29 June 2023: Database Analysis
Unlocking Endocrown Restoration Expertise Among Dentists: Insights from a Multi-Center Cross-Sectional Study
Mohammed M. Al Moaleem1ACDE*, Nasser M. Al Ahmari2DFG, Saeed M. Alqahtani2BEG, Thrya S. Gadah2DFG, Amal K. Jumaymi3BG, Mansoor Shariff2ACF, Amal S. Shaiban4DG, Wafa H. Alaajam4BDG, Bandar M.A. Al Makramani1CEF, Masood A.N. Depsh5BG, Fayez Y. Almalki5BG, Nasser A. Koreri5BGDOI: 10.12659/MSM.940573
Med Sci Monit 2023; 29:e940573






Abstract
BACKGROUND: This study, employing an online questionnaire, aimed to assess and contrast the awareness, knowledge, and perceptions of dentists in Saudi Arabia (SA) regarding endocrowns (EC) as post-endodontic restorations with those of dentists educated in various other countries.
MATERIAL AND METHODS: We conducted a cross-sectional survey among dental interns and practicing dentists in government facilities, private dental centers, and dental colleges in SA, including participants of diverse nationalities. We disseminated validated, closed-ended questionnaires through WhatsApp via Google Forms. The Chi-square test was applied to assess associations between categorical variables, with a P-value of ≤0.05 indicating statistical significance.
RESULTS: The majority of participants (61.2%) indicated that EC restorations are best suited for molar teeth. Furthermore, 69.6% asserted that the primary objective of employing EC is to accomplish minimally invasive preparations while preserving the existing tooth structure. Among the responses, 68.3% pinpointed debonding of ECs as a significant cause of failure. Notably, substantial differences were observed in responses concerning the knowledge or practice of EC across various factors such as gender, educational attainment, country of graduation, and workplace.
CONCLUSIONS: The findings reveal a comparatively low adoption of ECs among the participants, irrespective of experience or country of education. This underscores the need for incorporating ECs into dental curricula through theoretical and clinical discussions or considering them as a subject for post-graduate continuing education programs.
Keywords: Endodontics, Surveys and Questionnaires, Humans, Cross-Sectional Studies, Educational Status, Curriculum, Molar, Dentists
Background
The management of endodontically treated teeth (ETT) from the perspective of restorative care is a contentious topic as retention in such teeth is typically weakened. In order to treat these endodontically treated molars, post-and-core followed by metal or ceramic crowns have historically been the preferred gold standard restorative materials [1]. Post-and-core crown is a dental prosthesis for such ETT teeth, and it is usually completed by implanting a metal [2] or a fiber-reinforced composite [3] post-and-core into the root canal. However, with technological advancement, a macro-retentive design like a post is no longer necessary for the restoration of severely damaged teeth and this paradigm changes towards post-less restorations by using the pulp chamber as an extension has been made possible by adhesive techniques, which integrate the crown and core into a single monobloc [4]. This Monoblock approach, which served as the predecessor of endocrown (EC) was introduced by Pissis in 1995 and was used for the first time by Bindl and Mormann in 1999 [1]. In 2018, Tzimas et al described ECs as indirect monoblock restorations that rely on the pulp chamber of endodontically treated teeth (ETT) for retention and is made up of a pulp chamber, a circular butt-joint edge, and a central retention cavity [5]. The EC approach is indicated mainly when there is an extreme dental coronal loss and restricted interproximal distance. Additionally, ECs have shown advantages over conventional crowns in terms of application, less preparation and working time, and cost [6]. In teeth with short, destroyed, dilacerated, or narrow and calcified roots, ECs have become a viable restorative option [7,8] by providing a more favorable distribution of masticatory stresses and are more practical, conservative, and aesthetically pleasing [9]. This results in macromechanical retention (given by the pulpal walls) and microretention (by utilizing adhesive cementation) thereby preserves and protects the remaining tooth structure by reducing fracture resistance [10].
Also, there is a growing consensus that single, all-ceramic ECs with excellent mechanical qualities and high biocompatibility should be produced thanks to advancements in ceramic technology, particularly dental CAD/CAM systems [11,12]. These advancements in CAD/CAM technology, which offers accuracy, esthetics, and less time-consuming restorative procedures, has opened up new possibilities in material processing and tooth restoration [4] as the anatomic contour and surface textures of the ECs created using the CAD/CAM approach are superior. Thus, ECs fabricated using CAD/CAM and pressable ceramic technology can be considered as a reliable option for the restoration of moderately mutilated endodontically treated posterior teeth [13].
Despite the rising popularity of EC restorations among dental practitioners, the question that remains is whether dental professionals should consider utilizing EC instead of conventional procedures with intra-radicular posts. Most studies on endodontic crowns for teeth showed outcomes that were similar to or slightly superior to other conventional procedures (ETT). Several in vitro studies also examined how well the EC performs in comparison to conventional post retention crowns [9,14,15]. A study by Rasidi et al was also carried out in India in 2021 to evaluate dental professionals’ awareness, knowledge, and opinions regarding the use of EC as a postendodontic care strategy demonstrating an appropriate level of understanding and awareness of the use of EC as a post-endodontic care tool [16]. Another retrospective study was also carried out by Alotaiby et al in 2021 by dental students and residents in Riyadh, Saudi Arabia, and they concluded that EC is a conservative restoration method for endodontically treated teeth, particularly molars, with a very acceptable long-term survival rate and good biomechanical and functional efficiency [10]. Another study, by Soliman et al in 2021, was conducted amongst dentists in SA to evaluate post-core-crown restoration [17].
However, to the best of our knowledge, no international studies have been conducted to evaluate the knowledge and practice of ECs. To satisfy the patient’s demands and expectations with long-term restorative success, dentists should be knowledgeable about every possible dental treatment option. Thus, this web-based cross-sectional survey was conducted to evaluate the level of awareness, state of knowledge, and opinions towards EC as post-endodontic restoration among Saudi Arabia (SA) dentists and to compare their knowledge with some dentists who graduated from other countries.
Material and Methods
STUDY SETTING:
A cross-sectional, web-based questionnaire study was conducted amongst interns or graduated dentists practicing in government set-ups, private dental centers, and dental colleges from (SA) and different nationalities (dentists graduated from other countries) through an e-survey using Google Forms between December 2022 and January 2023.
STUDY POPULATION AND SAMPLING TECHNIQUE:
Snowball sampling technique was used to select the peers from SA and other countries among different groups. Sample size was calculated using G Power 3.1.9.4 at 95% confidence interval where α=0.05, (1−β)=80% and effect size=0.2. A total of 580 sample size was calculated.
STUDY TOOLS AND DATA COLLECTION:
The 18-item closed questionnaire was framed in accordance with the 2021 study by Soliman et al, with some modifications [17]. Lawshe’s methods [19] were used for content validity using judgments from a panel of 10 subjects matter experts (SME’s). The reliability was also established by test-retest among 20 volunteers of similar populations. The kappa value was 0.9, which indicated high reliability. This was followed by pilot testing among 10 volunteers who were asked to answer the questionnaire and provide feedback on content, clarity, and brevity of the questionnaire.
Check boxes were provided, and participants had to click on any one option for each question. Care was taken that one person could answer the questionnaire only once and all questions were mandatory. The responses were directly recorded through Google Forms. Since this was an e-survey, the informed consent was included in the Google form, and they were sent through WhatsApp.
QUESTIONNAIRE PARTS:
An English version of a web-based self-administrated questionnaire divided into 3 parts was distributed. The questionnaire consisted of a brief explanation of the purpose of the study, method of data collection, and close-ended questions. The first part of the questionnaire included questions regarding socio-demographic characteristics of the participants. The second part of the questionnaire consisted of 11 questions in relation to general knowledge of EC. The third part of the questionnaire consisted of 7 questions in relation to general practicing of EC and dental practicians. The responses were completely anonymous to ensure confidentiality.
DATA ANALYSIS:
Data were analyzed using statistical software R, version 4.2.2 (R Foundation for Statistical Computing) and Microsoft Excel. Categorical variables were represented by frequency and percentages. Chi-square test was used check the association between categorical variables. P-value less than or equal to 0.05 indicates statistical significance.
Results
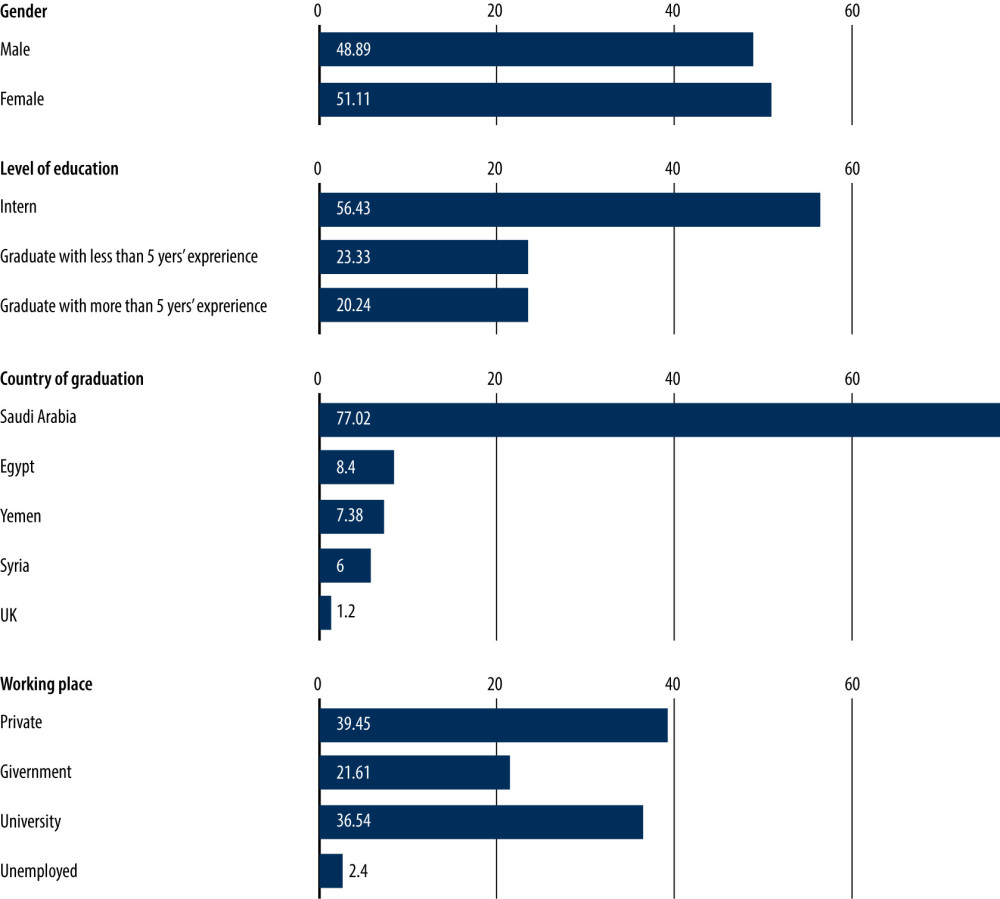
A total of 583 participants were included in the survey. Among them, 51.11% were females and 48.89% were males; 56.43% of the participants were interns, 23.33% of the participants being graduated with less than 5 years of experience; 20.24% of the participants graduated with more than 5 years of experience; 50% of participants graduated from Saudi Arabia (SA); and 39.45% were working in the private sector and 21.61% were from the government sector (Figure 1).
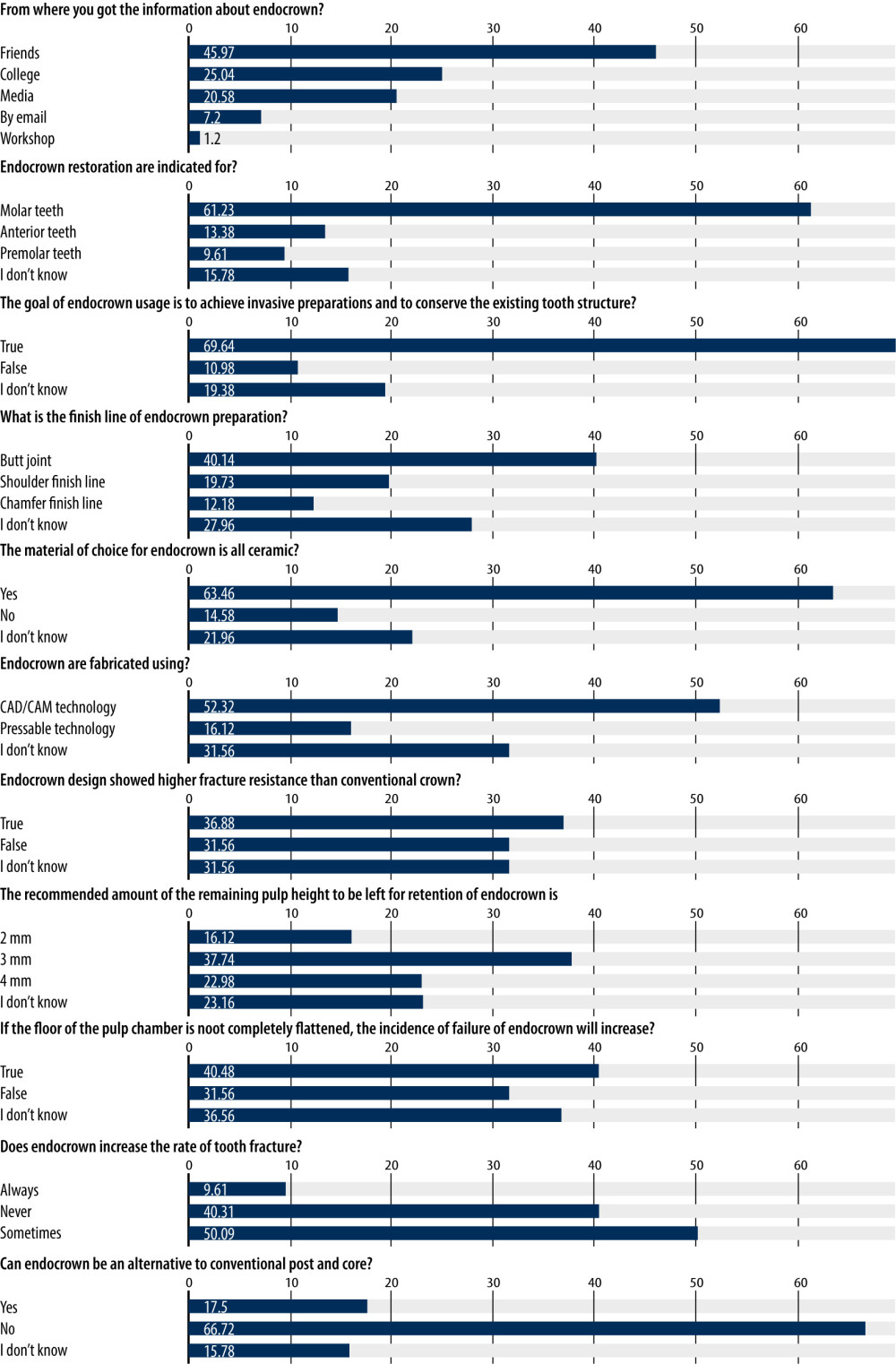
On asking the participants about the information on EC, 45.97% stated that they were informed about EC through friends, and 61.23% of the participants stated that EC restorations are indicated for molar teeth. The goal of EC usage is to achieve minimally invasive preparations and to conserve the existing tooth structure as suggested by 69.64% of the participants; 40.14% of the participants also stated that the finish line of EC preparation is butt joint; and 63.46% of the participants answered that the material of choice for EC is all ceramic. Almost 52.32% stated that ECs are fabricated using CAD/CAM technology and 36.88% indicated it was true that EC design showed higher fracture resistance than conventional crowns. The recommended amount of the remaining pulp chamber height to be left for retention of EC is 3 mm, which was stated by 37.74% of the participants. Additionally, 40.48% participants also stated that if the floor of the pulp chamber is not completely flattened, the incidence of failure of ECs will increase; 50.09% mentioned that EC sometimes increases the rate of tooth fracture and 66.72% of participants answered that EC was an alternative to conventional post-and-core (Figure 2).
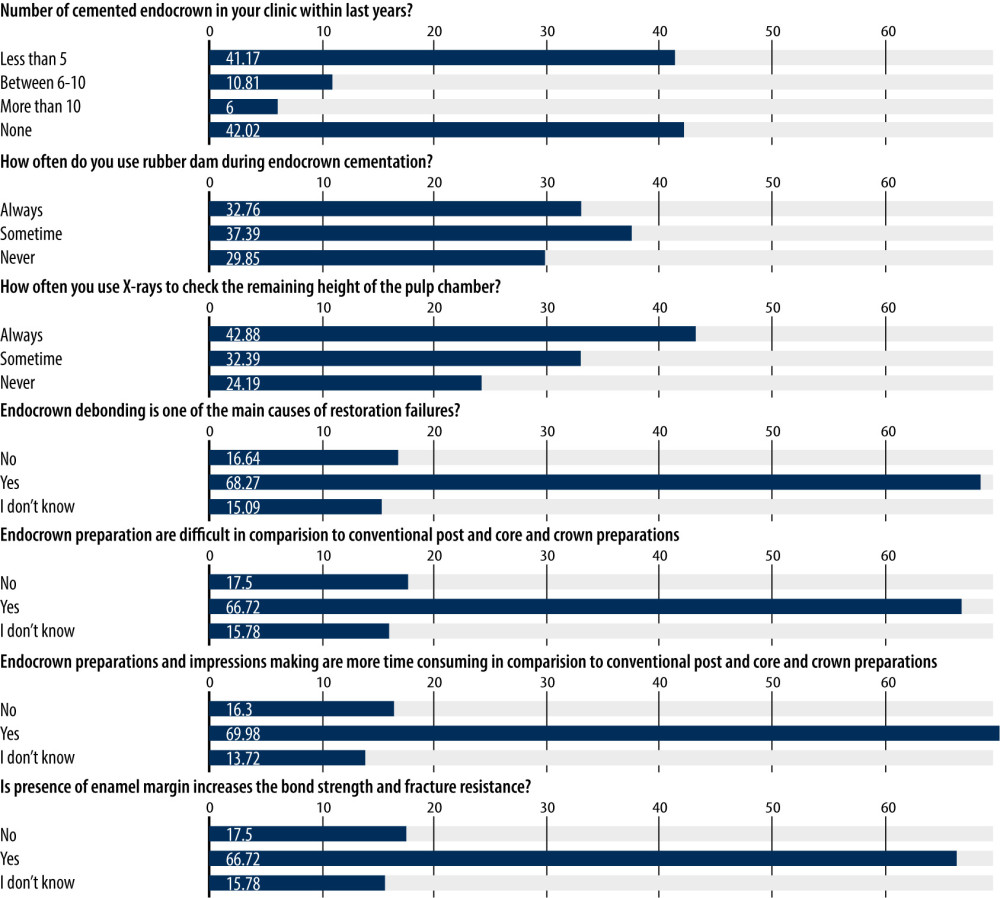
On questioning about EC practices in their clinics, only 41.17% of participants had performed cementation of EC in their clinic in the past years. Also, 37.39% of participants sometimes use rubber dams during EC cementation, and 42.88% of participants used X-rays to check the remaining height of the pulp chamber. When asked about the cause of restoration failures, 68.27% of the participants answered ECs debonding as one of the main cause of restoration failures and 66.72% of the participants stated that preparing ECs is more difficult than conventional post-and-core and crown preparations, and 69.98% of the participants stated that EC preparations and making impressions are more time-consuming than conventional post-and-core and crown preparations (Figure 3).
Using chi-square test alone and chi-square test with Monte Carlo simulation, there was a significant association (p<0.05) of knowledge and practice with the parameters such as gender, level of education, country of graduation, and working place of the participants (Tables 1, 2).
Discussion
The adoption of EC in clinical practice recently provided several benefits over post-core, which has been considered as a gold standard procedure in restoring ETT [20]. EC aims to preserve the remaining tooth structure available for bonding while maintaining the biomechanical integrity of ETT-compromised structures. ECs offer greater mechanical characteristics, minimum tooth structure loss, fewer clinical processes, reduced costs, and better esthetics [1,21–23]. Thus, we conducted this web-based cross-sectional survey to comprehensively and objectively evaluate the level of awareness, state of knowledge, and opinions towards EC as post-endodontic restoration among SA dentists and to compare their knowledge with some dentists who graduated from other countries. We used a Google questionnaire instead of a face-to-face questionnaire as we wanted to collect data from different nationalities and an e-survey was most suitable.
The samples included participants from SA and other countries who had different levels of knowledge and experience. Duration and language of teaching in SA for under graduation is 6 years study with an additional 1 year of compulsory internship, whereas in other countries it is only 5 years of study and a 1-year internship. Additionally, the language of teaching in SA is primarily English because of high number of Western staff members, while in other countries staff members teach in the local language only. Thus, economic status plays a significant role for offering payment for this type of costly treatment and this could be the reason for less knowledge and practice regarding EC usage among dental practitioners in SA. Based on the current study findings, they still employ traditional techniques, but the interns were the most enthusiastic about using it in clinical settings compared to dentists with experience of less and more than 5 years.
A successful and primarily minimally invasive EC prostheses can reduce the frequency of post-placement failures [11]. EC restorations have fewer interfaces in the restorative system [24], needless ETT preparation, and increased durability of the tooth structure [25–27]. In the present study assessing dental practitioners’ knowledge, most (69.64%) stated that the goal of EC usage is to achieve minimally invasive preparations and to conserve the existing tooth structure. The interns found this to be true the most and it could be attributed to their recent gain of knowledge from college.
The materials used for EC are ceramics that have been strengthened with lithium disilicate, or monolithic zirconia. Lithium disilicate is the most preferred material for EC due to its high aesthetic value and adequate mechanical strength [25,27]. Resin composite materials have problems with microleakage [24], it is less durable and more prone to fracture than LDGC [28]. However, while using this approach, the preparatory design and material selection should be considered [23,29,30]. Similar findings were recording by Wahab et al, who investigated the preferences of Jordanian dentists for EC materials [22]. The present study demonstrated the related finding that most participants (63.46%) preferred LDGC as the material of choice for EC. the interns from SA had more recent knowledge of about these materials than other dentists.
In relation to bonding surface, a butt-joint margin or a flat EC displays more remaining tooth tissue and less bonding area than a 90-degree shoulder EC produces [11,31]. However, there is not much scientific data to support this suggestion. Additionally, increased consistent stress distributed over the cervical butt-joint and axial walls was seen in the butt-joint margin and 20° bevel margin [13,32] in comparisons with the shoulder margin. This might significantly increase the risks of restoration debonding [33]. In a survey conducted by Rasidi et al, the majority of dentists (80.83%) responded that butt-joint finish line was used during EC preparation [16]. This is because forces applied to this type will reduce the amount of pressure on the pulpal floor [1,8,9,34]. Thus, EC preparation consists of an equigingival butt-joint margin and a central retention cavity into the pulp chamber. This is comparable to the present results, as a majority (40.14%) stated butt-joint as the finish line of EC preparation, which was mostly correctly answered by interns.
In support of these results, Sedrez-Porto et al demonstrated that EC restorations outperformed conventional restorations and have high fracture strength and are preferred over other conventional restorations [9]. This is in line with other research that has established the validity of bonded ECs over conventional ones [11,16]. Abu-Nawareg et al revealed that ECs had greater fracture strength values than conventional crowns [35]. In our study, 36.88% of participants stated that EC design showed higher fracture resistance than conventional crowns. The rest mostly replied with “I don’t know”. This may be because there is less use of ECs in private clinics in SA and other countries compared to traditional crowns. Thus, EC designs demonstrated superior fracture resistance to conventional post-core-crown design [4,35].
According to a qualitative survey by Rasidi et al, most participants (82.5% dentists) believed that pressable ceramic technology can be used to construct an EC [16], but the present study results disagree with those findings. On questioning about ECs fabrication, interns from SA were more likely to answer that ECs are fabricated using CAD/CAM technology. Also, in the study by Rasidi et al, when asked to list the advantages of EC has over a traditional crown, the majority (56.67%) said it will take the least amount of time and 25.0% said it requires the least amount of preparation [16]. This was contrary to our study findings, as 66.72% of interns stated that preparing ECs is difficult in comparison to conventional post-core-crown preparations. Rasidi et al [16] found that only 27.5% of dental practitioners said that they have really used EC, whereas most (72.5%) said they had never used it before based on their training experience. This also supported our findings, as the majority of participants (42.02%) had never cemented ECs in their clinics. This is due to the fact that the most popular procedure is prefabricated post-core, followed by EC and cast post-core [17].
Moreover, in the present survey, the majority of interns (50.09%) claimed that EC can occasionally increase the rate of tooth fracture, and 66.72% mentioned EC as a substitute for traditional post-core. In addition, Ghoul et al showed that 90% of EC failures involved tooth fractures and displacement of the restoration on the side opposite the incidence of stress [36]. To ensure proper isolation, a rubber dam was used. The tooth surface was treated with etchant (37% phosphoric acid) for 15 seconds, after which it was thoroughly washed and allowed to dry naturally. Next, a bonding agent was applied to the tooth, and it was polymerized for 20 seconds under a curing light [37,38]. In this study also, very few participants (37.39%) sometimes used rubber dams during EC cementation.
Further, the difference in elasticity between tougher ceramics and softer dentine causes danger of debonding and root fracture with ceramics as they have different moduli of elasticity. Hence, choosing the right case is essential to the clinical success of ECs [16]. Debonding was cited as the main drawback of EC by the majority of dental professionals (80.0%) [14]. These findings were comparable to the present study findings (68.27%), as debonding of ECs is one of the main causes of restoration failure [39]. This has been proved to be an excellent strategy since the procedure is uncomplicated and facilitates the steps of impression taking and protects the periodontium. Moreover, ceramic has similar wear characteristics to actual teeth and has the benefits of biocompatibility. However, in our study the majority were interns (69.98%) who also stated that EC preparations and impression-making are more time-consuming in comparison to others. Deepak et al also conducted a cross-sectional survey to examine the dentists in Chennai’s level, concluding that ECs can be a viable alternative to severely damaged crowns [11]. The different answers found in this study indicated the need for clear protocol for diagnosis, indication, application, and cementation of EC. This was specifically true for the graduates with and without experience, as it depends on the constant use of the material and procedures in practice to be abreast of the knowledge associated with them. Additionally, future research is needed also about partially explored variables such as flexural [40] and compressive strengths [41] of EC. Further research is needed to test mechanical properties of these frameworks. Another reason for the above findings could be the economic status playing a role in offering payment for this type of costly treatment.
The limitation of this study firstly includes the sample size from a single population and a brief study period, which does not accurately reflect the size of the population, and the results of this retrospective study should be evaluated cautiously. Secondly, the FIFA world cup was conducted in Qatar during our study, contributing to a low response rate. Also, the duration of BDS programs in the included countries is different, which could be responsible for rigorous training. The language of teaching is mainly English in SA because of the high number of international staff as compared to the remaining countries, which have local staff members. This may also be responsible for disparities in understanding among the participants.
Conclusions
ECs can be used as an alternative to the traditional post-core for restoring root canal-treated teeth with severely damaged dental tissue. Overall knowledge and practice of ECs were low among all participants regardless of their experience and country of graduation. The above results with respect to dentists from SA highlight the fact that ECs must be included in the curricula for theory and clinicals. It should be considered as a topic for continuing education programs after graduation so that dentists can perform different treatment modalities to best suit the needs of patients.
References
1. Sevimli G, Cengiz S, Oruc MS, Endocrowns: Review: J Istanb Univ Fac Dent, 2015; 49(2); 57-63
2. Farid F, Mahgoli H, Hosseini A, Chiniforush N, Effect of eugenol-containing and resin endodontic sealers on retention of prefabricated metal posts cemented with zinc phosphate and resin cements: J Prosthodont Res, 2013; 57(4); 284-87
3. Scribante A, Vallittu PK, Özcan M, Fiber-reinforced composites for dental applications: Biomed Res Int, 2018; 2018; 4734986
4. Gupta R, Thakur S, Pandey NK, Endocrown – a paradigm shift in rehabilitation: A report of two cases: Contemp Clin Dent, 2021; 12(2); 195-98
5. Tzimas K, Tsiafitsa M, Gerasimou P, Tsitrou E, Endocrown restorations for extensively damaged posterior teeth: Clinical performance of three cases: Restor Dent Endod, 2018; 43(4); e38
6. Singh A, Abrol K, Agarwal S, Madan R, Endocrown restorations: A review: Chronicles of Dental Research, 2019; 8(2); 21-26
7. Biacchi GR, Basting RT, Comparison of fracture strength of endocrowns and glass fiber post-retained conventional crowns: Oper Dent, 2012; 37(2); 130-36
8. Dogui H, Abdelmalek F, Amor A, Douki N, Endocrown: An alternative approach for restoring endodontically treated molars with large coronal destruction: Case Rep Dent, 2018; 2018; 1581952
9. Sedrez-Porto JA, Rosa WL, da Silva AF, Endocrown restorations: A systematic review and meta-analysis: J Dent, 2016; 52; 8-14
10. Alotaiby F, Aldulaijan J, Alotaibi M, Endocrowns: A retrospective study among Riyadh Elm university dental clinics: Int J Community Med Public Health, 2021; 8; 3280-84
11. Deepak S, Nivedhitha MS, Endocrown-post endodontic restoration – a questionnaire survey: J Pharmace Sciences Research, 2017; 9(10); 1827-30
12. Alkhafaji AM, Valizadeh S, Endocrown restorations on endodontically treated premolars teeth: A review: Annals Romanian Society Cell Biology, 2021; 25(6); 18606-14
13. Zheng Z, Sun J, Jiang L, Influence of margin design and restorative material on the stress distribution of endocrowns: A 3D finite element analysis: BMC Oral Health, 2022; 22(1); 1-8
14. Anwarullah A, Konagala R, Raju MK, Endocrown – the realm of post-free endodontic restorations: J Evolution Med Dent Sci, 2021; 10(16); 1187-90
15. Hamdy A, Effect of full coverage, endocrowns, onlays, inlays restorations on fracture resistance of endodontically treated molars: J Dent Oral Health, 2015; 1(5); 1-5
16. Rasidi Mq, Priscilla Sd, Knowledge, attitude, and practice of endocrown in post-endodontic management among general practitioners: J Contemp Issues Business Government, 2021; 27(2); 2982
17. Soliman M, Alshamrani L, Yahya B, Monolithic endocrown vs. hybrid intraradicular post/core/crown restorations for endodontically treated teeth; Cross-sectional study: Saudi J Biol Sci, 2021; 28(11); 6523-31
18. : WMA declaration of Helsinki – ethical principles for medical research involving human subjects, 2013, Brazil, World Medical Association https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/
19. Lawshe C, A quantitative approach to content validity: Personnel Psychology, 1975; 28; 563-75
20. Sun J, Ruan W, He J, Clinical efficacy of different marginal forms of endocrowns: Study protocol for a randomized controlled trial: Trials, 2019; 20(1); 454
21. Carvalho AO, Bruzi G, Anderson RE, Influence of adhesive core buildup designs on the resistance of endodontically treated molars restored with lithium disilicate CAD/CAM Crowns: Oper Dent, 2016; 41(1); 76-82
22. Wahab FK, Mahasneh SA, Sawair FA, Restoration of root filled teeth; Current opinions and techniques: Prim Dent J, 2016; 5(2); 29-35
23. Govare N, Contrepois M, Endocrowns: A systematic review: J Prosthet Dent, 2020; 123(3); 411-418e9
24. El-Damanhoury HM, Haj-Ali RN, Platt JA, Fracture resistance and microleakage of endocrowns utilizing three CAD-CAM blocks: Oper Dent, 2015; 40(2); 201-10
25. Carvalho MA, Lazari PC, Gresnigt M, Current options concerning the endodontically-treated teeth restoration with the adhesive approach: Braz Oral Res, 2018; 32(Suppl 1); e74
26. Badr AA, Abozaid AA, Wahsh MM, Morsi TS, Fracture resistance of anterior CAD/CAM nanoceramic resin endocrowns with different preparation designs: Brazilian Dental Science, 2021; 24(3); 1-9
27. Menezes-Silva R, Espinoza CAV, Atta MT, Endocrown: A conservative approach: Brazilian Dental Science, 2016; 19(2); 121-31
28. Guo J, Wang Z, Li X, A comparison of the fracture resistances of endodontically treated mandibular premolars restored with endocrowns and glass fiber post-core retained conventional crowns: J Adv Prosthodont, 2016; 8(6); 489-93
29. Haralur SB, Alamrey AA, Alshehri SA, Effect of different preparation designs and all ceramic materials on fracture strength of molar endocrowns: J Appl Biomater Funct Mater, 2020; 18 2280800020947329
30. Bada BA, Abozaid AA, Wahsh MM, Morsy TS, Fracture resistance of anterior CAD/CAM nanoceramic resin endocrowns with different preparation designs: Braz Dent Sci, 2021; 24(3); 1-12
31. Taha D, Spintzyk S, Schille C, Fracture resistance and failure modes of polymer infiltrated ceramic endocrown restorations with variations in margin design and occlusal thickness: J Prosthodontic Research, 2018; 62(2); 293-97
32. Einhorn M, DuVall N, Wajdowicz M, Preparation ferrule design effect on endocrown failure resistance: J Prosthodont, 2019; 28(1); e237-e42
33. Ahmed MAA, Kern M, Mourshed B, Fracture resistance of maxillary premolars restored with different endocrown designs and materials after artificial ageing: J Prosthodont Res, 2022; 66(1); 141-50
34. Waad A, Endocrowns: A review article: Sch J Dent Sci, 2018; 5(5); 306-9
35. Abu-Nawareg M, Elbann K, Abouelseoud H, Fracture resistance of CAD/CAM endocrowns: Resin nano ceramic vs translucent zirconia: Int J Health Sci Res, 2022; 12(4); 33-43
36. Ghoul WE, Özcan M, Tribst JPM, Salameh Z, Fracture resistance, failure mode and stress concentration in a modified endocrown design: Biomater Investig Dent, 2020; 7(1); 110-19
37. Zainon NA, Kassim ZH, Lim TW, Endocrown: An alternative approach for restoring endodontically treated teeth: Malaysian Dent J, 2019; 1; 46-60
38. Alqahtani SM, Chaturvedi S, Alshahrani AA, Online questionnaire-based study to evaluate the attitudes and use of rubber dental dams by Saudi dental practitioners: Med Sci Monit, 2023; 29; e938672
39. Rocca GT, Rizcalla N, Krejci I, Fiber-reinforced resin coating for endocrown preparations: A technical report: Oper Dent, 2013; 38(3); 242-48
40. Cacciafesta V, Sfondrini MF, Lena A, Flexural strengths of fiber-reinforced composites polymerized with conventional light-curing and additional postcuring: Am J Orthod Dentofacial Orthop, 2007; 132(4); 524-27
41. Ghaffari T, Nourizadeh A, Shafiei E, Compressive strength of temporary crowns made from default design in two types of software: J Dent (Shiraz), 2023; 24(1); 47-52
Figures
Tables
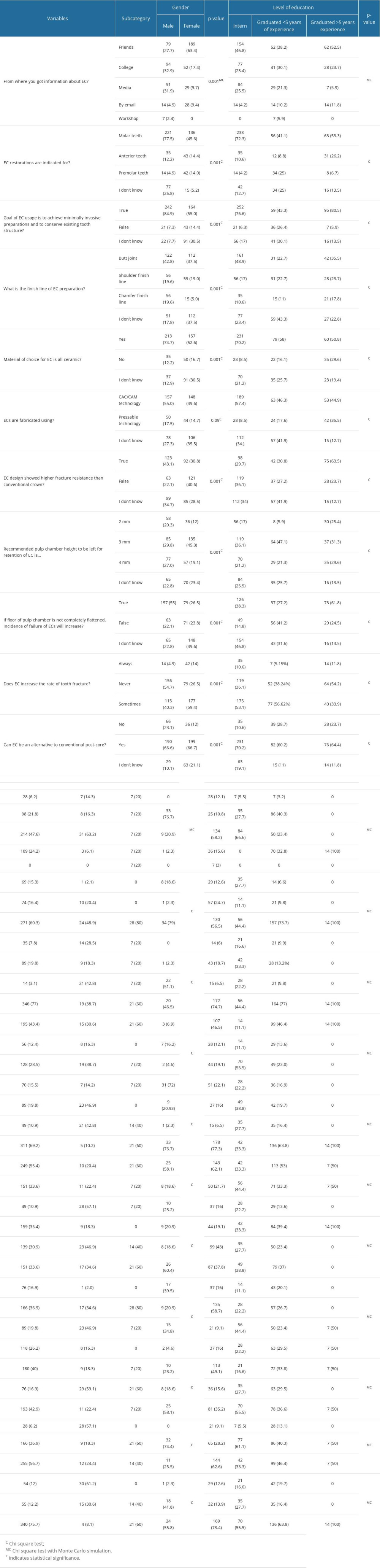 Table 1. Association of knowledge with gender, level of education, country of graduation, and working place.
Table 1. Association of knowledge with gender, level of education, country of graduation, and working place.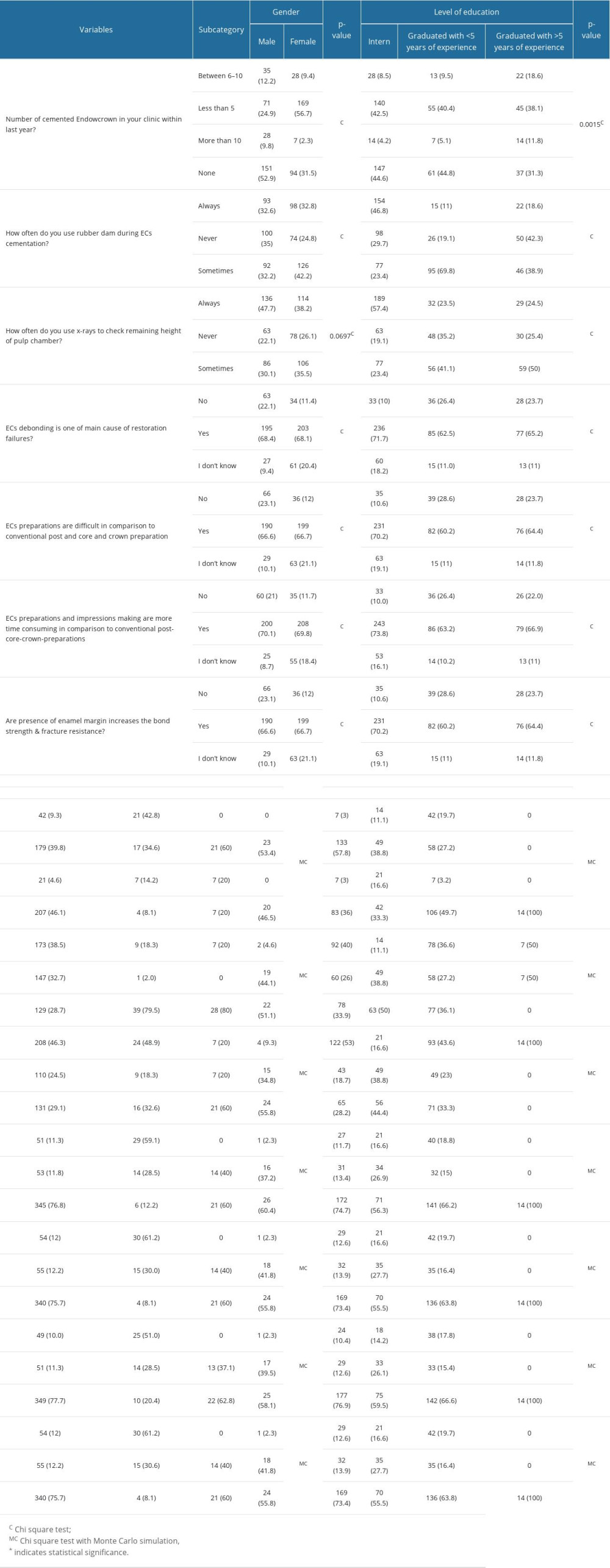 Table 2. Association of practice with gender, level of education, country of graduation, and working place.Table 1. Association of knowledge with gender, level of education, country of graduation, and working place.Table 2. Association of practice with gender, level of education, country of graduation, and working place.
Table 2. Association of practice with gender, level of education, country of graduation, and working place.Table 1. Association of knowledge with gender, level of education, country of graduation, and working place.Table 2. Association of practice with gender, level of education, country of graduation, and working place. In Press
18 Apr 2024 : Clinical Research
Comparative Analysis of Open and Closed Sphincterotomy for the Treatment of Chronic Anal Fissure: Safety an...Med Sci Monit In Press; DOI: 10.12659/MSM.944127
08 Mar 2024 : Laboratory Research
Evaluation of Retentive Strength of 50 Endodontically-Treated Single-Rooted Mandibular Second Premolars Res...Med Sci Monit In Press; DOI: 10.12659/MSM.944110
11 Mar 2024 : Clinical Research
Comparison of Effects of Sugammadex and Neostigmine on Postoperative Neuromuscular Blockade Recovery in Pat...Med Sci Monit In Press; DOI: 10.12659/MSM.942773
12 Mar 2024 : Clinical Research
Comparing Neuromuscular Blockade Measurement Between Upper Arm (TOF Cuff®) and Eyelid (TOF Scan®) Using Miv...Med Sci Monit In Press; DOI: 10.12659/MSM.943630
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952