11 September 2023: Review Articles
Neurological Complications of Regional Anesthesia: An Updated Review with Clinical Guidelines
Paweł Radkowski123ABCDF, Magdalena Fadrowska-SzleperDOI: 10.12659/MSM.940399
Med Sci Monit 2023; 29:e940399






Abstract
ABSTRACT: The main purpose of this article is to present the neurological complications of regional anesthesia. Our analysis may help clinicians determine when regional anesthesia can be administered safely and in which patients it needs additional precautions. Regional anesthesia has a major role in anesthesia practice. Here, we focus especially on the most common neurological complications: epidural hematoma, post-anesthesia headaches, and peripheral nerve function defect. We investigated risk factors of these states and propose ways of reducing the risks. This work is based on the available literature and the authors’ experience. The research process involved using relevant keywords in various electronic databases, resulting in the selection of 32 articles published between 1989 and 2022. This manuscript provides an overview and analysis of the existing literature related to neurological complications of regional anesthesia. We believe that our article provides up-to-date information on the most common regional anesthesia complications, emphasizing differences concerning children and pregnant women and provides important guidance for clinicians in preparing for and performing anesthesia.
Keywords: Anesthesia, Epidural, Anesthesia, Local, Anesthesia, Spinal, Postoperative Complications, Child, Female, Humans, Pregnancy, Anesthesia, Conduction, Anesthesiology, Databases, Factual, Headache, Risk Factors, Practice Guidelines as Topic
Background
Regional anesthesia is a widely used method for pain management during surgery and other medical procedures. However, it is not without its potential complications, particularly in the neurological realm. In recent years, there has been increasing interest in understanding the incidence, causes, and management of neurological complications associated with regional anesthesia. We discuss the most common complications of neuraxial anesthesia and peripheral nerve blocks in adults and children, and we emphasize differences occurring in obstetrics and pediatrics. The purpose of this article is to review the current literature on this topic, with a focus on the most common neurological complications, their mechanisms, and strategies for prevention and management. This review aims to provide an up-to-date overview of the field and to highlight areas in need of further research. It is intended to be a valuable resource for anesthesiologists, neurologists, and other healthcare professionals who manage patients undergoing regional anesthesia, as we believe reducing complications and taking better care of patients undergoing procedures that require anesthesia depends on cooperation among these specialists.
The work is based on the available literature and the author’s experience. The purpose of this study was to review the available literature on neurological complications after regional anesthesia. The search process involved using relevant keywords in various electronic databases, resulting in the selection of 32 articles published between 1989 and 2022. The MeSH tool was used during the preliminary stages and the search terms “neurological complications” and “regional anesthesia” were utilized. The final selection of articles was made after reviewing the titles and abstracts separately by 2 researchers. This article focuses on the clinical approach to the topic and aims to be useful for a variety of medical specialties. Hence, even though the topic is not new, our holistic approach and the inclusion of useful tables may make it a valuable resource for many doctors. We have paid considerable attention to both the latest publications and the fundamentals of anesthesiology. The main purpose of this article is to present the neurological complications of regional anesthesia. Our analysis may help clinicians determine when regional anesthesia can be administered safely and in which patients it needs additional precautions.
Neurological Complications After Neuraxial Anesthesia
Neurological defects are very rare but tragic complications of neuraxial anesthesia. Neurological defects occur via various mechanisms: vascular injuries, direct trauma, and infectious processes such as abscess. Several issues need to be discussed regarding neurological complications. Symptoms that resemble complications of anesthesia may be associated with perioperative procedures, surgical factors, iatrogenic injury, or nerve compression. In addition, pre-existing neurologic disease may become aggravated after surgical procedures, and resemble neurological complications of anesthesia. Sedation may also interfere with clinical evaluation, as it can mask early symptoms of complications. To diagnose neurological deficits early it is crucial to communicate to patients the importance of self-observation, as many patients presume postoperative symptoms are normal and do not report them to medical staff. Furthermore, because of postoperative immobilization and postoperative blur, the deficits often become recognizable many days after the operation, when a patient returns to normal activity. In the early postoperative time, neurologic examination cannot be done properly as there are many interfering factors, so the ability to recognize complications may be altered and results may be better with cooperation of the neurologist and anesthesiologist.
Most of the symptoms are transient and do not require major medical intervention, such as post-dural headaches [1]. Most neurological deficits are sensory-predominant. It is important to know which symptoms demand emergent imaging, consultation, and treatment.
Firstly, we discuss neurological damage that is a result of epidural hematoma. Fortunately, this complication is very rare, occurring in only 2 per 100 000 to 1 per 140 000–220 000 neuraxial procedures. Accordingly, the estimated incidence of spinal epidural hematoma is approximately 1 per 220 000 cases of spinal anesthesia and 1 per 150 000 cases of epidural anesthesia among patients who did not receive thromboprophylaxis [2]. It is especially important to diagnose it quickly, as the longer it takes to diagnose this condition, the more severe the neurological damage it can cause [3]. Early symptoms are vague sensory symptoms below the site of epidural hematoma, and flaccid paralysis of the lower extremities. Late complications are neurogenic bowel and bladder. There has been a reported case of paraplegia following spinal anesthesia [4].
Infectious complications such as meningitis, polyradiculopathy, and epidural abscess can also cause neurological defects. They are treatable, but tricky to diagnose and potentially devastating. All states concerning reduced immunity are risk factors, as well as diabetes. The first sign is pain, but because of the common use of analgesics after procedures, it is often masked. Fevers can occur, as well as elevated serologic inflammatory markers. Abscess presents with the most specific signs, such as sensory deficits, paraparesis, and, later, neurogenic bowel and bladder [5]. Meningitis potentially can present with seizures.
Vascular complications are potentially the most catastrophic, especially anterior spinal artery syndrome, which may be related to embolism, direct trauma, or vasoconstriction. An extreme drop in mean blood pressure can impair spinal blood circulation autoregulation, although watershed ischemia cases are reported, with rapid progression to paraplegia and tetraplegia, with spinal shock phase presenting with areflexia and flaccid tone.
Similar damage mechanisms can be involved when treating abscess after neuraxial anesthesia. It is important to know the risk factors for spinal epidural hematoma and spinal epidural abscess to improve the treatment and diagnostic process. Major risk factors are anticoagulation and bleeding diathesis. To avoid unnecessary risk of epidural hematoma, use of anticoagulants before the procedure should be conducted according to the latest recommendations.
Direct needle trauma is variable in prognosis and symptoms presented. Once it occurs, there is not much that can be done.
Neurological Complications After Peripheral Nerve Blocks
Peripheral nerve block is commonly used by anesthesiologists of various subspecialties, especially during orthopedic surgeries. It has many advantages over general surgery. It has been proven that it lowers the prevalence of postoperative pain and reduces the postoperative need for opioids and adverse effects of general anesthesia such as nausea and vomiting [6].
Risk factors for neurologic dysfunction after peripheral nerve block include pre-existing (but not clinical) neuropathy, hypothermia, hypovolemia, hypoxemia, hypotension, electrolyte imbalance, and even nutritional status.
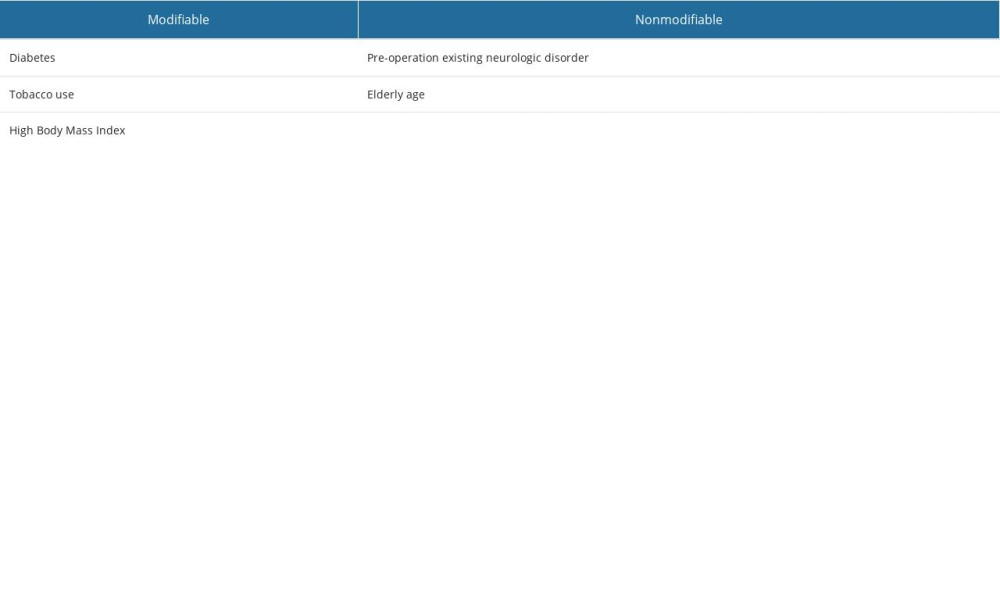
Most postoperative neurologic dysfunction resolves over time. There are many documented causes and mechanisms of peripheral nerve dysfunction occurring after nerve block. As Hewson et al [7] noted, many risk factors of nerve injury are patient-dependent, and some of them are modifiable, including pre-operative neurologic disorder, diabetes, tobacco use, high BMI, and older age.
Some of the damage observed after performing peripheral nerve block results from of positioning of patient’s limbs during the procedure [8]. It is sometimes hard to determine whether nerve injury is the result of anesthesia trauma or surgical trauma. There are signs that can alert anesthesiologists to neurological complications. Pain associated with the injection and paresthesia with needle placement can be symptoms of nerve injury. Other perioperative characteristics include prolonged tourniquet time and positioning/stretching and compression of nerves [9].
Mechanisms of nerve injury are similar to those occurring after neuraxial anesthesia, including direct trauma, hematoma, infections, and compartment syndrome, but when treating peripheral nerves, it is crucial to recognize active processes that can be treated, such as hematoma and infection. With a suspected active process, rapid diagnostic imaging should be performed.
If a patient’s sensory deficits are located away from distribution of the block, it may be assumed that the cause is nerve compression. Usually, the nerves compressed during surgical procedures are the ulnar nerve and peroneal nerve. Compression can also be caused by unnatural positioning of the patient’s extremities.
Interscalene brachial plexus block is especially associated with rare but severe complications such as diaphragmatic paresis, Horner’s syndrome, and dysphonia [10].
Many modern imaging techniques help lower the risk of damaging nerves during surgery.
Depending on the availability of particular methods, anesthesiologists should use them to lower the risk of unnecessary damage [11]. A common cause of neurological symptoms after surgery is inflammatory neuropathy. Autoimmune inflammatory response can be triggered by surgery or anesthesia and can develop hours to weeks after a stressor. About 90% of patients recover well. Weakness is usually multifocal, associated with severe pain (Table 1).
Neurological Complications After Neuraxial Anesthesia in Obstetrics
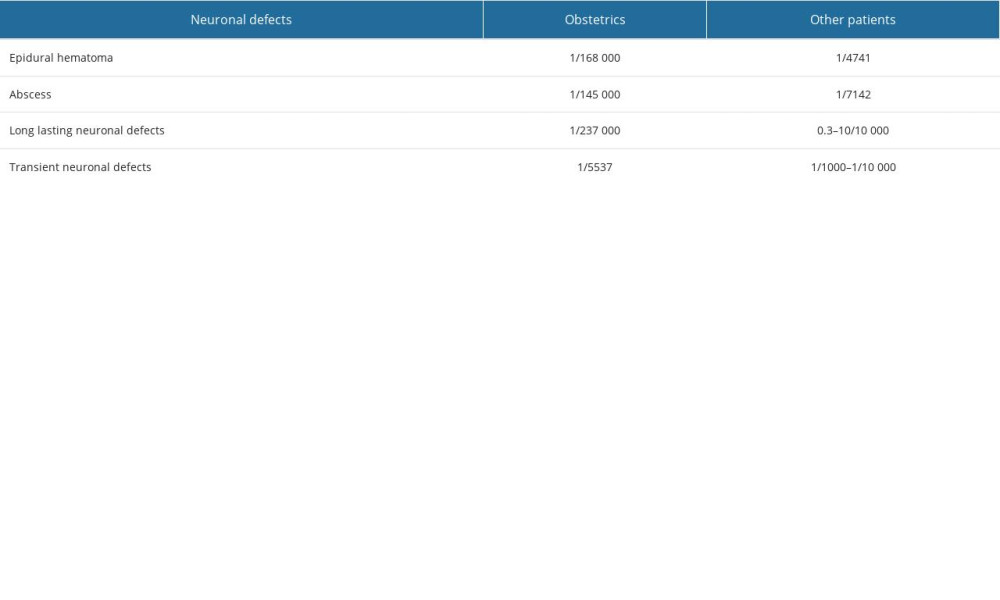
When treating pregnant woman, clinicians often have limited options. Spinal anesthesia is a method of choice during caesarian section due to being the safest option for the woman and fetus [12]. Moreover, being conscious during a procedure is why this method is also preferred by patients themselves. For these reasons, the decision to choose another type of anesthesia is not simple. However, complications due to spinal anesthesia can cause serious neurological complications [13]. Preeclampsia, absence, seizures, amniotic fluid embolism, pulmonary embolism, and acute cranial events are risk factors for neurological complications and are associated with caesarian section [14]. With the coagulation system being off balance, especially during the final period of pregnancy, special concern should be focused on vascular mechanisms of complications. While spinal cord ischemic syndromes are extremely rare, pregnant women during caesarian section may be at risk (Table 2).
Neurological Complications After Neuraxial Anesthesia in Pediatrics
Particularly for pediatric patients’ parents, neuraxial anesthesia may seem to be more traumatizing than general anesthesia. However, it is the responsibility of the doctor treating a pediatric patient to explain why it is actually a safer option. Although children are slightly more vulnerable to the toxicity of local anesthetics, they have enormously lower neurocognitive impact than anesthetics used during general anesthesia [15].
Postoperative apnea is a serious condition that can impair a child’s nervous system development, especially in preterm infants. In this group of patients, clinicians should prefer local anesthesia over general anesthesia.
Parents frequently assume that neuraxial anesthesia will be more traumatizing for their children, and it is the anesthesiologist’s responsibility to explain that the exact opposite is true. Historically, the risks of this procedure were believed to be high, but modern studies show that complications, especially neurological ones, are extremely rare [16].
The most common complication is post-dural puncture headache, but research shows it can be avoided by using atraumatic needles for dural puncture (25 or 27 G) [17]. Generally, the headache can be treated by a small dose of caffeine, and even when not treated, in contrast to adult patients, blood patch should be reserved for refractory cases.
Use of regional analgesia has been increasing as it has been repeatedly proven to be the safest way to provide anesthesia for children [18].
Caudal anesthesia is a frequently used and very safe technique [19]. It can be used in sub-umbilical procedures, including umbilical hernia. A retrospective study of 750 caudal blocks performed in children by Dalens et al showed a success rate of 96% [20], and Brown et al reported only a 0.69% rate of seizure [21].
Neurological Complications After Toxicity of Anesthetics
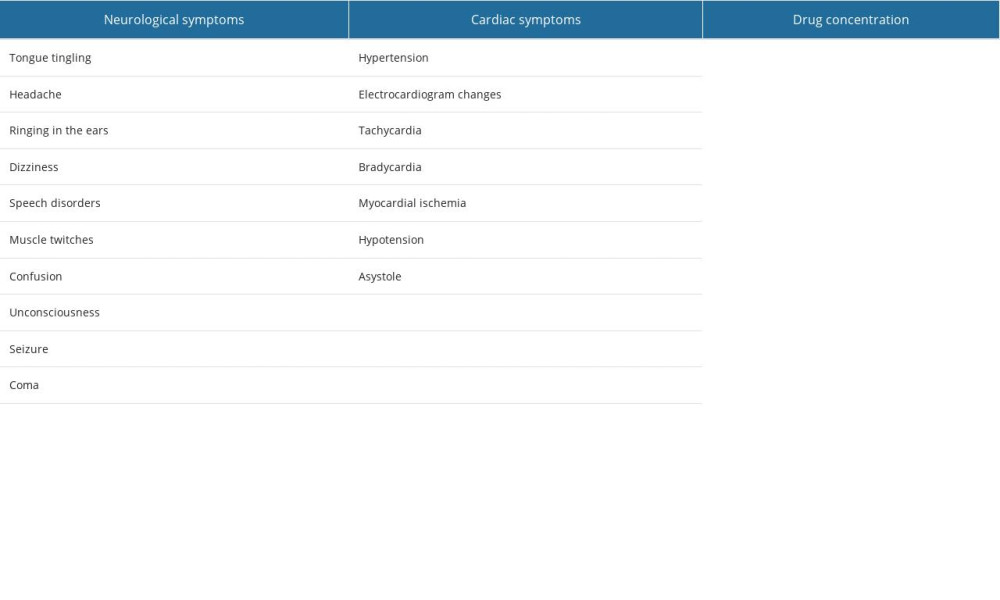
Pediatric patients are more vulnerable to the toxicity of anesthetics that adult patients, and this must be considered when performing local anesthesia in children [22]. Systemic absorption of local anesthetic can lead to neurological and cardiac complications that are potentially life threatening. As Neal et al point out, infants are a risk group [23]. The American Society of Regional Anesthesia and Pain Medicine (ASRA) created a checklist for the management of local anesthetic systemic toxicity (LAST). Consideration of lipid emulsion is recommended when observing the first signs of LAST [24]. Local anesthetic systemic toxicity is an extremely rare condition in children, with a reported incidence of 0.76 cases per 10 000 procedures [15]. Symptoms of LAST vary depending on drug uptake (Table 3).
Additional Findings
Nerve stimulation techniques have been recently used to decrease the likelihood of neurological problems, and studies have shown that use of nerve stimulation during peripheral nerve blocks can enhance the accuracy of needle positioning and reduce the risk of complications [22,25]. Consequently, nerve stimulation techniques have been included in protocols for the administration of peripheral nerve blocks [26,27].
There has been a heightened focus on the use of newer local anesthetics that have a lower risk of neurotoxicity than traditional anesthetics. For example, research has indicated that ropivacaine has a lower risk of neurotoxicity than bupivacaine [28,29]. Another recent study found that levobupivacaine, a stereoisomer of bupivacaine, has a lower risk of neurotoxicity compared to bupivacaine in peripheral nerve blocks [26].
Additionally, research is ongoing on the role of multimodal analgesia in decreasing the risk of neurological complications. These studies suggest that the addition of nonsteroidal anti-inflammatory drugs and gabapentinoids can reduce the amount of local anesthetic needed and thus reduce the risk of neurotoxicity [25,26]. These findings underscore the importance of ongoing research in this field and the need for continued education and training in the safe and effective use of regional anesthesia.
Recent research has shown the heightened risk of peripheral nerve damage when ultrasound guidance is used for regional anesthesia, with several studies indicating a higher incidence of peripheral nerve injury with ultrasound-guided techniques compared to other approaches. Consequently, it is necessary to emphasize the value of proper technique and training when using ultrasound-guided regional anesthesia.
Conclusions
It is important to select the correct anesthetic for every clinical situation. It has been reported that transient neurotic symptoms (TNS) syndrome is associated with lidocaine use [30]. It is especially important to recognize the importance of ultrasound imaging when performing local anesthesia [28]. According to numerous studies, use of ultrasound while performing local anesthesia significantly lowers the incidence of complications. The correlation is even stronger in pediatric patients [17]. Any suspected spinal cord dysfunction in a patient who underwent neuraxial anesthesia requires neuroimaging. In the pediatric population, complications are particularly rare.
Future Directions
Among imaging modalities, magnetic resonance is the method of choice if it is available. Peripheral nerve injury diagnosis should also include CT and USG to exclude acute conditions requiring surgical intervention [26,31,32]. Further steps, if available, should include some sort of electrophysiology nerve diagnosis. Two significantly different groups of patients should be specified: pregnant woman and pediatric patients. In pregnant woman, clinicians should be especially alert to and monitor potential neurological complications after local anesthesia.
References
1. Liu H, Brown M, Sun L, Complications and liability related to regional and neuraxial anesthesia: Best Pract Res Clin Anaesthesiol, 2019; 33(4); 487-97
2. Horlocker TT, Vandermeuelen E, Kopp SL, Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Fourth Edition): Reg Anesth Pain Med, 2018; 43(3); 263-309
3. Brull R, McCartney CJ, Chan VW, El-Beheiry H, Neurological complications after regional anesthesia: contemporary estimates of risk: Anesth Analg, 2007; 104(4); 965-74
4. Olivei MC, Tamanti P, Giachetti A, Transient paraplegia due to subarachnoid haemorrhage following spinal anaesthesia: Anesth Rep, 2020; 8(1); 40-43
5. Makito K, Mouri H, Matsui H, Spinal epidural hematoma and abscess after neuraxial anesthesia: A historical cohort study using the Japanese Diagnosis Procedure Combination database: Can J Anesth, 2021; 68(1); 42-52
6. Kettner SC, Willschke H, Marhofer P, Does regional anaesthesia really improve outcome?: Br J Anaesth, 2011; 107(Suppl 1); i90-95
7. Hewson DW, Bedforth NM, Hardman JG, Peripheral nerve injury arising in anaesthesia practice: Anaesthesia, 2018; 73; 51-60
8. Brull R, Hadzic A, Reina MA, Barrington MJ, Pathophysiology and etiology of nerve injury following peripheral nerve blockade: Reg Anesth Pain Med, 2015; 40(5); 479-90
9. Lam KK, Soneji N, Katzberg H, Incidence and etiology of postoperative neurological symptoms after peripheral nerve block: A retrospective cohort study: Reg Anesth Pain Med, 2020; 45(7); 495-504
10. Karina G, Victor P, Priya A, Incidence of vocal cord paresis following ultrasound-guided interscalene nerve block: An observational cohort study: Best Pract Res Clin Anaesthesiol, 2019; 33(4); 553-58
11. Sen S, Ge M, Prabhakar A, Recent technological advancements in regional anesthesia: Best Pract Res Clin Anaesthesiol, 2019; 33(4); 499-505
12. Kayaalti SIntermittent loss of consciousness during cesarean section under spinal anesthesia: A case report: Braz J Anesthesiol, 2019; 69(6); 631-34 [in Portuguese]
13. Kim HJ, Choi SH, Kwon H, Spinal versus general anesthesia for cesarean delivery in pregnant women with moyamoya disease: A retrospective observational study: Anesth Analg, 2022; 135(3); 617-24
14. Dontukurthy S, Tobias JD, Update on local anesthetic toxicity, prevention and treatment during regional anesthesia in infants and children: J Pediatr Pharmacol Ther, 2021; 26(5); 445-54
15. Walker BJ, Long JB, Sathyamoorthy M, Complications in pediatric regional anesthesia an analysis of more than 100,000 blocks from the pediatric regional anesthesia network: Anesthesiology, 2018; 129(4); 721-32
16. Greaney D, Everett T, Paediatric regional anaesthesia: Updates in central neuraxial techniques and thoracic and abdominal blocks: BJA Educ, 2019; 19(4); 126-34
17. Kaye AD, Green JB, Davidson KS, Newer nerve blocks in pediatric surgery: Best Pract Res Clin Anaesthesiol, 2019; 33(4); 447-63
18. Wiegele M, Marhofer P, Lönnqvist PA, Caudal epidural blocks in paediatric patients: A review and practical considerations: Br J Anaesth, 2019; 122(4); 509-17
19. Sanghvi C, Dua A, Caudal anesthesia: StatPearls [Internet] Dec 2, 2022, Treasure Island (FL), StatPearls Publishing
20. Dalens B, Hasnaoui A, Caudal anesthesia in pediatric surgery: Success rate and adverse effects in 750 consecutive patients: Anesth Analg, 1989; 68(2); 83-89
21. Brown DL, Ransom DM, Hall JA, Leicht CH, Regional anesthesia and local anesthetic-induced systemic toxicity: Seizure frequency and accompanying cardiovascular changes: Anesth Analg, 1995; 81(2); 321-28
22. Winnie AP, Mechanisms of nerve injury during peripheral nerve block: Anesthesiology, 2002; 97(4); 1082-88
23. Neal JM, Woodward CM, Harrison TK, The American Society of Regional Anesthesia and Pain Medicine Checklist for Managing Local Anesthetic Systemic Toxicity: 2017 Version: Reg Anesth Pain Med, 2018; 43(2); 150-53
24. Yurgil JL, Hulsopple CD, Leggit JC, Nerve blocks: Part I. Upper extremity: Am Fam Physician, 2020; 101(11); 654-64
25. Suresh S, Ganesh A, Suresh S, Incidence of spinal cord injury following spinal anesthesia: A systematic review of the literature: Anesthesiology, 2008; 109(4); 741-47
26. Rigg JR, Mulroy MF, Levobupivacaine neurotoxicity in peripheral nerve blockade: Br J Anaesth, 2017; 118(5); 541-48
27. Hadzic A, Williams BA, Karaca E, Ultrasound-guided peripheral nerve blocks: A review of the literature: Anesthesiology, 2010; 113(4); 816-29
28. Wong K, Chan L, Chan J, Ropivacaine versus bupivacaine for peripheral nerve blocks: A systematic review and meta-analysis: Anaesthesia, 2016; 71(4); 440-49
29. Koo CH, Shin HJ, Han SH, Ryu JH, Lidocaine vs. other local anesthetics in the development of transient neurologic symptoms (TNS) following spinal anesthesia: A meta-analysis of randomized controlled trials: J Clin Med, 2020; 9(2); 493
30. Liguori GA, Keats TE, Rosow CE, Incidence of neurologic complications from peripheral nerve blocks: A systematic review: Anesth Analg, 2011; 112(4); 1015-22
31. Rigg JR, Mulroy MF, Ultrasound-guided peripheral nerve blocks in the upper limb: Br J Anaesth, 2018; 121(3); 595-605
32. Novitch M, Prabhakar A, Siddaiah H, Point of care ultrasound for the clinical anesthesiologist: Best Pract Res Clin Anaesthesiol, 2019; 33(4); 433-46
In Press
18 Apr 2024 : Clinical Research
Comparative Analysis of Open and Closed Sphincterotomy for the Treatment of Chronic Anal Fissure: Safety an...Med Sci Monit In Press; DOI: 10.12659/MSM.944127
08 Mar 2024 : Laboratory Research
Evaluation of Retentive Strength of 50 Endodontically-Treated Single-Rooted Mandibular Second Premolars Res...Med Sci Monit In Press; DOI: 10.12659/MSM.944110
11 Mar 2024 : Clinical Research
Comparison of Effects of Sugammadex and Neostigmine on Postoperative Neuromuscular Blockade Recovery in Pat...Med Sci Monit In Press; DOI: 10.12659/MSM.942773
12 Mar 2024 : Clinical Research
Comparing Neuromuscular Blockade Measurement Between Upper Arm (TOF Cuff®) and Eyelid (TOF Scan®) Using Miv...Med Sci Monit In Press; DOI: 10.12659/MSM.943630
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952