Few studies have performed MRI evaluation in cases of arthroscopically proven SS tendon rupture [18,22]. We made all measurements considering that the accuracy would increase with the use of retrospective MRI scans of arthroscopically proven cases.
Malavolta et al showed that the MRI sensitivity of SS tendon tears was 0.68 (95% CI 0.64–0.72) in a meta-analysis study involving 1858 shoulders [1]. In our study, which was inspired by the study of Malavolta, we investigated whether it is possible to increase the sensitivity of occult SS tendon tears by measuring various angles and distances in retrospectively scanned MRIs. Therefore, this study from a single center in Turkey aimed to evaluate preoperative MRI parameters with arthroscopic validation of SS tendon abnormalities in 187 patients.
Material and Methods
ETHICS STATEMENT:
Approval for this study was obtained by the Institutional Review Board of Usak University Faculty of Medicine (date: 10/11/2022, decision number: 08/08/08), and informed consent was obtained from all participants.
SOURCE OF PATIENTS:
In our clinic, 355 patients who had undergone arthroscopic shoulder surgery by the senior author in the last 3 years (January 2019 to February 2023) were retrospectively analyzed.
INCLUSION AND EXCLUSION CRITERIA:
The inclusion criteria were patients who had undergone shoulder arthroscopy surgery by the senior author for any reason in the last 3 years. The exclusion criteria were preoperative MRI views that could not be obtained (n=12), the presence of systemic inflammatory disease (n=13), shoulder osteoarthritis (n=34), instability with or without bone defect (n=24), the coexistence of SSP and ISP tear (n=57), presence of significant subscapularis tendon total rupture on MRI (n=8), patients with a history of previous shoulder surgery (n=9), and age under 18 years (n=11).
DATA COLLECTED:
Preoperative MRI scans of 187 patients (53%) included in the study were evaluated by 3 researchers on the same picture archiving and communication system at different times. Patients with arthroscopically proven SS tendon rupture (n=69) and without rupture (n=118) were divided into 2 groups and compared with various distances and angles. Distances and angles evaluated included the coraco-humeral distance, coracoid morphology (according to the Leite-Torres classification [15]), coraco-glenoid angle, coraco-humeral angle, coracoid overlap, coracoid body-glenoid angle, coracoid tip-glenoid angle, coracoid tip-body angle, coraco-scapular angle, lesser tuberosity angle, and lesser tuberosity height. Measurements were made on the existing Fonet Dicom Viewer v4.1 (Fonet Bilgi Teknolojileri A.Ş., Gölbaşı, Ankara, TR), and no additional software was used. A comparison of these measurements was made between the 2 groups, with and without SS rupture. It was evaluated whether various measurements would be helpful in the diagnosis of occult SS tendon rupture, which is known to have a high false-negative rate [1,23,24].
Since the coraco-lesser tuberosity angle was calculated from radiography, it was not included in the MRI evaluation. In addition, age, categorical data of the patients such as sex, which dominant hand was used, and SS tendon evaluations on MRI (rupture, tendinosis, and intact) were noted.
Lafosse classification is frequently used in the evaluation of SS ruptures [25]. According to this classification, type I defines superior one-third partial lesion, type II defines superior one-third complete lesion, type III defines superior two-thirds complete lesion, and types IV and V define total lesions. Since occult ruptures of the SS were evaluated with MRI in this study, types I, II, and III were included, but types IV and V, which included total ruptures, were not included.
All MRI scans were done with 1.5 Tesla units (Siemens Magnetom Aera, Erlangen, Germany) and performed at 2-mm intervals. Dugarte et al showed that the sub-coracoid distance narrowed in the internal rotation position compared with the neutral position [12], and all MRI scans in our study were taken in the neutral position as standard. T2-weighted axial section and T1-weighted oblique sagittal section were used in MRI measurements.
Tan et al reported that there was no statistical difference between computed tomography and MRI in the evaluation of the sub-coracoid space [26]. In this study, MRI, which is frequently used in clinical practice in rotator cuff pathologies, was used when measurements were made.
STATISTICAL ANALYSIS:
SPSS (Statistical Package for the Social Sciences) version 24 (IBM Corp, Armonk, New York, USA) was used for statistical analysis. The Fisher’s exact test and chi-square test were used to compare categorical data. The Shapiro-Wilk test was applied to the measurements to be evaluated for normality analysis. The SS rupture group and the non-ruptured group were evaluated by applying Mann-Whitney U analysis to the parameters without normal distribution, and an independent
Results
DEMOGRAPHIC DATA:
The mean age was 55.7±11.1 (19–73) years in the rupture group, with arthroscopic confirmation of SS tendon rupture, and the mean age was 53.3±13.8 (18–80) years in the non-rupture group, which was found to have no SS tendon rupture (
SUBSCAPULARIS RUPTURE TYPES AND ASSOCIATION WITH OTHER ROTATOR CUFF TENDONS:
Of the 187 patients included in the study, 157 (84%; 56 and 101 patients in the rupture and non-rupture groups, respectively) had SSP lesions and 30 (16%; 13 and 17 patients in the rupture and non-rupture groups, respectively) had ISP lesions (P=0.419; Table 1). Patients with both SSP and ISP (n=57) tears were excluded from the study because they would adversely affect the measurements. According to the Lafosse classification, 36 (52%) patients in the rupture group had type I, 20 (29%) had type II, and 13 (19%) had type III subscapularis tears. Patients with type IV lesions (7 patients) and type V lesions (1 of 8 completely ruptured patients) were not included in the study. When 56 patients with SSP tears were evaluated, it was observed that in the group with SSP fatty atrophy (n=12), 9 patients had type III, 2 patients had type II, and 1 patient had type I SS tears, and in patients with SSP rupture without atrophy (n=44), 3 patients had type III, 14 patients had type II, and 27 patients had type I SS tears. Type III SS tendon tear was found in 1 patient, type II in 4 patients, and type I in 8 of 13 patients without SSP lesions (Spearman Rho=0.383, P=0.001).
MEASUREMENT PARAMETERS:
The false-negative rates of SS tendon ruptures and tendinosis on MRI were evaluated. Tendinosis was accepted as the presence of degeneration without rupture of the tendon. Detection of tendinosis findings on MRI was included in the rupture group because it showed that the SS tendon was not completely normal. Rupture or tendinosis was observed in 38 patients (55%) in the rupture group (n=69), while the subscapularis tendon was evaluated as intact in 31 patients (
According to the Leite-Torres classification, in the rupture group, 16 (23%) patients had type I, 35 (51%) had type II, and 18 (26%) had type III coracoids, while 75 (63%) had type I, 34 (29%) had type II, and 9 (8%) had type III coracoids in the non-rupture group (P<0.001; Table 2). While coracoid angle examined in the oblique sagittal MRI section was 103.6±8.6° (82–117°) in the rupture group, it was 117.2±7.1° (88–129°) in the non-rupture group (P<0.001; Table 3, Figure 1). According to the receiver operator characteristic (ROC) curve, sensitivity was 80% and specificity was 83% for SS tears at a cut-off value of 111.5° for the coracoid angle. When coracoid angle was evaluated according to the tear type, it was 107.2±7 (n=36) in the type I group, 101.94±8.5 (n=20) in the type II group, and 94.77±8 (n=13) in the type III group. When the rupture groups were evaluated, a statistically significant difference was found between type I and type III, but this difference was not observed between the other groups (type I vs II, P=0.16; type II vs III, P=0.21; type I vs III, P<0.001).
The coraco-humeral distance was 6.87±0.6 (5.3–7.8) mm in the arthroscopically confirmed rupture group, while it was 7.8±0.77 (6.3–10.7) mm in the non-ruptured group (P<0.001). Based on the ROC curve evaluation, 77% sensitivity and 76% specificity were found for SS tears at a cut-off value of 7.25 mm for the coraco-humeral distance (Table 3, Figure 2). In the rupture groups, 6.84±0.4, 6.82±0.23, and 6.79±0.23 values were determined for rupture groups I, II, and III, respectively. There was no statistically significant difference between the type of rupture groups (type I vs II, P=0.825; type I vs III, P=0.678; type II vs III, P=0.736).
While coraco-humeral angle was 109±4.4° (98–119°) in the rupture group, it was 105.2±5.8° (90.5–121°) in the non-rupture group (P<0.001) (Table 3; Figure 3). According to the ROC curve results, 67% sensitivity and 68% specificity were found for SS tears at a cut-off value of 107.25° for coraco-humeral angle. In the rupture groups I to III, 108.3±1.76, 109.2±1.3, and 109.2±1.18 values were determined, respectively. There was no statistically significant difference between these groups (type I vs II, P=0.69; type I vs III, P=0.18; type II vs III, P=0.69).
The coraco-glenoid angle was 131.7±4.7° (121.5–142.5°) in the rupture group and 133.3±4.2° (122–142°) in the non-rupture group (P=0.11; Table 3).
The coracoid overlap was 18.22±2.01 (14.2–21.3) mm in the rupture group and 13.7±2.73 (11.3–18.2) mm in the non-rupture group (P<0.001) (Table 3, Figure 4). Based on the ROC curve evaluation, 83% sensitivity and 80% specificity were found for SS tears at a cut-off value of 16.5 mm. When the overlap according to the tear type was evaluated, the values were 17.5±1.78, 18±1.41, and 20.7±1.66, respectively. When the groups were evaluated among themselves, the P=0.285 between type I and type II, and P<0.001 between the other groups.
The coracoid body-glenoid angle was 63.2±8.5° (43–85°) in the rupture group and 64±9.5° (42–95°) in the non-rupture group (P=0.441; Table 3).
The lesser tuberosity angle in the rupture group was 32.55±1.9° (27–38°), while in the non-rupture group, it was 31.81±1.35° (28–38°) (P=0.022; Table 3, Figure 5). According to the ROC curve, sensitivity was 65% and specificity was 51% for SS tears at a cut-off value of 31.7° for the lesser tuberosity angle. According to the tear type, the lesser tuberosity angle was 31.64±1.27 in the type I group, 33.01±2.21 in the type II group, and 34.36±1.35 in the type III group. When the groups were compared, the P value was 0.058 between groups type II and III, while P<0.001 for comparisons between type I and II, and type I and III.
Coracoid tip-glenoid angle, coracoid tip-body angle, lesser tuberosity height, and coraco-scapular angle measurements were not included in the intergroup comparisons owing to insufficient inter-observer reliability (κ=0.478, 0.239, 0.496, 0.309, respectively). Measurements with a Kappa value above 0.60 (substantial or almost perfect agreements) were included in the assessment (Table 4).
Power (1-
Discussion
This study showed that the decrease of coracohumeral distance, coracohumeral angle, coracoid angle, and lesser tuberosity angle and the increase in the degree of coracoid type and coracoid overlap are very important predictive values in the determination of SS tendon rupture (all
Seo et al defined coraco-lesser tuberosity angle, lesser tuberosity angle, and lesser tuberosity height as new predictors of SS tears [18]. The coraco-lesser tuberosity angle was not included in our study because it was measured on radiography. Seo et al found lesser tuberosity angle values in the SS tear group (33.4±4.3°) were statistically significantly higher than in the control group (31.0±3.9°,
Yu et al evaluated several parameters in addition to lesser tuberosity height that were in common with our study for sub-coracoid impingement on MRI, such as the coraco-humeral distance, coracoid overlap, coraco-glenoid angle, and coraco-humeral angle [14]. The coraco-humeral distance (4.7±1.2 mm, 7.7±1.5 mm;
In their study on MRI, Leite et al found the coracoid angle was the best predictor in the diagnosis of SS ruptures and that it was lower in the rupture group than in the normal group (
In one study, there was no relationship between measurements made by MRI and SS tendon lesions [27]. By contrast, in our study on arthroscopically validated cases, statistically significant differences were found between the rupture group and the other group at many angles and distances (Table 3).
Leite et al emphasized that narrowing the coracohumeral distance and an increase in the coracoid overlap distance are good indicators of SS ruptures [8]. Likewise, Zhu et al in a prospective study comparing bilateral shoulders, stated that coraco-humeral distance was the best predictor of SS ruptures (
In a study they conducted on MRI views, Asal et al found increased SS tendon tear in type C coracoid patients compared with those with type A and B. In the same study, they found that the decrease in the coraco-glenoid angle and coraco-humeral distance was associated with SS tendon tear (
Bergin et al found a moderate correlation in the relationship between SSP and SS tendon abnormalities (r=0.47,
Wang et al compared patients with and without partial SS rupture with different MRI parameters than in the present study [22], reporting that the fissure sign showed the highest diagnostic efficiency for partial SS tears (92% specificity, 75.3% sensitivity, and 81.3% accuracy). In the present study, coraco-humeral distance, coracoid overlap, coraco-humeral angle, lesser tuberosity angle, and coracoid angle measurements correctly identified SS ruptures before surgery.
The main limitation of the present study was the inability to measure all parameters in sufficient quality with MRI. Since MRI scans are performed at 2-mm intervals as standard, it may not be possible to evaluate some measurements accurately. Prospective planning would be more appropriate for thinner section MRI. A further limitation was that the MRI was 1.5 Tesla units, and measurements can be clearer with MRI with 3 Tesla units. The final limitation was the lack of radiological comparison of MRI views with measurements on other planes.
Conclusions
SS tendon rupture was associated with a reduction in the parameters of coraco-humeral distance, coraco-humeral angle, coracoid angle, and lesser tuberosity angle and an increase in coracoid overlap on MRI.
Figures
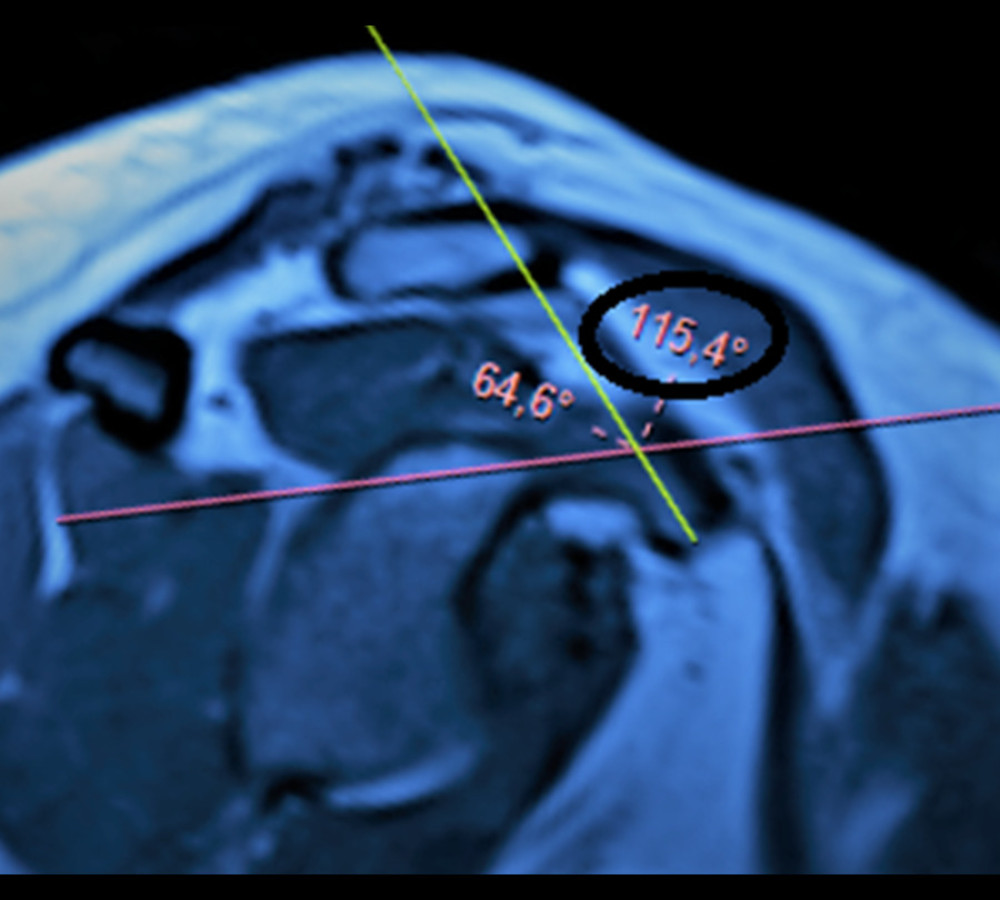 Figure 1. Coracoid angle. It is measured as the angle between the long axes of the proximal and distal segments of the coracoid process in a T1-weighted oblique sagittal magnetic resonance imaging section (circle). (Fonet Dicom Viewer, v4.1, Fonet Bilgi Teknolojileri A.Ş., Gölbaşı, Ankara, TR).
Figure 1. Coracoid angle. It is measured as the angle between the long axes of the proximal and distal segments of the coracoid process in a T1-weighted oblique sagittal magnetic resonance imaging section (circle). (Fonet Dicom Viewer, v4.1, Fonet Bilgi Teknolojileri A.Ş., Gölbaşı, Ankara, TR). 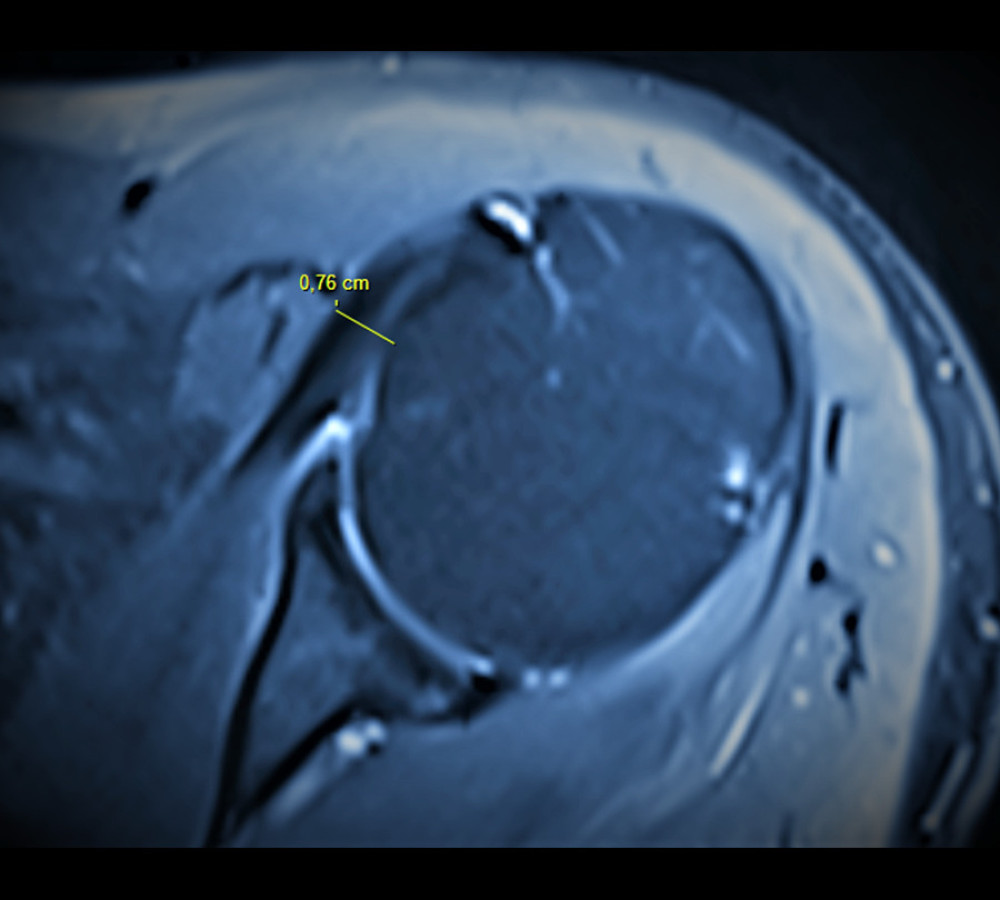 Figure 2. Coraco-humeral distance. It is measured as the shortest distance between the coracoid process and the tuberculum minus (axial T2-weighted magnetic resonance imaging section). (Fonet Dicom Viewer, v4.1, Fonet Bilgi Teknolojileri A.Ş., Gölbaşı, Ankara, TR).
Figure 2. Coraco-humeral distance. It is measured as the shortest distance between the coracoid process and the tuberculum minus (axial T2-weighted magnetic resonance imaging section). (Fonet Dicom Viewer, v4.1, Fonet Bilgi Teknolojileri A.Ş., Gölbaşı, Ankara, TR). 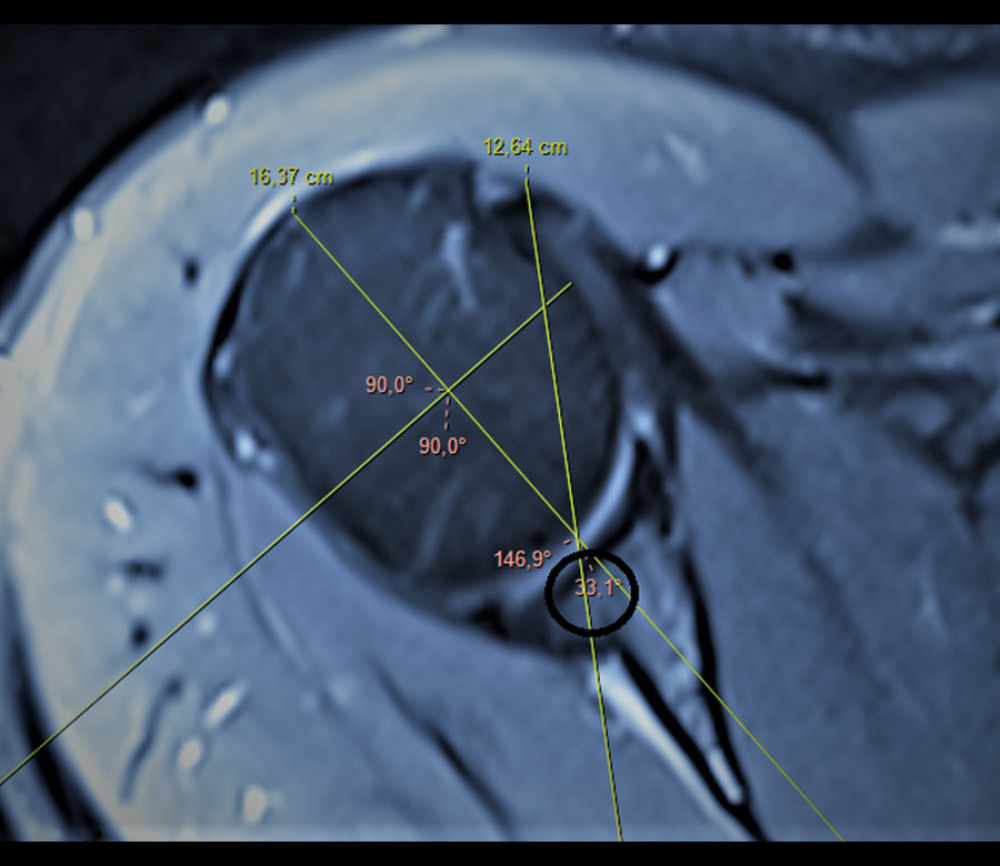 Figure 5. Lesser tuberosity angle. The angle between the vertical line that equally divides the line connecting the anterior and posterior cartilage of the humeral head and the most prominent part of the lesser tuberosity is measured (circle; axial T2-weighted magnetic resonance imaging section). (Fonet Dicom Viewer, v4.1, Fonet Bilgi Teknolojileri A.Ş., Gölbaşı, Ankara, TR).
Figure 5. Lesser tuberosity angle. The angle between the vertical line that equally divides the line connecting the anterior and posterior cartilage of the humeral head and the most prominent part of the lesser tuberosity is measured (circle; axial T2-weighted magnetic resonance imaging section). (Fonet Dicom Viewer, v4.1, Fonet Bilgi Teknolojileri A.Ş., Gölbaşı, Ankara, TR). 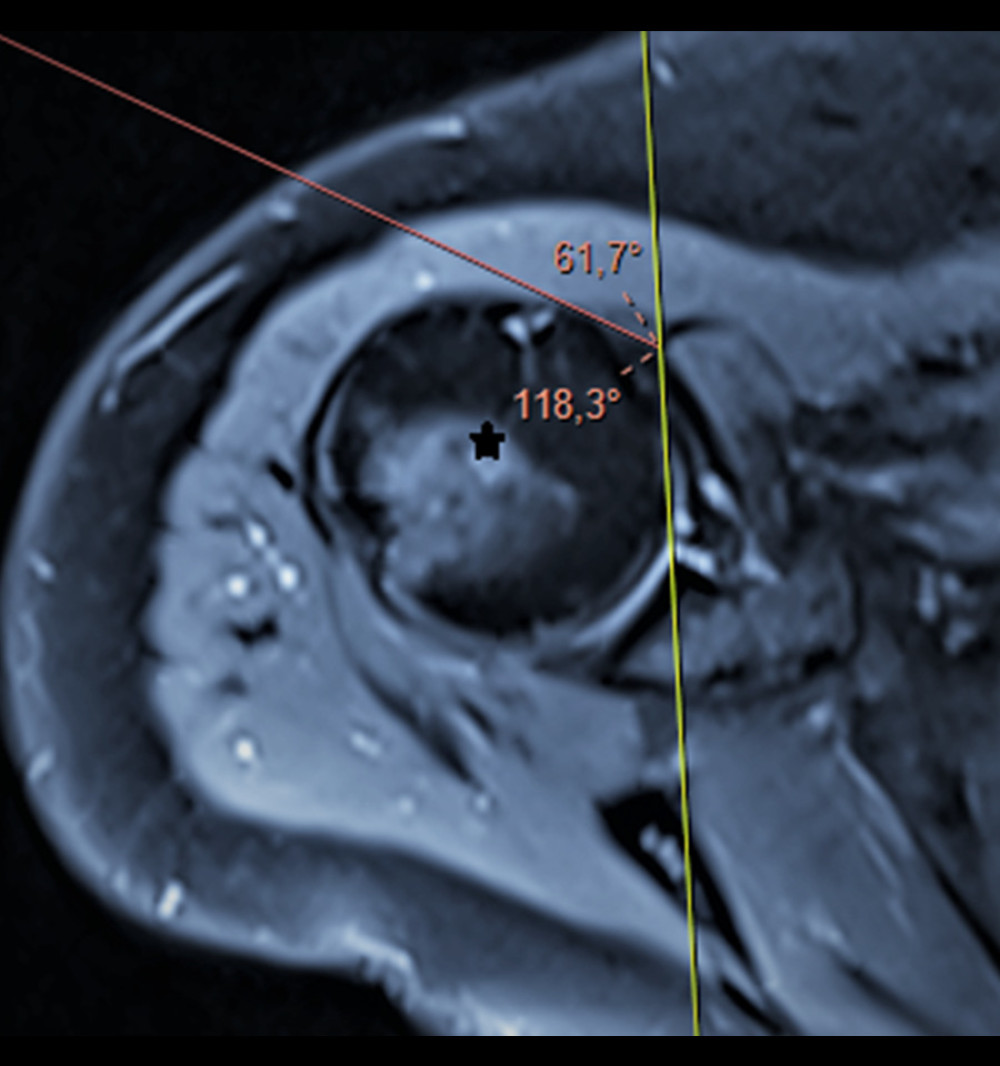 Figure 3. Coraco-humeral angle. It is measured as the angle between lines drawn tangentially from the tip of the coracoid process to the medial and lateral aspects of the humeral head (asterisk; axial T2-weighted magnetic resonance imaging section). (Fonet Dicom Viewer, v4.1, Fonet Bilgi Teknolojileri A.Ş., Gölbaşı, Ankara, TR).
Figure 3. Coraco-humeral angle. It is measured as the angle between lines drawn tangentially from the tip of the coracoid process to the medial and lateral aspects of the humeral head (asterisk; axial T2-weighted magnetic resonance imaging section). (Fonet Dicom Viewer, v4.1, Fonet Bilgi Teknolojileri A.Ş., Gölbaşı, Ankara, TR). 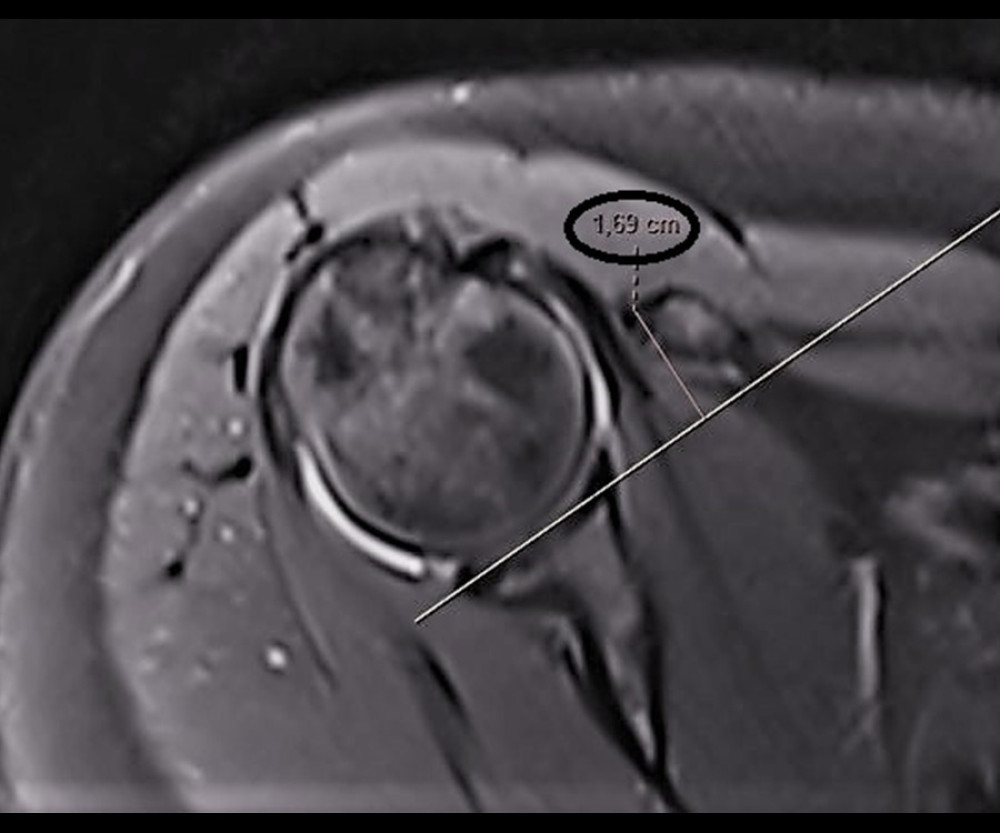 Figure 4. Coracoid overlap. The distance between the most distal part of the coracoid process and the glenoid is measured (circle; axial T2-weighted magnetic resonance imaging section). (Fonet Dicom Viewer, v4.1, Fonet Bilgi Teknolojileri A.Ş., Gölbaşı, Ankara, TR).CHD – coraco-humeral distance; CHA – coracohumeral angle; CGA – coraco-glenoid angle; CO – coracoid overlap; CBGA – coracoid-body glenoid angle; CTGA – coracoid tip-glenoid angle; CTBA – coracoid tip-body angle; LTA – lesser tuberosity angle; LTH – lesser tuberosity height; CSA – coraco-scapular angle; CA – coracoid angle; CI – confidence interval; agr – agreement.
Figure 4. Coracoid overlap. The distance between the most distal part of the coracoid process and the glenoid is measured (circle; axial T2-weighted magnetic resonance imaging section). (Fonet Dicom Viewer, v4.1, Fonet Bilgi Teknolojileri A.Ş., Gölbaşı, Ankara, TR).CHD – coraco-humeral distance; CHA – coracohumeral angle; CGA – coraco-glenoid angle; CO – coracoid overlap; CBGA – coracoid-body glenoid angle; CTGA – coracoid tip-glenoid angle; CTBA – coracoid tip-body angle; LTA – lesser tuberosity angle; LTH – lesser tuberosity height; CSA – coraco-scapular angle; CA – coracoid angle; CI – confidence interval; agr – agreement. Tables
Table 1. Demographic data and accompanying rotator cuff tear.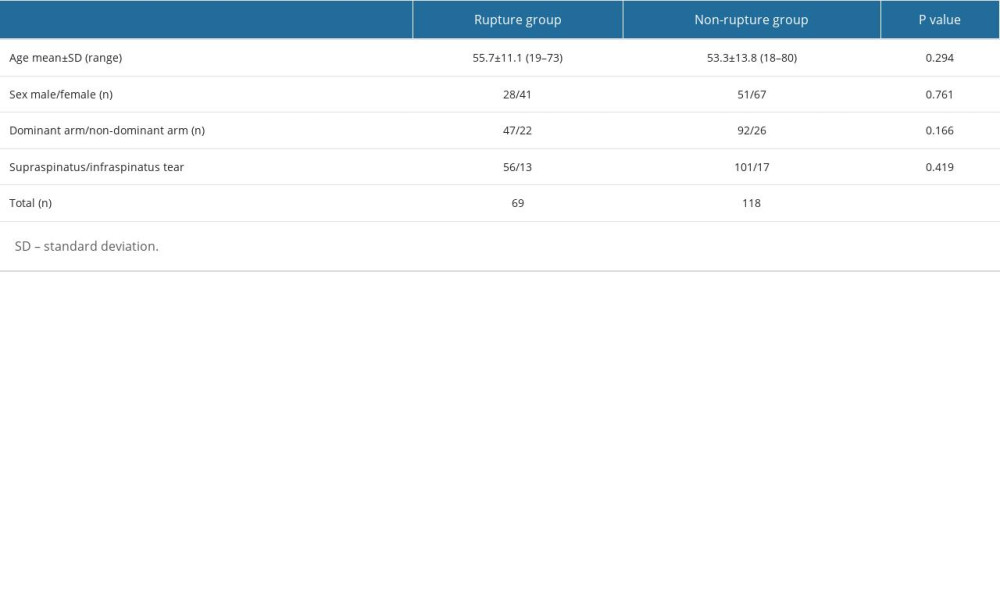 Table 2. The relationship of coracoid type* assessment with arthroscopic correlated subscapularis rupture.
Table 2. The relationship of coracoid type* assessment with arthroscopic correlated subscapularis rupture.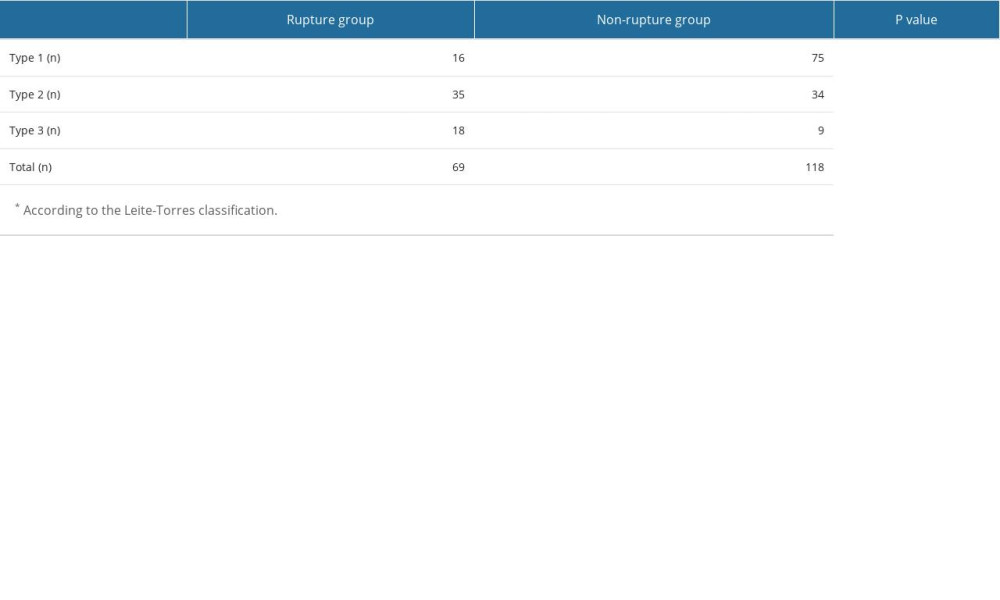 Table 3. Comparison of measured parameters in the 2 groups (rupture and non-rupture).
Table 3. Comparison of measured parameters in the 2 groups (rupture and non-rupture).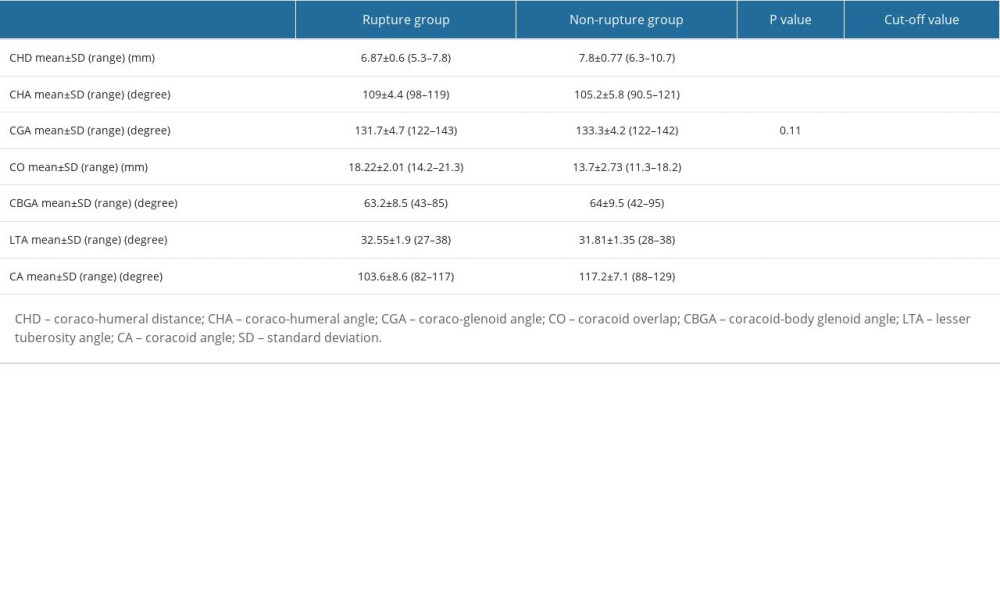 Table 4. Inter-observer reliability values.
Table 4. Inter-observer reliability values.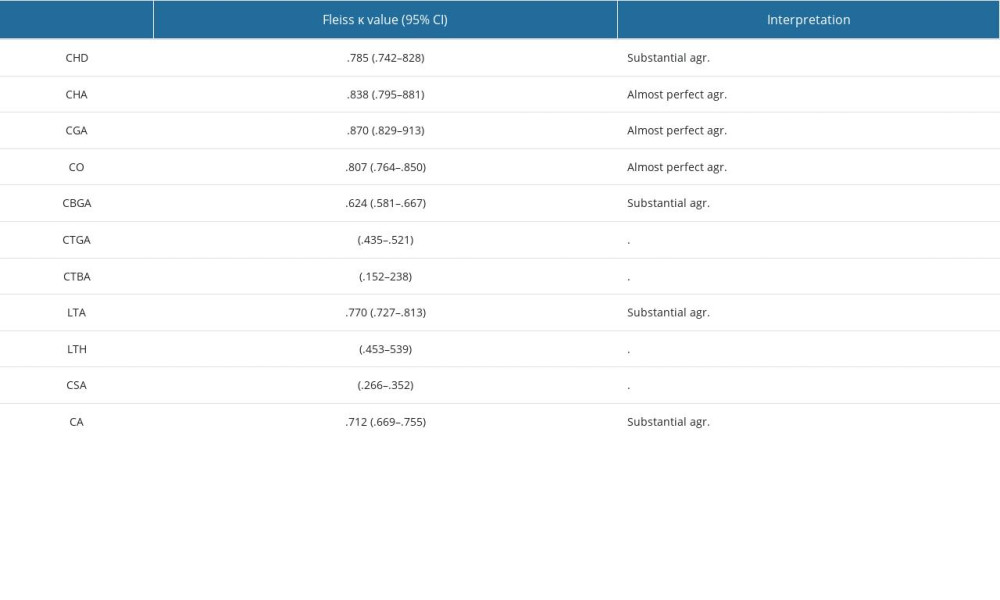
References
1. Malavolta EA, Assunção JH, Gracitelli MEC, Accuracy of magnetic resonance imaging (MRI) for subscapularis tear: A systematic review and meta-analysis of diagnostic studies: Arch Orthop Trauma Surg, 2019; 139(5); 659-67
2. Bigliani LU, Morrison DS, April EW, The morphology of the acromion and its relationship to rotator cuff tears: Orthop Trans, 1986; 10; 228
3. Gerber C, Terrier F, Ganz R, The role of the coracoid process in the chronic impingement syndrome: J Bone Joint Surg Br, 1985; 67; 703-8
4. Gerber C, Terrier F, Zehnder R, Ganz R, The subcoracoid space. An anatomic study: Clin Orthop Relat Res, 1987(215); 132-38
5. Lo IK, Burkhart SS, The etiology and assessment of subscapularis tendon tears: A case for subcoracoid impingement, the roller-wringer effect, and TUFF lesions of the subscapularis: Arthroscopy, 2003; 19(10); 1142-50
6. Richards DP, Burkhart SS, Campbell SE, Relation between narrowed coracohumeral distance and subscapularis tears: Arthroscopy, 2005; 21(10); 1223-28
7. Asal N, Şahan MH, Radiological variabilities in subcoracoid impingement: Coracoid morphology, coracohumeral distance, coracoglenoid angle, and coracohumeral angle: Med Sci Monit, 2018; 24; 8678-84
8. Leite MJ, Sá MC, Lopes MJ, Coracohumeral distance and coracoid overlap as predictors of subscapularis and long head of the biceps injuries: J Shoulder Elbow Surg, 2019; 28(9); 1723-27
9. Ashoor MMA, Hamed WM, Alfarsi HM, Relation between narrowed coracohumeral distance and subscapularis tears: The Egyptian Journal of Hospital Medicine, 2018; 70(7); 1164-68
10. Giaroli EL, Major NM, Lemley DE, Lee J, Coracohumeral interval imaging in subcoracoid impingement syndrome on MRI: Am J Roentgenol, 2006; 186(1); 242-46
11. Nair AV, Rao SN, Kumaran CK, Kochukunju BV, Clinico-radiological correlation of subcoracoid impingement with reduced coracohumeral interval and its relation to subscapularis tears in Indian patients: J Clin Diagn Res, 2016; 10(9); RC17-20
12. Dugarte AJ, Davis RJ, Lynch TS, Anatomic study of subcoracoid morphology in 418 shoulders: Potential implications for subcoracoid impingement: Orthop J Sports Med, 2017; 5(10); 2325967117731996
13. Watson AC, Jamieson RP, Mattin AC, Page RS, Magnetic resonance imaging based coracoid morphology and its associations with subscapularis tears: A new index: Shoulder Elbow, 2019; 11(1 Suppl); 52-58
14. Yu JF, Xie P, Liu KF, Identification of diagnostic magnetic resonance imaging findings in 47 shoulders with subcoracoid impingement syndrome by comparison with 100 normal shoulders: Med Sci Monit, 2022; 28; e936703
15. Leite MJ, Pinho AR, Sá MC, Coracoid morphology and humeral version as risk factors for subscapularis tears: J Shoulder Elbow Surg, 2020; 29(9); 1804-10
16. Torrens C, Alentorn-Geli E, Sanchez JF, Decreased axial coracoid inclination angle is associated with rotator cuff tears: J Orthop Surg (Hong Kong), 2017; 25(1); 2309499017690329
17. Soldado F, Kozin SH, The relationship between the coracoid and glenoid after brachial plexus birth palsy: J Pediatr Orthop, 2005; 25(5); 666-70
18. Seo JB, Kim SJ, Ham HJ, New predictors for subscapularis tear: Coraco-lesser tuberosity angle, lesser tuberosity angle, and lesser tuberosity height: Orthop Traumatol Surg Res, 2020; 106(1); 45-51
19. Kim BR, Lee J, Ahn JM, Predicting the clinically significant subscapularis tendon tear: Malposition and tear of the long head of the biceps tendon on shoulder magnetic resonance imaging: Acta Radiol, 2021; 62(12); 1648-56
20. Atinga A, Dwyer T, Theodoropoulos JS, Preoperative magnetic resonance imaging accurately detects the arthroscopic comma sign in subscapularis tears: Arthroscopy, 2021; 37(10); 3062-69
21. Bergin D, Parker L, Zoga A, Morrison W, Abnormalities on MRI of the subscapularis tendon in the presence of a full-thickness supraspinatus tendon tear: Am J Roentgenol, 2006; 186(2); 454-59
22. Wang Q, Zhao J, Zhou S, Quantitative MRI indicators and features for partial subscapularis tendon tears on conventional shoulder MRI: Insights Imaging 20, 2022; 13(1); 168
23. Malavolta EA, Assunção JH, Guglielmetti CL, Accuracy of preoperative MRI in the diagnosis of subscapularis tears: Arch Orthop Trauma Surg, 2016; 136(10); 1425-30
24. Ramadan LB, Baptista E, Souza FF, Diagnostic accuracy of preoperative magnetic resonance imaging for detecting subscapularis tendon tears: A diagnostic test study: Sao Paulo Med J, 2020; 138(4); 310-16
25. Lafosse L, Jost B, Reiland Y, Structural integrity and clinical outcomes after arthroscopic repair of isolated subscapularis tears: J Bone Joint Surg Am, 2007; 89(6); 1184-93
26. Tan V, Moore RS, Omarini L, Magnetic resonance imaging analysis of coracoid morphology and its relation to rotator cuff tears: Am J Orthop (Belle Mead NJ), 2002; 31(6); 329-33
27. Kucukciloglu Y, Aydın D, Relationship between radiological measurement of subcoracoid impingement and subscapularis tendon lesions: Clin Orthop Surg, 2022; 14(3); 441-49
28. Zhu S, Tan J, Wu D, Bilateral coracohumeral distance discrepancy is associated with subscapularis tear in rotator cuff rupture patients: Knee Surg Sports Traumatol Arthrosc, 2021; 29(12); 3936-42
Figures
Figure 1. Coracoid angle. It is measured as the angle between the long axes of the proximal and distal segments of the coracoid process in a T1-weighted oblique sagittal magnetic resonance imaging section (circle). (Fonet Dicom Viewer, v4.1, Fonet Bilgi Teknolojileri A.Ş., Gölbaşı, Ankara, TR).Figure 2. Coraco-humeral distance. It is measured as the shortest distance between the coracoid process and the tuberculum minus (axial T2-weighted magnetic resonance imaging section). (Fonet Dicom Viewer, v4.1, Fonet Bilgi Teknolojileri A.Ş., Gölbaşı, Ankara, TR).Figure 5. Lesser tuberosity angle. The angle between the vertical line that equally divides the line connecting the anterior and posterior cartilage of the humeral head and the most prominent part of the lesser tuberosity is measured (circle; axial T2-weighted magnetic resonance imaging section). (Fonet Dicom Viewer, v4.1, Fonet Bilgi Teknolojileri A.Ş., Gölbaşı, Ankara, TR).Figure 3. Coraco-humeral angle. It is measured as the angle between lines drawn tangentially from the tip of the coracoid process to the medial and lateral aspects of the humeral head (asterisk; axial T2-weighted magnetic resonance imaging section). (Fonet Dicom Viewer, v4.1, Fonet Bilgi Teknolojileri A.Ş., Gölbaşı, Ankara, TR).Figure 4. Coracoid overlap. The distance between the most distal part of the coracoid process and the glenoid is measured (circle; axial T2-weighted magnetic resonance imaging section). (Fonet Dicom Viewer, v4.1, Fonet Bilgi Teknolojileri A.Ş., Gölbaşı, Ankara, TR).CHD – coraco-humeral distance; CHA – coracohumeral angle; CGA – coraco-glenoid angle; CO – coracoid overlap; CBGA – coracoid-body glenoid angle; CTGA – coracoid tip-glenoid angle; CTBA – coracoid tip-body angle; LTA – lesser tuberosity angle; LTH – lesser tuberosity height; CSA – coraco-scapular angle; CA – coracoid angle; CI – confidence interval; agr – agreement. Tables
Table 1. Demographic data and accompanying rotator cuff tear.Table 2. The relationship of coracoid type* assessment with arthroscopic correlated subscapularis rupture.Table 3. Comparison of measured parameters in the 2 groups (rupture and non-rupture).Table 4. Inter-observer reliability values.Table 1. Demographic data and accompanying rotator cuff tear.Table 2. The relationship of coracoid type* assessment with arthroscopic correlated subscapularis rupture.Table 3. Comparison of measured parameters in the 2 groups (rupture and non-rupture).Table 4. Inter-observer reliability values. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387