28 July 2024: Clinical Research
Enhanced Postoperative Pain Management and Mobility Following Arthroscopic Knee Surgery: A Comparative Study of Adductor Canal Block with and without IPACK Block
Jian Zeng12ABCDEF, Xiongtiao Yang2ACDEF, Hongyi Lei2ACE, Xiao Zhong2BC, Xiaoqin Lu1BD, Xianbao Liu1ACDEFG*, Xiaomin Peng2FDOI: 10.12659/MSM.943735
Med Sci Monit 2024; 30:e943735






Abstract
BACKGROUND: Arthroscopic knee surgery (AKS) is minimally invasive, reducing hospital stay compared to traditional surgery, but postoperative pain remains a significant issue. This study compared the analgesic and functional outcomes following AKS following anesthesia using adductor canal block (ACB) with and without anesthesia using the interspace between the popliteal artery and posterior capsule of the knee (IPACK) block under spinal anesthesia (SA).
MATERIAL AND METHODS: We randomly allocated 120 patients into 3 groups: IPACK+ACB+SA for Group A (n=40), ACB+SA for Group B (n=40), and SA for Group C (n=40). The outcome was the visual analog scale (VAS) score evaluated at rest and during activity at 3 h, 6 h, 12 h, 24 h, and 48 h postoperatively, the frequency of administration of postoperative rescue analgesic, and the maximal walking distance at 24 h and 48 h postoperatively.
RESULTS: Compared with Group C, the VAS scores in Group A were significantly lower at 48 h postoperatively (P<0.05). There was a significant difference in the frequency of postoperative rescue analgesia use among the 3 groups (P=0.001). In a subgroup analysis of meniscus shaping under arthroscopy, the resting VAS score in Group A was lower than that in Group B and Group C at 48 h postoperatively (P<0.05). The maximum walking distance of Group A was longer than that of Group B and Group C at 24 h and 48 h postoperatively (P<0.01).
CONCLUSIONS: The effect of postoperative analgesia in the group receiving IPACK combined with ACB after AKS was obviously superior. In arthroscopic meniscus repair surgery, the duration of analgesia was longer, and the maximum walking distance at 48 h postoperatively was longer.
Keywords: Analgesia, Knee Joint, Nerve Block, Lower Extremity, pain management, Humans, Pain, Postoperative, Arthroscopy, Female, Male, Middle Aged, adult, Pain Measurement, Treatment Outcome
Introduction
Arthroscopic knee surgery (AKS), a minimally invasive procedure, is widely used in orthopedic surgery because it minimizes soft-tissue injury and reduces the length of hospital stay in the orthopedics unit compared with traditional open-field surgery [1]. However, postoperative pain is still a serious problem. Surgery is one of the main factors causing postoperative pain, including preoperative tissue damage, intraoperative pneumatic tourniquet use, postoperative inflammatory reaction, and other factors. Moderate to severe pain occurs in almost all patients undergoing knee arthroscopy at 1 h after surgery, and decreased at the end of 24 h. Intra-articular remifentanil can decrease postoperative pain and analgesic requirements in patients [2]. There are many ways to reduce acute pain after arthroscopic knee surgery. Oral or intravenous drugs for analgesia are the most basic way to relieve postoperative pain, but large amounts of postoperative rescue analgesia can increase the incidence of adverse drug reactions such as nausea, vomiting, itching, and gastrointestinal bleeding. Local anesthetics (Las) are commonly infiltrated into surgical wounds for postsurgical analgesia. Local infiltration analgesia is an essential component of multimodal analgesia after AKS [3]. Although local infiltration is effective in analgesia, it is very important to determine if this practice offers any protection against surgical site infections and the increased risk of local anesthetic toxicity [4,5].
Ultrasound-guided regional nerve block is a visualization technique that has the advantages of being a simple procedure and plays an important role in analgesic effects. Sciatic nerve block combined with femoral nerve block is effective when there is inadequate pain relief after AKS, but both can affect lower-limb muscle strength, limiting early recovery of motor function and increasing the risk of falls. It also delays patient recovery surgery [6]. Effective pain control is challenging after knee joint surgery owing to the complex innervation of the knee joint. The adductor canal block (ACB) is a space formed by the fascia envelope and is located in the inner part of the thigh. It mainly contains the saphenous nerve, femoral artery, femoral vein, and lymphatic vessels. The saphenous nerve is the main sensory nerve of the adductor duct, and it is one of the sensory nerve branches of the femoral nerve, which innervates the skin of the anterior, inner, and lower parts of the knee joint and some sensory areas in the joint cavity [7]. ACB can provide adequate pain relief to the anterior knee while sparing motor function of the quadriceps muscles [8,9]. Infiltration between the popliteal artery and capsule of the knee (IPACK) is a block that specifically targets the posterior knee. IPACK has been reported to deliver additional pain relief when administered along with other standard procedures, indicating the possible superiority of distal injection at the level of the femoral condyles for management of posterior knee pain [10,11].
A meta-analysis showed that adding IPACK to ACB reduced pain scores 24 h after TKA and improved functional recovery in patients compared with ACB alone [10], but there was no reduction in opioid analgesic consumption. However, different studies have shown that compared with ACB alone, IPACK can significantly reduce the postoperative pain score and the use of analgesics after TKA, but it does not significantly improve postoperative mobility [11]. TKA surgery creates serious trauma in the knee area caused by bone resection, soft-tissue release, prosthesis implantation, and wound suturing [12]. The lack of mobility improvement may be related to TKA trauma. For arthroscopic knee surgery, including meniscus dressing and molding, popliteal cyst resection, and simple cruciate ligament reconstruction surgery, the trauma is much less than with TKA. Because TKA causes less trauma than AKS, we hypothesized that compared with ACB alone, the addition of IPACK can significantly reduce the pain score and the use of analgesics after AKS, and that postoperative motor function can be significantly improved.
The purpose of this study was to analyze the effects of IPACK and ACB block on analgesia and functional recovery after AKS compared with ACB alone in patients undergoing different types of elective AKS. We hypothesized that IPACK combined with ACB would reduce the frequency of postoperative rescue analgesia and increase the maximum walking distance. We believe that this study will further validate the efficacy of IPACK combined with ACB in different types of elective AKS.
Material and Methods
RANDOMIZATION AND BLINDING:
This study was a randomized controlled trial evaluating the postoperative analgesic effects of 3 different anesthesia methods. The primary outcome measure was the visual analog scale (VAS) score. Based on preliminary experiments, the mean 24-h VAS scores for the 3 groups were 1.4, 2.2, and 2.4, with standard deviations of 0.98, 0.96, and 1.20, respectively. In accordance with the requirements of a bilateral test, setting α at 0.05 and power at 90% (1-β), PASS 15.0.5 software was used to calculate the required sample size of n=34 cases per group. Considering a potential loss or refusal rate of 10%, the software suggested a minimum of 37.4 cases per group. Therefore, this study ultimately included 40 samples per group, totaling 120 cases [13,14].
n represents the sample size per group and g represents the number of groups;
Patients were randomly allocated into 3 groups of 40 patients each. Randomization was performed using a computer-generated randomization sequence concealed in sealed opaque envelopes that were opened by trained research personnel on the day of surgery. Patients were randomized in a 1: 1: 1 ratio into Group A (patients received IPACK+ACB+SA), Group B (patients received ACB+SA), and Group C (patients received SA). The envelope was opened by an anesthesiologist who was not involved in the design of the study. The researchers who collected the data (Investigator A) and performed the statistical analysis (Investigator B) remained blinded to the trial grouping of patients throughout the study.
PARTICIPANTS:
A total of 120 patients ages 18–65 years with a physical status grade according to the American Society of Anaesthesiologists classification (ASA) of 1–3 undergoing unilateral AKS under SA were enrolled in this randomized controlled study. The study was conducted between April 2020 and March 2021. The exclusion criteria were body mass index (BMI) more than 40 kg/m2, chronic kidney disease or cardiac insufficiency, chronic use of analgesics (daily use at least 60 mg morphine equivalents for >4 weeks) or psychotropics, allergy to ropivacaine, preexisting lower-extremity neurological deficit, inability to comprehend or cooperate, patient refusal of either spinal anesthesia or regional block, and failure of the IPACK or ACB procedure prior to single SA.
:
ACB was performed with the patient supine. The patient was prepped in a sterile manner, and a linear transducer (GE Logiq V2, 10 to 12 MHz) was placed on the mid-thigh. The femur was visualized, and the transducer was moved medially until the superficial femoral artery, deep to the sartorius muscle, was visualized in the adductor canal. Below the sartorius muscle, the femoral artery was identified. The saphenous nerve is adjacent to the femoral artery. A 15° 0.71×80 mm, 22-G nerve block needle (Stimuplex D, B Braun) was inserted parallel to the long axis of the transducer from the lateral side. Normal saline with a volume of 1~2 mL was injected into the suspected adductor canal to confirm that the needle was placed in the correct position. Twenty mL of 0.25% ropivacaine was administered around the saphenous nerve in 5-mL increments after careful aspiration (Figure 1).
:
The IPACK block was performed with the patient supine, the knee elevated, and the hip slightly abducted and externally rotated to gain access to the medial surface of the distal thigh. A curvilinear transducer (GE Logiq V2, 10 to 12 MHz) was positioned on the medial thigh 1–2 fingerbreadths above the patella. The femur was identified along with the femoral shaft, popliteal artery, and posterior space of the femoral shaft. A 15° 0.71×80 mm, 22-G nerve block needle (Stimuplex D, B Braun) was then advanced in-plane to the transducer towards the posterior space between the femur and the popliteal artery. Twenty mL of 0.25% ropivacaine was injected in 5-mL increments with careful aspirations (Figure 2).
PERIOPERATIVE MANAGEMENT:
Adequate preoperative fasting was confirmed on the day of surgery. The patient was instructed to eat no solid food for ≥8 h and drink no fluids for ≥4 h preoperatively. Upon arrival to the operating theater, routine monitoring was performed continuously, including electrocardiography, noninvasive blood pressure readings, and pulse oximetry. Systolic blood pressure (SBP), heart rate (HR), and pulse oximetry were assessed every 5 min. The veins were cannulated with an 18-gauge venous cannula on the contralateral upper limb, and an infusion was started with lactated Ringer’s solution at a rate of 6–8 mL/kg/h. Oxygen was administered with a face mask (3–4 L/min). The study intervention was performed after opening the peripheral vein.
Ultrasound-guided IPACK and ACB were performed in Group A, and ACB was performed in Group B. The VAS was evaluated at 5–10 min after IPACK and/or ACB, including the posterior area of the knee (IPACK area) and the anterior, medial, and inferior area of the knee (ACB area). When patients in Group A and Group B developed sensory block, SA was administered using 15 mg 0.5% hyperbaric ropivacaine in the lateral decubitus position at the L3–L4 intervertebral space (patients in Group C only received lumbar anesthesia). The level of sensory block in SA was controlled between T8 and T10 by adjusting the body position, injection speed, and injection time. All of the above intraoperative procedures were performed by the same anesthesiologist, who was blinded to the study. All AKS procedures were performed by the same surgeon using a standard approach with a tourniquet. All patients received standardized postoperative analgesia using intravenous flurbiprofen (1.0 mg/kg) every 12 h and IV injection of pentazocine at a dose of 30 mg as rescue analgesia if the VAS score was more than 4 points, which was repeated if necessary. After hospital discharge, the patients who felt pain and requested an analgesic were instructed to take 200 mg oral celecoxib tablets once daily.
OUTCOME MEASUREMENT:
The outcomes were pain scores measured by the VAS 0–10 (0 cm no pain and 10 cm worst pain) at rest and during activity (joint flexion more than 45°). VAS scores were recorded at 3 h, 6 h, 12 h, 24 h, and 48 h postoperatively, at discharge and at 1 week after hospital discharge. The outcomes were the frequency of administration of postoperative rescue analgesics, doses of oral celecoxib taken at 1 week after discharge, maximum walking distance at 24 h and 48 h postoperatively, and incidence of postoperative complications (eg, postoperative nausea and vomiting, puncture site infection, puncture site haematoma, urinary retention, nerve injury and foot drop).
In this study, 2 sets of records were established:
Record table 1: Researcher A was responsible for training patients to document their VAS scores at various time points following surgery. VAS scores were recorded at 3 h, 6 h, 12 h, 24 h, and 48 h postoperatively; as well as upon discharge and 1 week after hospital discharge. With the assistance of nurses, patients documented their maximum walking distance at 24 and 48 h after surgery. A standardized scale was placed at the entrance of each ward to ensure accurate recording by patients. The completed form was collected by Researcher A, who remained blinded to the specific trial groups throughout the study.
Record table 2: Researcher A reviewed the physician’s order system and nursing record sheets, noting the patient’s postoperative ward analgesia requirements and any incidence of postoperative complications, respectively. Researcher A compiled all trial data, which were subsequently analyzed by Researcher B, who remained blinded to the specific trial groups throughout the study.
STATISTICAL ANALYSIS:
We used SPSS version 25.0 software (SPSS, Inc., Chicago, IL, USA) for statistical analysis. Continuous variables are presented as the mean±standard deviation or median (interquartile ranges). Categorical variables are represented as percentages. One-way analysis of variance with post hoc Bonferroni correction was used for normally distributed continuous variables, and the Kruskal-Wallis analysis with post hoc Nemenyi test was used for skewed continuous variables. Chi-square or Fisher’s tests were applied for categorical variables. Subgroup analysis was performed for different surgical methods. A
Results
COMPARISON OF BASIC CHARACTERISTICS OF PATIENTS IN THE 3 GROUPS:
There were no significant differences in the baseline characteristics in the 3 groups – age, sex, type of surgery, duration of surgery, operative time, ASA classification, body mass index (BMI) and VAS score at rest and during activity at 24 h preoperatively (P>0.05) (Table 1).
COMPARISON OF POSTOPERATIVE VAS SCORES AMONG THE 3 GROUPS:
The VAS scores at rest and during activity at 6 h, 12 h, 24 h, and 48 h postoperatively were highest in C Group and lowest in A Group (P<0.05). Resting and active VAS scores at discharge and 1 week after discharge were similar among the 3 groups (P>0.05). Table 2 shows the statistical significance of the differences among the 3 groups (Table 2).
COMPARISON OF POSTOPERATIVE ANALGESIC CONSUMPTION AMONG THE 3 GROUPS:
The lowest frequency of postoperative rescue analgesia was recorded in Group A and the highest in Group C (P=0.001). There was no significant difference in the dose of postoperative oral analgesics among the 3 groups at 1 week after hospital discharge (P>0.05) (Table 3).
COMPARISON OF POSTOPERATIVE MAXIMUM WALKING DISTANCE AMONG 3 GROUPS:
The maximum walking distance 24 h and 48 h postoperatively was longer in Group A than in the other 2 groups. Table 4 presents the statistical significance of the differences among the 3 groups (P<0.05) (Table 4).
COMPARISON OF THE INCIDENCES OF POSTOPERATIVE ADVERSE REACTIONS AMONG THE 3 GROUPS:
The incidence of nausea and vomiting in Group A was significantly lower than in Group C (P<0.05). There was no significant difference in the incidence of postoperative urinary retention, puncture site infection, puncture site haematoma, nerve injury, or foot drop among the 3 groups (P>0.05) (Table 5).
SUBGROUP ANALYSIS AND COMPARISON:
A subgroup analysis was performed for the 3 types of surgery, including knee arthroscopic meniscus repair (Type 1 Group), meniscus repair+popliteal cyst resection (Type 2 Group), and arthroscopic cruciate ligament reconstruction (Type 3 Group). During knee arthroscopic meniscus repair surgery (Type 1 Group), the VAS scores during activity at 6 h, 12 h, 24 h, and 48 h postoperatively were the highest in the C1 Group, and the lowest in the A1 Group (P<0.05), while the VAS scores during activity at 6 h, 12 h, and 24 h postoperatively were highest in the C1 Group and lowest in the A1 Group (P<0.05). The same change was observed in the Type 2 Group (P<0.05). During arthroscopic cruciate ligament reconstruction of the knee joint (in the Type 3 Group), the VAS score at rest and during activity at 6 h and 12 h postoperatively was the highest in the C3 Group and the lowest in the A3 Group (P<0.05) (Table 6). The frequency of administration of postoperative rescue analgesia was significantly lower in Group A than in the other 2 groups (P<0.05). The maximum walking distance in Group A1 at 24 h and 48 h postoperatively was longer than in Group B1 and Group C1 in the Type 1 Group (P <0.05), and there was no significant difference in the maximum walking distance at 24 h and 48 h postoperatively in the Type 2 group and Type 3 Group (P>0.05). Postoperative vomiting in Group A2 in the Type 2 Group was significantly lower than in Group B2 and Group C2 (P>0.05) (Table 7).
Discussion
STRENGTHS AND LIMITATIONS:
The innovations of this study are as follows: (1) Most current studies on IPACK and ACB focused on postoperative analgesia and functional recovery after TKA surgery, and rarely studied AKS. AKS is similar to TKA surgery, but the surgical trauma is less than in TKA, so the study of IPACK and ACB is very significant for clinical diagnosis and treatment. (2) Through subgroup analysis, we analyzed the effects of IPACK combined with ACB on postoperative analgesia and rehabilitation of different types of AKS, and found that the effect of knee arthroscopic meniscus dressing and molding surgery was significantly better, which is conducive to guiding clinicians to selectively apply IPACK and ACB analgesia methods.
The present study has certain limitations. It had a small sample size and was a single-center study, so larger studies are needed to produce more generalizable results. The type of AKS was not significantly different among the 3 groups, and meniscus repair was the main type of AKS in the 3 groups. The size of the cruciate ligament reconstruction group was small (22–25% of the total sample size). Finally, the precision with which ultrasound-guided IPACK and ACB are performed affects drug diffusion, and the duration of a single-injection nerve block was limited.
Conclusions
The effect of postoperative analgesia in IPACK combined with ACB after AKS was obviously improved. In arthroscopic meniscus repair surgery, the duration of analgesia was longer, and the maximum walking distance at 48 h after surgery was longer.
Figures
 Figure 1. Ultrasound images demonstrating ACB; F – distal left lower limb; N – proximal left lower limb; I – inner thigh; SM – sartorius; A – femoral artery; V – venae femoris; arrows indicate the needle; anesthetic stands for injection target; – puncture needle into needle position; – ultrasonic probe placement position.
Figure 1. Ultrasound images demonstrating ACB; F – distal left lower limb; N – proximal left lower limb; I – inner thigh; SM – sartorius; A – femoral artery; V – venae femoris; arrows indicate the needle; anesthetic stands for injection target; – puncture needle into needle position; – ultrasonic probe placement position. 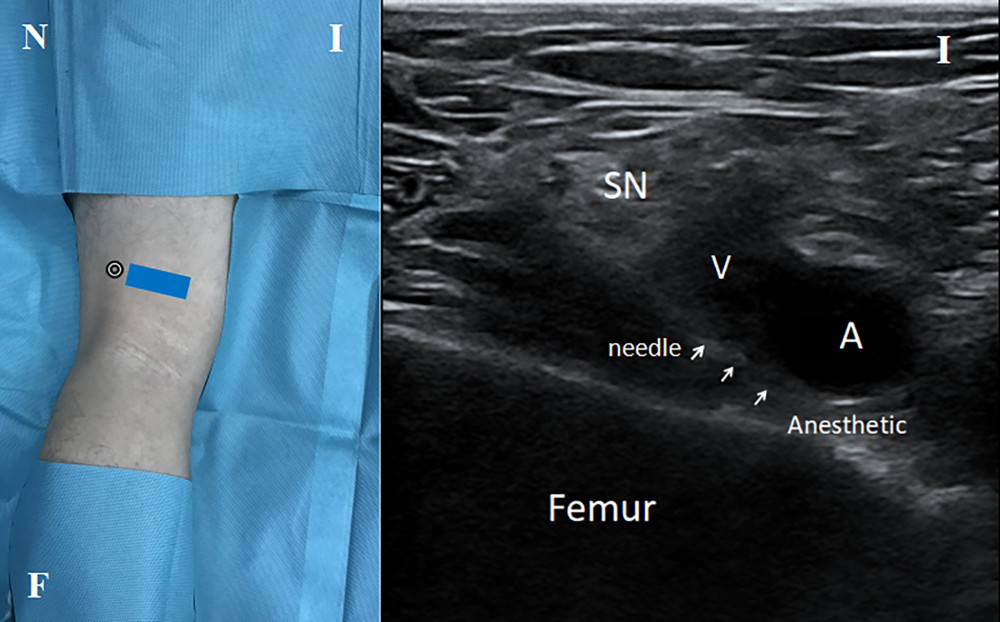 Figure 2. Ultrasound images demonstrating IPACK. SN – sciatic nerve; A – popliteal artery; V – popliteal vein; arrows indicate the needle; F – distal left lower limb; N – proximal left lower limb; I – inner thigh; SM – sartorius; A – popliteal artery; V – popliteal venae; arrows indicate the needle; anesthetic stands for injection target; – puncture needle into needle position; – ultrasonic probe placement position.
Figure 2. Ultrasound images demonstrating IPACK. SN – sciatic nerve; A – popliteal artery; V – popliteal vein; arrows indicate the needle; F – distal left lower limb; N – proximal left lower limb; I – inner thigh; SM – sartorius; A – popliteal artery; V – popliteal venae; arrows indicate the needle; anesthetic stands for injection target; – puncture needle into needle position; – ultrasonic probe placement position.  Figure 3. CONSORT diagram of patient flow through the study. ACB – adductor canal block; IPACK – Interspace between popliteal artery and posterior capsule of the knee; SA – apinal anesthesia; Group A – IPACK+ACB+SA (IPACK and ACB were selected as postoperative analgesia in arthroscopic knee surgery under single lumbar anesthesia); Group B – ACB+SA (ACB were selected as postoperative analgesia in arthroscopic knee surgery under single lumbar anesthesia); Group C – SA (nerve block is not selected as postoperative analgesia in arthroscopic knee surgery under single lumbar anesthesia).
Figure 3. CONSORT diagram of patient flow through the study. ACB – adductor canal block; IPACK – Interspace between popliteal artery and posterior capsule of the knee; SA – apinal anesthesia; Group A – IPACK+ACB+SA (IPACK and ACB were selected as postoperative analgesia in arthroscopic knee surgery under single lumbar anesthesia); Group B – ACB+SA (ACB were selected as postoperative analgesia in arthroscopic knee surgery under single lumbar anesthesia); Group C – SA (nerve block is not selected as postoperative analgesia in arthroscopic knee surgery under single lumbar anesthesia). Tables
Table 1. Comparison of basic data between the 3 groups (%). Table 2. Postoperative VAS pain scores at rest and during activity in the 3 groups (mean±SD).
Table 2. Postoperative VAS pain scores at rest and during activity in the 3 groups (mean±SD). Table 3. Frequency of postoperative rescue analgesia and the dose oral analgesics administered at 1-week after discharge in the 3 groups (mean±SD).
Table 3. Frequency of postoperative rescue analgesia and the dose oral analgesics administered at 1-week after discharge in the 3 groups (mean±SD). Table 4. Maximum postoperative distance in the 3 groups (mean±SD).
Table 4. Maximum postoperative distance in the 3 groups (mean±SD). Table 5. The incidence of postoperative complications in 3 groups (%).
Table 5. The incidence of postoperative complications in 3 groups (%). Table 6. Subgroup analysis of postoperative VAS scores after different types of surgery (mean±SD).
Table 6. Subgroup analysis of postoperative VAS scores after different types of surgery (mean±SD). Table 7. Subgroup analysis of different indicators after different types of surgery (mean±SD).
Table 7. Subgroup analysis of different indicators after different types of surgery (mean±SD).
References
1. Thorlund JB, Juhl CB, Roos EM, Arthroscopic surgery for degenerative knee: Systematic review and meta-analysis of benefits and harms: Br J Sports Med, 2015; 49(19); 1229-35
2. Alipour M, Sharifian Attar A, Akbari A, Intra-articular remifentanil on postoperative pain in knee arthroscopic surgery; A double blind randomized clinical trial: J Orthop Sci, 2023; 28(5); 1082-86
3. Tandra V, Koti M, Kohli S, Does local infiltration analgesia in total joint arthroplasty offer any protection from prosthetic joint infections? An invitro experimental study: J Perioper Pract, 2022; 1; 17504589221137981
4. Bhowmik S, Matthews D, Kumar AH, Targeting safe analgesia of the posterior knee capsule: J Knee Surg, 2024; 37(1); 84
5. Zhang LK, Li Q, Zhu FB, Comparison of adductor canal block with periarticular infiltration analgesia in total knee arthroplasty: A meta-analysis of randomized controlled trials: Medicine, 2019; 98(50); e18356
6. Edwards MD, Bethea JP, Hunnicutt JL, Effect of adductor canal block versus femoral nerve block on quadriceps strength, function, and postoperative pain after anterior cruciate ligament reconstruction: A systematic review of level 1 studies: Am J Sports Med, 2020; 48(9); 2305-13
7. Runge C, Moriggl B, Børglum J, The spread of ultrasound-guided injectate from the adductor canal to the genicular branch of the posterior obturator nerve and the popliteal plexus: A cadaveric study: Reg Anesth Pain Med, 2017; 42(6); 725-30
8. Khan MJ, Tauheed N, Siddiqui AH, Adductor canal block versus local infiltration analgesia for postoperative pain management in total knee arthroplasty: Cureus, 2024; 16(4); e57408
9. Tan M, Chen B, Li Q, Comparison of analgesic effects of continuous femoral nerve block, femoral triangle block, and adductor block after total knee arthroplasty: A randomized clinical trial: Clin J Pain, 2024; 40(6); 373-82
10. Hussain N, Brull R, Sheehy B, Does the addition of iPACK to adductor canal block in the presence or absence of periarticular local anesthetic infiltration improve analgesic and functional outcomes following total knee arthroplasty? A systematic review and meta-analysis: Reg Anesth Pain Med, 2021; 46(8); 713-21
11. Abdullah MA, Abu Elyazed MM, Mostafa SF, The interspace between popliteal artery and posterior capsule of the knee (IPACK) block in knee arthroplasty: A prospective randomized trial: Pain Physician, 2022; 25(3); E427-E33
12. Varacallo M, Luo TD, Mabrouk A: Total knee arthroplasty techniques, 2024, Treasure Island (FL), StatPearls Publishing Available from: https://www.ncbi.nlm.nih.gov/books/NBK499896/
13. Desu MM, Raghavarao D: Sample size methodology, 1990, New York(NY), Academic Press
14. Fleiss , Joseph L: The design and analysis of clinical experiments, 1986, New York(NY), John Wiley & Sons
15. Zheng FY, Liu YB, Huang H, The impact of IPACK combined with adductor canal block under ultrasound guidance on early motor function after total knee arthroplasty: Braz J Anesthesiol, 2022; 72(1); 110-14
16. Mou P, Wang D, Tang XM, Adductor canal block combined with IPACK block for postoperative analgesia and function recovery following total knee arthroplasty: A prospective, double-blind, randomized controlled study: J Arthroplasty, 2022; 37(2); 259-66
17. Tran J, Giron Arango L, Peng P, Evaluation of the iPACK block injectate spread: A cadaveric study: Reg Anesth Pain Med, 2019; 44; 689-94
18. Domagalska M, Reysner T, Kowalski G, Pain management, functional recovery, and stress response expressed by NLR and PLR after the iPACK block combined with adductor canal block for total knee arthroplasty – a prospective, randomised, double-blinded clinical trial: J Clin Med, 2023; 12(22); 7088
19. Kampitak W, Kertkiatkachorn W, Ngarmukos S, Comparison of analgesic efficacies of the iPACK (interspace between the popliteal artery and capsule of the posterior knee) and genicular nerve blocks used in combination with the continuous adductor canal block after total knee arthroplasty: a randomized clinical trial: J Arthroplasty, 2023; 38(9); 1734-41
20. Guo J, Hou M, Shi G, iPACK block (local anesthetic infiltration of the interspace between the popliteal artery and the posterior knee capsule) added to the adductor canal blocks versus the adductor canal blocks in the pain management after total knee arthroplasty: A systematic review and meta-analysis: J Orthop Surg Res, 2022; 17(1); 387
21. Tang X, Jiang X, Lei L, IPACK (interspace between the popliteal artery and the capsule of the posterior knee) block combined with SACB (single adductor canal block) versus SACB for analgesia after total knee arthroplasty: Orthop Surg, 2022; 14(11); 2809-21
22. Shoni M, Samineni AV, Salavati S, Combined single-shot infiltration between the popliteal artery and capsule of the knee and adductor canal block with bupivacaine, dexmedetomidine, and dexamethasone for total knee arthroplasty: A propensity-matched analysis: Arthroplast Today, 2023; 25; 101292
23. Kim J, Kim SH, Shin HY, Investigation of optimal needle position for radiofrequency ablation-based blockade of interspace between the popliteal artery and the posterior capsule of the knee: A cadaveric study: Medicina (Kaunas), 2024; 60(5); 689
24. Wang JH, Ma HH, Chou TA, Does the addition of iPACK block to adductor canal block provide improved analgesic effect in total knee arthroplasty? A systematic review and meta-analysis: J Knee Surg, 2023; 36(4); 345-53
25. Biehl M, Wild L, Waldman K, The safety and efficacy of the IPACK block in primary total knee arthroplasty: A retrospective chart review: Can J Anaesth, 2020; 67(9); 1271-73
26. Sreckovic SD, Tulic GDZ, Jokanovic MN, Delayed foot drop after a combination of the adductor canal block and IPACK block following total knee arthroplasty: J Clin Anesth, 2021; 73; 110363
27. Smulders PS, Ten Hoope W, Baumann HM, Adductor canal block techniques do not lead to involvement of sciatic nerve branches: A radiological cadaveric study: Reg Anesth Pain Med, 2024; 49(3); 174-78
28. Govender-Davies S, Davies L, Pillay-Addinall S, A cadaveric study investigating the spread of injectate following an interspace between the popliteal artery and the capsule of the posterior knee block in a neonatal sample: A pilot study: Anat Cell Biol, 2024; 57(2); 229-37
29. Wang CG, Ma WH, Liu R, The effect of continuous adductor canal block combined with distal interspace between the popliteal artery and capsule of the posterior knee block for total knee arthroplasty: A randomized, double-blind, controlled trial: BMC Anesthesiol, 2022; 22(1); 175
30. Hussain N, Brull R, Vannabouathong C, Analgesic effectiveness of motor-sparing nerve blocks for total knee arthroplasty: A network meta-analysis: Anesthesiology, 2023; 139(4); 444-61
31. Xue X, Lv X, Ma X, Postoperative pain relief after total knee arthroplasty: A Bayesian network meta-analysis and systematic review of analgesic strategies based on nerve blocks: J Clin Anesth, 2024; 96; 111490
Figures
Figure 1. Ultrasound images demonstrating ACB; F – distal left lower limb; N – proximal left lower limb; I – inner thigh; SM – sartorius; A – femoral artery; V – venae femoris; arrows indicate the needle; anesthetic stands for injection target; – puncture needle into needle position; – ultrasonic probe placement position.Figure 2. Ultrasound images demonstrating IPACK. SN – sciatic nerve; A – popliteal artery; V – popliteal vein; arrows indicate the needle; F – distal left lower limb; N – proximal left lower limb; I – inner thigh; SM – sartorius; A – popliteal artery; V – popliteal venae; arrows indicate the needle; anesthetic stands for injection target; – puncture needle into needle position; – ultrasonic probe placement position.Figure 3. CONSORT diagram of patient flow through the study. ACB – adductor canal block; IPACK – Interspace between popliteal artery and posterior capsule of the knee; SA – apinal anesthesia; Group A – IPACK+ACB+SA (IPACK and ACB were selected as postoperative analgesia in arthroscopic knee surgery under single lumbar anesthesia); Group B – ACB+SA (ACB were selected as postoperative analgesia in arthroscopic knee surgery under single lumbar anesthesia); Group C – SA (nerve block is not selected as postoperative analgesia in arthroscopic knee surgery under single lumbar anesthesia). Tables
Table 1. Comparison of basic data between the 3 groups (%).Table 2. Postoperative VAS pain scores at rest and during activity in the 3 groups (mean±SD).Table 3. Frequency of postoperative rescue analgesia and the dose oral analgesics administered at 1-week after discharge in the 3 groups (mean±SD).Table 4. Maximum postoperative distance in the 3 groups (mean±SD).Table 5. The incidence of postoperative complications in 3 groups (%).Table 6. Subgroup analysis of postoperative VAS scores after different types of surgery (mean±SD).Table 7. Subgroup analysis of different indicators after different types of surgery (mean±SD).Table 1. Comparison of basic data between the 3 groups (%).Table 2. Postoperative VAS pain scores at rest and during activity in the 3 groups (mean±SD).Table 3. Frequency of postoperative rescue analgesia and the dose oral analgesics administered at 1-week after discharge in the 3 groups (mean±SD).Table 4. Maximum postoperative distance in the 3 groups (mean±SD).Table 5. The incidence of postoperative complications in 3 groups (%).Table 6. Subgroup analysis of postoperative VAS scores after different types of surgery (mean±SD).Table 7. Subgroup analysis of different indicators after different types of surgery (mean±SD). In Press
Clinical Research
Body Weight and Insulin Resistance Indicators Among ChildrenMed Sci Monit In Press; DOI: 10.12659/MSM.951434
Clinical Research
Comparison of Radiographic Cervical Sagittal Alignment Parameters in Patients With Nonspecific Neck Pain, D...Med Sci Monit In Press; DOI: 10.12659/MSM.952950
Clinical Research
Combined Fibrinogen and Urinary α1-Microglobulin as Predictors of Respiratory Tract Infection in Children w...Med Sci Monit In Press; DOI: 10.12659/MSM.951066
Database Analysis
Evaluation of Salivary Total Oxidant Status (TOS) and Total Antioxidant Status (TAS) in Orthodontic Patient...Med Sci Monit In Press; DOI: 10.12659/MSM.952052
Most Viewed Current Articles
17 Jan 2024 : Review article 14,175,576
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,756,620
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,465,966
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,651
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387