04 November 2023: Clinical Research
Comparative Evaluation of Dimensional and Occlusal Accuracy of Non-Working Antagonist Casts: A Study on Different Impression Materials and 3D Printing
Bandar M.A. Al-MakramaniDOI: 10.12659/MSM.941654
Med Sci Monit 2023; 29:e941654






Abstract
BACKGROUND: The aim of this study was to assess and compare the vertical/horizontal dimensions and occlusal accuracy of non-working/opposing casts obtained from three different impression materials and 3D print cast.
MATERIAL AND METHODS: Dentulous Master models simulating a case of a fixed dental prosthesis were mounted on an articulator (control group). Opposing mandibular casts obtained from three different impression materialsand 3-dimensional print constituted test groups , ,and , respectively. Three points, anterior vertical (AV), posterior vertical (PV), and anteroposterior (AP) were compared for dimensional accuracy among casts. Occlusal accuracy was analyzed on Medit Link software at 3 teeth (#13, #17, and #27). After calculating means for each group, the differences were calculated at probability value of P≤0.05 using the single-sample t test, ANOVA, and Tukey test.
RESULTS: The dimensions were significantly different from those of the mounted master models except in Gp AL(E) and Gp AL(F) at AV dimension and Gp AL(E) at AP dimension (P>0.05). A statistically significant difference of the error of means among the 4 tested groupswere detected only at 2 dimensions (AV and PV) between the Gp AL(E) and Gp 3D-C and between Gp AL(F) and Gp 3D-C groups. Other groups showed no significant differences.
CONCLUSIONS: The opposing casts obtained from the extended-pour alginate and alginate alternative impression materials showed higher occlusal accuracy compared to conventional alginate and 3D printed casts.
Keywords: Alginates, Dental Casting Technique, Dental Occlusion, Centric, digital technology, Humans, Mandible, Models, Dental, Printing, Three-Dimensional, Software
Background
A competent and efficient occlusal scheme is essential for the health of a biologically functioning temporomandibular joint. The joint is overly sensitive to changes in occlusal load, which can assimilate during a routine fixed prosthodontic treatment (single-crown, fixed partial denture, implant-supported fixed prosthesis). It is unanimously accepted that fixed dental prosthesis (FDP) in occlusal harmony is a key objective of clinical practice [1]. Biological tolerance of an individual to occlusal changes like a premature, uneven, or high contact is extremely low, which is one of the primary reasons why chairside adjustment of FDP is invariably required despite using highly sophisticated instruments and technology. Chairside FDP occlusal adjustment can be difficult and tiring for both patient and clinician and has been reported to be one of the most frequent sources of frustration for a clinician [2], wasting valuable clinical time and risking loss of patient trust [3,4]. In extreme but common cases, it is mandatory for the clinician to remake the FDP, the financial burden of which becomes the clinician’s sole obligation. The remake rate of single-unit crowns at the scheduled delivery appointment has been reported to be 42% even after efforts at chairside adjustment [5]. Traditionally, FDPs are indirect restorations fabricated in dental laboratories by specialized dental technicians who rely heavily on the accuracy of impressions provided by the clinician. Accurate arch impressions are significantly affected by a clinician ‘s skill and techniques and are considered essential for FDP’s overall fit [6,7]. FDP misfit has been attributed to multiple factors that include poor communication (dentist and technician) [8], inadequate clinical procedures (gingival retraction) [9], and inherent inaccuracies of materials used in the laboratory (eg, dental stone, die materials, dental waxes, dental alloy, and porcelain) [8]. Irrespective of all due care and precautions exercised and despite the prior examination of prosthesis for occlusal contacts on articulated casts verifying them as correct, FDPs continued to be occlusally inaccurate upon final testing [10]. Introduction of computer-aided diagnosis and computer-aided machining (CADCAM) in dentistry with subsequent demand [11], has led to refinement of early heavy dental CADCAM systems, large scanners (3-dimensional) and multi-axis machines, to present-day automated scanners, lightweight milling machines (tabletop), and a plethora of customized software. Present-day digital dental technology using fully digital workflow have overcome many laboratory-related inaccuracies and have bettered or equaled traditional laboratory methods in terms of accuracy [12], efficiency, and methods preferred by both consumers (patients) and providers (clinicians) [13]. Highly sensitive intra-oral scanners eliminate impression material-related variations and collect analyzable data from a patient’s mouth; data are processed in the laboratory to make the restoration without use of a working model [14]. This direct method of obtaining required data from the patient is more accurate than the indirect method (from impression or a cast), but is limited by oral conditions (eg, salivary influence, space restriction, access to intricate areas) [15]. The indirect method (scanning of the cast) has also been shown to demonstrate better prosthesis adaptation than the direct method [15]. Laboratory fabrication of restorations has also been digitalized, from traditional manufacturing (casting using the lost wax technique) to sophisticated subtractive (milling) or additive manufacturing (3D printing) [16]. Additive manufacturing like 3D printing has an added advantage over milling, which allows it to fabricate anatomical structures that cannot be milled due to milling tool size limitations [17]. Other merits of 3D printing include reduced material loss, multiple/simultaneous production at a given time and replication of minute occlusal features [18]. However, the problem of clinical adjustment persists with several types of restorations manufactured digitally, some of which are harder to adjust, while others cannot be compensated, attributed chiefly to the materials used in fabrication of digitally fabricated restorations [19]. It is important to realize that all clinical adjustments are subjective (depending on the patient and clinician) and there is no accurate method that clinically determines the exact amount of adjustment that the clinician must make [20]. While the location of areas for adjustment can be identified, subjective removal can lead to loss of functional contact in occlusion (tripod cusp contact) [21], which renders the restoration functionally ineffective in terms of cusp-to-fossa contact with opposing tooth/teeth.
For achieving a technically, functionally, and esthetically acceptable indirect restoration involving occlusion, the focus has mostly centered on accurate reproduction of involved teeth (working cast), which are critically important for locating occlusal contacts and their intensity [22]. There has been little focus on the quality of opposing casts, which could be a potential source of inaccuracy in the completed restoration of the working cast. Despite having accurate definitive impression materials like addition of silicones, there are no studies that recommend the opposing or working cast to made using such impression materials. Alginate (irreversible hydrocolloid) continues to be the most common impression material used for making diagnosis, study, and opposing casts in both fixed/removable prosthesis and orthodontic related treatment procedures [23]. Despite having well established disadvantages like syneresis and imbibition, newer alginates have been formulated and marketed, with manufacturer’s claiming to have 5 days of dimensional stability (extended-pour alginates) and are scannable, which allows them access to digital workflow. Economic alternatives to alginates are called alginate alternatives (FreeAlgin), which are low-cost vinyl polysiloxane impression materials [24]. In FDP-related clinical practice, various alginates are used to make opposing arch impressions despite evidence that it contributes to occlusal discrepancies (high restorations) in final restorations [25]. All completed indirect restorations need to be evaluated on the working cast against the opposing non-working casts, which are mounted on an articulator using an inter-occlusal record with a vinyl polysiloxane bite registration material. The exquisitely detailed occlusal anatomy recorded by VPS bite registration paste is not replicated by alginate-made opposing casts, which in turn hampers accurate seating of the registration record [26]. Based on their comparative findings, authors have recommended the use of alginate alternatives for making an opposing arch impression [26]. Digitally manufactured restorations that involve locating precise occlusal contacts can be designed, and fabricated digitally (digital cast, and digital articulation) [27], but without a physical model, the complex treatment planning and appliance fabrication are challenging [28]. 3D-printed models for orthodontic purposes have been reported to have greater accuracy than milling methods [29]. The 3D printer uses four different techniques: stereolithography apparatus (SLA), triple jetting technology (PolyJet), digital light processing (DLP), and continuous liquid interface production (CLIP). SLA technology uses a laser (ultraviolet) to polymerize the drops of resin into the desired shape. The PolyJet technique is like an inkjet printer in that it applies drops of polymerizable polymer onto a building platform. The DLP technology uses a digital projector as the light source to polymerize the liquid resin layer-by-layer across the entire platform [30]. A study has compared the accuracy in terms of trueness and precision between SLA and PolyJet techniques, with better trueness in SLA models, while PolyJet models had better precision [31]. Another study has reported that the volumetric changes in casts obtained by conventional methods were significantly higher than 3D-printed models (assessed using three different printers) [32]. Another study comparing the accuracy of SLA 3D printing, digital models, and conventional dental stone casts (polyvinylsiloxane impression and dental stone), found the accuracy of SLA 3D printing was slightly inferior to that of stone casting [33]. Tooth arch measurement comparisons between digital models, 3D printing (DLP and PolyJet), and stone models (alginate impression poured with dental stone) showed high degrees of consensus for all studied parameters except crown height, with linear dimensions on printed models being less accurate than in stone models, with an error range of 0.20 to 0.30 mm [34]. Most studies on accuracy relate to the physical dimensions, which are significant for all purposes, but in relation to FDP, the most relevant is the digital occlusal contact recording, which is performed clinically using articulating foils and papers, silicone impressions, and bite waxes [35]. Digital articulation utilizing buccal scans for digital casts has been found to be at least equivalent to the conventional method in one study [36], and more accurate than conventional methods in another study [27,37]. Interpretation of digital occlusions was well defined in a study based on T-scan analysis in terms of identifying artifacts, pressure areas, occlusal threshold, and high points [35].
Studies evaluating use of alginate alternatives and extended-pour alginate as opposing cast to the digitally fabricated restoration (working cast) in terms of occlusal accuracy are lacking; therefore, the present study aimed to compare the occlusal accuracy of opposing casts generated through conventional alginate, extended-pour alginate, alginate alternative impression material, and 3D print cast. Our main objective was to determine which material is most suitable as an opposing cast so that the smallest possible errors in occlusion are incorporated during indirect restoration fabrication. We hypothesized that there would be significant differences between diverse materials based on different chemical ingredients. Alternately, the null hypothesis was that there would be no significant differences between opposing casts generated using these four varied materials/techniques in terms of occlusal accuracy.
Material and Methods
ETHICS:
This in vitro study was proposed to and approved by the Scientific Research Unit, College of Dentistry, Jazan University on 24th March 2022 (Reference No. CODJU-2203F).
STUDY DESIGN:
This in vitro study utilized a comparative study approach with strict adherence to standardization of materials/techniques/instruments/procedures used during fabrication of the test samples. The measurement of data was done by a calibrated examiner who was blinded to the groups/study outcome and test sample identity.
OPERATIONAL DEFINITION:
The working cast was defined as any cast that replicated the prepared tooth and ridge area in a quadrant/arch. The opposing or non-working cast was defined as any cast that replicated the opposite arch of the working cast and was used to determine the occlusion of the restoration after completion. 3D printing was defined as a procedure which prepared a physical object from a previously scanned object by laying down multiple layers and subsequently polymerizing them in succession.
ESTIMATION OF SAMPLE SIZE:
Assuming the study power (85%) with an alpha error of 5%, the minimum sample size estimated for the study (5 groups) through power analysis [38] was kept as ten specimens per group. One extra specimen was added to replace any faulty specimen.
MATERIAL SELECTION, SAMPLE PREPARATION, AND GROUPING:
All materials and instrumentation with their specification are presented in Table 1. An organized layout of the study is presented in a flowchart (Figure 1). To simulate a clinical case scenario, a maxillary/mandibular typodont model (Frasaco GmbH, Tettnang, Germany) containing a full set of typodont teeth (teeth – acrylic, soft tissues – silicone rubber) were used to represent the master model (Control) against which comparisons were made. Maxillary tooth number 15 (right second premolar) was removed to represent a missing tooth, with adjacent teeth (#14 and #16) serving as abutments for the FDP. Standard all-ceramic tooth preparation was done for adjacent teeth (#14 and #16) using a flat-end diamond bur (6856 314 016, Komet, Germany) on a high-speed hand piece (KaVo do Brazil Ind. Com. Ltd., Joinville, SC, Brazil) mounted to a dental cast surveyor (A3005 Surveyor Type A; Dentalfarm). Tooth preparation was done according to the standard principles of tooth preparation [39] (Table 1 shows tooth preparation specifications), which was verified through a multi-sectional putty index (addition of silicone) and a graduated (in millimeters) periodontal probe. An opposing mandibular typodont model that contained a full set of teeth was used to represent the opposing cast for the master model. The maxillary and mandibular Typodont models were then scanned with a benchtop scanner (Medit, Model MD-ID0300, Medit Corp., Seoul, South Korea), following which the data was transferred to a 3D printer (ST-1600, Satori Ltd., London, UK) to print 1 maxillary and 1 mandibular solid model using photopolymerized liquid resin (NextDent, Vertex-Dental B.V., Soesterberg, The Netherlands). The fabrication of solid models not only overcame the problem of loose typodont teeth affecting the scan process, but also represented the routine clinical and laboratory procedures when digital data of the impression of the patient are transferred to the dental laboratory. These 3D maxillary and mandibular models represented the master models, which were mounted on predetermined vertical dimension of occlusion on a semi-adjustable articulator (BioArt A7 plus, São Carlos, São Paulo, Brazil) (Figure 2). The maxillary master model was mounted using a compatible facebow (BioArt A7 plus, São Carlos, São Paulo, Brazil), while the mandibular master model was mounted in the maximum intercuspation position using hand articulation, with the incisal pin of the articulator touching the incisal guide table at zero inclination on the anterior guidance table. Three reproducible and repeatable indentations were made on the maxillary master model (A1 – anterior between the maxillary central incisors; P1 – posterior at maxillary right first molar, and P2 – posterior between maxillary right 1st and 2nd premolars) (Figure 3). Similarly, three indentations were made on the mandibular master model (A2 – anteriorly between mandibular central incisors parallel to the anterior indentation made in the maxillary master model; P3 – posterior at mandibular right first molar, and P4 – posterior between mandibular right 1st and 2nd premolars). All indentations were prepared just 2 mm below the gingival margin to enable registering the indentation in the mandibular master model with the impression.
FABRICATION AND MOUNTING OF OPPOSING (NON-WORKING) AND 3D-PRINTED CASTS:
A metallic rim lock perforated (mandibular) stock tray was selected to fit on the mandibular typodont model with at least a gap of 4 mm between the border of the tray and the surfaces of the teeth on either side. A total of ten perforated impression trays were used (size 6) to make ten conventional impressions for each group: Hydrogum Alginate (Conventional) [Gp AL(C)], Hydrocolor 5 (Extended-Pour Alginate) [Gp AL(E)], and FreeAlgin (Alginate Alternative) [Gp AL(F)]. All impressions were poured with vacuum (Mix-R, Dentalfarm, Torino, Italy)-mixed stone (type IV) (Elite Rock, Zhermack, Italy), and poured on the vibrator (Dentalfarm, Italy) according to the manufacturer’s recommendations. The mandibular master model was then scanned ten times with a Medit intra-oral scanner (Medit i700, Medit, Seoul, South Korea) and sent to the production laboratory for printing [three-dimensional (3D)] using a 3D printing machine (ST-1600, Satori, Ltd., London, UK). The stereolithography (SLA) machine printed ten models (3DCAST) using the photopolymerized liquid resin (JAMG HE, LOT No. WX353N02, Shenzhen, Guangdong, China), which represented the fourth test group for the study [Gp 3D-C]. In total, forty mandibular models obtained under four diverse groups (10 each) represented four different types of opposing casts: two from the alginate-related impression, 1 alginate alternative, and 1 3D-printed cast.
Mounting of mandibular models for each group against previously mounted maxillary master model was done using silicone bite registration paste (Maxill, Cortland, OH, USA), which was injected on a bite tray to make a bite registration record at the maximum intercuspation position. The bite registration record was used for mounting the mandibular stone casts made from the 3 impression materials, Hydrogum alginate (conventional), Hydrocolor 5 (Extended-Pour Alginate), FreeAlgin (Alginate Alternative), and the 3D-printed models (3DCAST) – with the upper maxillary master model being fixed standard (for all) on the semi-adjustable articulator (Figure 4). A 2-sided bite registration tray ensured standardization of interocclusal records.
MEASUREMENTS AND DATA EVALUATION, COLLECTION, AND ANALYSIS:
The distances between the pre-marked master models mounted on the articulator were measured for 3 different dimensions – A1–A2: Anterior Vertical (midline) for measurement of vertical changes anteriorly; P1–P3: Posterior Vertical for measurement of vertical changes posteriorly; and P1–P4: Diagonal posterior for measurement of anterior-posterior (horizontal) changes. The mounted maxillary and mandibular master models on the semi-adjustable articulator were further scanned with a benchtop 3D scanner (MD-ID0300, SN 1V19045DE406, Medit Corp., Seoul, South Korea). Three scan files were obtained for each mounted model (upper jaw, lower jaw, and bite for occlusion) at 1 time for one sample in each group. For scanning the bite, a customized compatible attachment was used for mounting the articulator on the benchtop scanner for repeatable and accurate positioning of all samples. Each cast was oriented to a level where the occlusal plane would lie in the same plane for each sample. For each case, the three files were imported into the Medit Link software (Medit Link v 2.4.4; Medit, Seoul, Republic of Korea) for measurement. The manual alignment tool in the software was used aligning of the maxillary and mandibular jaws using the bite (Figure 5). Once the digital models showed the desired occlusal contacts, the measurement tool was selected and used to measure the anterior vertical (A1–A2), posterior vertical (P1–P3), and anterior-posterior (P1–P4) distances between the digital master models and digital opposing casts of each group (Figure 6). Each distance on the articulated master models was measured ten times. Average values were calculated and used as the control to compare it with the four groups of the mounted maxillary master model and the mandibular casts in each group: Gp AL(C), Gp AL(E), Gp AL(F), and Gp 3D (C).
OCCLUSAL ACCURACY:
The occlusal contacts for each opposing cast in each group against the working cast (master model) were analyzed using Occlusal Analysis tools in Medit Link software (Medit Link v 2.4.4; Medit, Seoul, Republic of Korea) (Figure 7). The software system analyzes occlusion while displaying the results in a color map that has various intensities of blue and red with an intervening single color of green. The occlusal areas that are within the acceptable range of tolerance are shown in green [40,41]. The occlusal contacts in the green zone showing a deviation value of −0.100 to + 0.100 were considered the acceptable occlusal contacts. Areas that are high (occlusal interferences) are depicted as higher positive values on the screen with a change in color intensity (intensity signifies the amount). Non-interferences are colored with grades of blue color and have negative values.
All digital measurements were done by a single calibrated investigator who was blinded (file names and codes and the outcome of the study). Intra-rater reliability was achieved prior to measuring the final samples, during which ten samples from different groups were randomly selected and analyzed by the investigator. Occlusal measurements were done on three separate days for samples in the reliability test. Intra-rater reliability for measurement of the scanned images and occlusal accuracy was 0.911 and 0.897, respectively (good) [95% confidence interval, 4 levels of precision] [42]. The reproducibility of the measurements was analyzed using SPSS version 24.0 (SPSS 24.0; SPSS, Inc., Chicago, Illinois, USA), thereby calculating the intra-class correlation coefficient (ICC), which was also high (0.901).
STATISTICAL ANALYSIS:
All data were coded, corrected, and refined within Microsoft excel sheets, then data were entered into SPSS version 24.0 (SPSS 24.0; SPSS, Inc., Chicago, Illinois, USA) for statistical analysis and testing. The test for distribution of the data was performed using the Shapiro-Wilk test. Descriptive statistics calculations produced mean and standard deviations. A one-sample
Results
The mean and standard deviation of anterior vertical, posterior vertical, and anterior-posterior measurements (in millimeters) on the articulated master model and the four tested groups – Gp AL(C), Gp AL(E), Gp AL(F), and Gp 3D (C) – are presented in Table 2. Gp AL(C) and Gp 3D-C showed statistically significant differences in anterior vertical, while all groups showed significant differences in means for posterior vertical. For anterior-posterior dimensions, only Gp AL(E) did not show any significant differences in means from the master model. Both Gp AL(C) and Gp 3D-C showed significant differences in means for all measured dimensions. Pairwise comparison using the
Occlusal accuracy was determined by observing the relative occlusal contacts between teeth number 13, 17, and 27 between articulated master models and 4 different opposing casts/groups. Occlusal contacts falling in the green zone (−0.100 to + 0.100) were ideal and clinically acceptable. For master models, all 3 teeth (13, 17, and 27) showed contacts in the green zone. When opposed by conventional alginate [Gp AL(C)], all occlusal contacts were ideal (green zone) except for 1 sample at tooth number 27, where it was in the blue zone (−0.200 to −2.00). When opposed by a cast made from extended-pour alginate Gp AL(E), 3 samples showed occlusal contacts in the blue zone at tooth number 27 (−0.200 to −2.00). When the master model was opposed by cast obtained from alternative alginate or alginate-free AL(F), 4 samples out of 10 were in the blue zone (−0.200 to −2.00) at tooth number 27. When the master model was opposed by the same opposing cast Gp 3D-C, 4 samples showed blue zone contacts (−0.200 to −2.00) at tooth number 3. To summarize, the opposing casts obtained in Gp AL(C) showed better occlusal distribution since most contacts at the 3 investigated locations (13, 17, and 27) were in the green zone, followed by Gp AL(E), Gp AL(F), and Gp 3D-C.
Discussion
STRENGTHS AND LIMITATIONS OF THE STUDY:
Very few studies have assessed the occlusal accuracy of digitally derived whole casts and ours is first to study the effect of the opposing cast on the occlusion. Limitations of the present study include the in vitro design and using ideal models rather than the patient’s occlusion, which varies individually. Another limitation is that only one brand of scanner was used with a single brand of 3D printer, while there are many commercially available. The study lacks simulation of oral conditions that have been shown to influence the scanning procedure (eg, saliva, tongue, light, access). This necessitates further studies which evaluate the accuracy of other scanners and printers in conditions such as those inside the oral cavity.
CLINICAL IMPLICATIONS:
These findings support the benefits of using 3D-printed models that should be limited to diagnosis, treatment planning, and fabrication of temporary restorations only, and their use as antagonist/opposing cast may result in significant occlusal errors in the definitive restoration and/or prosthesis.
Conclusions
Within the limitations of this study, the following conclusions can be drawn:
Figures
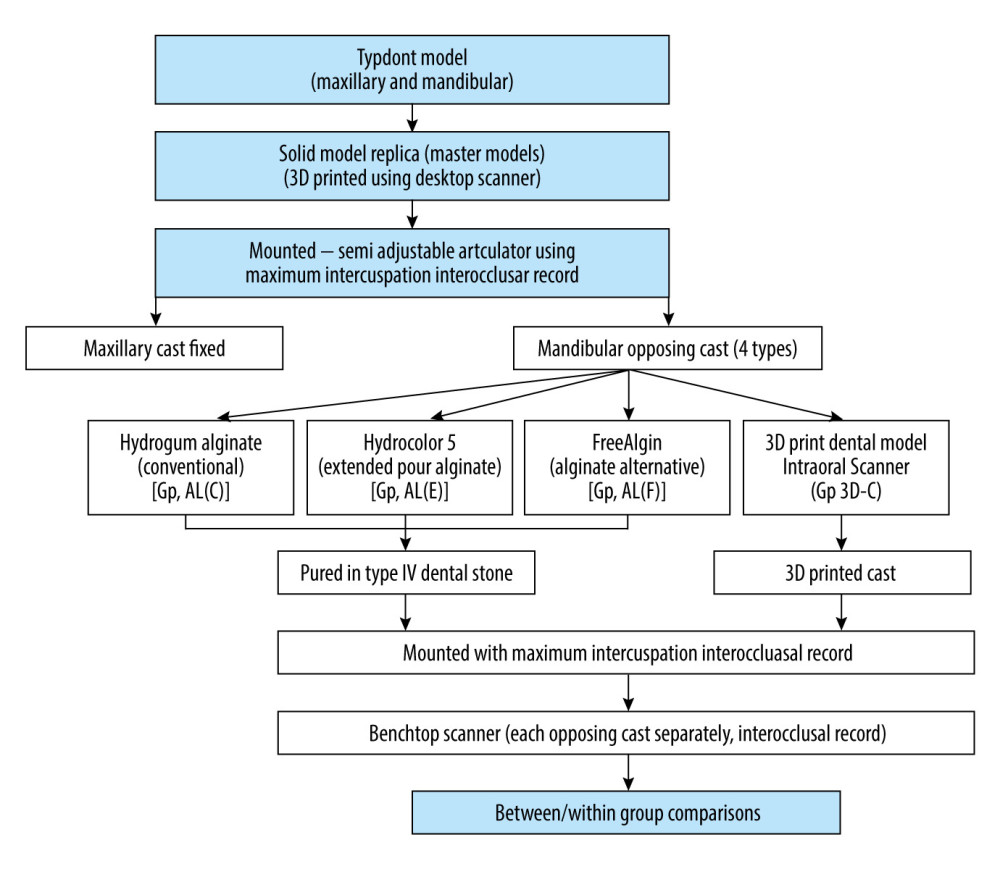 Figure 1. Flow chart showing sample preparation and group distribution. Figure created using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation).
Figure 1. Flow chart showing sample preparation and group distribution. Figure created using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation). 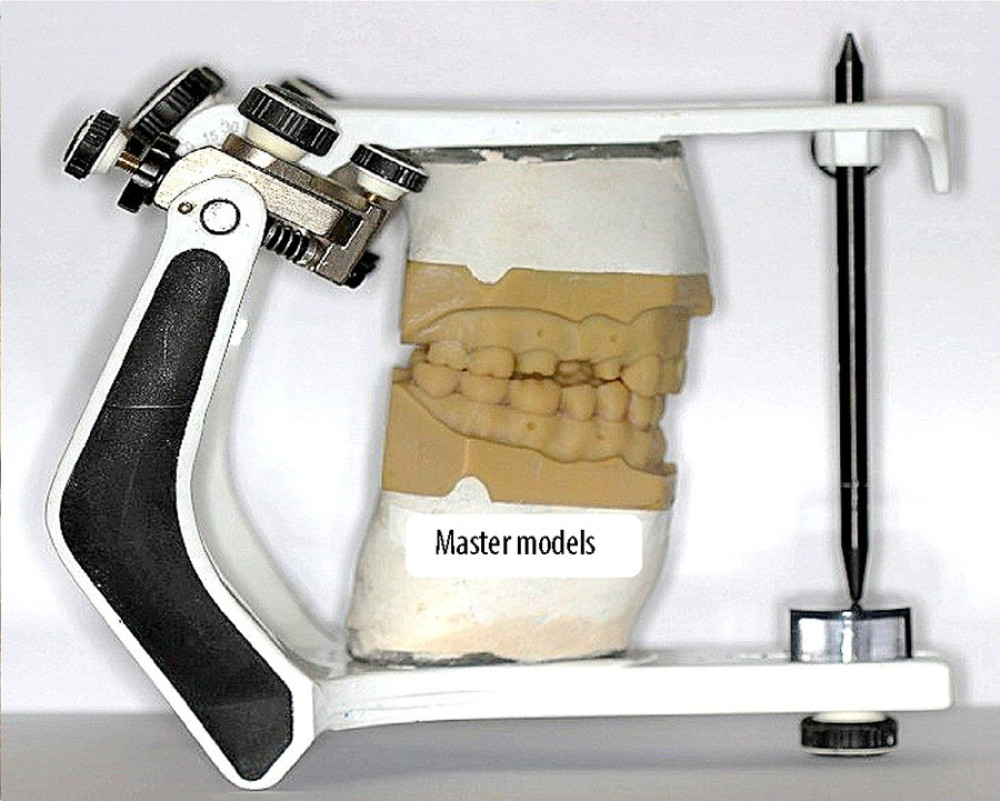 Figure 2. Master models mounted on a semi-adjustable articulator (BioArt A7 plus). Figure edited and labelled using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation).
Figure 2. Master models mounted on a semi-adjustable articulator (BioArt A7 plus). Figure edited and labelled using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation). 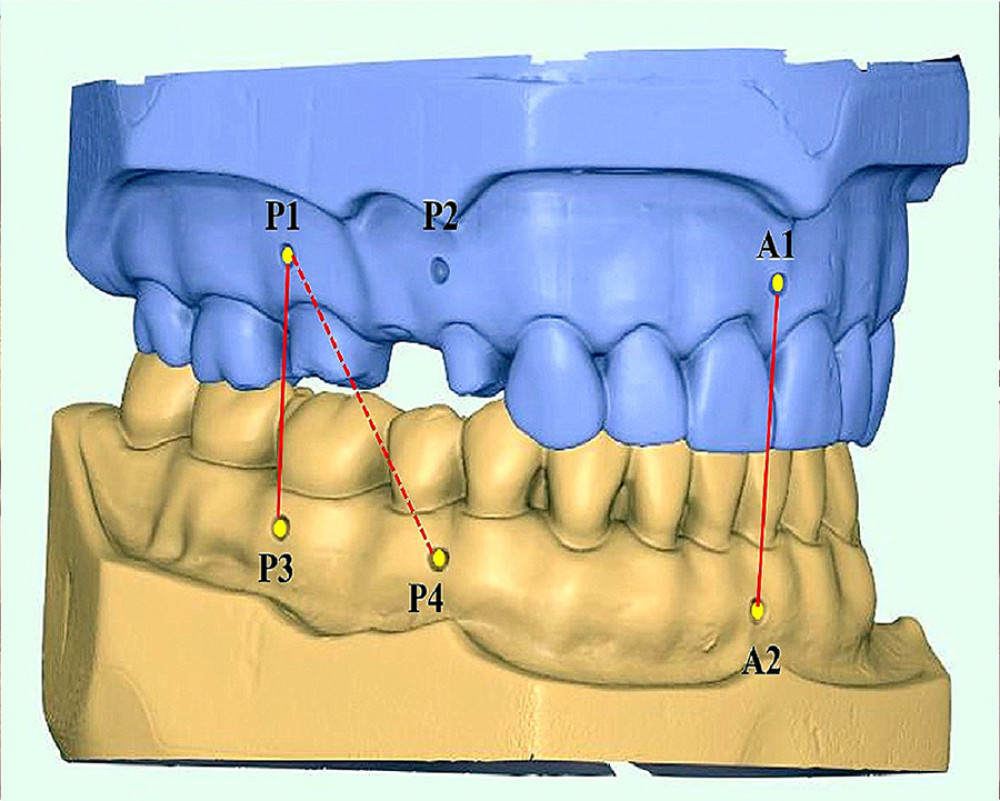 Figure 3. Three repeatable and reproducible indentations made on the maxillary and mandibular master models with A1 between maxillary central incisors, A2 between mandibular central incisors, P1 at right maxillary first molar, P2 between maxillary right first and second premolar, P3 at mandibular first molar and P4 between mandibular right first and second premolar. Figure edited and labelled using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation).
Figure 3. Three repeatable and reproducible indentations made on the maxillary and mandibular master models with A1 between maxillary central incisors, A2 between mandibular central incisors, P1 at right maxillary first molar, P2 between maxillary right first and second premolar, P3 at mandibular first molar and P4 between mandibular right first and second premolar. Figure edited and labelled using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation). ![Four different mandibular casts mounted to the same maxillary master model cast on the semi-adjustable articulator using a maximum intercuspation bite registration record. Clockwise right - Hydrogum Alginate (Conventional) [Gp AL(C)], Hydrocolor 5 (Extended-Pour Alginate) [Gp AL(E)], 3D Print Dental Model (Gp 3D-C), FreeAlgin (Alginate Alternative) [Gp AL(F)]. Photographs taken using Digital Single-Lens Reflex (DSLR) (Canon EOS 700D) with 100 mm macro lens) with/without ring flash. Compiled Figure created using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation)](https://jours.isi-science.com/imageXml.php?i=medscimonit-29-e941654-g004.jpg&idArt=941654&w=1000) Figure 4. Four different mandibular casts mounted to the same maxillary master model cast on the semi-adjustable articulator using a maximum intercuspation bite registration record. Clockwise right - Hydrogum Alginate (Conventional) [Gp AL(C)], Hydrocolor 5 (Extended-Pour Alginate) [Gp AL(E)], 3D Print Dental Model (Gp 3D-C), FreeAlgin (Alginate Alternative) [Gp AL(F)]. Photographs taken using Digital Single-Lens Reflex (DSLR) (Canon EOS 700D) with 100 mm macro lens) with/without ring flash. Compiled Figure created using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation)
Figure 4. Four different mandibular casts mounted to the same maxillary master model cast on the semi-adjustable articulator using a maximum intercuspation bite registration record. Clockwise right - Hydrogum Alginate (Conventional) [Gp AL(C)], Hydrocolor 5 (Extended-Pour Alginate) [Gp AL(E)], 3D Print Dental Model (Gp 3D-C), FreeAlgin (Alginate Alternative) [Gp AL(F)]. Photographs taken using Digital Single-Lens Reflex (DSLR) (Canon EOS 700D) with 100 mm macro lens) with/without ring flash. Compiled Figure created using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation) 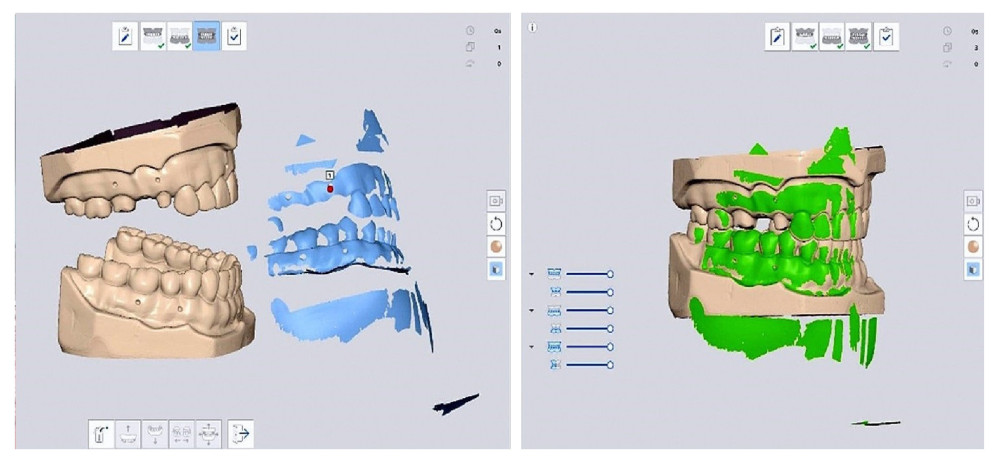 Figure 5. Digital articulation between the maxillary and mandibular digital casts showing the casts separated and in articulation position after using the manual alignment tool in the software (Medit Link). Compiled Figure created using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation).
Figure 5. Digital articulation between the maxillary and mandibular digital casts showing the casts separated and in articulation position after using the manual alignment tool in the software (Medit Link). Compiled Figure created using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation). 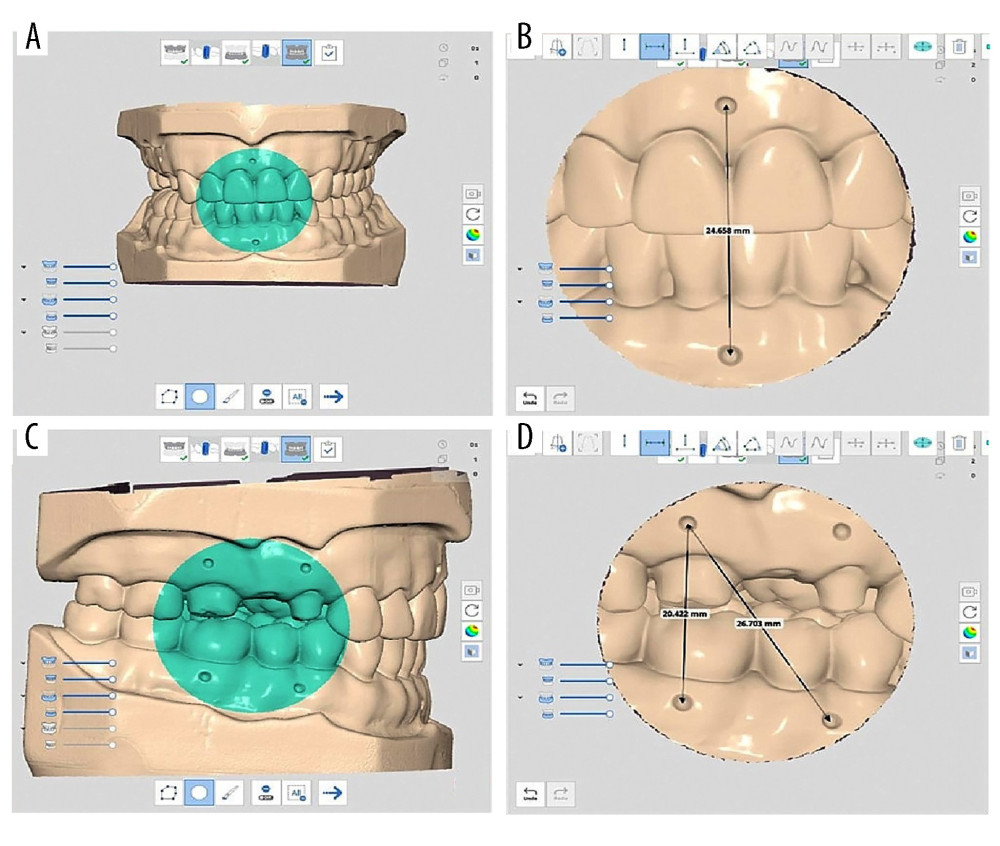 Figure 6. Digital measurement of reference points (A) Identifying the measuring landmarks (B) cropping the image and measuring the distance between anterior points (A1–A2) (C) identifying the posterior landmark area (D) cropped image to measure the posterior distances (P1–P3) and (P1–P4). Compiled Figure created using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation).
Figure 6. Digital measurement of reference points (A) Identifying the measuring landmarks (B) cropping the image and measuring the distance between anterior points (A1–A2) (C) identifying the posterior landmark area (D) cropped image to measure the posterior distances (P1–P3) and (P1–P4). Compiled Figure created using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation). 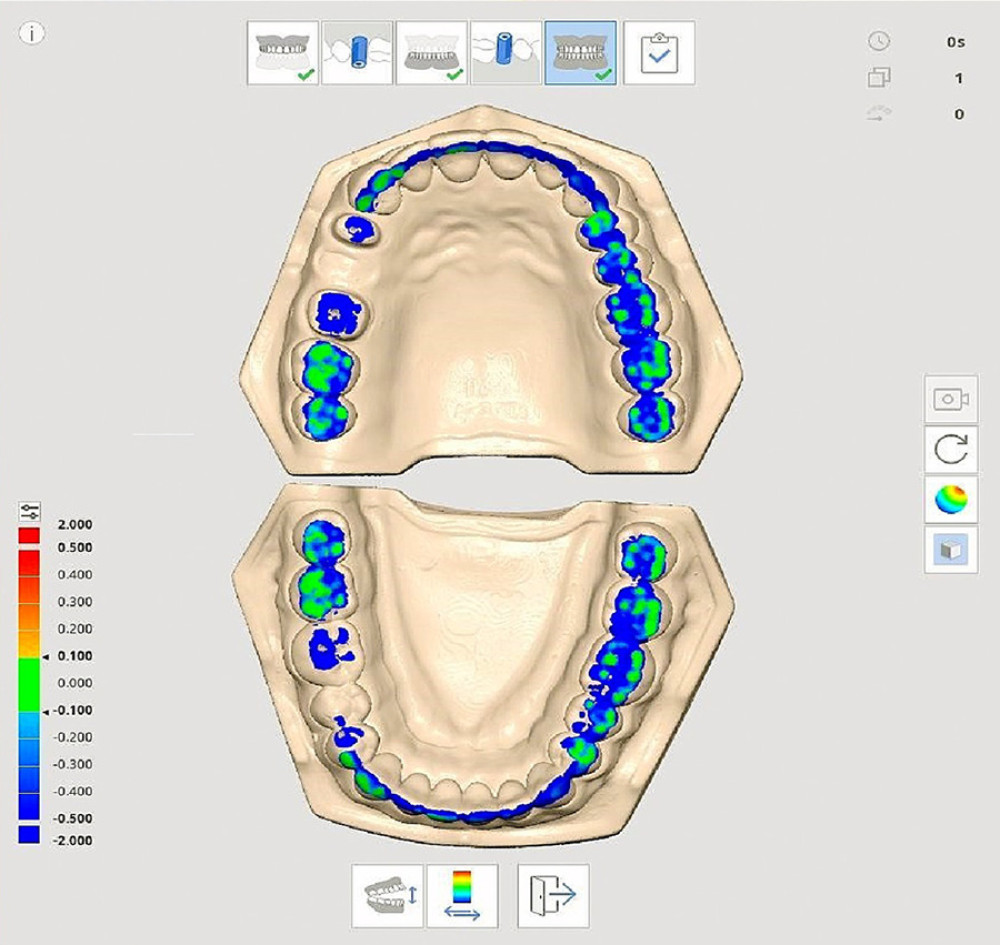 Figure 7. Digital occlusal analysis of articulated exemplary master model using Occlusal Analysis tool (Medit Link software) [Color green indicates occlusal contacts and the degree of occlusal contact (pressure) while blue indicates no contact. Compiled Figure created using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation).
Figure 7. Digital occlusal analysis of articulated exemplary master model using Occlusal Analysis tool (Medit Link software) [Color green indicates occlusal contacts and the degree of occlusal contact (pressure) while blue indicates no contact. Compiled Figure created using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation). Tables
Table 1. Armamentarium, materials used and group distribution in the study.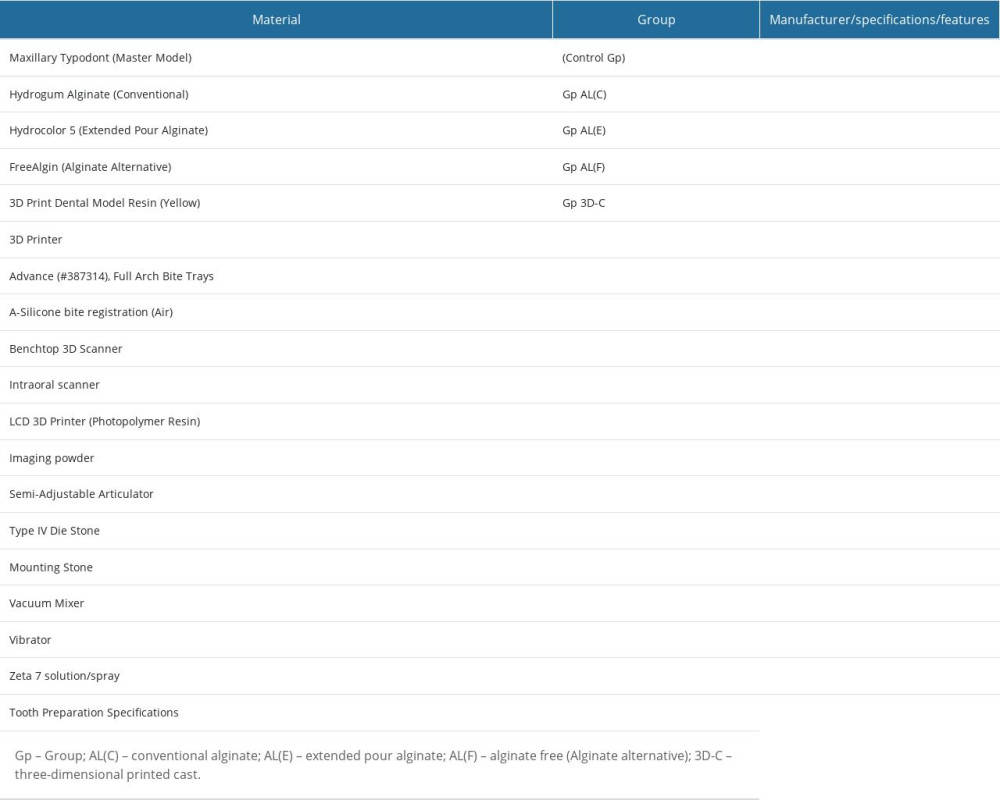 Table 2. Comparative differences in the mean value measurements (millimeters) between the articulated master model and the 4 tested groups.
Table 2. Comparative differences in the mean value measurements (millimeters) between the articulated master model and the 4 tested groups.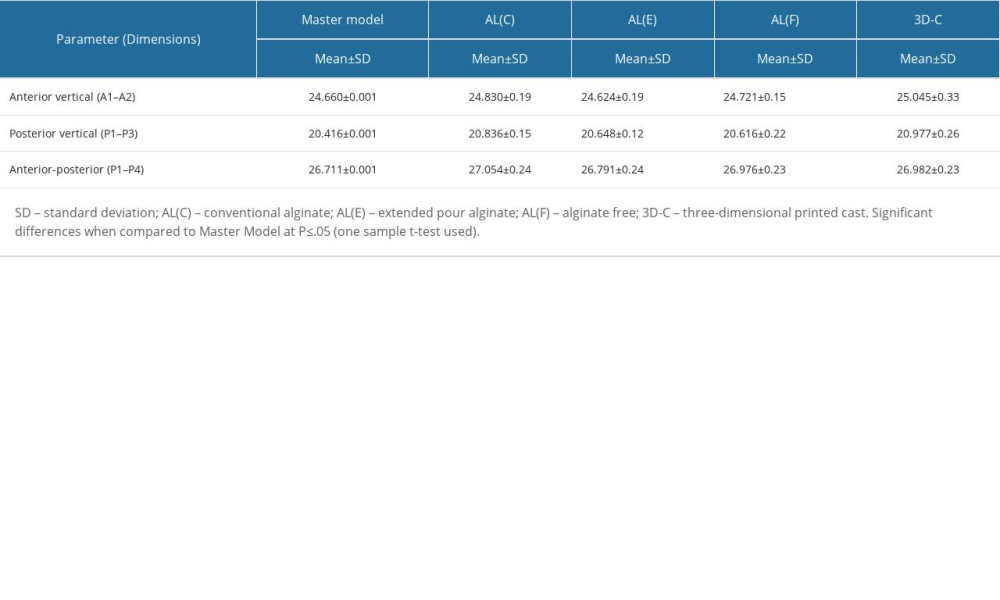 Table 3. One-sample t test showing the dispersion of the measurements and relative differences of each group measurement against the test values of the Articulated Master model.
Table 3. One-sample t test showing the dispersion of the measurements and relative differences of each group measurement against the test values of the Articulated Master model.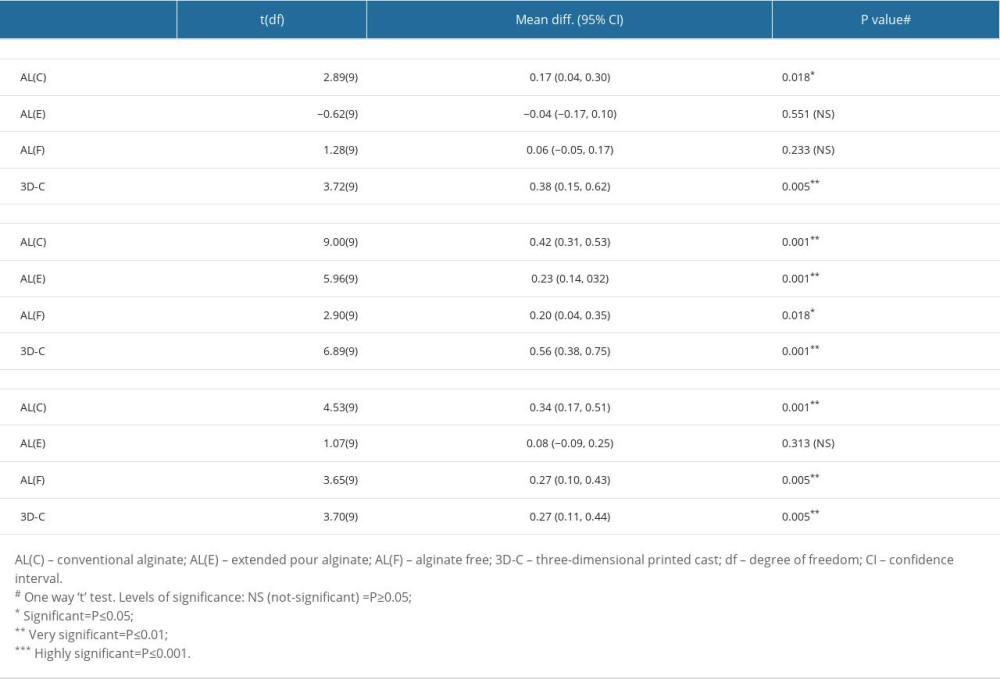 Table 4. Comparative mean error at 3 observed measurements for each group relative to the reference master model (mm).
Table 4. Comparative mean error at 3 observed measurements for each group relative to the reference master model (mm).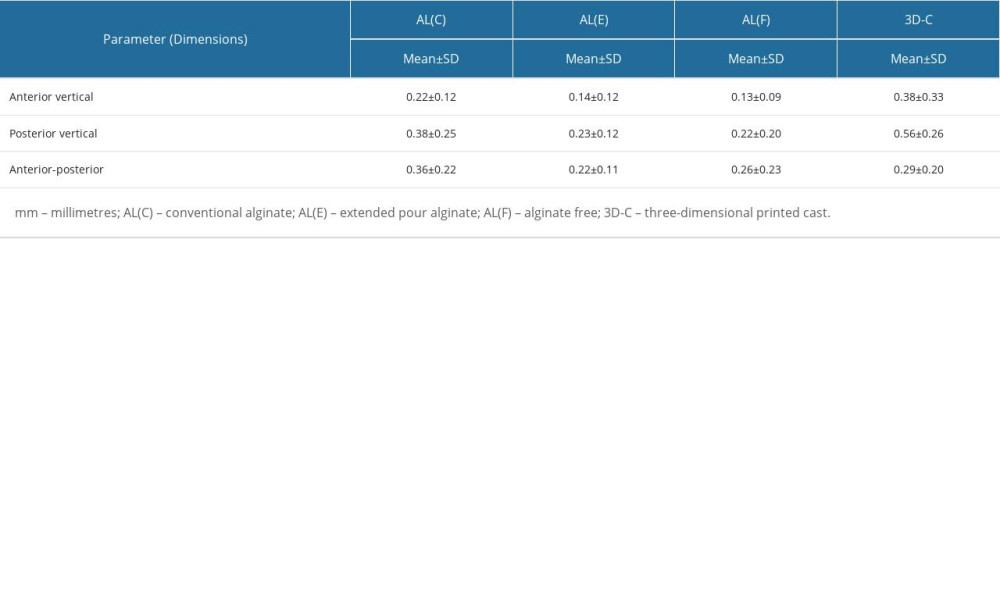 Table 5. Comparative differences of mean errors for various measurements among studied groups in relation to the reference master model.
Table 5. Comparative differences of mean errors for various measurements among studied groups in relation to the reference master model.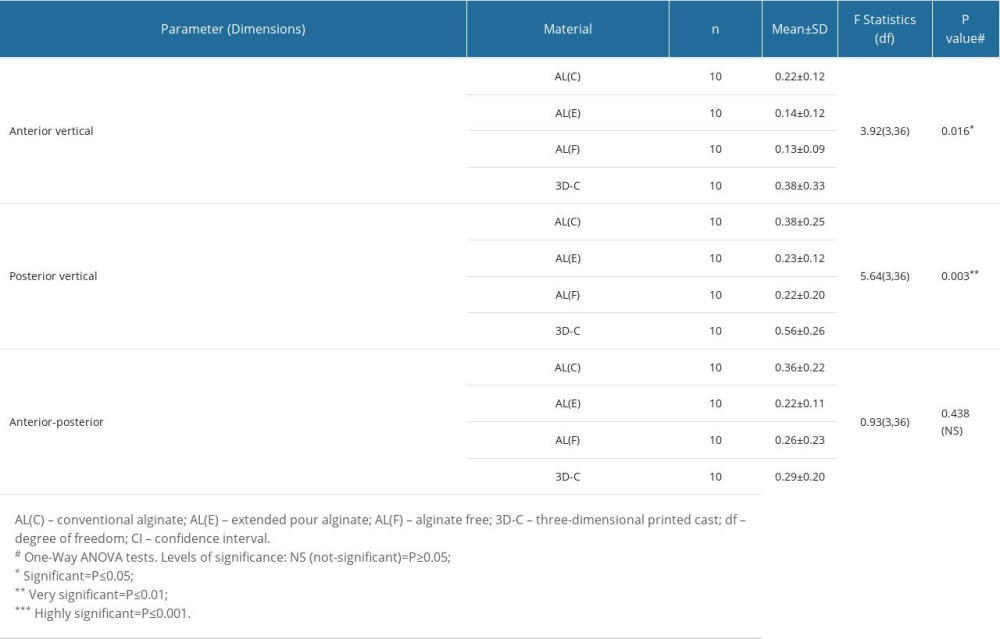 Table 6. Multiple pairwise comparisons of the accuracy of the articulated casts by the 3 impression materials and 3D printed system using Tukey’s HSD test.
Table 6. Multiple pairwise comparisons of the accuracy of the articulated casts by the 3 impression materials and 3D printed system using Tukey’s HSD test.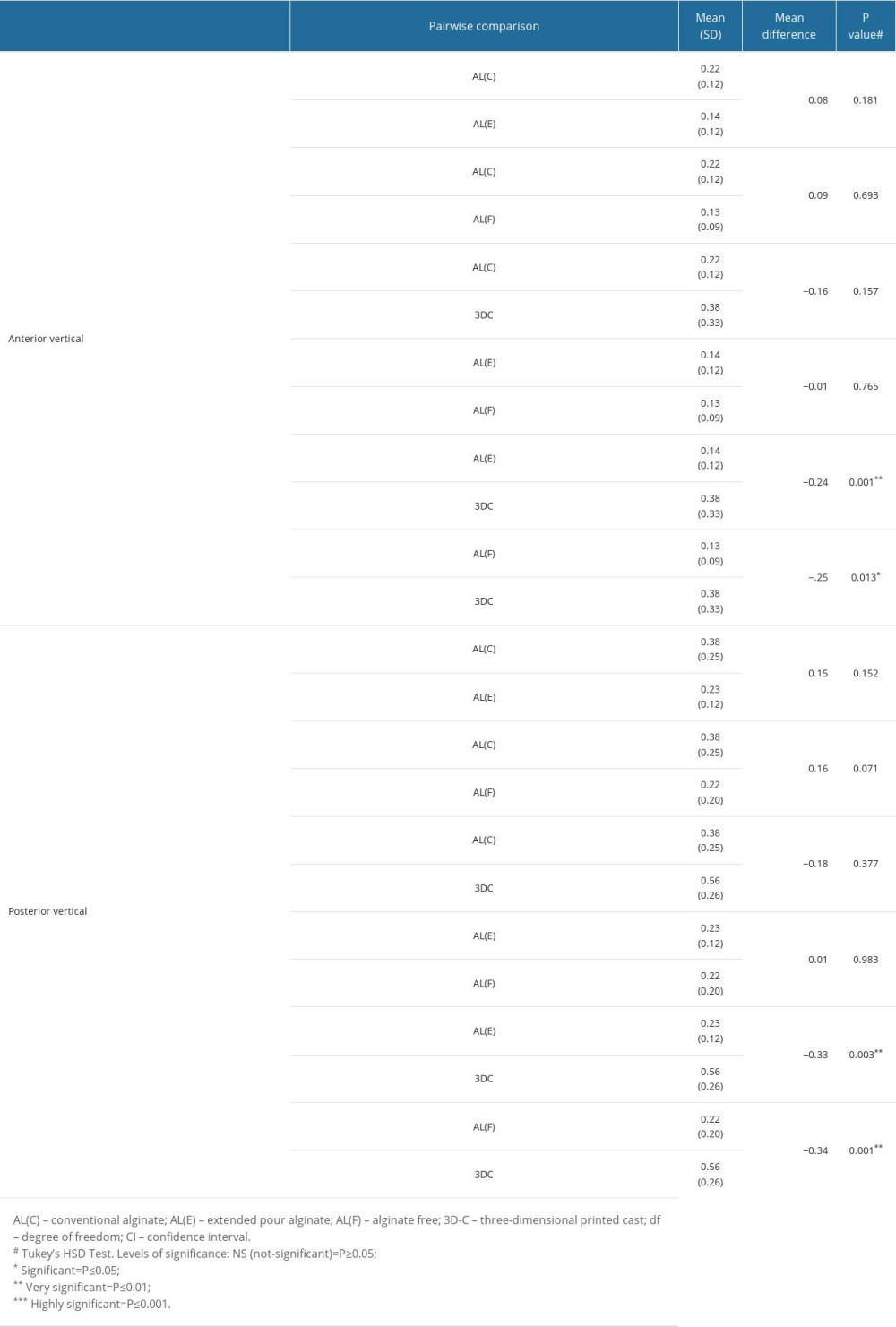
References
1. Carlsson GE, Dental occlusion: Modern concepts and their application in implant prosthodontics: Odontology, 2009; 97; 8-17
2. Meng JC, Nagy WW, Wirth CG, The effect of equilibrating mounted dental stone casts on the occlusal harmony of cast metal complete crowns: J Prosthet Dent, 2010; 104; 122-32
3. Sharma A, Kalra T, Jain S, Comparative evaluation in linear dimensions among various interocclusal recording materials at various mounting times: An in vitro study: World J Dent, 2020; 11(6); 462-67
4. Cowie RR, The successful crown delivery: J Dent Technol, 2015; 38-44
5. McCracken MS, Litaker MS, Gordan VV, Remake rates for single-unit crowns in clinical practice: Findings from The National Dental Practice-Based Research Network: J Prosthodont, 2019; 28; 122-30
6. Christensen GJ, The state of fixed prosthodontic impressions: Room for improvement: J Am Dent Assoc, 2005; 136; 343-46
7. Alghamdi NS, Alamoudi RA, Baba SM, A scanning electron microscopy study comparing 3 obturation techniques to seal dentin to root canal bioceramic sealer in 30 freshly extracted mandibular second premolars: Med Sci Monit, 2023; 29; e940599
8. Waylen A, The importance of communication in dentistry: Dent Update, 2017; 44(8); 774-80
9. Kumar L, Mattoo KA, Jain S, A clinical study of 50 partially edentulous patients with fixed partial denture restorations to compare clinical parameters and changes in gingival sulcus width after displacement with 2 different gingival retraction cord materials (cotton and polymer): Med Sci Monit, 2023; 29; e940098
10. Loos LG, Boyarsky HP, Quiring DJ, Procedure for occlusal refinement of mounted definitive casts to reduce clinical time required for adjustment of occlusion: J Prosthet Dent, 2001; 85; 246-51
11. Jain S, Mattoo K, Khalid I, A study of 42 partially edentulous patients with single-crown restorations and implants to compare bone loss between crestal and subcrestal endosseous implant placement: Med Sci Monit, 2023; 29; e939225
12. Seelbach P, Brueckel C, Wöstmann B, Accuracy of digital and conventional impression techniques and workflow: Clin Oral Investig, 2013; 17; 1759-64
13. Alves de Carvalho IF, Santos Marques TM, Araújo FM, Clinical performance of CAD/CAM tooth-supported ceramic restorations: A systematic review: Int J Periodontics Restor Dent, 2018; 38; e68-78
14. Fasbinder DJ, Digital dentistry: Innovation for restorative treatment: Compend Contin Educ Dent, 2010; 31; 2-11
15. Luthardt RG, Bornemann G, Lemelson S, An innovative method for evaluation of the 3-D internal fit of CAD/CAM crowns fabricated after direct optical versus indirect laser scan digitizing: Int J Prosthodont, 2004; 17; 680-85
16. Christensen GJ, Impressions are changing: Deciding on conventional, digital or digital plus in-office milling: J Am Dent Assoc, 2009; 140; 1301-4
17. Keating AP, Knox J, Bibb R, Zhurov A, A comparison of plaster, digital and reconstructed study model accuracy: J Orthod, 2008; 35; 191-201
18. Yau HT, Yang TJ, Lin YK, Comparison of 3-D printing and 5-axis milling for the production of dental models from intra-oral scanning: Comput Aided Des Appl, 2016; 13; 32-38
19. Şeker E, Ozcelik TB, Rathi N, Yilmaz B, Evaluation of marginal fit of CAD/CAM restorations fabricated through cone beam computerized tomography and laboratory scanner data: J Prosthet Dent, 2016; 115(1); 47-51
20. Indicators SO, Accuracy, reliability and clinical implications of static compared to quantifiable occlusal indicators: Eur J Prosthod Rest Dent, 2020; 28; 1-2
21. Koyano K, Tsukiyama Y, Kuwatsuru R, Rehabilitation of occlusion – science or art?: J Oral Rehabil, 2012; 39(7); 513-21
22. Filtchev AD, Kalachev YS, Phenomenon of domination of the strongest contacts in centric occlusion: Quintessence Int, 2008; 39; 99-106
23. Saeed F, Muhammad N, Khan AS, Prosthodontics dental materials: From conventional to unconventional: Mater Sci Eng C, 2020; 106; 110167
24. Nassar U, Hussein B, Oko A, Dimensional accuracy of 2 irreversible hydrocolloid alternative impression materials with immediate and delayed pouring: J Can Dent Assoc, 2012; 78(78); c2
25. Christensen GJ, Making fixed prostheses that are not too high: J Am Dent Assoc, 2006; 137; 96-98
26. Boksman L, Optimizing occlusal results for crown and bridge prostheses: Dent Today, 2011; 30; 154-57
27. Iwauchi Y, Tanaka S, Kamimura-Sugimura E, Baba K, Clinical evaluation of the precision of interocclusal registration by using digital and conventional techniques: J Prosthet Dent, 2022; 128(4); 611-17
28. Hazeveld A, Slater JJ, Ren Y, Accuracy and reproducibility of dental replica models reconstructed by different rapid prototyping techniques: Am J Orthod Dentofacial Orthop, 2014; 145; 108-15
29. Jeong YG, Lee WS, Lee KB, Accuracy evaluation of dental models manufactured by CAD/CAM milling method and 3D printing method: J Adv Prosthodont, 2018; 10; 245-51
30. Dawood A, Marti Marti B, Sauret-Jackson V, 3D printing in dentistry: Br Dent J, 2015; 219; 521-29
31. Jin SJ, Kim DY, Kim JH, Accuracy of dental replica models using photopolymer materials in addictive manufacturing: In vitro three-dimensional evaluation: J Prosthodont, 2018; 2; e557-e62
32. Park ME, Shin SY, Three-dimensional comparative study on the accuracy and reproducibility of dental casts fabricated by 3D printers: J Prosthet Dent, 2018; 119(5); 861e1-e7
33. Aly P, Mohsen C, Comparison of the accuracy of three-dimensional printed casts, digital, and conventional casts: An in vitro study: Eur J Dent, 2020; 14(2); 189-93
34. Brown GB, Currier GF, Kadioglu O, Kierl JP, Accuracy of 3-dimensional printed dental models reconstructed from digital intraoral impressions: Am J Orthod Dentofacial Orthop, 2018; 154(5); 733-39
35. Millstein P, Maya A, An evaluation of occlusal contact marking indicators: A descriptive quantitative method: J Am Dent Assoc, 2001; 132(9); 1280-86
36. Zimmermann M, Ender A, Attin T, Mehl A, Accuracy of buccal scan procedures for the registration of habitual intercuspation: Oper Dent, 2018; 43; 573-80
37. Tabatabaian F, Namdari M, Mahshid M, Accuracy and precision of intraoral scanners for shade matching: A systematic review: J Prosthet Dent, 2022 Online ahead of print
38. Festing MF, Altman DG, Guidelines for the design and statistical analysis of experiments using laboratory animals: ILAR J, 2002; 43; 244-58
39. Rosenstiel SF, Land MF, Fujimoto J, Principles of tooth preparation: Contemporary fixed prosthodontics, 1995; 2; 135-67, St. Louis, Mosby-Year Book, Inc
40. Revilla-León M, Kois DE, Zeitler JM, An overview of the digital occlusion technologies: Intraoral scanners, jaw tracking systems, and computerized occlusal analysis devices: J Esthet Restor Dent, 2023; 35(5); 735-44
41. : Medit occlusal analyzer Available at:https://support.medit.com/hc/en-us/articles/360021126151-Occlusion-analysis
42. Koo TK, Li MY, A guideline of selecting and reporting intraclass correlation coefficients for reliability research: J Chiropr Med, 2016; 15; 155-63
43. Jain S, Mattoo K, Khalid I, A study of 42 partially edentulous patients with single-crown restorations and implants to compare bone loss between crestal and subcrestal endosseous implant placement: Med Sci Mon, 2023; 29; e939225
44. Stansbury JW, Idacavage MJ, 3D printing with polymers: Challenges among expanding options and opportunities: Dent Mater, 2016; 32; 54-64
45. Rungrojwittayakul O, Kan JY, Shiozaki K, Accuracy of 3D printed models created by two technologies of printers with different designs of model base: J Prosthodont, 2020; 29(2); 124-28
46. Patzelt SB, Bishti S, Stampf S, Accuracy of computer-aided design/computer-aided manufacturing-generated dental casts based on intraoral scanner data: J Am Dent Assoc, 2014; 145; 1133-40
47. Favero CS, English JD, Cozad BE, Effect of print layer height and printer type on the accuracy of 3-dimensional printed orthodontic models: Am J Orthod Dentofacial Orthop, 2017; 152(4); 557-65
48. Zyzalo JR: Masked projection stereolithography: improvement of the Limaye model for curing single layer medium sized part: [thesis], 2008, Albany, New Zealand, Massey University
49. Abduo J, Accuracy of casts produced from conventional and digital workflows: A qualitative and quantitative analyses: J Adv Prosthodont, 2019; 11(2); 138-46
50. Ender A, Attin T, Mehl A, In vivo precision of conventional and digital methods of obtaining complete-arch dental impressions: J Prosthet Dent, 2016; 115; 313-20
51. Al-Imam H, Gram M, Benetti AR, Gotfredsen K, Accuracy of stereolithography additive casts used in a digital workflow: J Prosthet Dent, 2018; 119; 580-85
52. Cho SH, Schaefer O, Thompson GA, Guentsch A, Comparison of accuracy and reproducibility of casts made by digital and conventional methods: J Prosthet Dent, 2015; 113; 310-15
53. Labib MA, El-Beialy AR, Attia KH, Evaluation of the accuracy of digital models obtained using intraoral and extraoral scanners versus gold standard plaster model (diagnostic accuracy study): Open J Med Imaging, 2020; 10(03); 151
54. Darraj A, Mattoo KA, Gupta I, Full mouth rehabilitation of a rheumatoid arthritis patient – the muzyanas challenge: AIMDR, 2017; 3(6); 10
55. Lee JD, Gallucci GO, Lee SJ, An in-vitro evaluation of articulation accuracy for digitally milled models vs. conventional gypsum casts: Dent J, 2022; 10(1); 11
56. Al Sunbul H, Silikas N, Watts DC, Polymerization shrinkage kinetics and shrinkage-stress in dental resin-composites: Dent Mater, 2016; 32; 998-1006
57. Chuang SF, Huang PS, Chen TYF, Shrinkage behaviors of dental composite restorations – the experimental-numerical hybrid analysis: Dent Mater, 2016; 32; e362-e73
58. Winder J, Bibb R, Medical rapid prototyping technologies: State of the art and current limitations for application in oral and maxillofacial surgery: J Oral Maxillofac Surg, 2005; 63(7); 1006-15
59. Edher F, Hannam AG, Tobias DL, Wyatt CC, The accuracy of virtual interocclusal registration during intraoral scanning: J Prosthet Dent, 2018; 120(6); 904-12
60. Abdulateef S, Edher F, Hannam AG, Clinical accuracy and reproducibility of virtual interocclusal records: J Prosthet Dent, 2020; 124(6); 667-73
61. Colombo M, Gallo S, Poggio C, New resin-based bulk-fill composites: In vitro evaluation of micro-hardness and depth of cure as infection risk indexes: Materials (Basel), 2020; 13(6); 1308
62. Cacciafesta V, Sfondrini MF, Lena A, Scribante A, Flexural strengths of fiber-reinforced composites polymerized with conventional light-curing and additional postcuring: Am J Orthod Dentofac Orthop, 2007; 132(4); 524-27
63. Rodríguez-Ivich J, Razaghy M, Henriques B, Magne P, Accelerated fatigue resistance of bonded composite resin and lithium disilicate screw-retained incisor crowns with long and short titanium bases: Int J Perio Restor Dent, 2022; 42(4); 459-69
Figures
Figure 1. Flow chart showing sample preparation and group distribution. Figure created using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation).Figure 2. Master models mounted on a semi-adjustable articulator (BioArt A7 plus). Figure edited and labelled using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation).Figure 3. Three repeatable and reproducible indentations made on the maxillary and mandibular master models with A1 between maxillary central incisors, A2 between mandibular central incisors, P1 at right maxillary first molar, P2 between maxillary right first and second premolar, P3 at mandibular first molar and P4 between mandibular right first and second premolar. Figure edited and labelled using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation).Figure 4. Four different mandibular casts mounted to the same maxillary master model cast on the semi-adjustable articulator using a maximum intercuspation bite registration record. Clockwise right - Hydrogum Alginate (Conventional) [Gp AL(C)], Hydrocolor 5 (Extended-Pour Alginate) [Gp AL(E)], 3D Print Dental Model (Gp 3D-C), FreeAlgin (Alginate Alternative) [Gp AL(F)]. Photographs taken using Digital Single-Lens Reflex (DSLR) (Canon EOS 700D) with 100 mm macro lens) with/without ring flash. Compiled Figure created using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation)Figure 5. Digital articulation between the maxillary and mandibular digital casts showing the casts separated and in articulation position after using the manual alignment tool in the software (Medit Link). Compiled Figure created using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation).Figure 6. Digital measurement of reference points (A) Identifying the measuring landmarks (B) cropping the image and measuring the distance between anterior points (A1–A2) (C) identifying the posterior landmark area (D) cropped image to measure the posterior distances (P1–P3) and (P1–P4). Compiled Figure created using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation).Figure 7. Digital occlusal analysis of articulated exemplary master model using Occlusal Analysis tool (Medit Link software) [Color green indicates occlusal contacts and the degree of occlusal contact (pressure) while blue indicates no contact. Compiled Figure created using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft corporation). Tables
Table 1. Armamentarium, materials used and group distribution in the study.Table 2. Comparative differences in the mean value measurements (millimeters) between the articulated master model and the 4 tested groups.Table 3. One-sample t test showing the dispersion of the measurements and relative differences of each group measurement against the test values of the Articulated Master model.Table 4. Comparative mean error at 3 observed measurements for each group relative to the reference master model (mm).Table 5. Comparative differences of mean errors for various measurements among studied groups in relation to the reference master model.Table 6. Multiple pairwise comparisons of the accuracy of the articulated casts by the 3 impression materials and 3D printed system using Tukey’s HSD test.Table 1. Armamentarium, materials used and group distribution in the study.Table 2. Comparative differences in the mean value measurements (millimeters) between the articulated master model and the 4 tested groups.Table 3. One-sample t test showing the dispersion of the measurements and relative differences of each group measurement against the test values of the Articulated Master model.Table 4. Comparative mean error at 3 observed measurements for each group relative to the reference master model (mm).Table 5. Comparative differences of mean errors for various measurements among studied groups in relation to the reference master model.Table 6. Multiple pairwise comparisons of the accuracy of the articulated casts by the 3 impression materials and 3D printed system using Tukey’s HSD test. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387