09 November 2023: Database Analysis
Comparative Finite Element Analysis of Endocrowns and Traditional Restorations for Endodontically Treated Mandibular First Molars
Waleed M.S. Al Qahtani1ABCDEFG*DOI: 10.12659/MSM.941314
Med Sci Monit 2023; 29:e941314






Abstract
BACKGROUND: This study evaluated 2 endocrown designs and traditional restoration with a conventional crown using post and core to find the best restoration design for endodontically treated mandibular first molars.
MATERIAL AND METHODS: Three 3D finite element models were constructed: (1) post and core restoration, (2) endocrown butt joint margin design, and (3) endocrown with shoulder finish line. The intact tooth geometry was extracted with computed tomography, then modified to the selected restoration designs. Bone and mucosa geometry was simplified and represented as 3 cylinders. Two loading cases were examined on E-max crowns as 400N and 200N vertically and 45º oblique, respectively, that were located at buccal cusp tips and central fossa by nodal force distributed on circular areas with 0.5-mm diameter in each location.
RESULTS: Traditional restoration kept crown deformation and stresses at lower levels than did endocrowns. Results of the butt joint margin design were comparable to that of shoulder finish line design. Cement had the lowest stress values under shoulder finish line design, while the remaining tooth indicated the superiority of butt joint margin design, with less stresses by 20% and 24%, compared with traditional and shoulder finish line restorations, respectively.
CONCLUSIONS: The 3 tested restoration designs worked well. Although the differences were small, according to stress analysis results, conventional restoration by post and core achieved the best performance, followed by butt joint margin, which ensures lowest level of stresses on dentine. Finally, the shoulder finish line endocrown can replace the other designs but with higher stress levels.
Keywords: Finite Element Analysis, Molar, Post and Core Technique, Dental Pulp Cavity, Root Canal Therapy, Tooth Preparation, Prosthodontic, Prosthesis Design
Background
The goal of endodontic treatment is the conservation and protection of the root canals of precious teeth to avoid predictable destruction. However, teeth with root canal treatment have a high risk of biomechanical breakdown, compared with teeth with sound structure [1]. The loss of structural integrity combined with caries, trauma, and extensive cavity preparation, as well as dehydration or physical changes in the dentin, are the main causes for the decrease in rigidity and fracture or fatigue resistance of the teeth with root canal treatment. The rehabilitation of endodontically treated multirooted teeth with massive loss of coronal structure is a main goal. The coronal part is frequently considerably destroyed after endodontic treatment and has traditionally been restored with metal posts and cores and prosthetic crowns. Initially, it was believed that the endocrown would offer enhanced reinforcement of the remaining dental structure [2]. The effects of ferrule length, and post type, diameter, and length are topics of research studies on post and core.
On the other hand, the model or study representation used in those studies frequently had a single root and straight canal. However, information about the multiple or curved canals of premolars and molars is not easily found. The difficult root canal anatomies of premolar and molar teeth, in addition to the stiffness and positions of the occlusal forces loaded, make it difficult to use the same steps that are used for single canals when fabricating posts and cores for molar teeth restorations. However, the negative influence on the bond between resin cement and root dentin surface was found for many reasons, including endodontic sealers, irrigants, intracanal medications, grease of temporary cements, and fit checkers [3].
The most common difficulties influencing the filling of endodontically treated molars, with the multiple root canal shapes of posterior teeth, are as follows: multiple root canals with curvature, intensity and direction of occlusal loading force, restricted interocclusal space, accessibility, difficulty in moisture control, retention and resistance form, tilting, supra eruption, or crossbite, and occlusal interference. These definite factors can affect the scenario of the post and core. Therefore, teeth with multiple root canals need an unusual treatment concept, such as separations or a single post for each canal, to increase fracture resistance [4–6].
With the progress in adhesive systems, the new designs of endocrowns are used to replace broken coronal and cervical parts of affected teeth. These endocrown restorations are suggested in case of injured or fractured posterior crowns, in addition to many factors, such as narrow and short roots, obturated root canals, and restricted interarch opening. These endocrowns are seated mechanically in root canals up to 3 to 4 mm by using resin cements for bonding the hard dental tissues. In cases of little dental structures preparation, in comparison to posts and cores, it is advantageous to use these restorations and avoid intervention in the root canals. Nevertheless, the conventional technique needs less time and fewer interfaces between the teeth and each part of the restoration [7].
In finite element studies, using static load to examine extreme load effect does not match the clinical situation of fatigue load and duration [8].
A biomechanical cyclic load examination is superior to a static one, as it is not easy to simulate clinical conditions. With the different forces obtained from cyclic loading applied in the study by Dorriz et al, the load was a standard and equal force. However, the influence of masticatory forces varies in clinical conditions. Making comparisons between different groups is difficult, as cyclic loading tests show a huge spread and unequal results [9].
The endocrown was created by Pissis in 1995 and is the prototype of the endocrown technique, using the “monoblock porcelain technique” [10]. Today, owing to the improvements in adhesive techniques and materials, the endocrown concept of intracoronal replacements is recommended for broken posterior teeth as an alternative to the conventional post and core. Endocrowns are also indicated for reduced inter-occlusal spaces [11].
Endocrowns are commonly made of feldspathic ceramic [7]. The endocrown has proven reliability and success as a traditional technique for restoring endodontically treated teeth4[12–14]. On the other hand, conventional approaches tend to prevent complications associated with the traditional placement of posts, namely the weakening of the root, radicular thinning and perforation, and stress distribution capacity and decay caused by endocrowns. Endocrowns are considered as a first solution for endodontically treated posterior teeth; furthermore, inlays and onlays retain the tooth and have proven their good prognosis and reliability for conservatively treating missing teeth [13].
Collecting the data from the stresses shared inside the roots of multiple-rooted teeth will determine the possibility of a tooth fracture [15]. It has been concluded that posterior teeth filled by endocrowns have less chance of fatigue and fracture than do conventional posts [15]. In the present study, we aimed to compare traditional restoration by post and core and 2 endocrown designs (butt joint margin and shoulder finish line) using finite element analysis.
Material and Methods
Three 3-dimensional (3D) finite element models were specially prepared in this study for the selected designs. Model 1 simulated traditional restoration by post and core; model 2 simulated an endocrown with the butt joint margin design; and model 3 simulated an endocrown with the shoulder finish line. Figure 1 shows schematic drawings of the 3 studied designs.
Left mandibular first molar geometry was extracted from complete mandible computed tomography (CT) scan images. A standard triangle language (STL) file of the intact tooth was manipulated on intermediate software (3-Matic versions 15.01, Materialize, NV, USA) to trim the acquired tooth body points [16] and correct STL file errors to construct the solid tooth model (Figure 2A, 2B).
The mucosa was modeled as a 2-mm-thick cylinder, while the bone geometry was simplified and simulated as 2 co-axial cylinders. The inner cylinder represented the cancellous bone (14 mm in diameter × 22 mm in height), filling the internal space of the outer cylinder (1-mm-thick shell) that represented cortical bone (18 mm in diameter × 26 mm in height), as presented in Figure 2C.
Solid modeling of the bone (cortical and cancellous), mucosa, post, core, 20-μm cement layer, and treated canals. Gutta-percha (GP) were created on “Solidworks” version 2014 (Dassault Systèmes Inc., 13090 Aix-en-Provence, France). These components were exported as STEP files, to be assembled in the finite element package [17]. A set of Boolean operations between the modeled components was performed before obtaining the complete assembled models. The complete models were assembled under the ANSYS environment (ANSYS Inc., Canonsburg, PA, USA), as presented in Figure 2D–2F.
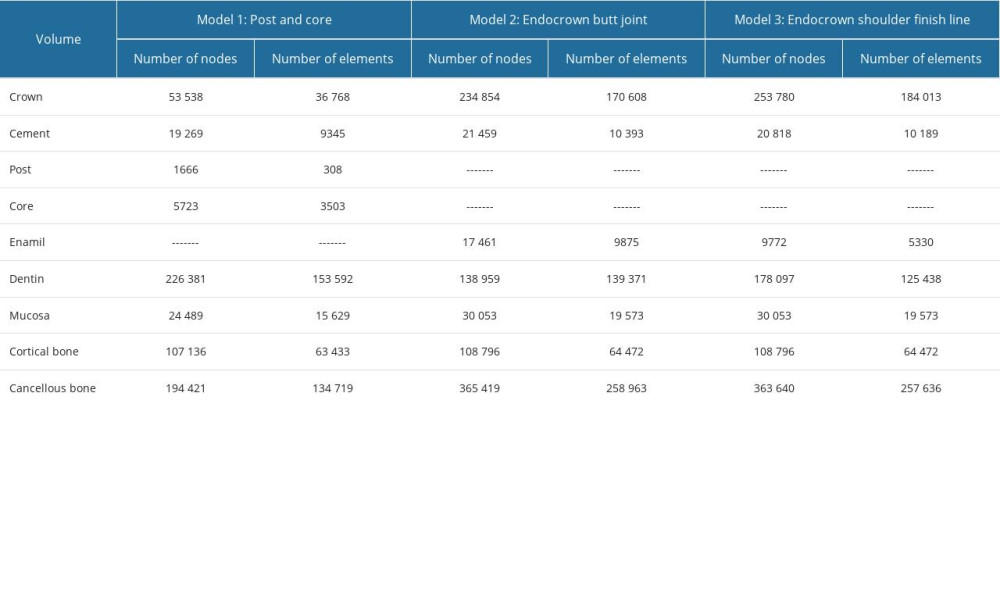
In this study, all materials, except the fiber post, were assumed to be isotropic, homogenous, and linearly elastic; their properties are listed in Table 1. These materials were assigned to the models’ components prior to meshing. Then, a meshing convergence test (based on a less than 3% change in results) was performed. The used numbers of nodes and elements in the analyses are listed in Table 2, and a sample of the meshed models’ components are presented as screenshots from ANSYS in Figure 3.
For each model, 2 loading conditions were tested: 400N vertical compressive load and 200N oblique 45° load placed on the E-max crowns. In both cases, the applied load was located at the buccal cusp tips and central fossa by nodal force distributed on circular areas of 0.5-mm diameter of each location. The lowest plane of each model was considered as fixed in the 3 directions as a boundary condition [1,6,18].
Linear static analyses were performed on Workstation HP Z820 (Dual Intel Xeon E5–2670 v2 processors, 2.5 GHz, 64.0 GB RAM), using the commercial multipurpose finite element software package (ANSYS version 16.0), and the results of these models were verified against similar studies [1,6,18].
Results
Six linear static analyses were performed, and results were compared on each component separately to identify the superiority of each model. Samples of the obtained results are presented in Figure 4.
The recorded deformations and stresses of the E-max crowns were found to be of the same order of magnitude on both endocrown designs, while the traditional restoration (post and core) showed much lower values (Figure 5A). Under vertical loading, the von Mises stress value of the conventional crown was 68% of that of the endocrown, while the butt joint margin crown showed a 5% lower value than the shoulder finish line endocrown. Again, the butt joint margin design showed 10% less von Mises stress value than the shoulder finish line endocrown under oblique loading. On the other hand, the traditional restoration was still superior, with 50% less stress value. All stresses that appeared on the E-max crowns were still in the safe region (away from yielding stress @400 MPa).
The cement layer will receive less stress under the endocrowns than under the traditional restoration. The shoulder finish line design induced the lowest stress values on the cement layer, followed by the butt joint margin design, and finally the traditional restoration. The von Mises value was nearly doubled by switching from one design to the other (Figure 5B).
Dentine (or remaining tooth) results indicated the superiority of the endocrown butt joint margin design, followed by the traditional restoration, and finally the shoulder finish line design. About 20% and 24% less stress was exerted on the remaining tooth by the butt joint margin design in comparison with traditional restoration and shoulder finish line designs, respectively (Figure 5C).
As presented in Figure 5D, neither type of bone (cortical or cancellous) was sensitive to the crown restoration type, and the recorded variation between the studied models was less than 1%.
Finally, mucosa, enamel (if present), post, post cement, and core results were not discussed here due to the insensitivity to crown design and/or no similar parts in the other models to be compared. Generally, all results obtained within this study showed acceptable values that did not exceed physiological limit the model’s component.
Discussion
The cervical sidewalk, or butt joint, is considered the base of restoration. To optimize bonding, a band of peripheral enamel is present. Crimping is forbidden, which is different from shoulder preparation or chamfer techniques. Because compressive stresses are very common on molars, we aimed to achieve a stable wide surface to resist these stresses [19]. To assure stress resistance alongside the main axis of the tooth, the prepared surface is aligned as parallel to the occlusal plane. The trapezoidal shape in mandibular molars and the triangular shape in maxillary molars are crucial to enhance the stability of the restoration [20]; whereas, stability and retention are assured by the pulpal chamber cavity.
If sufficient tooth surfaces are present for bonding, a macroretentive design is no longer essential. Therefore, more conservative modalities, such as endocrowns used to restore endodontically treated teeth, have been presented, especially because of the latest progress achieved in adhesive dentistry [21]. As in clinical situations, the static loading in the present study was applied to fracture resistance as a test to indicate material and type of restoration suitability immediately after bonding. Moreover, fracture resistance values attained are probably not suggestive of success of the restoration in the long term [22]. The results in the present study revealed higher mean fracture resistance values in endocrowns by doing the reduction parallel to long axis with a marked finishing line (shoulder) compared to those with butt margin design. Due to the fact that butt joint designs are prepared corresponding to the occlusal plane, a constant surface resistive to tensile stresses is attained. On the other hand, from a biological and mechanical perspective, the endocrowns permit strains at the bonded part. Therefore, the forces were disseminated either on all axial walls (shear force) or on the cervical butt joint (compression). Accordingly, moderate load on the pulpal floor was achieved by adding a marked finish line (shoulder) with small axial walls. These steps probably also offset the shear stresses by all surfaces, hence creating superior distributed loading at the border [23].
Ceramic endocrowns can be used for anterior teeth restoration. This is due to these benefits and mainly to their aesthetic appeal [21].
Unfortunately, anterior teeth vary from posterior teeth regarding their biomechanics. One study showed that the crowns of anterior teeth are more narrow (7.0 mm) and taller (10.5 mm) than those of molars (where crowns had a length of 7.5 mm, and the bucco-lingual diameter was 10.0 mm at the cervix) [20]. In accordance with lever equilibrium, in incisors, bending stress on restorations appears to be higher than similar stresses imposed on molars. Nevertheless, in endocrowns, the bonding surface is 2 times smaller than in molars, as it is 60 mm2 versus an average of 30 mm2 in anterior teeth. It is worth noting that retention of restorations is negatively affected by all these factors [24].
Using the E-max crown in restoration of the mandibular first molar on a traditional post and core or as endocrowns (butt joint margin and shoulder finish line) revealed long-life results. In this study, crown body results showed that traditional restoration is superior to endocrown designs. This finding may be attributed to the geometry continuity established, which avoided sharp or sudden changes (shoulders) in both thicknesses and shape.
CAD/CAM technology is frequently used in preparing ceramic endocrowns [25]. Sintering and pressing is used as well. High strength is delivered successfully on endocrown-restored molars. This was noted during masticatory simulation using 3D-finite element analysis of these molars and posts [26] and fracture resistance during loading. Failure type and individuality of lithium disilicate, fracture strength, and multiphase resin composite of endocrowns below resulted in forces parallel to the long axis and laterally [27]. This was stated in a study comparing fracture strength of glass fiber post-retained conventional crowns and endocrowns [28]. A 5-year follow-up clinical study showed that 87.1% of endocrowns in posterior teeth were well functioning, with no tendency to fracture or debonding. The survival of ceramic CAD/CAM crowns bonded to preparations with reduced macroretention geometry are more accurate and long-lasting [29]. In fact, treatment failures occurred more often in premolars than in molars (75% vs 90.5%) during a 12-year interval. Clinical results of CAD/CAM with feldspathic ceramic molar shoulder crowns and endocrowns showed survival up to 12 years [30].
Resin cement will not fail under the applied loads whatever the crown design. The stresses that appeared on the resin cement were relatively low in comparison with its yielding strength. The greatest contact area with the cement layer is encountered in the endocrown possessing a shoulder finish line; this design can cause a noticeable reduction in cement layer stresses.
Treatment decisions have markedly changed and become more conservative for endodontically treated teeth. This coincided with the enhancements in adhesive dentistry. Therefore, conventional posts and cores are not required as before. Instead, other modalities have been adopted, such as ceramic indirect inlays and onlays, as well as endocrowns for root canal–treated molars [6].
Endocrowns are appropriate for all posterior teeth, mainly for persons with a small coronal part clinically, root canals with calcifications, and a very tapered form of roots. The adhesive technique is required for placement of endocrowns, and proper isolation is mandatory, otherwise using endocrowns is contraindicated when the depth of the root canal is less than 3 mm, or when the cervical border is less than 2 mm of the entire boundary [20].
In an attempt to avoid fracture of the root, new adhesives are applied in patients with thin root canal structures. These adhesives are applied with a greater Young’s modulus and have the ability to absorb shock caused by the effect of long-term chewing, mastication, and occlusion applied on the root canal. Adhesives with a greater Young’s modulus are similarly suggested for patients with thick root canal tissues. Therefore, these different types of adhesives could help in reducing the concentrated stresses on the root canal orifice [31].
When the marginal adaptation of the restoration with a prepared tooth structure is perfect, it is reflected in the success of all fixed restorations. When the luting material is left unprotected from the oral environment and is in the presence of increased marginal discrepancies, cement softening can result [14]. Moreover, another study confirmed that the increase in marginal and internal gaps of endocrown restorations is directly proportional to that of the intraradicular extension of endocrown restorations [32].
The perfect positions for cementation to the tooth, cementation of the post, and the layers of cement are not always found in the oral cavity. An additional limitation in this study was the use of manual force to preserve the crowns with their posts in a location that could not give a uniform applying force and load. Also, the ferrule stature was frequently not the same in the region of the tooth boundary [8].
The major factor for stress distribution patterns are the functional loads in the finite element analysis (FEA) study. In former studies, an axial load was applied to the occlusal surface centered on the 3 points of articulation in a tripoidism model (considered as function contacts). This caused the stress of the restoration to be constantly put on the loading point. Practically, throughout the chewing cycle, the functional contacts are local, rather than single points. Nevertheless, the texture of the food bolus affects the mastication in the oral milieu as a motor activity. Therefore, in the present study, to simulate the chewing procedure better, the food bolus was applied in a way that could equally distribute the load on the surface of the endocrown [31]. With respect to clinical operability, arranging endocrowns with a 20° bevel margin and a butt joint margin is a more competent and less sensitive technique than are endocrowns based on the other 2 margins. Nevertheless, it is worth mentioning that we observed greater uniform stress disseminated over the cervical butt joint axial walls in the butt joint margin and 20° bevel margin in this study [31].
Neither type of bone (cortical and cancellous) or mucosa were not sensitive to the crown restoration type. This finding indicated good mechanisms of load transferring by the 3 tested designs within this study. Our results matched those of a similar study [33], in which the bone did not differ regarding stress distribution for 3 units bridge design and the bridge was retained by endocrown with 2 abutments. That study concluded that the highest stresses where located on the finishing line of the tooth [33].
In contrast with a conventional post-core crown, the endocrowns decreased stress absorption for the inner wall of the root canal structure. The higher stresses were obtained with endocrowns at the external root walls, although crowns with a post and core demonstrated increased stresses at the internal root canal surfaces, specially the metallic ready-made and casted post. Endocrowns restoring posterior teeth are less sensitive to fracture of the root than are those with posts [15].
Conclusions
The 3 tested restoration designs can work well, with expected high success rates, while each of them showed advantages and disadvantages when compared to each other. Traditional restoration by post and core is the best restoration for crown body lifetime and function, while it falls in the middle among tested designs for dentine stresses. Traditional restoration had the worst behavior on the cement layer. The butt joint margin endocrown design ensures the lowest level of stress on dentine, while the shoulder finish line endocrown can be kept cemented under a higher level of loads than the 2 other designs.
Figures
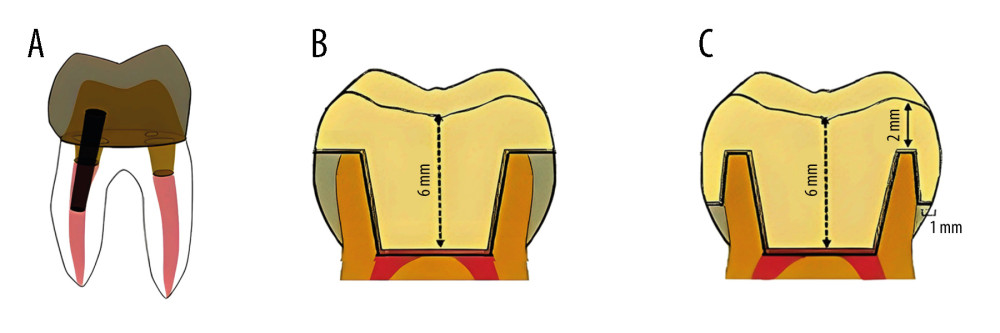 Figure 1. Schematic of the 3 restorations designs (A) post and core restoration, (B) endocrown butt joint margin, (C) endocrown with shoulder finish line. Software: MS Paint and Adobe Illustrator (version 2023, Adobe Co., CA, USA).
Figure 1. Schematic of the 3 restorations designs (A) post and core restoration, (B) endocrown butt joint margin, (C) endocrown with shoulder finish line. Software: MS Paint and Adobe Illustrator (version 2023, Adobe Co., CA, USA). 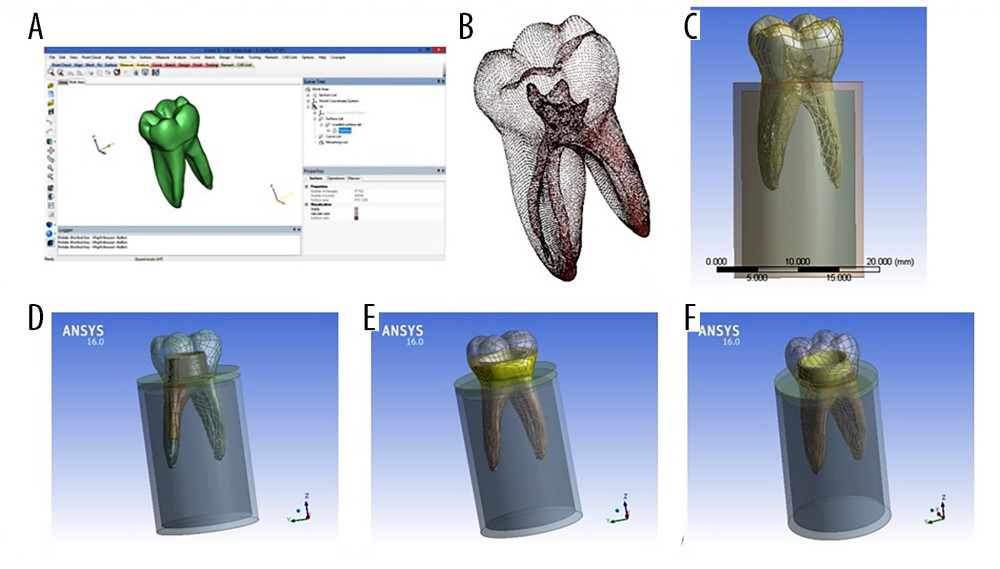 Figure 2. Models’ components during preparation (A) 3-matic screen during tooth extracting, (B) STL file points, (C) intact tooth inside bone cylinders, and the 3 final finite element models geometries; (D) post and core restoration, (E) endocrown butt joint margin, (F) endocrown with shoulder finish line. Software: 3-Matic (version 15.01, Materialize, NV, USA); software: ANSYS (version 16, ANSYS Inc., Canonsburg, PA, USA).
Figure 2. Models’ components during preparation (A) 3-matic screen during tooth extracting, (B) STL file points, (C) intact tooth inside bone cylinders, and the 3 final finite element models geometries; (D) post and core restoration, (E) endocrown butt joint margin, (F) endocrown with shoulder finish line. Software: 3-Matic (version 15.01, Materialize, NV, USA); software: ANSYS (version 16, ANSYS Inc., Canonsburg, PA, USA). 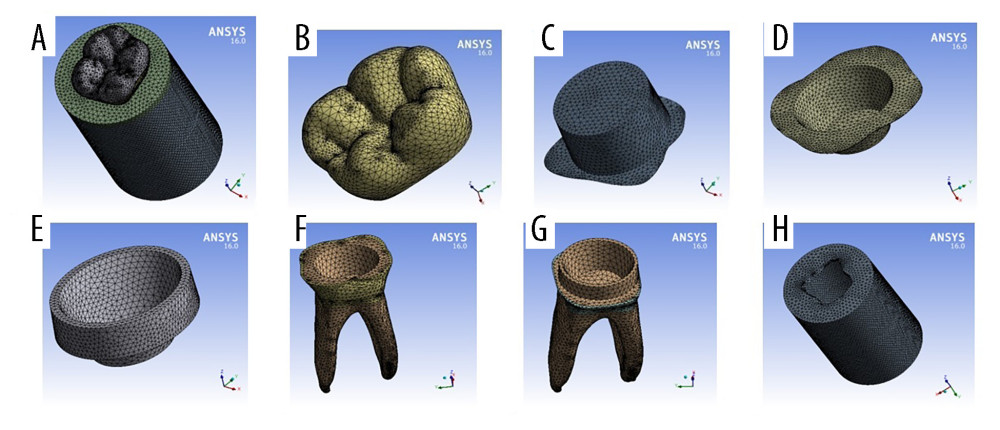 Figure 3. Final models meshed components from Ansys screen; (A) full model, (B) crown; (C) cement above core, (D) butt joint margin cement, (E) shoulder finish line cement, (F) remaining tooth under butt joint margin, (G) remaining tooth under shoulder finish line, (H) cortical bone. Software: ANSYS (version 16, ANSYS Inc., Canonsburg, PA, USA).
Figure 3. Final models meshed components from Ansys screen; (A) full model, (B) crown; (C) cement above core, (D) butt joint margin cement, (E) shoulder finish line cement, (F) remaining tooth under butt joint margin, (G) remaining tooth under shoulder finish line, (H) cortical bone. Software: ANSYS (version 16, ANSYS Inc., Canonsburg, PA, USA).  Figure 4. Sample results obtained during the vertical loading analyses; (A–D) model 1, (E, F) model 2, (H–I) model 3. Software: ANSYS (version 16, ANSYS Inc., Canonsburg, PA, USA).
Figure 4. Sample results obtained during the vertical loading analyses; (A–D) model 1, (E, F) model 2, (H–I) model 3. Software: ANSYS (version 16, ANSYS Inc., Canonsburg, PA, USA). 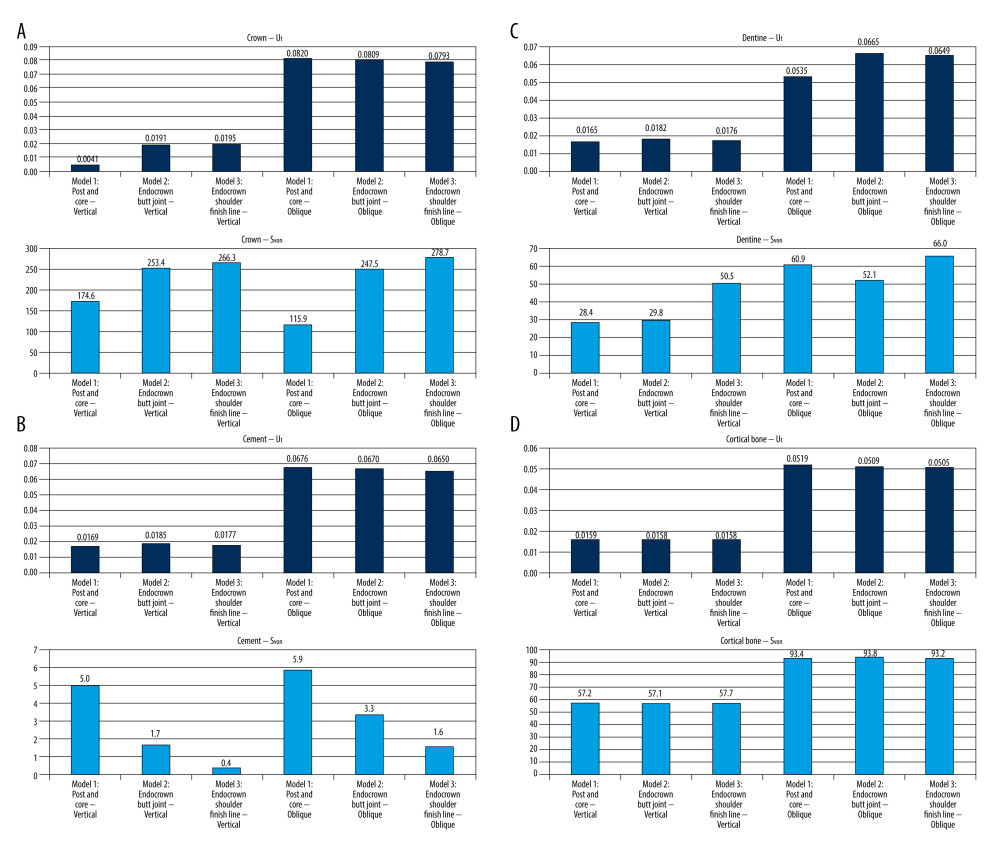 Figure 5. Total deformation and von Mises stress on selected components; (A) crown, (B) cement, (C) dentine, and (D) cortical bone. Software: MS Excel (version 2007, Microsoft Inc., Redmond, WA, USA).
Figure 5. Total deformation and von Mises stress on selected components; (A) crown, (B) cement, (C) dentine, and (D) cortical bone. Software: MS Excel (version 2007, Microsoft Inc., Redmond, WA, USA). 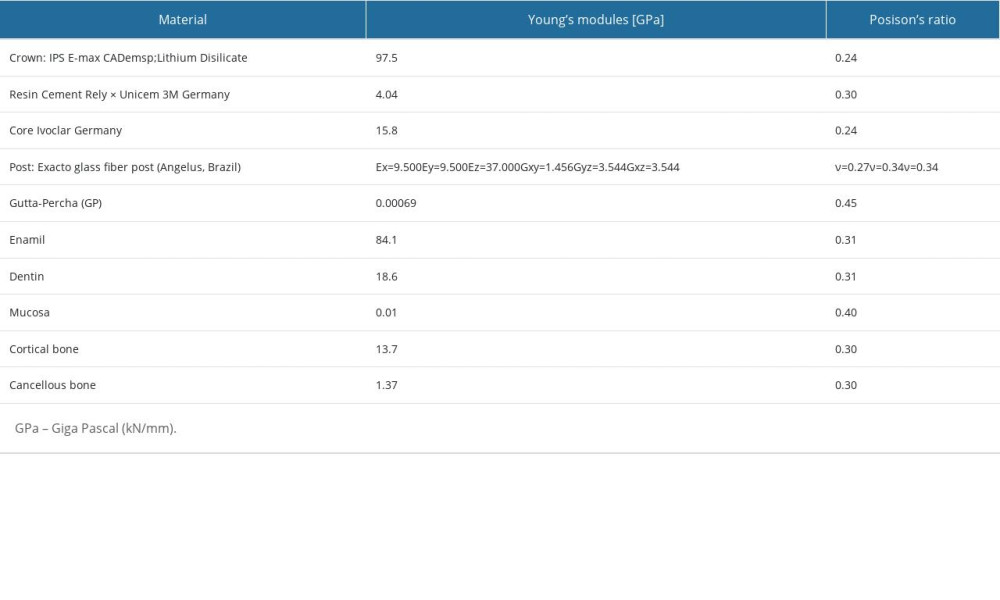
References
1. Taha D, Spintzyk S, Schille C, Fracture resistance and failure modes of polymer infiltrated ceramic endocrown restorations with variations in margin design and occlusal thickness: J Prosthodont Res, 2018; 62(3); 293-97
2. Tribst JPM, Borges ALS, Silva-Concílio LR, Effect of restorative material on mechanical response of provisional endocrowns: A 3D-FEA study: Materials (Basel), 2021; 14(3); 649
3. Zheng Z, Wang H, Mo J, Effect of virtual cement space and restorative materials on the adaptation of CAD-CAM endocrowns: BMC Oral Health, 2022; 22; 580
4. Liu M, Restoration of endodontically treated premolars and molars: A review of rationales and techniques: J Prosthodont Implantol, 2014; 3(1); 1-16
5. Shafiei F, Memarpour M, Effect of chlorhexidine application on long-term shear bond strength of resin cements to dentin: J Prosthodont Res, 2010; 54; 153-58
6. Soliman KM, Mandor MH, El Mekkawi W, Marginal adaptation of lithium disilicate endocrowns with different cavity depths and margin designs: Al-Azhar Dental Journal for Girls, 2019; 6(2); 177-85
7. El-Damanhoury HM, Haj-Ali RN, Platt JA, Fracture resistance and microleakage of endocrowns utilizing three CAD-CAM blocks: Oper Dent, 2015; 40(2); 201-10
8. Abduljabar A, Iskander A, Elfezary M, Endocrown feasibility for primary molars: A finite element study: Eur J Dent, 2023 [Online ahead of print]
9. Dorriz H, Alikhasi M, Mirfazaelian A, Hooshmand T, Effect of ferrule and bonding on the compressive fracture resistance of post and core restorations: J Contemp Dent Pract, 2009; 10(1); 001-008
10. Pissis P, Fabrication of a metal-free ceramic restoration utilizing the monobloc technique: Pract Periodontics Aesthet Dent, 1995; 7(5); 83-94
11. Shin Y, Park S, Park JW, Evaluation of the marginal and internal discrepancies of CAD/CAM endocrowns with different cavity depths: an in vitro study: J Prosthet Dent, 2017; 117(1); 109-15
12. Bernhart J, Bräuning A, Altenburger MJ, Wrbas KT, Cerec 3D endocrowns-two year clinical examination of CAD/CAM crowns for restoring endodontically treated molars: Int J Comput Dent, 2010; 13; 141-54
13. Iglesia-Puig MA, Arellano-Cabornero A, Inlay fixed partial dentures a conservative approach for restoring posterior missing teeth: J Prosthet Dent, 2003; 89; 443-45
14. Bindl A, Richter B, Mormann WH, Survival of ceramic computeraided design/manufacturing crowns bonded to preparations with reduced macroretention geometry: Int J Pros, 2005; 18; 219-24
15. Lin J, Lin Z, Zheng Z, Effect of different restorative crown design and materials on stress distribution in endodontically treated molars: A finite element analysis study: BMC Oral Health, 2020; 20(1); 226
16. Al Qahtani WMS, El-Anwar MI, Advanced computational methods in Bio-Mechanics: Open Acces Maced J Med Sci, 2018; 6(4); 742-46
17. Al Qahtani WMS, Yousief SA, El-Anwar MI, Recent advances in material and geometrical modelling in dental applications: Open Access Maced J Med Sci, 2018; 6(6); 1138-44
18. Dejak B, Młotkowski A, Strength comparison of anterior teeth restored with ceramic endocrowns vs custom-made post and cores: J Prosthodont Res, 2018; 62(2); 171-76
19. Tribst J, Piva A, Jager N, Full crown versus endocrown approach: A 3D analysis of both restorations and the effect of ferrule and restoration material: J Prosthodont, 2021; 30(4); 335-44
20. Fages M, Bennasar B, The endocrown: A different type of all-ceramic reconstruction for molars: J Can Dent Assoc, 2013; 79; d140
21. Tribst J, Piva A, Muris J, Kleverlaan C, Feilzer A, Endocrown fixed partial denture: Is it possible?: J Prosthet Dent, 2023 [Online ahead of print]
22. Goodacre CJ, Campagni WV, Aquilino SA, Tooth preparations for complete crowns: An art form based on scientific principles: J Prosthet Dent, 2001; 85; 363-76
23. Skouridou N, Pollington S, Rosentritt M, Tsitrou E, Fracture strength of minimally prepared all-ceramic CEREC crowns after simulating 5 years of service: Dent Mater, 2013; 29; e70-77
24. Ash M, Nelson S: Wheeler’s dental anatomy, physiology and occlusion, 2003; 297-314, Philadelphia, Saunders Co
25. Sedrez-Porto JA, Rosa WL, da Silva AF, Endocrown restorations: A systematic review and meta-analysis: J Dent, 2016; 52; 8-14
26. Zheng Z, Sun J, Jiang L, Influence of margin design and restorative material on the stress distribution of endocrowns: A 3D finite element analysis: BMC Oral Health, 2022; 22(1); 30
27. Huang Y, Fokkinga WA, Zhang Q, Biomechanical properties of different endocrown designs on endodontically treated teeth: J Mech Behav Biomed Mater, 2023; 140; 105691
28. Cheng X, Zhang XY, Qian WH, Influence of different base materials and thicknesses on the fracture resistance of endocrown: A three-dimensional finite element analysis: BMC Oral Health, 2022; 22(1); 363
29. Abduljabar AH, Iskander AW, Elfezary MT, Endocrown feasibility for primary molars: A finite element study: Eur J Dent [Online ahead of print]
30. Zhai XY, Zhang JY, Zhang SK, Finite-element analysis of mandibular first molar with two marginal designs of endocrown for the repair of different defects: Hua Xi Kou Qiang Yi Xue Za Zhi, 2019; 37(5); 480-84
31. Zheng Z, Sun J, Jiang L, Influence of margin design and restorative material on the stress distribution of endocrowns: A 3D finite element analysis: BMC Oral Health, 2022; 22(1); 30
32. Gaintantzopoulou MD, El-Damanhoury HM, Effect of preparation depth on the marginal and internal adaptation of computer-aided design/computer-assisted manufacture endocrowns: Oper Dent, 2016; 41; 607-16
33. Morsi TS, Hussein GAF, El-Anwar MI, Stress distribution of different endocrown retained bridge designs replacing missing upper first molar (finite element analysis study): Dent Adv Res, 2020; 5(1); 169
Figures
Figure 1. Schematic of the 3 restorations designs (A) post and core restoration, (B) endocrown butt joint margin, (C) endocrown with shoulder finish line. Software: MS Paint and Adobe Illustrator (version 2023, Adobe Co., CA, USA).Figure 2. Models’ components during preparation (A) 3-matic screen during tooth extracting, (B) STL file points, (C) intact tooth inside bone cylinders, and the 3 final finite element models geometries; (D) post and core restoration, (E) endocrown butt joint margin, (F) endocrown with shoulder finish line. Software: 3-Matic (version 15.01, Materialize, NV, USA); software: ANSYS (version 16, ANSYS Inc., Canonsburg, PA, USA).Figure 3. Final models meshed components from Ansys screen; (A) full model, (B) crown; (C) cement above core, (D) butt joint margin cement, (E) shoulder finish line cement, (F) remaining tooth under butt joint margin, (G) remaining tooth under shoulder finish line, (H) cortical bone. Software: ANSYS (version 16, ANSYS Inc., Canonsburg, PA, USA).Figure 4. Sample results obtained during the vertical loading analyses; (A–D) model 1, (E, F) model 2, (H–I) model 3. Software: ANSYS (version 16, ANSYS Inc., Canonsburg, PA, USA).Figure 5. Total deformation and von Mises stress on selected components; (A) crown, (B) cement, (C) dentine, and (D) cortical bone. Software: MS Excel (version 2007, Microsoft Inc., Redmond, WA, USA). In Press
18 Apr 2024 : Clinical Research
Comparative Analysis of Open and Closed Sphincterotomy for the Treatment of Chronic Anal Fissure: Safety an...Med Sci Monit In Press; DOI: 10.12659/MSM.944127
08 Mar 2024 : Laboratory Research
Evaluation of Retentive Strength of 50 Endodontically-Treated Single-Rooted Mandibular Second Premolars Res...Med Sci Monit In Press; DOI: 10.12659/MSM.944110
11 Mar 2024 : Clinical Research
Comparison of Effects of Sugammadex and Neostigmine on Postoperative Neuromuscular Blockade Recovery in Pat...Med Sci Monit In Press; DOI: 10.12659/MSM.942773
12 Mar 2024 : Clinical Research
Comparing Neuromuscular Blockade Measurement Between Upper Arm (TOF Cuff®) and Eyelid (TOF Scan®) Using Miv...Med Sci Monit In Press; DOI: 10.12659/MSM.943630
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952