14 March 2024: Clinical Research
Comparison of Presentation Types and Clinical Findings of Rural and Urban Patients with Mastalgia: A Retrospective Analysis of 730 Patients from Turkey
Gultekin Ozan Kucuk1ABCDEF*DOI: 10.12659/MSM.943448
Med Sci Monit 2024; 30:e943448






Abstract
BACKGROUND: Breast pain, prevalent among women of reproductive age, varies during menstrual cycles and is influenced by sociodemographic and clinical factors. This study aimed to assess these demographic and clinical variables in women with breast pain, considering the spatial distinctions between urban and rural locations.
MATERIAL AND METHODS: This retrospective study included 730 women presenting with mastalgia between 2010 and 2023. The study evaluated patient demographics, pain characteristics (eg, breast pain duration, site, quadrant-based localization, and radiation of breast pain), radiologic findings, and the presence of comorbid medical conditions.
RESULTS: There were 498 patients in the urban group and 232 patients in the rural group. Among the radiologic findings, the rate of mastitis was higher in the rural group (P<0.05). Regarding the localization of breast pain within the quadrants, left breast upper-inner (LUI) quadrant pain was more common in the rural group (P=0.014). Regarding comorbid medical conditions, the prevalence of gastrointestinal system disease was higher in the rural group (P=0.009). Using logistic regression analysis, gastrointestinal disease was determined to be a significant independent risk factor for increased LUI quadrant pain in the rural group (odds ratio [OR]: 3.132, P=0.014), while pre-existing thyroid disease (OR: 2.482, P=0.004), hypertension (OR: 2.534, P=0.006), and radiologic evidence of ductal ectasia (OR: 2.878, P=0.03) were independent risk factors in the urban group.
CONCLUSIONS: Patient outcomes may be improved by a tailored, population-based approach to mastalgia patients in rural and urban locations focused on their radiologic findings and comorbid medical conditions.
Keywords: Epidemiology, Mastodynia, Rural Health, Diagnosis, Pain
Background
Breast pain, also known as mastalgia or mastodynia, is a common yet challenging concern that does not necessarily indicate a specific illness, and it frequently leads to repeated visits to primary care, general surgery, and breast surgery outpatient clinics [1]. Women ages 30–50 years are more likely to experience breast pain, but it can occur at any age, including the postmenopausal period [2]. Furthermore, the dichotomization or categorization of geographic locations as rural-urban codes is a prevailing paradigm, especially in cancer disparity studies, and affects screening for breast cancer and care quality [3–8]. The way in which patient-related barriers contribute to the diagnosis and outcomes of disorders is of great importance, especially in a situation such as mastalgia, which is a common health problem experienced by 70–80% of women at some time in their lives [9].
The management of mastalgia, according to the UK’s National Institute for Health and Care Excellence (NICE) guidelines, is currently implemented in many centers [1]. According to these guidelines, providing psychological relief to the patient and demonstrating the absence of underlying pathology in the breast generally reassures patients and results in the resolution of breast pain in over 70% of cases [1,10]. However, when breast pain persists for more than 3 months and begins to affect the patient’s daily life, it is necessary to refer the patient to a breast clinic for second-line medications [1]. While this may not be a problem for those residing near teaching hospitals with breast clinics, it can be a challenge for patients living in rural areas. Therefore, this study aimed to compare the presentation types and clinical findings of rural and urban patients who were admitted with breast pain as a primary symptom within the Black Sea region of Turkey.
Material and Methods
ETHICS STATEMENT:
The study was conducted in accordance with the tenets of the Declaration of Helsinki and approval for this study was obtained from Samsun Training and Research Hospital Ethics Committee (reference number: SUKAEK-2023-8/14). Before obtaining ethics approval, separate consents were secured from each of the 4 hospitals where the study was conducted, and these were subsequently submitted to the ethics committee.
INCLUSION AND EXCLUSION CRITERIA:
The study included all patients who presented with breast pain as the main concern at the time of admission, and patients with a breast mass or abscess with breast pain, history of trauma to the breast, nipple discharge, pregnant patients, and male patients were excluded. The study included patients with a primary concern of breast pain who had an incidentally detected breast mass or abscess during clinical work-up (with physical exam or radiologically).
STUDY DESIGN AND PATIENTS:
This study was a retrospective review of collected data recorded by a single surgeon in 730 patients presenting with mastalgia at 4 hospitals (Samsun Vezirkopru, Samsun Gazi State, Giresun University Medical Faculty, Samsun Training and Research Hospital) from June 2010 to July 2023.
The patients were divided into 2 groups: those living in rural areas and those living in urban areas. The following data were extracted from medical records: age in years, body mass index (BMI) in kg/m2, menopausal status, parity history, educational status, marital status, personal and family history of breast cancer, history of previous breast biopsy or surgery, history of any pre-existing disease, history of hormonal contraception or hormone replacement therapy use, smoking history, lactation history, and fear of breast cancer. Physical examination findings and pain characteristics of patients, including breast pain duration, site (right/left), quadrant-based localization, and radiation of breast pain (isolated breast/radiating pain), were evaluated. For the evaluation of comorbidities, existing conditions were determined by reviewing patients’ prior diagnoses and medications as documented in their hospital records. In addition, all patients were evaluated by adapting the National Comprehensive Cancer Network (NCCN) guidelines for breast cancer risk stratification [11].
DEFINITION OF RURALITY:
The concept of ‘rural’ is complex, multifaceted, and often vague [12]. Government agencies often define rurality based on 1 or 2 factors: population size and adjacency to metro areas. In this study, rural and urban residents were assessed and defined using rural or urban zip codes from the index of the residence developed by government.
BREAST PAIN ASSESSMENT:
In assessing the patients’ pain, a comprehensive history was gathered, including inquiries about their medical backgrounds and family histories related to cancer. Both breasts with pain were divided into 4 quadrants, and the patients indicated where they felt the most pain during the breast examination. Some patients also stated that they had pain in the nipple-areola complex adjacent to painful breast quadrants. In addition, an unvalidated questionnaire that included 3 categories was administered and scored to reveal the effects of pain on the patient’s quality of life. A score of 1 was given to the statement “I am used to living with this pain”; 2 points were scored for “This pain affects my daily activities and social life”; and 3 points were given for “This pain wakes me up at night or requires an admission to the emergency clinic due to the pain.”
DEFINITION OF COMORBID MEDICAL CONDITIONS:
Assessment of patients included review of past records, admissions, and medications, referring to the International Classification of Diseases (ICD-10) codes. A patient with no history of treatment or specialist referral related to a particular disease was not considered to have a comorbid medical condition. When confirming diagnoses, due care was given to align the ICD code, medication use, laboratory results, and radiological and endoscopy reports with each comorbid diagnosis. Patients with gastrointestinal tract problems, such as gastritis, duodenitis, peptic ulcers, and gastroesophageal reflux, were categorized together. Patients with biliary tract disease were also included in this group.
DEFINITION OF RADIOLOGIC FINDINGS:
In radiologic evaluation, mammography was conducted for patients above 40 years old, while ultrasound was performed without restrictions for necessary cases. For patients above 30 years old exhibiting a solid mass via ultrasonography, mammography was also conducted. Radiological results were aligned with the specific breast quadrant(s) where the patient experienced pain. If radiological findings corresponded with the pain location, they were considered specific and recorded as such. Otherwise, they were listed as normal or non-specific. For cases where a biopsy was conducted following radiological imaging, pathology reports were monitored, and the final results were documented.
STATISTICAL ANALYSIS:
Statistical analyses were performed using SPSS version 22.0 (IBM Co., Armonk, NY, USA). Descriptive statistics for categorical variables were presented as numbers and percentages. Cross tables and Pearson’s chi-squared test, Yates’s correction, and Fisher’s exact test were used for categorical variables. The normality of the variables was evaluated using the Kolmogorov-Smirnov and Shapiro-Wilk tests. The Mann-Whitney U test was used when the numerical data were not normally distributed. The numerical variables that were not normally distributed are presented as medians and ranges. A
Results
PATIENT CHARACTERISTICS:
Of the 730 participants, the urban group included 498 (68.21%) patients, and the rural group comprised 232 (31.78%) patients. The median ages for the rural and urban groups were 37 (range, 18–81) and 38 years (range, 18–85), respectively. There were no significant differences with respect to age, BMI, menopause status, history of breast biopsy or surgical intervention, or use of oral contraceptive pills or hormone replacement therapy between the 2 groups (P>0.05). Regarding parity history, there was a significant difference between the groups, and the number of pregnancies was higher in the rural group (3 vs 2, respectively, P<0.001). There was a significant difference between the groups in terms of education level (P<0.001), and as expected, the education level was higher in the urban group. Regarding marital status, the proportion of single people was significantly lower in the rural group than in the urban group (15.1% vs 22.7%, P=0.017). According to the family history of breast cancer, the proportion of those with a family history of breast cancer was lower in the rural group than in the urban group (6.9% vs 19.1%, P<0.001). The difference between the rural and urban groups according to smoking status was significant, and the proportion of smokers was lower in the rural group (17.7% vs 32.7%, P<0.001). The was a significant difference between those living in rural and urban groups with respect to lactation status, and the proportion of lactating women was higher in the rural group (4.7% vs 0.4%, P<0.001). The proportion of women with a fear of breast cancer was lower in the rural group (25.9% vs 39.2%, P<0.001). The characteristics of the patients in the rural and urban groups are presented in Table 1.
PAIN CHARACTERISTICS:
There were no significant differences between the rural and urban groups with respect to pain location (right, left, or bilateral), pain distribution in the breast (focal vs diffuse), duration of pain, concomitant nipple-areola complex pain located adjacent to the affected breast quadrants, isolated breast or radiating pain as the presentation type of mastalgia, or pain scores (P>0.05). Regarding the pattern of mastalgia (cyclic or non-cyclic), cyclic mastalgia status was significantly higher in the urban group (42.2% vs 30.2%, P=0.002). When the groups were compared in terms of pain localization according to breast quadrants, the proportion of patients with pain in the left breast upper-inner (LUI) quadrant was higher in the rural group (32.3% vs 23.7%, P=0.014). The characteristics of pain and comparisons of groups are presented in Table 2.
RADIOLOGIC FINDINGS AND PREVALENCE OF COMORBID MEDICAL CONDITIONS OF PATIENTS:
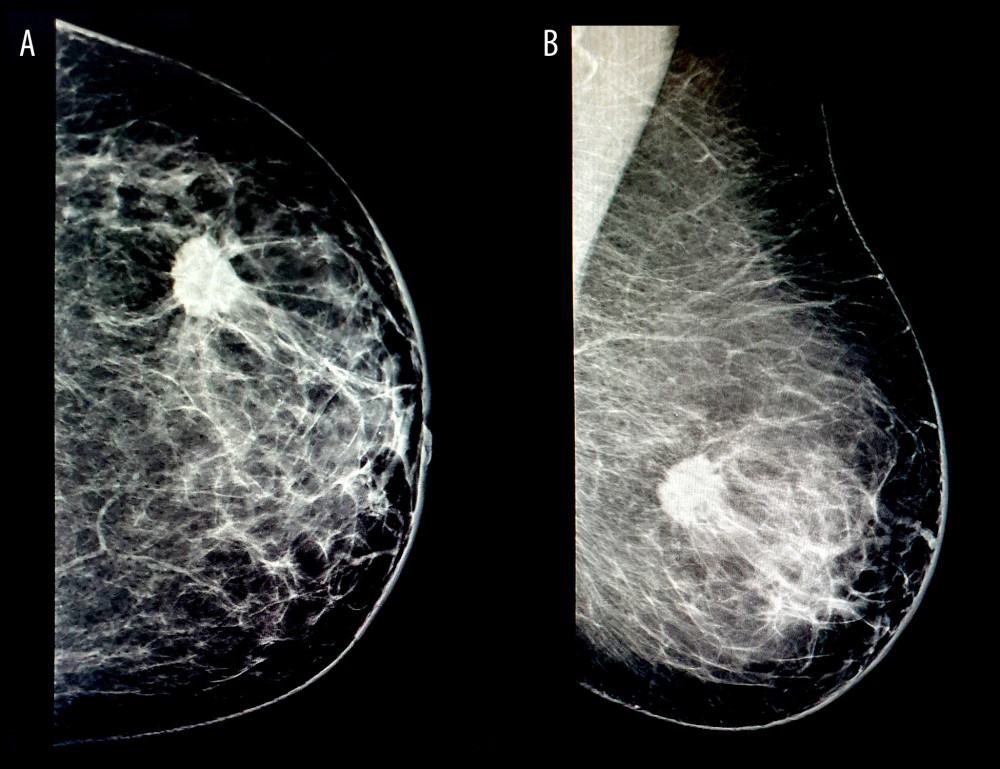
The mastitis/inflammation rate was significantly higher in the rural group (6% vs 2.2%, P=0.015), while the simple or complex cyst rate was significantly higher in the urban group (20.7% vs 13.4%, P=0.017). No statistically significant difference was detected between the groups in terms of other radiologic findings. A significant difference in pre-existing diseases was found only between groups regarding gastrointestinal diseases, and it was significantly higher in the rural group (9.1% vs 4.2%, P=0.009). A comparison of patients with breast pain according to their radiologic findings and comorbid medical conditions is given in Table 3. Figure 1 displays the mammographic images and diagnoses of a patient presenting with mastalgia.
DETERMINATION OF FACTORS AFFECTING LUI QUADRANT PAIN IN THE 2 GROUPS:
Since a significant difference was found between the rural and urban groups with respect to LUI quadrant pain, 2 new groups were formed to include patients with and without LUI quadrant pain. A new comparison between these 2 new groups was performed using the previously mentioned statistical methods. Variables that were significantly different between the 2 new groups, such as menopausal status (P=0.049), parity history (P=0.005), radiologic finding as ductal ectasia (P=0.069), mastitis status (P=0.021), thyroid disease (P=0.023), and gastrointestinal system diseases (P=0.021), regarding medical history were selected for analysis. To determine the independent risk factors affecting LUI quadrant pain, univariate and multivariate logistic regression analyses were performed, and the results are presented in Table 4. Pre-existing gastrointestinal disease was found to be a significant independent factor for LUI quadrant pain in the rural group and caused an increase in the presence of LUI quadrant pain by 3.312 times (OR: 3.132, 95% CI: 1.257–7.806, P=0.014). Pre-existing thyroid disease (OR: 2.482, 95% CI: 1.33–4.634, P=0.004), hypertension (OR: 2.534, 95% CI: 1.3–4.939, P=0.006), and radiologic evidence of ductal ectasia (OR: 2.878, 95% CI: 1.108–7.475, P=0.03) were found to be independent factors causing an increase in LUI quadrant pain in the urban group.
Discussion
The present study compared the demographic characteristics and clinical presentations of patients from rural and urban areas who presented with breast pain as their primary symptom. Our study results indicate that concerning the localization of breast pain within the quadrants, LUI quadrant pain was more prevalent in the rural group. In terms of comorbid medical conditions, there was a higher prevalence of gastrointestinal system diseases in the rural group. Among the radiological findings, mastitis/inflammation rates were significantly higher in the rural group, while the rates of simple or complex cysts were significantly higher in the urban group. Based on these findings, a logistic regression analysis was conducted to identify independent factors associated with increased LUI quadrant pain in both groups. It was determined that gastrointestinal disease was a significant independent factor for increased LUI quadrant pain in the rural group, while pre-existing thyroid disease, hypertension, and radiological evidence of ductal ectasia were identified as independent factors in the urban group.
Mastitis is defined as inflammation of the breast and can be lactational or non-lactational [13]. One of the major issues in patients with lactational mastitis is that they may not have signs of acute inflammation, such as erythema and a localized temperature increase, and these patients may present with breast pain as the only symptom. Eglash et al [14] found that only 16% of patients who presented with lactational mastitis had erythema and increased warmth in breast tissue. In the present study, the rate of mastitis was higher in rural patients presenting with mastalgia as the primary symptom. This finding may be explained by the higher proportion of lactating patients in the rural group. Additionally, in these cases, factors such as poor living and working conditions may contribute to a higher rate of mastitis in patients living in rural areas. Consequently, educating pregnant and/or lactating women from rural areas on nipple hygiene may reduce hospital admissions for mastalgia resulting from puerperal or lactational mastitis. Furthermore, smoking is widely accepted to be associated with chronic periductal mastitis [15]. Although the smoking rate was significantly higher in the urban group, mastitis was more common among patients living in rural areas. Further research is needed on other risk factors for rural populations, such as tuberculosis of the breast, immunosuppression with associated increased infection risk, and diabetes, which can cause mastitis.
In this study, both the rate of radiologically detected simple or complex cysts and the rate of a family history of breast cancer were significantly higher in women from urban areas. This finding might be due to a higher rate of breast self-examinations and a greater awareness in those who have a family history of breast cancer. Ucuncu et al [16] studied the behavioral patterns of breast cancer patients living in rural and urban areas and concluded that health awareness was significantly higher in patients with a higher education level, those who lived in urban areas, and those with a family history of breast cancer. These findings are consistent with the results of the present study regarding the education level and family history of breast cancer, which appear to be related to an increase in the detection of cystic or solid masses in patients presenting with mastalgia in urban settings. Furthermore, the present study confirmed clinical observations by revealing a high prevalence of breast cancer in family histories (19.1% vs 6.9%), along with a heightened fear of breast cancer among urban women (39.2% vs 25.9%).
Numerous studies indicate that mastalgia does not signify or contribute to the risk of breast cancer [17]. Past studies have shown the breast cancer detection rate in patients with breast pain ranges from 0.5% to 3.3% [18]. In the present study, the breast cancer detection rate among all patient groups was 1.5%, which aligns with the rates reported in previous research. When patients were divided into rural and urban groups, there was a 1.7% detection rate in women from rural areas and 1.4% in those from urban areas, but the difference was not statistically significant.
Referred pain is defined as pain originating from an internal organ, and chest pain from the abdomen or gastrointestinal tract may be a result of a wide range of upper gastrointestinal diseases [19]. Patients with epigastric or retrosternal pain resulting from gastritis, peptic ulcer disease, or reflux esophagitis may also experience chest pain similar to mastalgia [20,21]. In this study, when painful breast quadrants were evaluated, the proportion of patients with pain in the LUI quadrant was significantly higher in the rural group. In addition, patients with a history of gastrointestinal disease were also significantly more prevalent in the rural group. Regarding studies on the epidemiology of gastrointestinal diseases in rural areas, Machlis et al [22] reported that gastroesophageal reflux disease impairs the quality of life, especially in rural patients. In another study, Lin et al [23] emphasized that rural patients sought more medical help for gastritis, duodenitis, and ulcer disease than urban patients, and they highlighted an important disparity between rural and urban patients due to barriers to accessing specialists, such as gastroenterologists, in rural areas. Consistent with these findings, based on logistic regression analysis, the presence of gastrointestinal disease as a comorbid medical condition was found to be an independent factor that affects pain in the LUI quadrant in rural patients. The independent factors that cause an increase in LUI quadrant pain were found to be hypertension, thyroid disease, and radiologic evidence of ductal ectasia in urban patients. Regarding thyroid diseases as a cause of referred breast pain, both hyperthyroidism and untreated hypothyroidism can have detrimental effects on the heart due to the increase/decrease in endogenous hormone production or unregulated exogenous thyroid hormone intake [24]. Additionally, chest pain may also occur in some patients with giant mediastinal goiters [25]. In summary, some thyroid-related diseases can cause chest pain and may mimic breast pain in the LUI quadrant.
Many studies have examined the objective assessment of breast pain using tools such as the Visual Analog Scale (VAS), Cardiff Pain Score, and Short Form Modified McGill Pain Questionnaire [26,27]. This scale was introduced to our study’s participants, but some struggled with the VAS system, responding with statements like “I have no pain at the moment” or “I am not currently experiencing pain; it occurs from time to time.” Scoring methods such as the VAS and Cardiff chart may be best applied in specialized settings like breast clinics [27]. The utilization of a Visual Analog Scale (VAS) necessitates potential re-admission to the hospital and a certain level of literacy skills. There can be additional challenges with these pain scales if a patient resides in a rural area or has cyclical breast pain linked to their menstrual cycle. Factors such as education level, social and cultural influences on pain tolerance, and the necessity to travel for breast pain assessment can affect the patient’s test performance and compliance [28]. The present study inquired about the impact of breast pain on patients’ quality of life to help differentiate breast pain from its presentation in other conditions such as cardiac diseases, mastitis, peptic ulcers, lung diseases, and psychiatric disorders. In essence, factors such as the patients’ lower literacy rates, orientation challenges, absence of pain at the time of admission, and the complexity of these scoring systems led to use of a simpler scoring system; therefore, the VAS score was not considered.
This study had some limitations. First, the rural and urban groups were unequal in size. Another limitation is that this was a retrospective review of a single surgeon’s practice. Third, the study’s results mainly included patients living in the Black Sea region and cannot be generalized to all regions in Turkey. Finally, this study focused on the results of clinical presentation and clinical findings of patients presenting with mastalgia rather than long-term treatment outcomes.
Conclusions
This study provides some evidence for patients with mastalgia concerning the place-based factor of rural or urban locations. Patients presenting with only mastalgia in rural areas may experience a higher frequency of mastitis based on radiologic findings compared to those in urban areas. Furthermore, it is noteworthy that in certain patients, the presence of LUI quadrant pain may be attributed to referred pain stemming from concurrent medical conditions such as gastrointestinal disease, thyroid disease, hypertension, and radiological evidence of ductal ectasia. These results underscore the importance of conducting population-based, stratified, prospective studies to explore these associations further.
Tables
Table 1. Baseline characteristics and comparison of patients by rural vs urban location.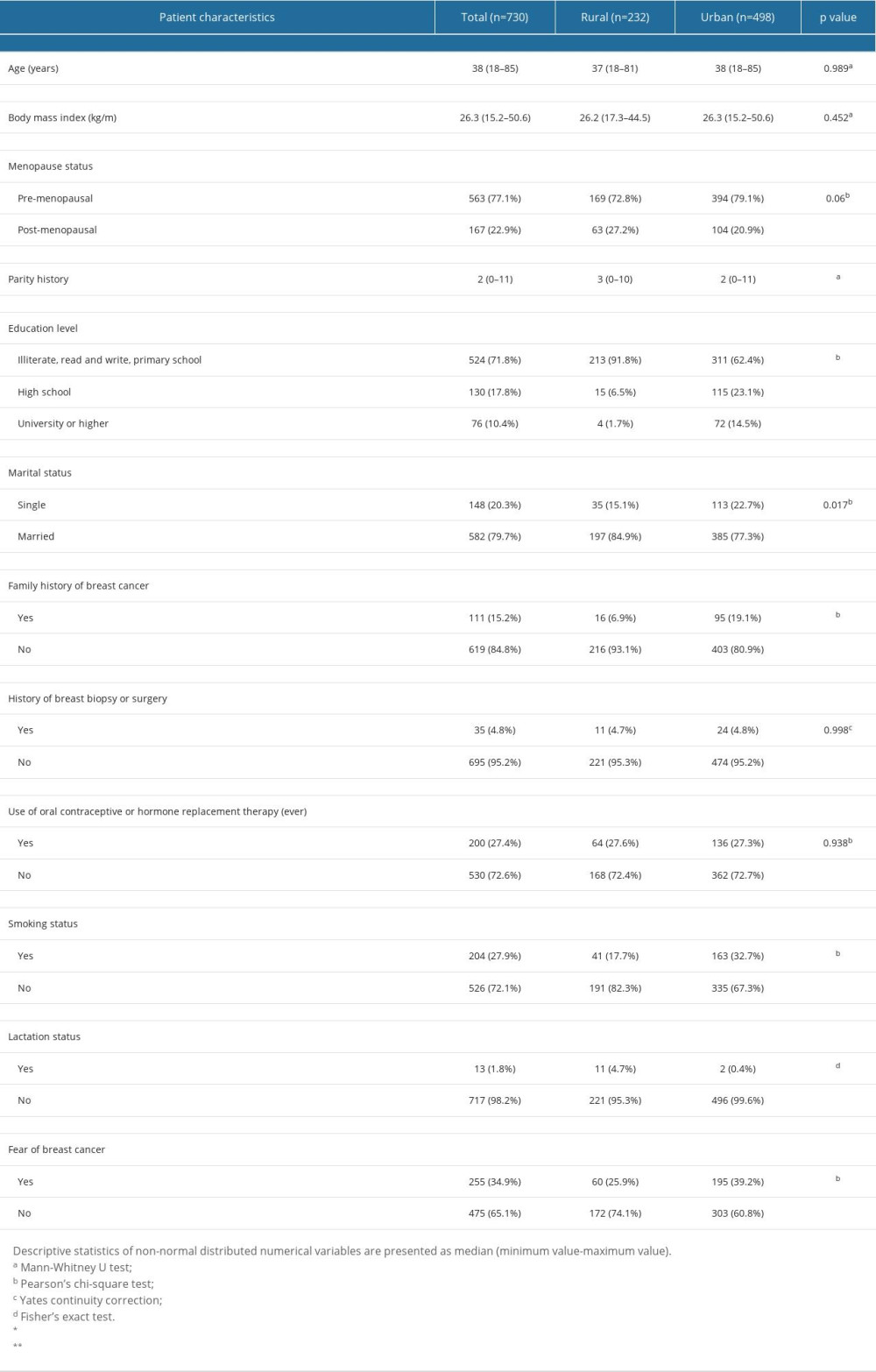 Table 2. Pain characteristics of patients and comparisons by rural vs urban location.
Table 2. Pain characteristics of patients and comparisons by rural vs urban location.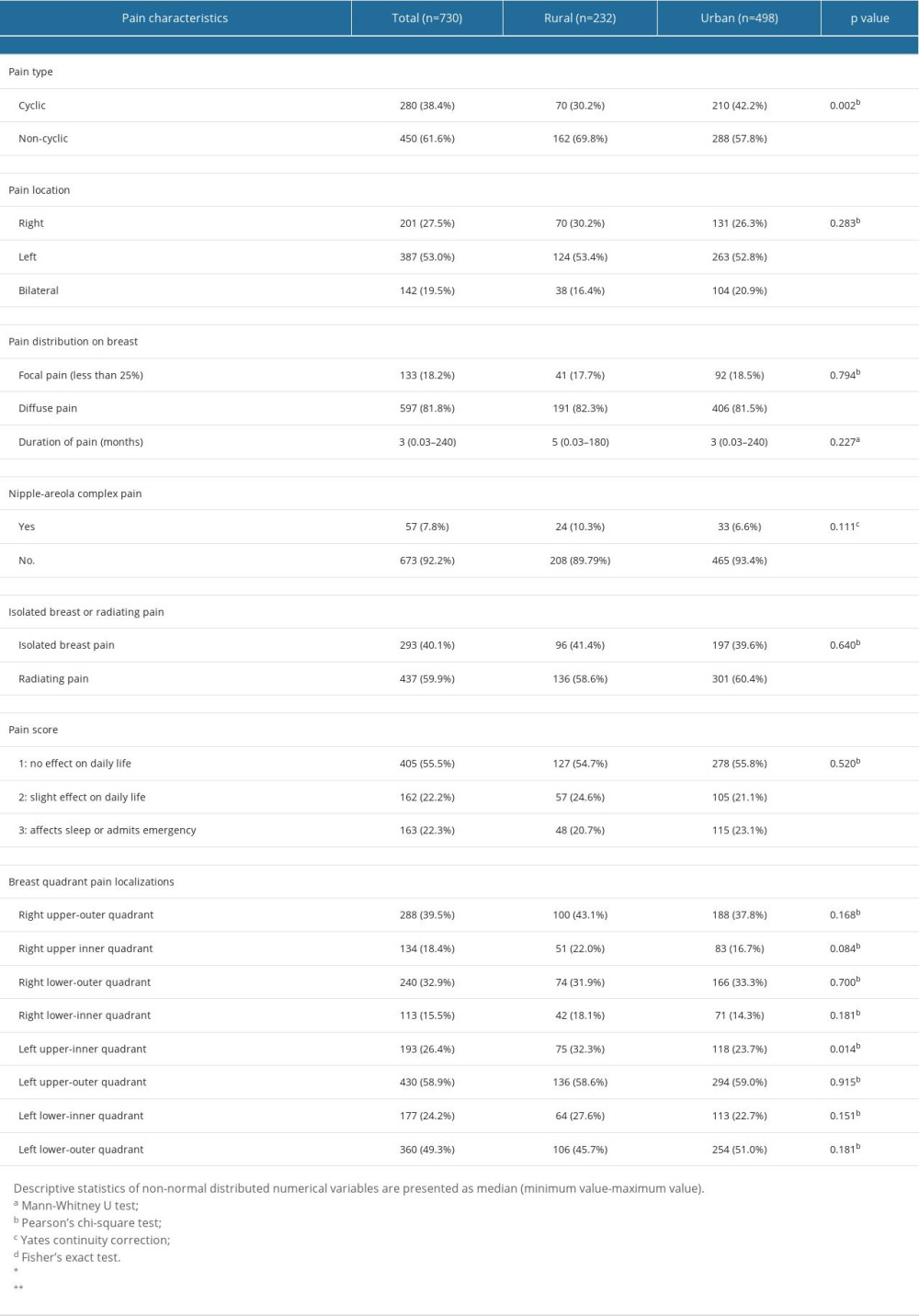 Table 3. Radiologic findings and comorbid medical conditions of patients presenting with mastalgia.
Table 3. Radiologic findings and comorbid medical conditions of patients presenting with mastalgia.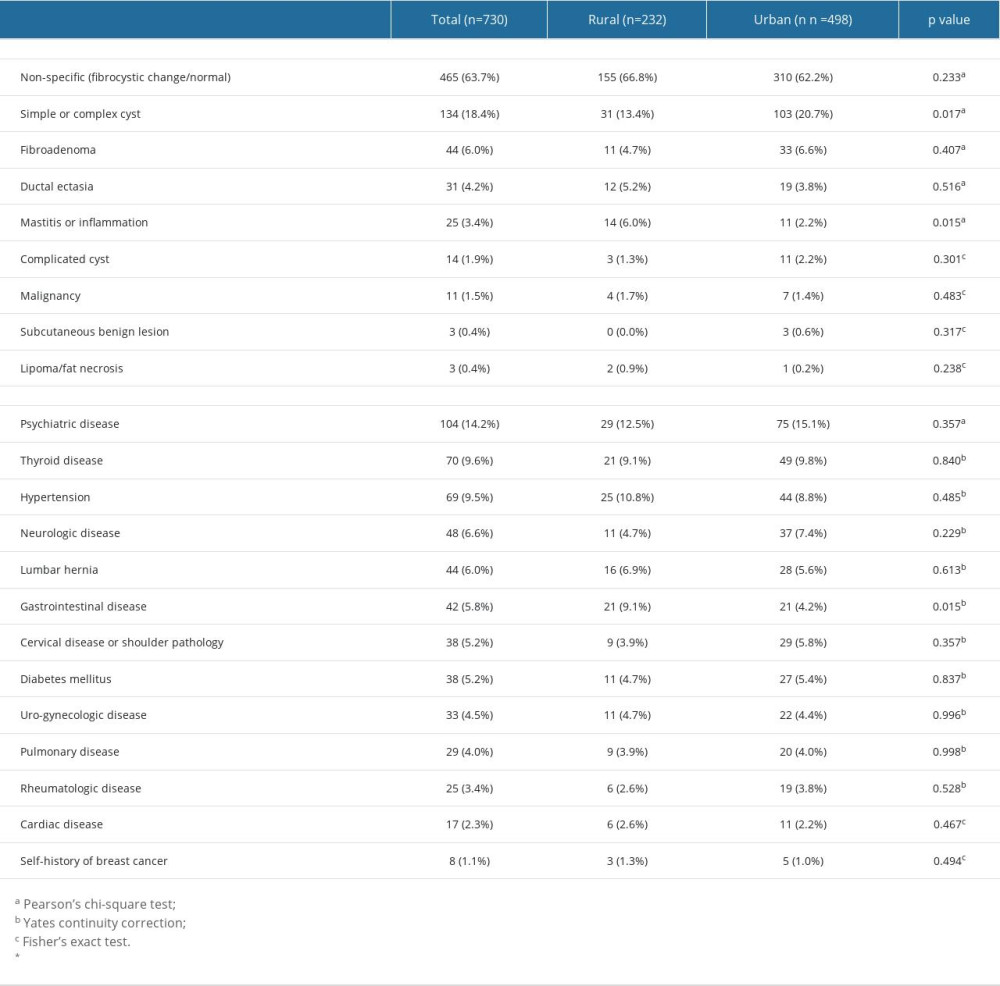 Table 4. Logistic regression analysis results for risk factors affecting left breast upper-inner quadrant pain.
Table 4. Logistic regression analysis results for risk factors affecting left breast upper-inner quadrant pain.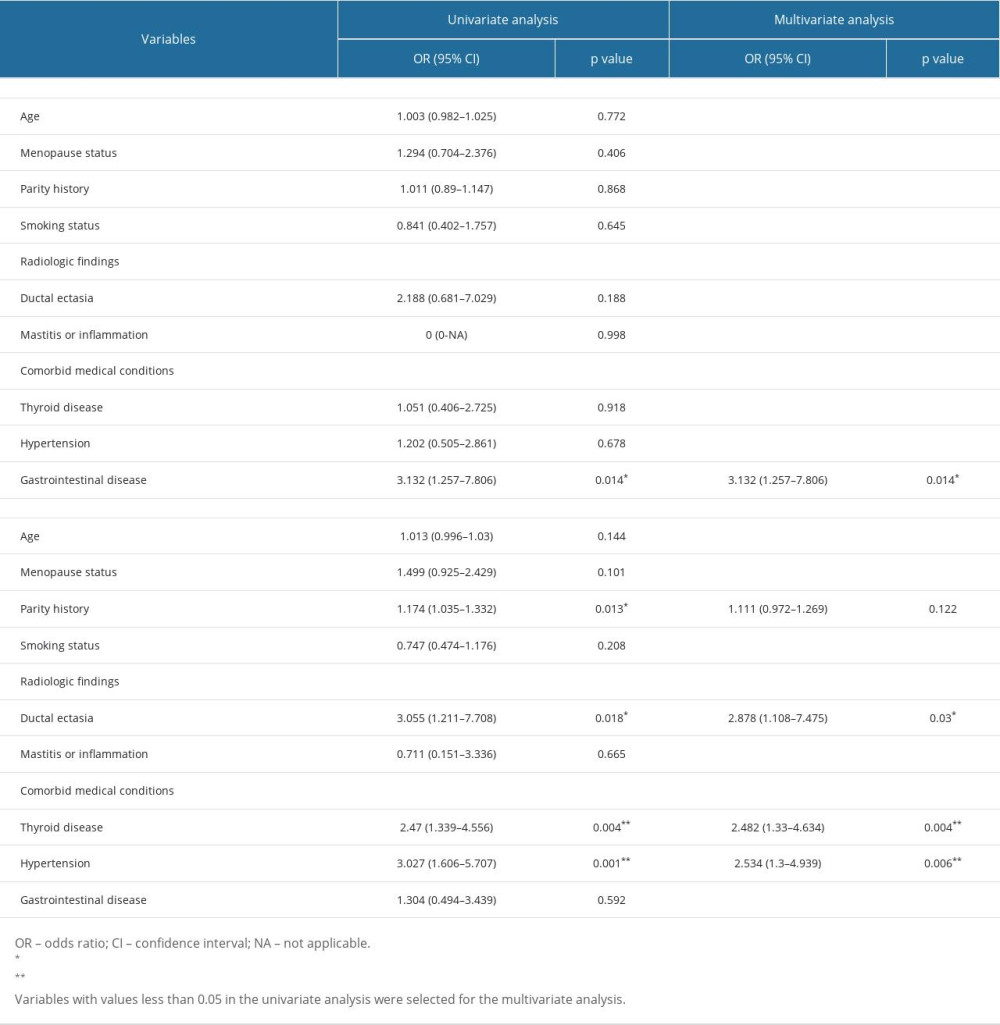
References
1. Hafiz SP, Barnes NLP, Kirwan CC, Clinical management of idiopathic mastalgia: A systematic review: J Prim Health Care, 2018; 10(4); 312-23
2. Goyal A, Breast pain: Am Fam Physician, 2016; 93(10); 872-73
3. Longacre CF, Neprash HT, Shippee ND, Evaluating travel distance to radiation facilities among rural and urban breast cancer patients in the medicare population: J Rural Health, 2020; 36(3); 334-46
4. Nguyen-Pham S, Leung J, McLaughlin D, Disparities in breast cancer stage at diagnosis in urban and rural adult women: A systematic review and meta-analysis: Ann Epidemiol, 2014; 24(3); 228-35
5. Leung J, McKenzie S, Martin J, McLaughlin D, Effect of rurality on screening for breast cancer: A systematic review and meta-analysis comparing mammography: Rural Remote Health, 2014; 14(2); 2730
6. LeBlanc G, Lee I, Carretta H, Luo Y, Rural-urban differences in breast cancer stage at diagnosis: Womens Health Rep (New Rochelle), 2022; 3(1); 207-14
7. Zahnd WE, Sherman RL, Klonoff-Cohen H, Disparities in breast cancer subtypes among women in the lower Mississippi Delta Region states: Cancer Causes Control, 2019; 30(6); 591-601
8. Kucuk GO, The effect of sociocultural factors in the stage of breast cancer: An astonishing image from a rural area: Breast J, 2012; 18(5); 485-86
9. Holbrook AI, Moy LExpert Panel on Breast Imaging: J Am Coll Radiol, 2018; 15(11S); S276-S82
10. Barros AC, Mottola J, Ruiz CA, Reassurance in the treatment of mastalgia: Breast J, 1999; 5(3); 162-65
11. Daly MB, Pal T, Berry MP, Genetic/familial high-risk assessment: Breast, ovarian, and pancreatic, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology: J Natl Compr Canc Netw, 2021; 19(1); 77-102
12. Lourenco AE, The meaning of ‘rural’ in rural health: A review and case study from Brazil: Glob Public Health, 2012; 7(1); 1-13
13. Dener C, Inan A, Breast abscesses in lactating women: World J Surg, 2003; 27(2); 130-33
14. Eglash A, Plane MB, Mundt M, History, physical and laboratory findings, and clinical outcomes of lactating women treated with antibiotics for chronic breast and/or nipple pain: J Hum Lact, 2006; 22(4); 429-33
15. Furlong AJ, al-Nakib L, Knox WF, Periductal inflammation and cigarette smoke: J Am Coll Surg, 1994; 179(4); 417-20
16. Ucuncu MZ, Ucuncu MM, Toprak D, Evaluation knowledge, attitude, and behaviour for breast cancer among young women living in two different habitats of Turkey: Asian Pac J Cancer Prev, 2018; 19(11); 3179-85
17. Altintas Y, Bayrak M, Evaluation of 1294 female patients with breast pain: A retrospective study: Adv Ther, 2018; 35(9); 1411-19
18. Grullon S, Bechmann S, Mastodynia [Updated 2023 Jun 5]: StatPearls [Internet], 2023, Treasure Island (FL), StatPearls Publishing Available from: https://www.ncbi.nlm.nih.gov/books/NBK559249/
19. Noda K, Ikusaka MTips for taking history of pain: Brain Nerve, 2012; 64(11); 1273-77 [in Japanese]
20. ElSherif A, Valente SA, Management of mastalgia: Surg Clin North Am, 2022; 102(6); 929-46
21. Tahir MT, Shamsudeen S, Mastalgia: StatPearls November 1, 2022, Treasure Island (FL), StatPearls Publishing
22. Kaplan-Machlis B, Spiegler GE, Revicki DA, Health-related quality of life in primary care patients with gastroesophageal reflux disease: Ann Pharmacother, 1999; 33(10); 1032-36
23. Lin YH, Tseng YH, Chen YC, The rural-urban divide in ambulatory care of gastrointestinal diseases in Taiwan: BMC Int Health Hum Rights, 2013; 13; 15
24. Ertek S, Cicero AF, Hyperthyroidism and cardiovascular complications: A narrative review on the basis of pathophysiology: Arch Med Sci, 2013; 9(5); 944-52
25. Iacobellis G, Huge mediastinal goiter: An unusual cause of precordial pain: Thyroid, 2004; 14(8); 635
26. Khan SA, Apkarian AV, The characteristics of cyclical and non-cyclical mastalgia: A prospective study using a modified McGill Pain Questionnaire: Breast Cancer Res Treat, 2002; 75(2); 147-57
27. Gautam S, Srivastava A, Kataria K, New breast pain chart for objective record of mastalgia: Indian J Surg, 2016; 78(3); 245-48
28. Campbell CM, Edwards RR, Ethnic differences in pain and pain management: Pain Manag, 2012; 2(3); 219-30
Tables
Table 1. Baseline characteristics and comparison of patients by rural vs urban location.Table 2. Pain characteristics of patients and comparisons by rural vs urban location.Table 3. Radiologic findings and comorbid medical conditions of patients presenting with mastalgia.Table 4. Logistic regression analysis results for risk factors affecting left breast upper-inner quadrant pain.Table 1. Baseline characteristics and comparison of patients by rural vs urban location.Table 2. Pain characteristics of patients and comparisons by rural vs urban location.Table 3. Radiologic findings and comorbid medical conditions of patients presenting with mastalgia.Table 4. Logistic regression analysis results for risk factors affecting left breast upper-inner quadrant pain. In Press
12 Mar 2024 : Database Analysis
Risk Factors of Age-Related Macular Degeneration in a Population-Based Study: Results from SHIP-TREND-1 (St...Med Sci Monit In Press; DOI: 10.12659/MSM.943140
12 Mar 2024 : Clinical Research
Preoperative Blood Transfusion Requirements for Hemorrhoidal Severe Anemia: A Retrospective Study of 128 Pa...Med Sci Monit In Press; DOI: 10.12659/MSM.943126
12 Mar 2024 : Clinical Research
Tissue Inhibitors of Metalloproteinase 1 (TIMP-1) and 3 (TIMP-3) as New Markers of Acute Kidney Injury Afte...Med Sci Monit In Press; DOI: 10.12659/MSM.943500
12 Mar 2024 : Review article
Optimizing Behçet Uveitis Management: A Review of Personalized Immunosuppressive StrategiesMed Sci Monit In Press; DOI: 10.12659/MSM.943240
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952