22 September 2023: Clinical Research
Comparative Analysis of Morphological Characteristics and Localization of Maxillary Impacted Canines using Cone Beam Computed Tomography
Vilte Viktoraviciute1ABCDEF, Guoda MockuteDOI: 10.12659/MSM.941476
Med Sci Monit 2023; 29:e941476






Abstract
BACKGROUND: This study aimed to evaluate the crown length and width and root length and dilacerations in unilateral impacted maxillary canines, compared with contralateral erupted canines, and to investigate the relationship between the morphology of impacted canines and their localization.
MATERIAL AND METHODS: Pretreatment cone beam computed tomography (CBCT) of 40 patients (age range 11-34 years) with unilateral impacted maxillary canines (IC) were analyzed. The crown length, crown width, root length, and dilacerations of IC were assessed and compared with that of contralateral erupted canines (CC). The eruption path length, impaction depth, and impaction height were measured, and mesio-distal and labio-palatal positions of the IC were determined.
RESULTS: Crown length and width of IC were significantly greater, by 0.15 mm and 0.26 mm, respectively, than that of CC (P<0.001). Root length of IC was shorter than that of CC by 1.46 mm (P<0.001). Root dilaceration was found in 72.5% of IC and 60% of CC (P=0.213). The mean dilaceration angle of IC was 8.84° higher than that of CC (P>0.05). Correlations existed between direction of dilaceration and length of the eruption path (P=0.027), IC root length and depth of impaction (P=0.017), root length (P=0.037), and direction of root dilaceration (P=0.03) and the position of the IC in the mesio-distal direction.
CONCLUSIONS: IC crown length and width were significantly longer than that of CC, while IC root length was shorter. Longer root length was observed in impacted canines with greater mesio-distal and horizontal dislocation.
Keywords: Cone-Beam Computed Tomography, Orthodontics, Tooth, Impacted, Humans, Child, Adolescent, young adult, Adult, Maxilla, Cuspid, Palate, Retrospective Studies
Background
The treatment of impacted canines, a common issue affecting 1% to 3% [1–4] of the population, continues to pose challenges, owing to its complex nature and potential complications. Studies evaluating factors that influence the success and duration of orthodontic eruption have revealed the effects of age, sex, impaction side, root-cortex relationship, inclination, and height or mesio-distal localization of impacted teeth [5–9]. The morphology of the impacted tooth itself can also have an impact on the complexity of the treatment. Impacted canines with dilacerated roots show longer duration and higher external root resorption values than those with normal roots [8]. Treatment of impacted canines with root dilacerations is complicated and requires continuous monitoring of the situation [10–12]. Becker et al indicate that the major reasons for forced extrusion failure are inadequate anchorage (48.6%), mistaken location (40.5%), and ankylosis (32.4%) [13]. Authors emphasize the use of 3-dimensional (3D) imaging for correct diagnosis and treatment planning [13,14].
Cone beam computed tomography (CBCT), commonly recognized as digital volume tomography, pertains to the conversion of image data into digital formats and, of utmost significance, to the visual portrayal of anatomical structures in 3 dimensions [15]. This method allows a thorough analysis of high-quality images in the axial, coronal, and sagittal planes as well as the determination of impaction complexity, which results in better treatment outcomes [16–18]. With the knowledge of the impacted canine eruption path length, impaction depth, and impaction height, it is possible to predict the forced eruption time of the impacted canine [19]. Several studies emphasize the superior diagnostic accuracy of CBCT over conventional radiography [20–23]. Bodner et al, after analyzing the accuracy of impacted teeth images by comparing conventional radiography and computed tomography, stated that the crown and root shape, crown-root ratio, and inclination of the tooth were observed more clearly in computed tomography images than in 2D radiographs [22]. Similarly, Alfailany et al reported that CBCT demonstrated superior performance compared with 2D radiography in accurately determining the position of the impacted maxillary canines (labio-palatal, mesio-distal, and vertical), assessing the development of the root apex, detecting the presence of resorption in the adjacent incisors, and diagnosing the ankylosis of impacted canines [23].
A limited number of studies have analyzed the morphology of impacted canines compared with that of normally erupted canines [10,11,24,25] and the influence of the severity of impaction on the morphology of the impacted canine [10,11,25]. However, research methodologies differ. In the studies by Kim et al [24] and Dekel et al [25], control groups consisted of contralateral erupted canines, while the studies of Cao et al [11] and Hettiarachchi et al [10] had matched controls. The criteria for evaluation of impacted canine localization also differ. Horizontal dislocation of impacted canines was assessed only in the study by Dekel et al [25]. The morphological characteristics of upper permanent impacted canines, such as crown length, crown width, root length, root dilaceration angle, length, and direction, and the location of the impacted tooth in the labio-palatal, vertical, and mesio-distal directions are significant factors for orthodontic or surgical treatment.
Therefore, this study aimed to evaluate the crown length and width and root length and dilacerations in unilateral impacted maxillary canine teeth, compared with that of contralateral erupted canines, and to investigate the relationship between the morphology of the impacted canine and its localization.
Material and Methods
CBCT ANALYSIS:
To perform the research work, the data of the CBCT were used in DICOM format, which was obtained with White Fox 3D imaging (Aceton Group, Rome, Italy). The set parameters of the White Fox 3D scanner performing CBCT are 16 mA, 105 kV, the field of view 150×130 mm, and dose value 1100 mGy cm2.
Images were analyzed by White Fox Imaging software, version 4.0. Tomograms were analyzed in the axial, sagittal, and coronal planes. For the analysis of radiological images, the measurement functions of the programs used to measure the segment and angle (measure distance; measure angle) and the units of measurement of millimeters (mm) and degrees (°) were used. The measurements were performed by one investigator. To assess the reliability, the second investigator measured 10 randomly selected CBCT records, and 2 sets of measurements were evaluated by intraclass correlation coefficient. After a reasonable time interval, again, 10 randomly selected CBCT records were reviewed, and repeated measurements of quantitative parameters were performed. The reliability of the assessment was calculated using the Wilcoxon test.
EVALUATION OF IMPACTED CANINE CROWN LENGTH AND WIDTH:
Linear measures were taken along the tooth long axis. The CBCT images were analyzed in coronal and sagittal planes in order to measure the crown length of the impacted canines. The crown length was determined to be the distance between the cusp tip and the midpoint of the labial cementoenamel junction (Figure 1A) [10].
The width of the impacted canine crown was measured after finding a suitable diagonal cut in the axial projection, where the widest mesio-distal part of the crown was found (Figure 1B).
EVALUATION OF IMPACTED CANINE ROOT LENGTH AND DILACERATION:
The root length of the impacted canines was considered as the distance from the midpoint of the labial cementoenamel junction to the root apex [10].
If the tooth root had a curve (dilaceration), then the measurement method of Hettiarachchi et al [10] was used. The length of the dilacerated part of the impacted canine root was considered as the distance from the apex to the long axis of the canine (Figure 2, distance a). In this case, to measure the total impacted canine root length, the length of the dilacerated part of the root (distance a) and the distance from the midpoint of the cementoenamel junction to the starting point of the root curve (distance b) were summed (Figure 2).
To measure the impacted canine dilaceration angle, the methodology of Lyu et al and Sun et al [14,26] was used. The root dilaceration angle was determined as the angle between the 2 dilacerated parts: the longitudinal axis of the crown and that of the dilacerated portion of the root (Figure 3). The dilaceration direction (mesial, distal, labial, or palatal) was recorded.
EVALUATION OF CONTRALATERAL CANINE:
The morphological characteristics of the contralateral canines (crown length and width, root length and dilaceration) were evaluated according to previously described methods.
LABIO-PALATAL POSITION: The position of the impacted canine tooth in the labio-palatal direction was determined in the axial projection. Three positions were distinguished based on the relationship with the lateral incisor [27]: (1) labial (vestibular): when the impacted canine was on the labial side of the dental arch, in relation to the contour of adjacent lateral incisor; (2) intra-alveolar: when the impacted canine was in the area bounded by the vestibular and palatal contours of the adjacent teeth; and (3) palatal: when the impacted canines was on the palatal side of the dental arch, in relation to the contour of adjacent lateral incisor.
MESIO-DISTAL POSITION: The localization of the impacted canine in the mesio-distal direction was determined by considering the relationship between the cusp tip of the impacted canine and the adjacent teeth [28]. The mesio-distal position of the impacted canine cusp tip was classified by 5 sectors: sector 1 corresponds to the boundaries of the deciduous canine; sector 2 indicates the distal aspect to the midline of the lateral incisor; sector 3 indicates the midline of the lateral incisor to the distal aspect of the central incisor; sector 4 indicates the distal aspect to the midline of the central incisor; and sector 5 indicates the midline of the central incisor to the midline of the maxillary arch.
ERUPTION PATH LENGTH: The CBCT simplified analysis method of eruption path length measurement was used [19]. To find the eruption path, the distance between the cusp tip of the impacted tooth crown and the point of its anticipated correct position was measured (Figure 4).
IMPACTION DEPTH AND HEIGHT: The CBCT trigonometric analysis method described by Schubert et al was used [19]. The distance x – the horizontal movement component – was defined as the impaction depth. The distance y – the vertical movement component – was defined as the impaction height.
STATISTICAL DATA ANALYSIS:
The statistical data analysis was conducted using IBM SPSS Statistics program, version 28.0.1.0 (IBM Corp, Armonk, NY, USA). The normality of the distribution of quantitative variable values was assessed by the Shapiro-Wilk test. The non-parametric Mann-Whitney U test was used for comparison of data in case of non-normality. In cases with several independent groups, the non-parametric Kruskal-Wallis test was used. The homogeneity of the distribution of qualitative values in the comparative independent groups was checked by applying the chi-square criterion of homogeneity or Fisher’s exact test. To assess the correlation between 2 quantitative characteristics satisfying the conditions of normal distribution, the Pearson correlation coefficient was used, and between 2 quantitative characteristics not satisfying the conditions of normal distribution, the Spearman correlation coefficient was used. Identified differences and dependencies between characteristics were statistically significant when
Results
EVALUATION OF IMPACTED AND CONTRALATERAL CANINE MORPHOLOGY:
Differences between impacted and contralateral canine crown length and width are shown in Table 1. Crown width and length were significantly greater in impacted teeth. A statistically significant difference was found between impacted and contralateral canine root lengths, with the root length of impacted canines 1.46 mm shorter than the contralateral canines.
Root dilaceration was found in 29 (72.5%) impacted canines and 24 (60%) contralateral canines. No statistically significant difference was observed between impacted and contralateral canines’ frequency of dilacerations (
Mesial root dilaceration direction was observed in 20 (69.0%) impacted canines, distal in 4 (13.80%), palatal in 4 (13.80%), and labial direction in 1 (3.45%) impacted canine. Contralateral canines showed distal root dilaceration direction in 15 (62.5%) cases, labial in 5 (20.83%), mesial in 4 (16.67%) cases, and palatal dilaceration was not determined. No statistically significant difference was assessed between impacted and contralateral canines when the frequency of occurrence of root dilaceration direction was evaluated (
In evaluating the dilaceration angle and the length of the dilacerated part of the root in impacted and contralateral maxillary canines, a statistically significant difference was not found, although the mean dilaceration angle of the impacted canines was 8.84° higher than that of the contralateral canines (Table 2).
No statistically significant relationship was found between the dilaceration angle of the root and the length of the dilacerated part of the root (distance from the apex of the root to the long axis of the canine), when evaluating impacted and contralateral canines (
EVALUATION OF DEPENDENCE OF IMPACTED CANINE MORPHOLOGY (CROWN LENGTH AND WIDTH, ROOT LENGTH, AND DILACERATION) ON ITS LOCALIZATION:
Statistically significant differences were not found between impacted canine crown lengths, widths, root lengths, angle of root dilaceration, length of the dilacerated root part, direction of dilacerations, and position of the impacted canines in the labio-palatal direction (
There was no statistically significant correlation between crown lengths, crown widths, and the position of the impacted canines in the mesio-distal direction (
There was no statistically significant correlation between the impacted canine root dilaceration angle, length of the dilacerated part of the root, and position of the impacted canines in the mesio-distal direction (
The longest eruption path length was estimated in labially impacted canines (16.19 [6.22] mm), and the shortest in intra-alveolar impacted canines (12.44 [4.28] mm). The eruption path of palatally impacted canines was 14.10 [5.40] mm. There was no statistical dependence between impacted canine crown length and width, root length, and eruption path length (
No statistically significant difference (
A statistically significant correlation was found between the direction of dilaceration of the roots and the length of the eruption path (Table 3). The palatal direction of dilaceration was associated with the longest impacted canine eruption path.
No significant correlations were found in the dependence of impacted canine morphology on impaction depth, with the exception of a correlation between root length and depth of impaction (
No statistically significant correlation was found in the dependence of impacted canine morphology on impaction height.
Discussion
EVALUATION OF IMPACTED AND CONTRALATERAL CANINE MORPHOLOGY:
In evaluating the morphology of impacted and contralateral canines, there was a statistically significant difference between the crown length and width of impacted and contralateral canines. Longer (by 0.15 mm) and wider (by 0.26 mm) crowns were found in impacted canines. Our findings agree with the results of similar studies [10,24]. Kim et al found a similar significant difference between the crown volumes of impacted and contralateral canines and emphasized the necessity of creating more space in the dental arch for the orthodontic extrusion of impacted canines [24]. The greater crown length should also be considered when planning orthodontic forced eruption and occlusal plane formation. Although the statistically significant difference in crown length and width between impacted and contralateral canines was observed, clinically such a difference should not cause much difficulty during orthodontic treatment. In addition, the difference in crown length could be due to measurement difference: the length of impacted canines was measured on unerupted teeth, whereas the length of contralateral canines was measured on already erupted teeth, which could have been affected by attrition.
However, contrary results could be observed in studies that evaluated crown width using digital dental casts [29,30]. Such a discrepancy between the digital dental casts and CBCT examinations could not be due to the inaccuracy of the CBCT. Hofmann et al analyzed crown widths of treated impacted canines by comparing the image of an impacted tooth on multi-slice spiral computed tomography and the width of a canine in a dental cast [31]. The results of the study revealed a very high coincidence of measurements, assessing the mesio-distal crown width of the impacted canine. Meanwhile, Sakabe et al compared the crown width of the impacted tooth using CBCT and dental casts and found a statistically significant measurement deviation of 0.09 mm, with CBCT measurement results being larger than those of the laboratory measurements [32]. However, the authors stressed that such a small difference is clinically insignificant.
The present study supports previous studies, showing significant shorter root lengths in impacted canines (by 1.46 mm) than in contralateral canines (P<0.001). Hettiarachchi et al estimated 2.66-mm shorter root lengths on the impaction side compared with that of the matched control group (P<0.001) [10]. A similar tendency is observed in the study of Dekel et al, in which the root length of palatally and labially impacted canines were shorter by 0.9 mm and 1.3 mm, respectively, compared with the contralateral erupted canines (P<0.01) [25]. However, no significant differences were found between root length and position of contralateral canines in the labio-palatal direction in the present study. Short roots can result in an unfavorable crown-to-root ratio [10].
In this study, the incidence of dilaceration was higher than in other similar studies. In the study conducted by Dekel et al, the occurrence of palatally and labially contralateral canine dilacerations compared with that of the contralateral control group was 4: 1 and 6: 2, respectively, but the difference was also not statistically significant [25]. Meanwhile, contrasting results were observed in studies in which the control groups consisted of patients without canine impaction. In studies by Cao et al and Hettiarachchi et al, the occurrence of root dilacerations for contralateral canines was significantly more frequent than in the matched control groups [10,11]. CBCT analysis of maxillary width show that patients with palatally impacted canines have generally narrower maxilla, both skeletally and dento-alveolary, at the premolar area than do patients without impaction [33,34]. Limited space can result in a formation of dilaceration for impacted and contralateral canines. Therefore, early preventive measures, such as expansion of the dental arch and removal of the primary canine, are important in facilitating self-correction of displaced canines, reducing the incidence of impaction [35] and creating more space for the formation of canine tooth roots.
There was no statistically significant difference in the direction of root dilaceration between impacted and contralateral canines in the present study (P>0.05). The mesial root dilaceration direction was the most prevalent in contralateral canines, accounting for 69% of cases, whereas 62.5% cases of contralateral canine root dilacerations were in the distal direction. In the study of Hettiarachchi et al, the most common direction of palatally impacted canine root dilacerations was mesial, when compared with a control group (P<0.001) [10]. According to Hettiarachchi et al, mesial dilaceration direction of palatally impacted canines can be associated with the developing root’s attempt to find the least resistant pathway to growth. Due to that, the mesially dilacerated root apex is often localized between the sinus floor and the lateral wall of the adjacent nasal fossa [10].
EVALUATION OF DEPENDENCE OF IMPACTED CANINES MORPHOLOGY (CROWN LENGTH AND WIDTH, ROOT LENGTH, AND DILACERATION) ON ITS LOCALIZATION:
The second aim of this study was to evaluate whether the morphology of impacted canines is related to their localization, assuming that severity of impaction can affect canine root development. We found no statistically significant dependencies in the root lengths, dilaceration angle, direction, and length of the dilacerated part of the root and the impacted canine position in the labio-palatal direction (P>0.05). Conversely, Cao et al showed a significant dependence between the impacted canine root length and the labio-palatal position of the tooth when the average root length of labially impacted canines was shorter than that of the palatally impacted canines (12.42 (1.68) mm) and (13.54 (2.24) mm, respectively) [11].
In this study, we found root length to be significantly correlated with the position of impacted canines in the mesio-distal direction. Furthermore, impacted canine root lengths depended on the depth of impaction (the horizontal dislocation from the anticipated correct tooth’s position). Based on the study results, it could be said that longer impacted canine root length was observed in cases of larger mesio-distal and horizontal crown dislocation. It seems that with a smaller dislocation of the crown, the roots have less room for development and remain shorter.
LIMITATIONS OF THE STUDY:
There were small groups used for assessing the impact of mesio-distal localization on tooth morphology and the direction of dilaceration. Therefore, these results should be evaluated with caution. Further studies need to be done in order to make precise clinical recommendations. Moreover, another potential limitation of the study could be the wide age range of patients. Since the inclusion criterion was the complete formation of the tooth root, patients of any age who met this criterion were included.
Conclusions
The crown lengths and widths of impacted canines were significantly greater than that of contralateral canines. The root length of impacted canines was found to be significantly shorter than that of contralateral canines. Longer root length was observed in impacted canines with greater mesio-distal and horizontal dislocation.
Figures
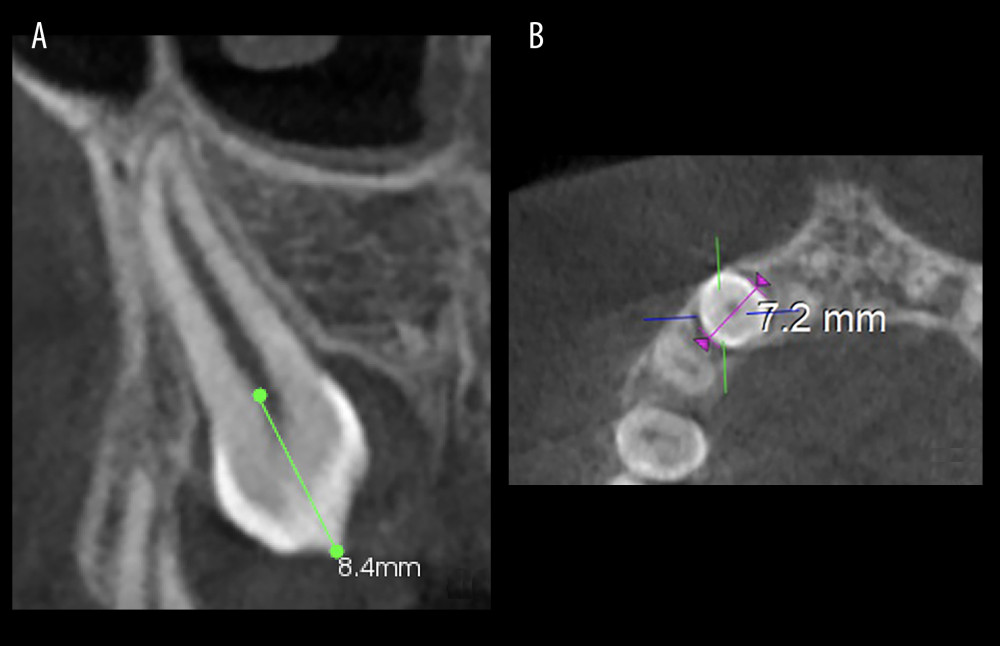 Figure 1. Measurement of the impacted canine crown. (A) Measurement of the crown length; (B) measurement of the crown width.
Figure 1. Measurement of the impacted canine crown. (A) Measurement of the crown length; (B) measurement of the crown width. 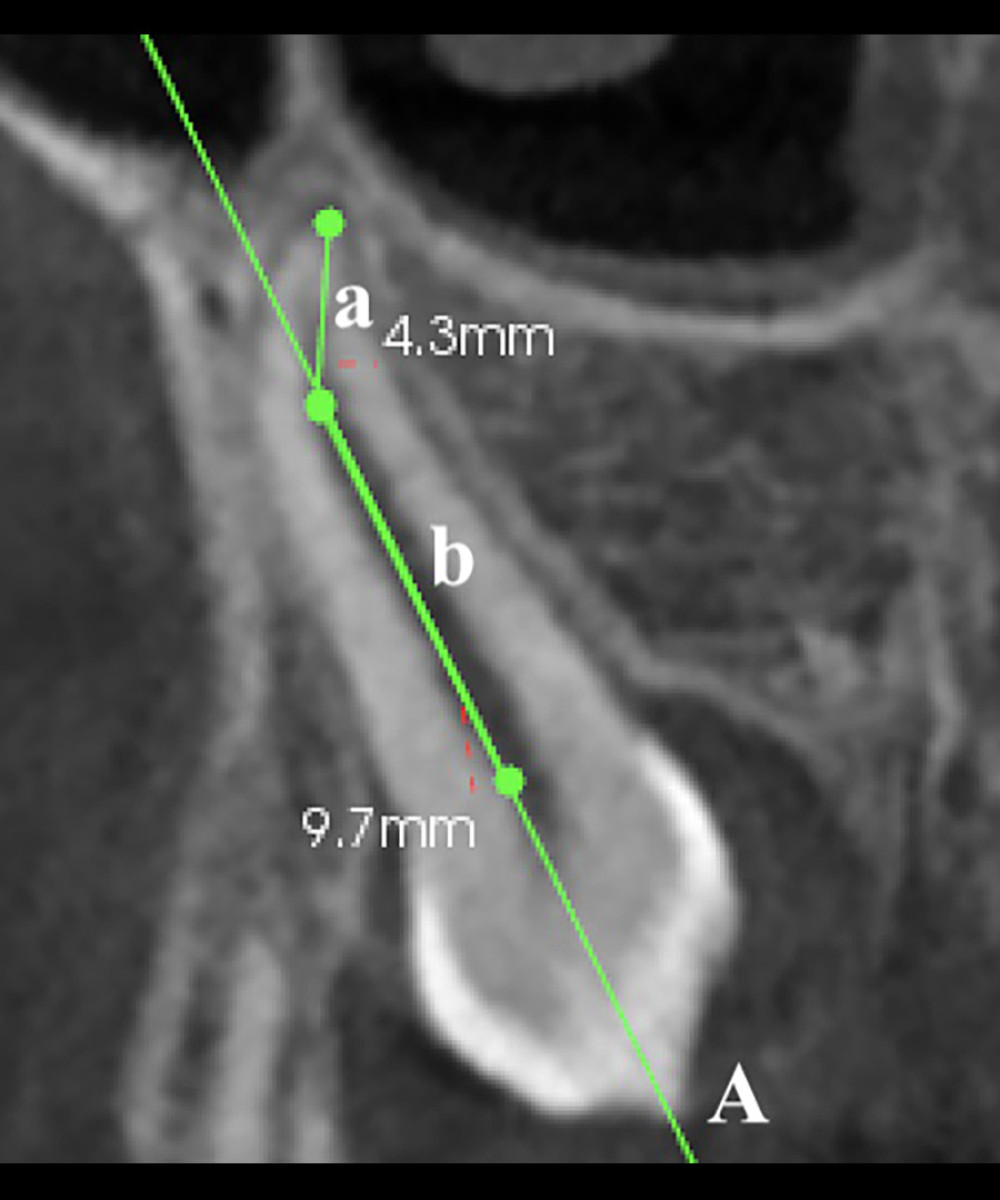 Figure 2. Measurement of dilacerated impacted canine root length. A) indicates the long axis of impacted canine tooth; a) indicates the length of the dilacerated part of the root (from root apex to the long axis of the tooth); b) indicates the length of straight part of the root (from the midpoint of the cementoenamel junction to starting point of the root curve). Total root length=a+b.
Figure 2. Measurement of dilacerated impacted canine root length. A) indicates the long axis of impacted canine tooth; a) indicates the length of the dilacerated part of the root (from root apex to the long axis of the tooth); b) indicates the length of straight part of the root (from the midpoint of the cementoenamel junction to starting point of the root curve). Total root length=a+b. 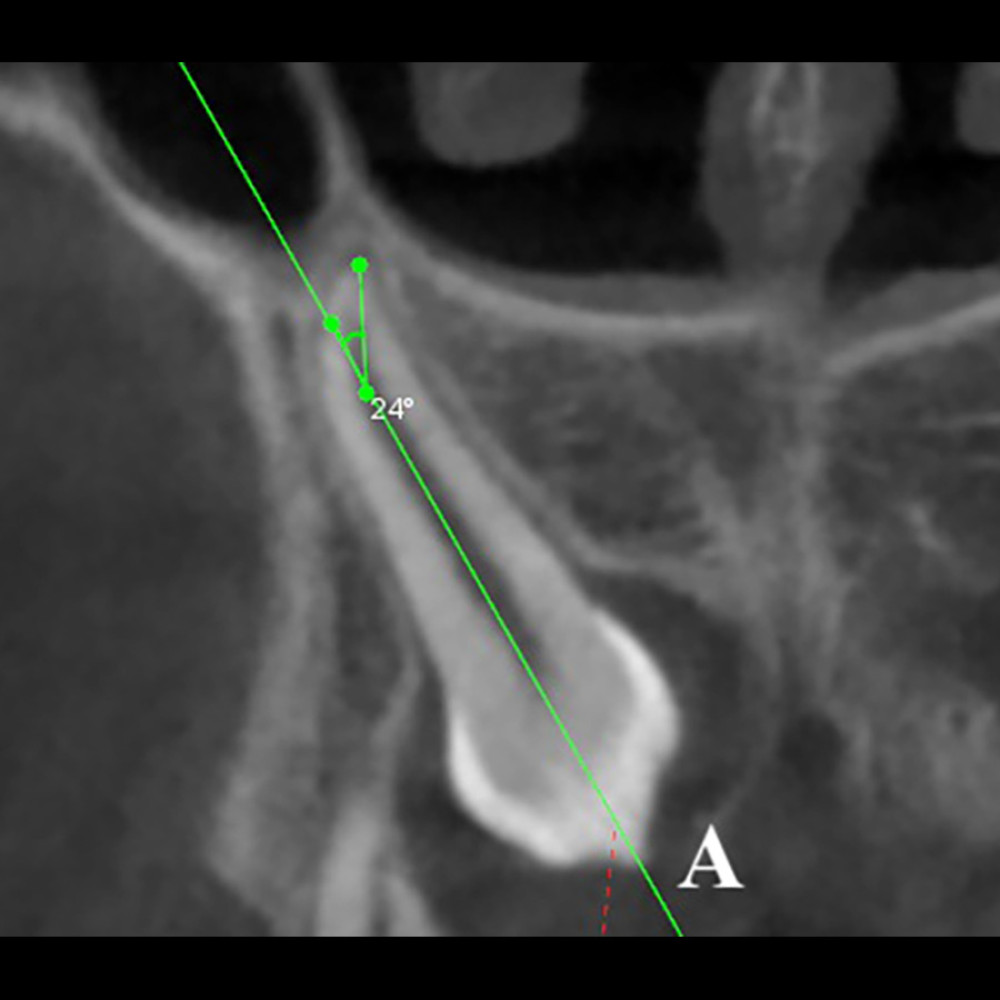 Figure 3. Measurement of the impacted canines root dilaceration angle. Line A indicates the long axis of the impacted canine.
Figure 3. Measurement of the impacted canines root dilaceration angle. Line A indicates the long axis of the impacted canine. 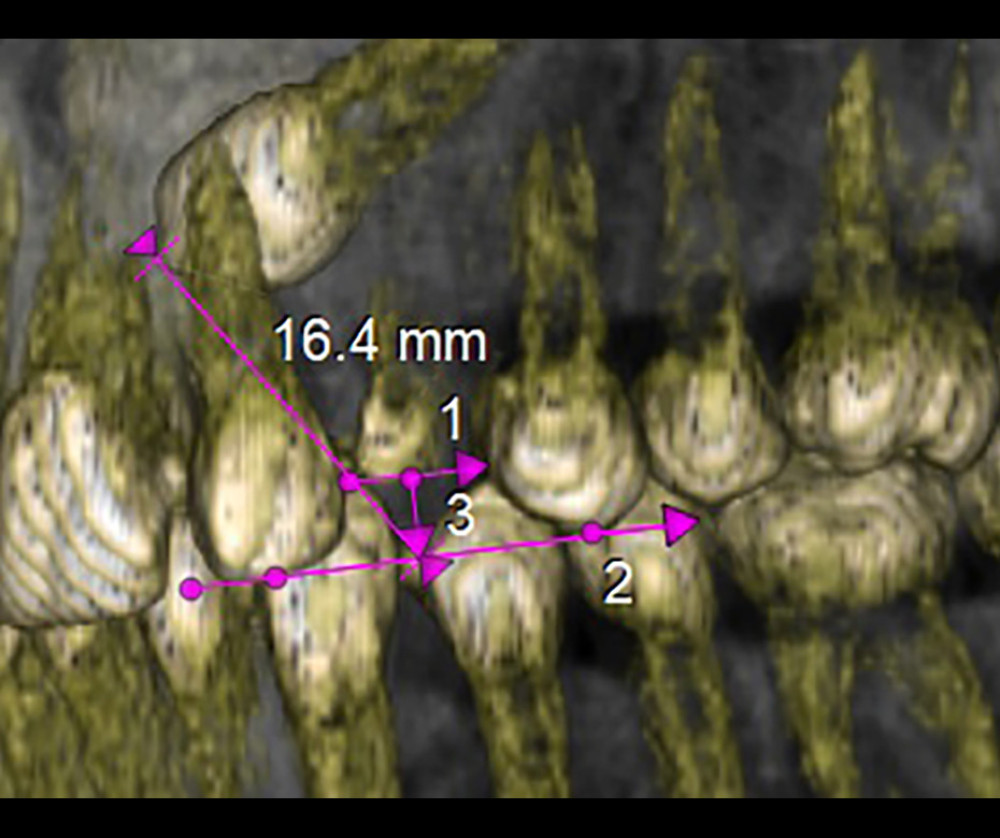 Figure 4. Measurement of the of impacted canine eruption path length. A line (1) is drawn indicating the shortest distance between the proximal contacts of the lateral incisor and the first premolar. Then a tangent (2) to the incisal edge of the lateral incisor and the buccal cusp tip of the first premolar and finally a perpendicular line (3) is drawn from the midpoint of the first line (1) to the tangent (2). The point where lines (2) and (3) intersect is defined as the correct crown cusp of the impacted canine. The eruption path length is defined as the distance between the cusp tip of the impacted tooth crown and the point of its anticipated correct position.
Figure 4. Measurement of the of impacted canine eruption path length. A line (1) is drawn indicating the shortest distance between the proximal contacts of the lateral incisor and the first premolar. Then a tangent (2) to the incisal edge of the lateral incisor and the buccal cusp tip of the first premolar and finally a perpendicular line (3) is drawn from the midpoint of the first line (1) to the tangent (2). The point where lines (2) and (3) intersect is defined as the correct crown cusp of the impacted canine. The eruption path length is defined as the distance between the cusp tip of the impacted tooth crown and the point of its anticipated correct position. Tables
Table 1. Comparison of crown length and width and root length of impacted and contralateral canines.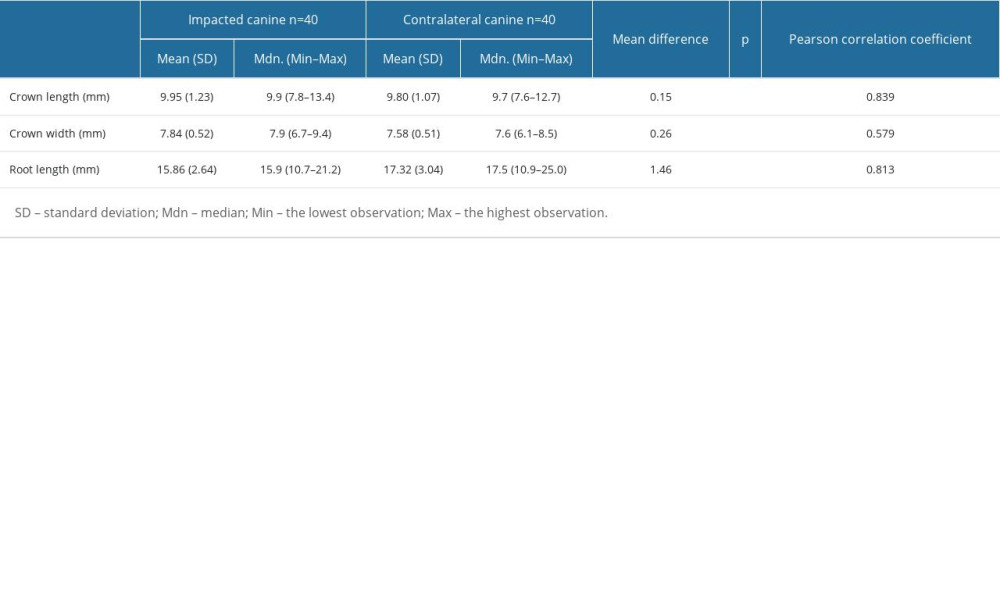 Table 2. Evaluation of root dilaceration angle and length of the dilacerated part of the root.
Table 2. Evaluation of root dilaceration angle and length of the dilacerated part of the root.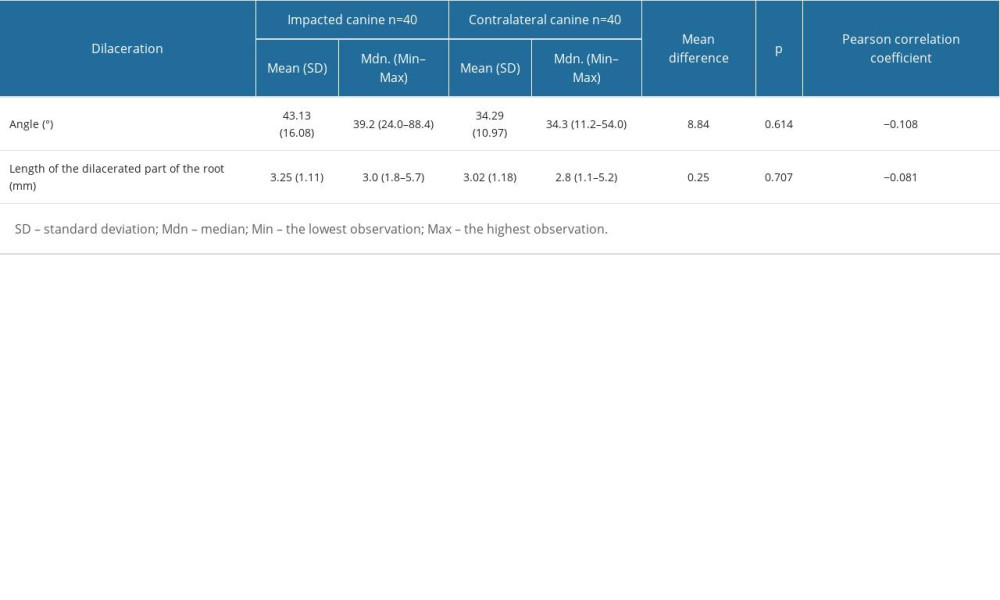 Table 3. The root dilaceration direction dependence on the eruption path length, impaction depth, and impaction height of impacted canines.
Table 3. The root dilaceration direction dependence on the eruption path length, impaction depth, and impaction height of impacted canines.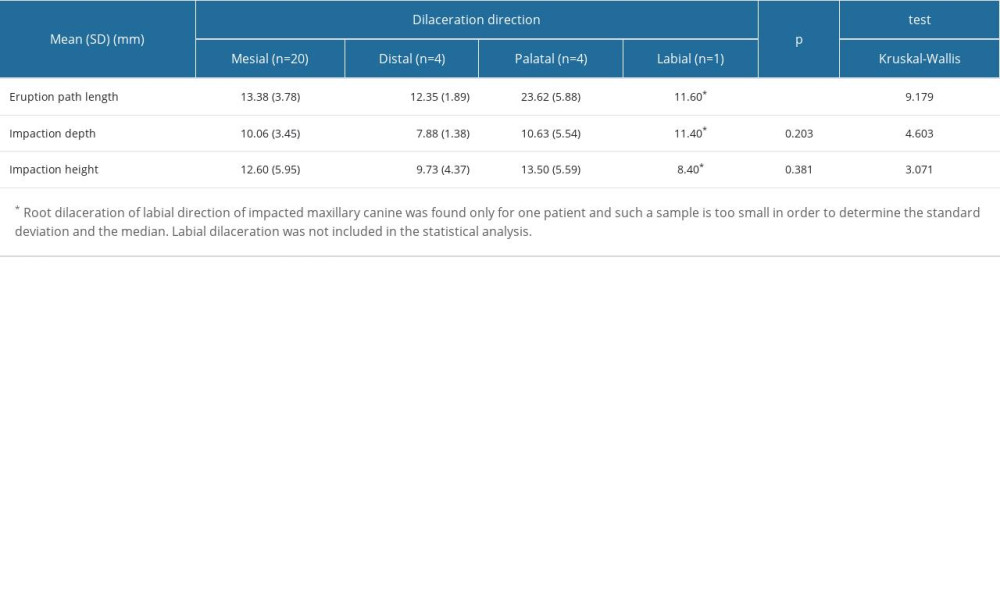
References
1. Celikoglu M, Kamak H, Oktay H, Investigation of transmigrated and impacted maxillary and mandibular canine teeth in an orthodontic patient population: J Oral Maxillofac Surg, 2010; 68(5); 1001-6
2. Aydin U, Yilmaz HH, Yildirim D, Incidence of canine impaction and transmigration in a patient population: Dentomaxillofac Radiol, 2004; 33(3); 164-69
3. Cooke J, Wang HL, Canine impactions: incidence and management: Int J Periodontics Restorative Dent, 2006; 26(5); 483-91
4. Lövgren ML, Dahl O, Uribe P, Prevalence of impacted maxillary canines – an epidemiological study in a region with systematically implemented interceptive treatment: Eur J Orthod, 2019; 41(5); 454-59
5. Yang JS, Cha JY, Lee JY, Choi SH, Radiographical characteristics and traction duration of impacted maxillary canine requiring surgical exposure and orthodontic traction: A cross-sectional study: Sci Rep, 2022; 12(1); 19183
6. Grisar K, Luyten J, Preda F, Interventions for impacted maxillary canines: A systematic review of the relationship between initial canine position and treatment outcome: Orthod Craniofac Res, 2021; 24(2); 180-93
7. Arriola-Guillén LE, Aliaga-Del Castillo A, Influence of maxillary canine impaction characteristics and factors associated with orthodontic treatment on the duration of active orthodontic traction: Am J Orthod and Dentofacial Orthoped, 2019; 156(3); 391-400
8. Amuk M, Gul Amuk N, Ozturk T, Effects of root–cortex relationship, root shape, and impaction side on treatment duration and root resorption of impacted canines: Eur J Orthod, 2021; 43(5); 508-15
9. Arriola-Guillén LE, Ruíz-Mora GA, Rodríguez-Cárdenas YA, Influence of impacted maxillary canine orthodontic traction complexity on root resorption of incisors: A retrospective longitudinal study: Am J Orthod Dentofac Orthop, 2019; 155(1); 28-39
10. Hettiarachchi PVKS, Olive RJ, Monsour P, Morphology of palatally impacted canines: A case-controlled cone-beam volumetric tomography study: Am J Orthod Dentofacial Orthop, 2017; 151(2); 357-62
11. Cao D, Shao B, Izadikhah I, Root dilaceration in maxillary impacted canines and adjacent teeth: A retrospective analysis of the difference between buccal and palatal impaction: Am J Orthod Dentofacial Orthop, 2021; 159(2); 167-74
12. da Silva Santos LM, Bastos LC, Oliveira-Santos C, Cone-beam computed tomography findings of impacted upper canines: Imaging Sci Dent, 2014; 44(4); 287-92
13. Becker A, Chaushu G, Chaushu S, Analysis of failure in the treatment of impacted maxillary canines: Am J Orthodon Dentofacial Orthoped, 2010; 137(6); 743-54
14. Lyu J, Lin Y, Lin H, New clues for early management of maxillary impacted central incisors based on 3-dimensional reconstructed models: Am J Orthod Dentofacial Orthop, 2018; 154(3); 390-96
15. Kaasalainen T, Ekholm M, Siiskonen T, Kortesniemi M, Dental cone beam CT: An updated review: Phys Med, 2021; 88; 193-217
16. Wang H, Li T, Lv C, Risk factors for maxillary impacted canine-linked severe lateral incisor root resorption: A cone-beam computed tomography study: Am J Orthod Dentofacial Orthop, 2020; 158(3); 410-9
17. Zeno KG, Ghafari JG, Palatally impacted canines: A new 3-dimensional assessment of severity based on treatment objective: Am J Orthod Dentofacial Orthop, 2018; 153(3); 387-95
18. Ali IH, Al-Turaihi BA, Mohammed LK, Alam MK, Root resorption of teeth adjacent to untreated impacted maxillary canines: A CBCT study: Biomed Res Int, 2021; 2021; 6635575
19. Schubert M, Proff P, Kirschneck C, Improved eruption path quantification and treatment time prognosis in alignment of impacted maxillary canines using CBCT imaging: Eur J Orthod, 2018; 40(6); 597-607
20. Hajeer MY, Al-Homsi HK, An evaluation of inter- and intraobserver reliability of conebeam computed tomography- and two dimensional-based interpretations of maxillary canine impactions using a panel of orthodontically trained observers: J Contemp Dent Pract, 2015; 16(8); 648-56
21. Hajeer MY, Al-Homsi HK, Alfailany DT, Murad RMT, Evaluation of the diagnostic accuracy of CBCT-based interpretations of maxillary impacted canines compared to those of conventional radiography: An in vitro study: Int Orthod, 2022; 20(2); 100639
22. Bodner L, Bar-Ziv J, Becker A, Image accuracy of plain film radiography and computerized tomography in assessing morphological abnormality of impacted teeth: Am J Orthod Dentofacial Orthop, 2001; 120(6); 623-28
23. Alfailany DT, Shaweesh AI, Hajeer MY, The diagnostic accuracy of cone-beam computed tomography and two-dimensional imaging methods in the 3D localization and assessment of maxillary impacted canines compared to the gold standard in-vivo readings: A cross-sectional study: Int Orthod, 2023; 21(3); 100780
24. Kim Y, Hyun HK, Jang KT, Morphological relationship analysis of impacted maxillary canines and the adjacent teeth on 3-dimensional reconstructed CT images: Angle Orthod, 2017; 87(4); 590-97
25. Dekel E, Nucci L, Weill T, Impaction of maxillary canines and its effect on the position of adjacent teeth and canine development: A cone-beam computed tomography study: Am J Orthod Dentofacial Orthop, 2021; 159(2); e135-e147
26. Sun H, Wang Y, Sun C, Root morphology and development of labial inversely impacted maxillary central incisors in the mixed dentition: A retrospective cone-beam computed tomography study: Am J Orthod Dentofacial Orthop, 2014; 146(6); 709-16
27. Grisar K, Piccart F, Al-Rimawi AS, Three-dimensional position of impacted maxillary canines: Prevalence, associated pathology and introduction to a new classification system: Clin Exp Dent Res, 2019; 5(1); 19-25
28. Jung YH, Liang H, Benson BW, The assessment of impacted maxillary canine position with panoramic radiography and cone beam CT: Dentomaxillofac Radiol, 2012; 41(5); 356-60
29. Al-Khateeb S, Abu Alhaija ES, Rwaite A, Burqan BA, Dental arch parameters of the displacement and nondisplacement sides in subjects with unilateral palatal canine ectopia: Angle Orthod, 2013; 83(2); 259-65
30. Naoumova J, Alfaro GE, Peck S, Space conditions, palatal vault height, and tooth size in patients with and without palatally displaced canines: A prospective cohort study: Angle Orthod, 2018; 88(6); 726-32
31. Hofmann E, Medelnik J, Keller T, Measuring mesiodistal width of impacted maxillary canines: CT-assisted determination: J Orofac Orthop, 2011; 72(1); 33-44
32. Sakabe J, Kuroki Y, Fujimaki S, Reproducibility and accuracy of measuring unerupted teeth using limited cone beam X-ray CT: Dentomaxillofac Radiol, 2007; 36(1); 2-6
33. Genc E, Karaman A, Investigation of the relationship between maxillary dimensions and labial and palatal maxillary impacted canines using cone beam computed tomography: J Stomatol Oral Maxillofac Surg, 2023; 124(1S); 101282
34. Arboleda-Ariza N, Schilling J, Arriola-Guillén LE, Maxillary transverse dimensions in subjects with and without impacted canines: A comparative cone-beam computed tomography study: Am J Orthod Dentofacial Orthop, 2018; 154(4); 495-503
35. Alyammahi AS, Kaklamanos EG, Athanasiou AE, Effectiveness of extraction of primary canines for interceptive management of palatally displaced permanent canines: A systematic review and meta-analysis: Eur J Orthod, 2018; 40(2); 149-56
Figures
Figure 1. Measurement of the impacted canine crown. (A) Measurement of the crown length; (B) measurement of the crown width.Figure 2. Measurement of dilacerated impacted canine root length. A) indicates the long axis of impacted canine tooth; a) indicates the length of the dilacerated part of the root (from root apex to the long axis of the tooth); b) indicates the length of straight part of the root (from the midpoint of the cementoenamel junction to starting point of the root curve). Total root length=a+b.Figure 3. Measurement of the impacted canines root dilaceration angle. Line A indicates the long axis of the impacted canine.Figure 4. Measurement of the of impacted canine eruption path length. A line (1) is drawn indicating the shortest distance between the proximal contacts of the lateral incisor and the first premolar. Then a tangent (2) to the incisal edge of the lateral incisor and the buccal cusp tip of the first premolar and finally a perpendicular line (3) is drawn from the midpoint of the first line (1) to the tangent (2). The point where lines (2) and (3) intersect is defined as the correct crown cusp of the impacted canine. The eruption path length is defined as the distance between the cusp tip of the impacted tooth crown and the point of its anticipated correct position. Tables
Table 1. Comparison of crown length and width and root length of impacted and contralateral canines.Table 2. Evaluation of root dilaceration angle and length of the dilacerated part of the root.Table 3. The root dilaceration direction dependence on the eruption path length, impaction depth, and impaction height of impacted canines.Table 1. Comparison of crown length and width and root length of impacted and contralateral canines.Table 2. Evaluation of root dilaceration angle and length of the dilacerated part of the root.Table 3. The root dilaceration direction dependence on the eruption path length, impaction depth, and impaction height of impacted canines. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387