11 June 2024: Clinical Research
Development and Evaluation of the Italian Version of the Dichotic Digit Test: Insights from 39 Normal-Hearing Children Aged 11 to 13 Years
Milaine Dominici SanfinsDOI: 10.12659/MSM.944090
Med Sci Monit 2024; 30:e944090






Abstract
BACKGROUND: The dichotic digit test (DDT) is one of the tests for the behavioral assessment of central auditory processing. Dichotic listening tests are sensitive ways of assessing cortical structures, the corpus callossum, and binaural integration mechanisms, showing strong correlations with learning difficulties. The DDT is presently available in a number of languages, each appropriate for the subject’s native language. However, there is presently no test in the Italian language. The goal of this study was to develop an Italian version of the one-pair dichotic digit test (DDT-IT) and analyze results in 39 normal-hearing Italian children 11 to 13 years old. We used 2 conditions of presentation: free recall and directed attention (left or right ear), and looked at possible effects of sex and ear side.
MATERIAL AND METHODS: This study involved 3 steps: creation of the stimuli, checking their quality with Italian speakers, and assessment of the DDT-IT in our subject pool. The study involved 39 children (26 girls and 13 boys), aged 11-13 years. All participants underwent basic audiological assessment, auditory brainstem response, and then DDT-IT.
RESULTS: Results under free recall and directed attention conditions were similar for right and left ears, and there were no sex or age effects.
CONCLUSIONS: The Italian version of DDT (DDT-IT) has been developed and its performance on 39 normal-hearing Italian children was assessed. We found there were no age or sex effects for either the free recall condition or the directed attention condition.
Keywords: Auditory Perceptual Disorders, Dichotic Listening Tests, Hearing Tests, Language Development Disorders, Speech Perception, Humans, Female, Male, Child, Adolescent, Italy, Language, Hearing, Auditory Perception, Attention
Introduction
Adequate functioning of the peripheral auditory system and the central auditory nervous system (CANS) are crucial for communication and learning. The American Speech-Language-Hearing Association [1] recommends that 6 underlying auditory mechanisms be evaluated in assessing central auditory processing (CAP). Among them, ability to separate competing acoustic signals is arguably the most important. The standard way to assess this is to present different acoustic stimuli to both ears simultaneously and ask the listener to repeat what they heard in each ear. This is the basis of the dichotic listening task. Such dichotic listening tests are sensitive ways of assessing cortical structures, the corpus callossum, and successful binaural integration. There is a strong correlation between poor dichotic performance and learning difficulties [2].
Since the 1960s there has been continuing interest in one specific test – the Dichotic Digit Test (DDT) – and its relationship with information processing and cortical structures. DDT has been widely used to assess binaural integration, the ability to process different stimuli presented to each ear at the same time [3]. Kimura [4] was one of its pioneers, and used DDT based on 3 pairs of digits in patients with unilateral lesions of the temporal lobe. Kimura found that there was a deterioration in the recognition of digits in the left ear when stimuli were presented simultaneously. Recent research has shown that central auditory processing disorder (CAPD) can be identified in subjects with traumatic brain injury [5].
Research has demonstrated that individuals with damage to the left temporal lobe have a higher percentage of correct responses in the right ear during dichotic listening tasks, even more so than normal individuals without auditory processing deficits, indicating a right ear advantage (REA). These findings prove the superiority of the right ear, which has more numerous contralateral than ipsilateral pathways, reflecting the fact that the left cerebral hemisphere plays a more important role in the perception of verbal stimuli [4].
DDT has also been mentioned as a possible screening protocol for auditory ability. The advantage of using DDT is that it is easy to perform, it is relatively quick, and it is a test model that reduces memory dependency [6–9]. This test revealed inferior binaural integration in mouth breathers with abnormal polysomnography [10], attention deficit disorder, hyperactivity (ADHD), dyslexia [11,12], phonological disorders [13], stroke [5,14], and school difficulties [15,16].
The research potential of dichotic tests, especially the DDT, derives from the fact that changes in the DDT may be associated with impairments in learning, academic performance, reading and writing skills, difficulties in classroom behavior, and others [16–19]. It can be applied from the age of 5 years, enabling assessment from the earliest school years [20–21]. Because of these features, it is widely recommended and is considered the most valuable of the CAPD tests. The DDT is recommended in children, since if any alteration is found an auditory training program can be developed to improve communication [22–24].
DDT is capable of monitoring interaural asymmetry, which can be impaired, particularly in elderly adults who have difficulty understanding speech [25]. In a literature review and meta-analysis of subjects with dementia who underwent the dichotic digit test, the authors found that, in terms of REA, participants with dementia had an increased REA. After 1.5 years of follow-up, such subjects also had more of an REA than did controls, and this was due to a decrease in the DDT score for the left ear. These findings suggest a possibly higher rate of corpus callosum atrophy in patients with Alzheimer disease [26].
There are different modes of implementing DDT. For example, the primary stimuli on which it is based can involve digits or syllables, and the stimuli can be presented in a single pair or multiple pairs. However, tests with 1 or 2 pairs are the most used [27]. Other more cognitively challenging variations of DDTs were also used in previous research to avoid the ceiling effects found in 2-digit pairs test paradigms [28] such as using 3-digit pairs [29] or randomly presented 1-, 2-, and 3-pair dichotic digit stimuli [30]
The DDT test is available in different languages and should be applied in the child’s native language [20,31–34]. However, until now the test has not been available in Italian. The goal of the present study was to develop an Italian version of the 1-pair dichotic digit test (DDT-IT). We aimed to evaluate the performance of typically hearing Italian children aged 11 to 13 years old under 2 conditions: free recall and directed attention (to the left or right ear). Specifically, we focused on examining the influence of sex and ear side.
Material and Methods
ETHICS:
This study was approved by the University of Ferrara’s Ethics in Research Committee (protocol number 160387). Written informed consent was obtained from the parents of all the participating children prior to data collection.
PARTICIPANTS:
The sample size was calculated based on the sample mean estimator, with an error of ±0.3 on average, a significance level of 5%, and considering the standard deviation of a previous study related to the same measure in this study. The result was a target sample size of 25 individuals. In practice, however, this study recruited 39 children, comprising 26 girls and 13 boys, with ages between 11 and 13 years (mean 11.9,
INCLUSION AND EXCLUSION CRITERIA: All subjects passed the following inclusion criteria: a hearing threshold <15 dB HL (250 to 8000 Hz) [35]; type A tympanogram with presence of ipsilateral and contralateral acoustic reflexes (500 to 4000 Hz) in both ears [36]; otorhinolaryngological evaluation showing no anatomical changes or presence of earwax; and values within the limits of normality for click auditory brainstem responses (ABRs) for waves I, III, and V and inter-peak intervals I–III, III–V, and I–V for both ears [37].
EXCLUSION CRITERIA:
Exclusion criteria were a diagnosis of neurodevelopmental disorder (ADHD, dyslexia, or others), hearing loss, history of otitis media, and history of other neurological or psychiatric condition. In addition, the pedagogical coordinator of the school provided a profile of the child’s academic performance via a questionnaire.
PERIPHERAL AUDITORY SYSTEM: Tympanometry and acoustic reflexes were measured with an Interacoustic AT235 audiometer and a 226 Hz probe. Acoustic reflexes had a maximum compliance near 0 da Pa and an equivalent volume of 0.3 to 1.3 ml according to Jerger’s proposal [36]. Pure tone audiometry (PTA) was performed using an Interacoustic AC40 audiometer and TDH39 earphones following the normality criterion from the World Health Organization classification for children [35]. The speech audiometry involved speech recognition threshold (list of disyllables with 50% accuracy score) and speech recognition index (list of monosyllabic words 40 dB above the average tonal threshold and an accuracy score between 88% and 100%).
AUDITORY BRAINSTEM RESPONSES (ABRS): The integrity of the auditory pathway was checked using the Navigator Pro equipment from Biologic/Natus. The active electrode (Fz) was placed on the forehead and the reference electrodes were on the right (M2) and left (M1) mastoids, with the ground electrode on Fpz [38]. Stimuli were 0.1 ms rarefaction clicks delivered at 19.3 clicks/sec, low/high pass filter 0.1–3 kHz, analysis window of 12 ms, 2000 stimuli, 80 dB HL. Measurements were made of the amplitude of waves I, III, and V and the inter-peak latencies of I–III, I–V, and III–V. To check reproducibility, 2 recordings were made on each side and the criteria values were from Gorga et al [37].
DEVELOPMENT OF DDT-IT: The development of DDT-IT was based in previous studies where single-pair stimuli were used [20–32]. The individual steps were as listed below.
STEP 1: CREATION OF STIMULUS:
Audacity software was used to create pairs of Italian spoken digits. The digits were spoken by an Italian native male, aged 36 years old, in a normal clear voice and recorded in an anechoic chamber. Five Italian disyllables (quattro, cinque, sette, otto, and nove) were chosen and these numbers were randomly combined 2 by 2, eliminating cases of equal numbers.
The digits were edited to remove noise or excessive silence between them. The onsets of each pair of digits coincided to within 70 ms, which is the normal range of onset times critical for maintaining dichotic perception. Similarly, the offset times did not differ by more than 70 ms, and a 0.5-sec silent interval between each pair of dichotic digits was added. An interstimulus interval of 5 sec was inserted between each pair to allow an adequate response time [20]. The digits were then dichotically presented over 2 separate channels. The ordering of the pairs was random, creating a list of 20 pairs of digits. The one-pair DDT-IT has 2 lists (see Table 1).
STEP 2: PREPARATORY CHECK BY ITALIAN SPEAKERS:
After the auditory material had been produced, a quality control check was made by playing the digits to 20 native Italians to confirm that all the digits could be clearly heard and identified. The participants in this stage of the study were professionals who are part of the Audiology and ENT team at our university. It should be noted that no type of adjustment was necessary in the test. An Italian version of the one-pair DDT-IT can be downloaded as Supplementary Material. Additionally, the file is available in an open-source database such as Zenodo (
STEP 3: PRESENTATION OF THE ACTUAL DDT-IT: The DDT-IT test involves presenting list 1 to the left ear and list 2 to the right ear (Table 1). That is, the subject hears 2 digits in one ear and 2 in the other, amounting to 4 in total. The pairs are presented through 2 channels of the Interacoustic AC40 audiometer and TDH39 earphones at an intensity of 50 dB SL (average of 500, 1000, and 2000 Hz). The test is administered 4 times. The test is also done in 2 different ways: a free recall task and a directed attention task.
Free recall (FR): This procedure tests for binaural integration. The list of 20 pairs of digits is presented dichotically and individuals are asked to repeat all the digits heard (Figure 1). Before each presentation of 4 digits, the subject hears the word “repeat”, reinforcing the message that they need to repeat all the digits heard (in any order).
Directed attention (DA): This procedure tests the subject’s ability to selectively attend to 1 ear. A list of 20 pairs of digits is presented dichotically and individuals are instructed to repeat only the digits presented to the specified ear. Before each presentation, the individual hears the word “repeat” to reinforce the message that they need to repeat the stimuli heard. There are 2 possible conditions: directed attention to the right ear (DARE) (Figure 2) and directed attention to the left ear (DALE) (Figure 3), and both were part of the stimulus protocol.
The answers were recorded by placing a circle around the identified digit by researcher. Each correctly identified number was considered a success and each omitted or wrongly identified number was considered an error. The total number of errors made was computed.
To calculate the DDT-IT score, it was considered that a total of 20 sequences of 4 digits are presented, 2 digits to each ear, for a total of 80 digits (40 to ear). The participant is instructed to repeat all 4 digits they heard. The score is calculated for each ear separately. Each correctly repeated digit represents 2.5% of the total score (2.5×40=100%). Therefore, the maximum score for each ear in the free recall protocol is 100%.
For the directed attention protocol, we assumed that a total of 20 sequences of 4 digits are presented, 2 digits to each ear, for a total of 40 digits in each ear. The participant is instructed to repeat only the digits presented to the specific ear being tested (eg, left ear only). Each correctly repeated digit in the designated ear represents 2.5% of the total score (2.5×40=100%). The maximum score for each ear in the directed attention protocol is also 100%.
STATISTICAL ANALYSES:
Descriptive statistics were calculated for quantitative variables and a Shapiro-Wilk test was used to check the assumption of normality. A Wilcoxon test for paired samples (the result of this test is denoted by the symbol Z), and a Mann-Whitney U test (the symbol is U) or a Kruskal-Wallis test (the symbol is H), were also applied. Statistical analysis was performed using IBM SPSS Statistics (v.24);
Results
DDT-IT RESULTS BY GENDER AND AGE:
In terms of sex, 1-pair DDT-IT results obtained by girls and boys were similar, and this is shown in Figure 4.
DDT results in girls and boys did not differ significantly for any of the conditions: free recall right ear,
Table 3 shows the mean scores and standard deviations calculated for groups of children of different ages. There were no statistically significant differences in DDT-IT results between the age groups. Children in different age groups did not differ in terms of results obtained in the free recall condition for the right ear (H=0.21; P=0.900), nor for the left ear (H=0.19; P=0.910). They had similar results in the directed attention condition for the right ear (H=1.91; P=0.384), and for the left ear (H=1.40; P=0.497).
Discussion
FREE RECALL (FR):
Dichotic tests are essentially binaural integration tasks and employ the performance of the corpus callosum and the right and left cerebral hemispheres. The lack of difference in performance as a function of age of our subjects may be explained by the maturation and myelination of these structures. We did not see an advantage of the right ear over the left, as observed in other studies carried out in younger children (<9 years). The DDT in the FR condition assesses selective attention and figure-ground separation ability [2,7,9,10,18,32,39,46].
Children diagnosed with central auditory processing disorder, cognitive disabilities, trauma, or brain injuries may benefit from the DDT evaluation, as their performance was lower than that of their peers without abnormalities. The observed inefficiency in dichotic information processing could potentially be linked to challenges encountered during sustained attention, impaired hemispheric integration of auditory information, or difficulty recognizing verbal sounds [47]. Performance in children seems to depend very much on attention and memory, and so we expected that performance might be impaired in children lacking these abilities [2,3,5,7–9,11,12,14–20]. Auditory skills that require the interaction of the 2 hemispheres, such as tested with the dichotic listening task, depend on the integrity of the corpus callosum. Any changes in the corpus callosum can lead to major impairments in auditory skills and, consequently, in speech, oral language, written language, and learning skills [48–52].
The values we have calculated for the FR condition are similar to those described in the literature [15,20,32,33,44]. Our study corroborates the findings of other research which has employed one-pair DDT: typically, children over 11 years of age and without hearing disorders achieve scores around 100% and have no (or only subtle) differences between the ears [32,33,44]. In our comparison of the different age groups in the FR task, the scores were very similar in those aged 11, 12, or 13. This finding agrees with Keith (2000), who found that children of this age display similar values to those of adults. A performance ceiling seems to be reached at about 11 years of age [53].
DIRECTED ATTENTION (DA):
In the DA condition, the DDT evaluates figure-ground ability for verbal sounds and the effects of sustained attention and selective attention [7,15,18,46]. In the literature, normative values differ depending on age. We found that at ages 11 to 13 years values for both DARE and DALE are like those found in previous studies [15,20,32]. In this context, the literature reports that from the age of 11 onwards, children’s responses are similar to those found in adults [41,43,44,54].
In dichotic tests the right ear always presents an advantage, and this has been reported in multiple studies. The advantage of the right ear is called REA and is probably due to the greater involvement of the left hemisphere in the processing of verbal stimuli. The effective participation of the corpus callosum is also important [55,56]. REA is more pronounced in young children and fades away with advancing age [41,57,58].
Although we found no statistically significant differences, our data (Table 3) show a better DA response in the right ear at 11 and 13 years old, while at 12 years old the DARE and DALE are about the same. These findings may be related to the degree of difficulty, or rather the lack thereof, in the 1-pair DDT. Experiments based on 1-pair DDT, that is, using a pair of digits in each ear, show that such digits can be easily identified [59–62]. Furthermore, individuals use digits constantly in their daily lives, meaning there could be no need for involvement of the dominant hemisphere, particularly in older children and adults [63].
Prior research conducted on children has demonstrated that REA is not evident in children who have articulation disorders and learning disabilities [12,64–66]. Children who experienced challenges in reading and writing exhibited changes in their left auditory performance [54,63]. People who have a stutter tend to exhibit reduced RE, particularly in children, compared to adults with the same condition [67]. Finally, researchers demonstrated that hemispheric lesions caused altered outcomes in the contralateral ear, but the altered results in both ears indicate alterations in the left hemisphere. Particularly in children, it can serve as a useful screening method for identifying central auditory dysfunctions [15,17,39].
The more difficult the task to be performed, the greater the difference between the ears; however, attentional and cognitive aspects can also influence the responses. A study comparing literate and non-literate subjects showed that a right-ear advantage was only observed in the non-literate [68], which suggests that learning a language stimulates both hemispheres – that is, activity in the corpus callosum tends to even out left and right ear responses.
In future studies, it may help to make the test more difficult by increasing the number of pairs of digits and/or randomizing the presentation of numbers. This might lead to a greater difference in responses between the ears [43,69,70]. It appears that the 1-pair DDT is not an effective way of measuring REA, even though it has been shown to be a sensitive instrument for monitoring general changes in the CANS [21].
FINAL CONSIDERATIONS:
Dichotic digit test protocols are an audiological part of diagnostic batteries. The DDT has been shown to be very effective in identifying neurological disorders in the main central auditory relay stations, such as the brainstem, cortex, and corpus collosum [1,2,20]. DDT has also been mentioned as a possible screening protocol for auditory abilities. The advantage of the DDT is that the test is easy to perform, relatively quick, and requires a low level of linguistic ability [7,8].
The DDT evaluation under both assessment situations (FR and DA) will provide relevant information regarding dichotic listening ability and can be utilized to analyze the integrity of the central auditory nervous system [1,4,6,7,15,20]. Evaluators have the option to select a single evaluation condition, but this decision will be influenced by the patient’s cognitive condition and the desire to obtain more detailed information about the auditory system, such as the analysis of binaural separation (DA) or binaural integration (FR) [1,2,7–9,20,25,30,39,46,62].
By analyzing the current literature, it is possible to find other behavioral tests that can evaluate dichotic listening (eg, dichotic sentences test). The inclusion of a comparative test could strengthen the application of DDT-IT. However, finding another test that taps into these exact aspects can be difficult because existing tests might focus on different aspects of CAP altogether (eg, sound localization), specific auditory processing skills not directly related to dichotic listening (eg, speech comprehension), and suffer from different influences (eg, short-term auditory memory), which could make this comparison less direct and less meaningful [1,4,9,11,15,19].
LIMITATIONS AND THE FUTURE:
One of the limitations of the present study is that the individuals were close in age and there were no younger children. Nevertheless, the current research has allowed an Italian version of a 1-pair dichotic digit test (DDT-IT) to be developed. Nevertheless, further investigation is required, and normative data must be acquired. Additionally, we suggest that the assessment be implemented for children who, among other conditions, suffer from learning disabilities and auditory processing disorders. Exploring age effects in a broader age range, including either a group of elderly participants or young children, could be an interesting avenue for future research. Examining populations with potentially immature corpus callosum development could provide valuable insights into the development of dichotic listening abilities.
Conclusion
An Italian version of the DDT (DDT-IT) has been developed and the responses of a small group of Italian normal children tested. Analysis has shown that, for both the free recall and directed attention condition, there are no statistically significant differences for age or sex.
Supplementary File
Italian Version of Dichotic Digit Test (DDT-IV).
https://zenodo.org/records/10783638
Figures
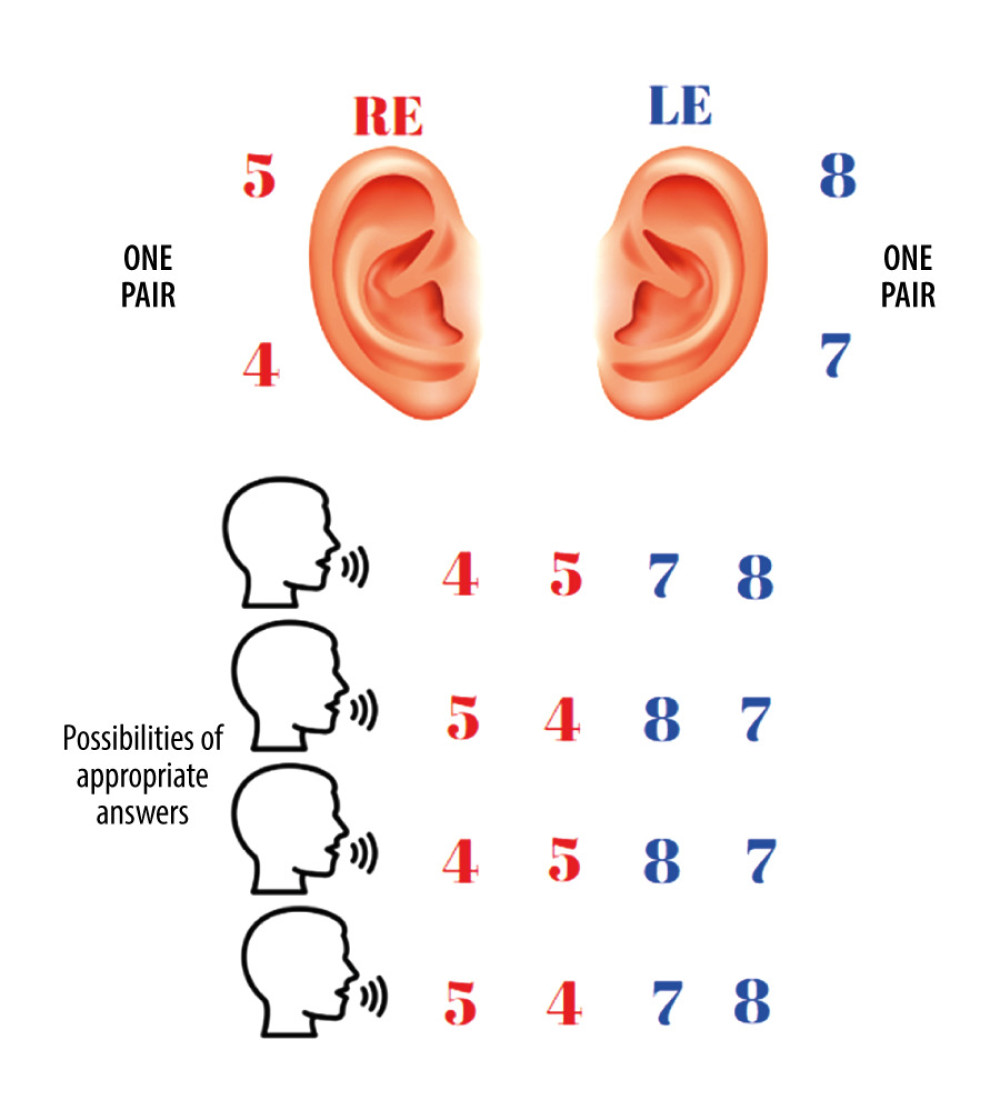 Figure 1. Diagram of the free recall condition and possible answers. The digits can be repeated in any order.
Figure 1. Diagram of the free recall condition and possible answers. The digits can be repeated in any order. 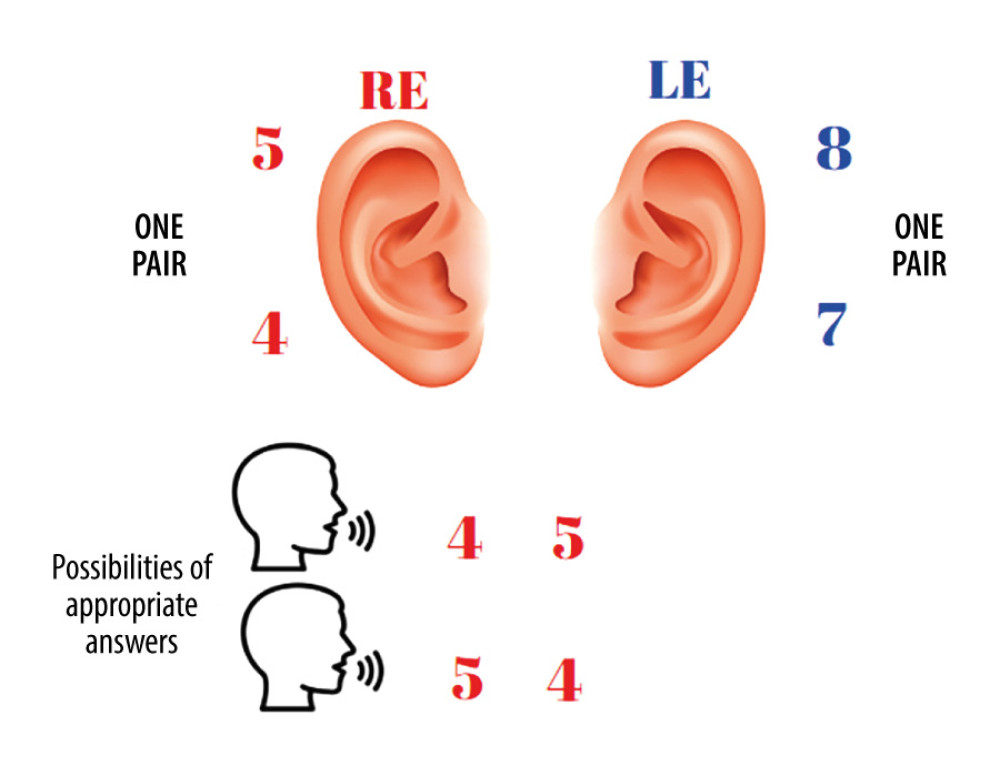 Figure 2. Diagram of directing attention only to the right ear (DARE) and possible answers.
Figure 2. Diagram of directing attention only to the right ear (DARE) and possible answers. 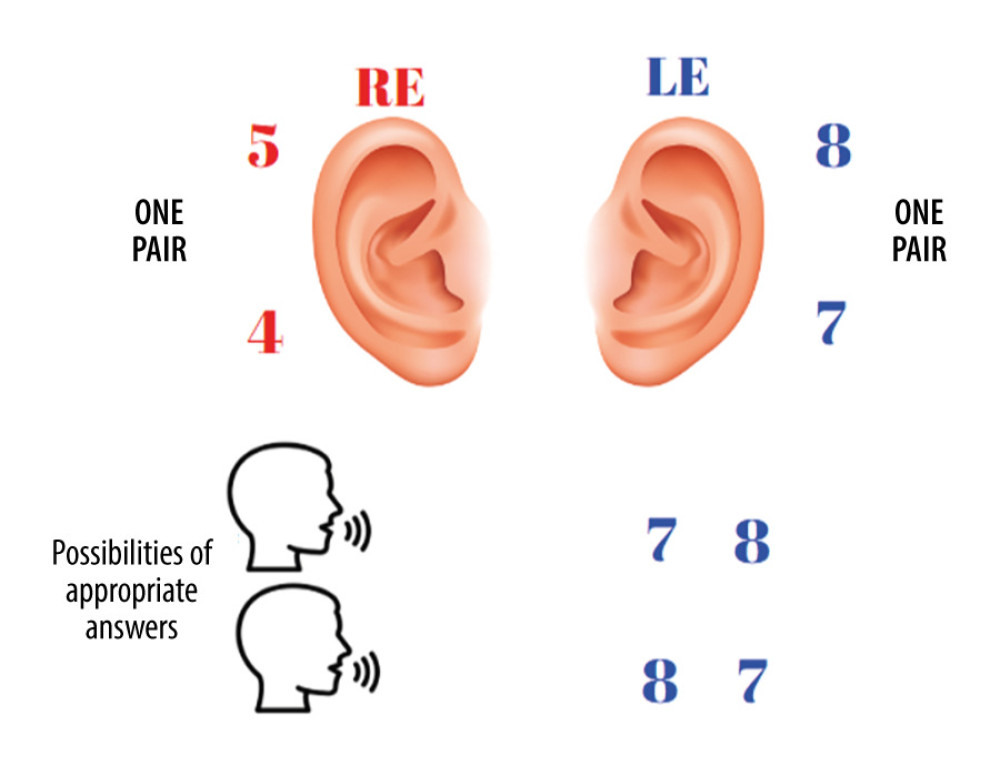 Figure 3. Diagram of directing attention to the left ear (DALE) and possible answers.
Figure 3. Diagram of directing attention to the left ear (DALE) and possible answers. 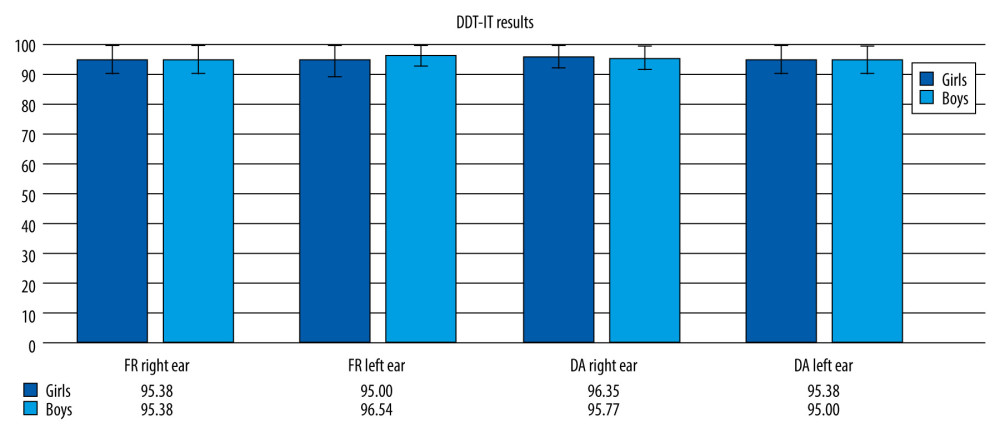 Figure 4. One-pair DDT-IV results in girls and boys.
Figure 4. One-pair DDT-IV results in girls and boys. References
1. American Speech-Language-Hearing Association: 2005 (central) auditory processing disorders – the role of the audiologist [Position Statement] Available from: www.asha.org/policy
2. Weihing J, Atcherson SR, Dichotic listening tests: Handbook of central auditory processing disorder, 2014; 369-404, San Diego, CA, Plural Publishing
3. Fischer ME, Cruickshanks KJ, Nondahl DM, Dichotic digits test performance across the ages: Results from two large epidemiologic cohort studies: Ear Hear, 2017; 38(3); 314-20
4. Kimura D, Some effects of temporal-lobe damage on auditory perception: Can J Psychol, 1961; 156-65
5. Godoy CCF, Andrade AN, Suriano I, Central auditory processing in children after traumatic brain injury: Clinics (Sao Paulo), 2022; 77; 100118
6. Musiek FE, Chermak GD, Weihing J, Diagnostic accuracy of established central auditory processing test batteries in patients with documented brain lesions: J Am Acad Audiol, 2011; 22(6); 342-58
7. Jerger J, Musiek F, Report of the consensus conference on the diagnosis of auditory processing disorders in school-aged children: J Am Acad Audiol, 2000; 11(9); 467-74
8. Carvalho NG, Novelli CVL, Colella-Santos MF, Performance of school-aged children in the basic audiological evaluation and the binaural integration task: Audiology Communication Research, 2018; 23; e2016
9. Gokula R, Sharma M, Cupples L, Valderrama JT, Comorbidity of auditory processing, attention, and memory in children with word reading difficulties: Front Psychol, 2019; 10; 2383
10. Ziliotto KN, Santos MFC, Monteiro VG, Avaliação do processamento auditivo em crianças com síndrome da apneia/hipopnéia obstrutiva do sono: Rev Bras Otorrinolaringol, 2006; 72(3); 321-27 [in Portuguese]
11. Wit E, Dijk PV, Hanekamp S, Visser-Bochane MI, Same or different: The overlap between children with auditory processing disorders and children with other developmental disorders: A systematic review: Ear Hear, 2017; 39(1); 1-19
12. Thomson JM, Leong V, Goswami U, Auditory processing interventions and developmental dyslexia: A comparison of phonemic and rhythmic approaches: Reading and Writing: An Interdisciplinary Journal, 2013; 26(2); 139-61
13. Attoni TM, Quintas VG, Mota HB, Auditory processing, acoustic reflex and phonological expression: Braz J Otorhinolaryngol, 2010; 76(6); 753-61
14. Elias KMIF, Moura-Ribeiro MVL, Stroke caused auditory attention déficits in children: Arq Neuropsiquiatr, 2013; 71(1); 11-17
15. Skarzynski PH, Wlodarczyk AW, Kochanek K, Central auditory processing disorder (CAPD) tests in a school-age hearing screening programme – analysis of 76,429 children: Ann Agric Environ Med, 2015; 22; 90-95
16. Sanfins MD, Borges LR, Ubiali T, Colella-Santos MF, Speech auditory brainstem response (speech ABR) in the differential diagnosis of scholastic difficulties: Braz J Otorhinolaryngol, 2017; 83; 112-16
17. Carvalho NG, Ubiali T, Amaral MIR, Colella-Santos MF, Procedures for central auditory processing screening in school children: Rev Bras Otorrinolaringol, 2019; 85(3); 319-28
18. Bamiou DE, Musiek FE, Luxon LM, Etiology and clinical presentations of auditory processing disorders: Arch Dis Child, 2001; 85(5); 361-65
19. Dawes P, Bishop DVM, Sirimanna T, Bamiou DE, Profile and aetiology of children diagnosed with auditory processing disorder (APD): Int J Pediatr Otorhinolaryngol, 2008; 72; 483-89
20. Musiek FE, Assessment of central auditory dysfunction: The dichotic digit test revisited: Ear Hear, 1983; 4; 79-83
21. Dillard LK, Fischer ME, Pinto AK, Longitudinal decline on the dichotic digits test: Am J Audiol, 2020; 29(4); 862-72
22. Sanfins MD, Borges LR, Ubiali T, Colella-Santos MF, Speech auditory brainstem response (speech ABR) in the differential diagnosis of scholastic difficulties: Braz J Otorhinolaryngol, 2017; 83; 112-16
23. Donadon C, Sanfins MD, Borges LR, Colella-Santos MF, Auditory training: Effects on auditory abilities in children with history of otitis media: Int J Pediatr Otorhinolaryngol, 2019; 118; 177-80
24. Loo JHY, Rosen S, Bamiou DE, Auditory training effects on the listening skills of children with auditory processing disorder: Ear Hear, 2016; 37(1); 38-47
25. Bellis T, Differential diagnosis of CAPD in older listeners: Handbook of central auditory processing disorder: volume 1: Diagnosis, 2007, San Diego, Plural
26. Utoomprurkporn N, Hardy CJD, Stott J, “The Dichotic Digit Test” as an index indicator for hearing problem in dementia: Systematic review and meta-analysis: J Am Acad Audiol, 2020; 31(9); 646-55
27. Rajabpour E, Hajiabolhasan F, Tahaei AA, Jalaei S, Development of persian single dichotic digit test and its reliability in 7 to 9 year old male students (Persian): Audiology, 2014; 23(5); 68-77
28. Strouse A, Wilson RH, Stimulus length uncertainty with dichotic digit recognition: J Am Acad Audiol, 1999; 10(4); 219-29
29. Duchek JM, Balota DA, Failure to control prepotent pathways in early stage dementia of the Alzheimer’s type: Evidence from dichotic listening: Neuropsychology, 2005; 19(5); 687-95
30. Strouse A, Wilson RH, Recognition of one-, two-, and three-pair dichotic digits under free and directed recall: J Am Acad Audiol, 1999; 10(10); 557-71
31. Bellis TJ: Assessment and management of central auditory processing disorders in the educational setting: From science to practice, 1996; 347, San Diego, Singular
32. Santos MF, Pereira LD, Escuta com dígitos: Processamento auditivo central – manual de avaliação, 1997; 147-50, São Paulo, Lovise [in Portuguese]
33. Rezapour M, Abdollahi FZ, Delphi M, Normalization and reliability evaluation of persian version of two-pair dichotic digits in 8 to 12-year-old children: Iranian Rehabilitation Journal, 2016; 14(2); 115-20
34. Andrade AN, Gil D, Iorio MCM, Benchmarks for the Dichotic Sentence Identification test in Brazilian Portuguese for ear and age: Braz J Otorhinolaryngol, 2015; 81(5); 459-65
35. WHO: Grades of hearing impairment 2014 [Available from:]https://www.who.int/pbd/deafness/hearing_impairment_grades/en/
36. Jerger J, Clinical experience with impedance audiometry: Arch Otolaryngol, 1970; 92(4); 311-24
37. Gorga MP, Kaminishi JR, Beauchaine KL, Auditory brainstem responses from children three months to three years of age: normal patterns of response: J Speech Hear Res, 1989; 32; 281-88
38. Jasper HA, The ten-twenty system of the International Federation: Electroenceph Clin Neurophysiol, 1958; 10; 371-75
39. Musiek FE, Gollegly KM, Kibbe KS, Verkest-Lenz SB, Proposed screening test for central auditory disorders: Follow-up on the Dichotic Digits Test: Am J Otol, 1991; 12; 109-13
40. Asbjørnsen AE, Helland T, Dichotic listening performance predicts language comprehension: Laterality, 2006; 11(3); 251-62
41. Jutras B, Mayer D, Joannette E, Assessing the development of binaural integration ability with the French dichotic digit test: Ecoute dichotique de chiffres: Am J Audiol, 2012; 21(1); 51-59
42. Liu SY, Liao JS, Dichotic digit listening in Mandarin and English by Mandarin-speaking adults: Journal of the Acoustical Society of America, 2010; 127(3); 1956-58
43. Castro FZ, Suárez MS, Cosialls SM, Prat JJB, La evaluación del procesamiento auditivo central: el test de dígitos dicóticos: Revista de Logopedia, Fonitatria Y Audiologia, 2007; 27(2); 74-85 [in Portuguese]
44. Mukari SZ, Keith RW, Tharpe AM, Johnson CD, Development and standardization of single and double dichotic digit tests in the Malay language: Int J Audiol, 2006; 45(6); 344-52
45. Kimura D, Speech lateralization in young children as determined by an auditory test: J Comp Physiol Psychol, 1963; 56; 899-902
46. Morris R, Bakker DJ, Satz P, Van der Vlugt H, Dichotic listening ear asymmetry: Patterns of longitudinal development: Brain Lang, 1984; 2; 49-66
47. Musiek FE, Weihing J, Perspectives on dichotic listening and the corpus callosum: Brain Cogn, 2011; 76(2); 225-32
48. Demopoulos C, Arroyo MS, Dunn W, Individuals with agenesis of the corpus callosum show sensory processing differences as measured by the sensory profile: Neuropsychology, 2015; 29(5); 751-58
49. Van der Knaap LJ, van der Ham IJ, How does the corpus callosum mediate interhemispheric transfer? A review: Behav BrainRes, 2011; 223(1); 211-21
50. De Lacoste MC, Kirkpatrick JB, Ross ED, Topography of the human corpus callosum: Neuropathol Exp Neural, 1985; 44; 578-91
51. Arndt S, Wesarg T, Stelzig YInfluence of single-sided deafness on the auditory capacity of the better ear. German version: HNO, 2019; 67; 739-49 [in German]
52. Humes LE, Dubno JR, Gordon-Salant S, Central presbycusis: Are view and evaluation of the evidence: J Am Acad Audiol, 2012; 23; 635-66
53. Keith RW, Diagnosing central auditory processing disorders in children: Audiology: Diagnosis , 2000; 337353, New York, Thieme Medical Publishers
54. Amiriani F, Tahaei AA, Kamali MComparative evaluation of auditory attention in 7 to 9 year old learning disabled student (Persian): Audiology, 2011; 20(1); 54-63 [in Farsi]
55. Roeder MB, Mahone EM, Larson JG, Left-right differences on timed motor examination in children: Child Neuropsychol, 2008; 14; 249-62
56. Greenwald RR, Jerger J, Aging affects hemispheric asymmetry on a competing speech task: J Am Acad Audiol, 2001; 12(4); 167-73
57. Kimura D, Functional asymmetry of the brain in dichotic listening: Cortex, 1967; 3; 163-78
58. Musiek FE, Baran JA, Central auditory evaluation of patients with neurological involvement: Handbook of clinical audiology, 2002; 532-44, Baltimore, Lippincott Williams and Wilkins
59. Berlin CI, Hughes LF, Lowe-Bell SS, Berlin HS, Dichotic right ear advantage in children 5 to 13: Cortex, 1973; 9(4); 394-402
60. Kinsboume M, The ontogeny of cerebral dominance: Ann NY Acad Sci, 1975; 263; 244-50
61. Kinsboume M, Hiscock M, Does cerebral dominance develop?: Language development and neurological theory, 1977; 171-91, New York, Academic Press
62. Obrzut JE, Hynd GW, Obrzut A, Pirozzolo FJ, Effect of directed attention on cerebral asymmetries in normal and learning-disabled children: Developmental Psychology, 1981; 17; 118-25
63. Moncrieff DW, Dichotic Listening in children: Age-related changes in direction and magnitude of ear advantage: Brain Cogn, 2011; 76; 316-22
64. Slorach N, Noehr B, Dichotic listening in stuttering and dyslalic children: Cortex, 1973; 9(3); 295-300
65. Noffsinger D, Martinez CD, Wilson RH, Dichotic listening to speech: Background and preliminary data for digits, sentences and nonsense syllables: J Am Acad Audiol, 1994; 5; 248-54
66. Musiek FE, Baran JA, Pinheiro ML, Neuroaudiology: Cases studies: San Diego: Singular, 1994
67. Sommers RK, Brady WA, Moore WH, Dichotic ear preferences of stuttering children and adults: Percep Mot Skill, 1975; 41; 931-38
68. Tzavaras A, Kaprinis G, Gatzoyas A, Literacy and hemispheric specialization for language: Dichotic listening in illiterates: Neuropsychologia, 1982; 19; 565-70
69. Wilson EH, Jaffe MS, Interactions of age, ear, and stimulus complexity on dichotic digit recognition: J Am Acad Audiol, 1996; 7(5); 358-64
70. Neijenhuis K, Snik A, Priester G, Age effects and normative data on a Dutch test battery for auditory processing disorders: Int J Audiol, 2002; 41(6); 334-46
Figures
Figure 1. Diagram of the free recall condition and possible answers. The digits can be repeated in any order.Figure 2. Diagram of directing attention only to the right ear (DARE) and possible answers.Figure 3. Diagram of directing attention to the left ear (DALE) and possible answers.Figure 4. One-pair DDT-IV results in girls and boys. Tables
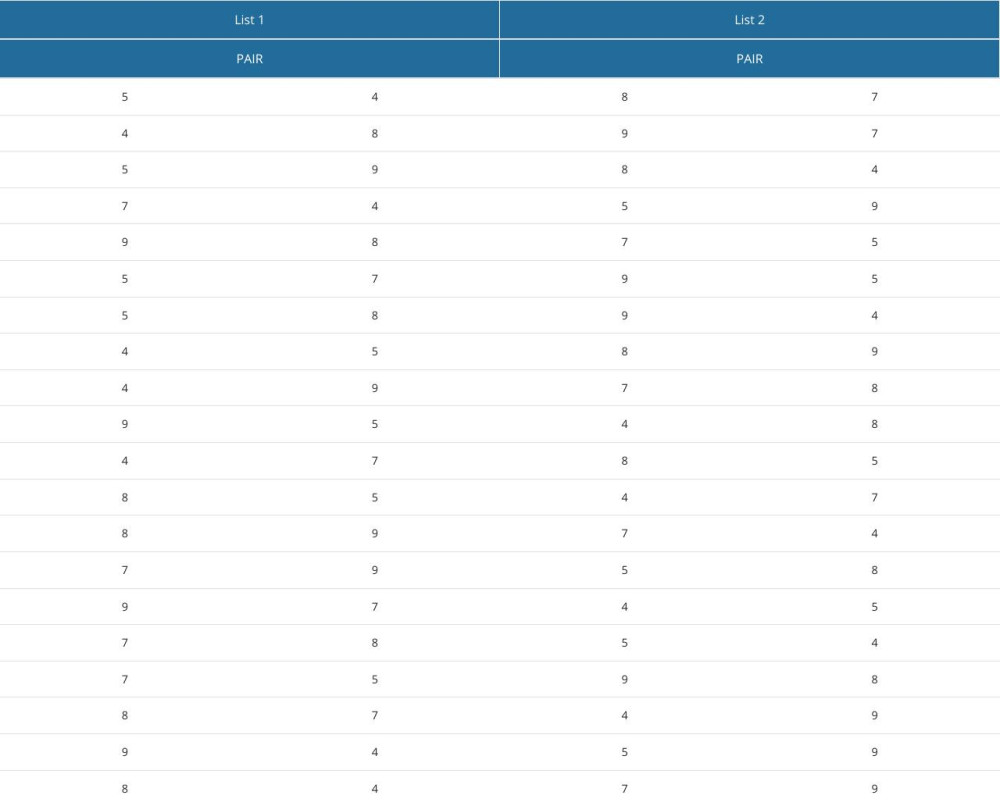 Table 1. Lists of the Italian version Dichotic Test of Digits and a schematic representation of the presentation of the digits.
Table 1. Lists of the Italian version Dichotic Test of Digits and a schematic representation of the presentation of the digits.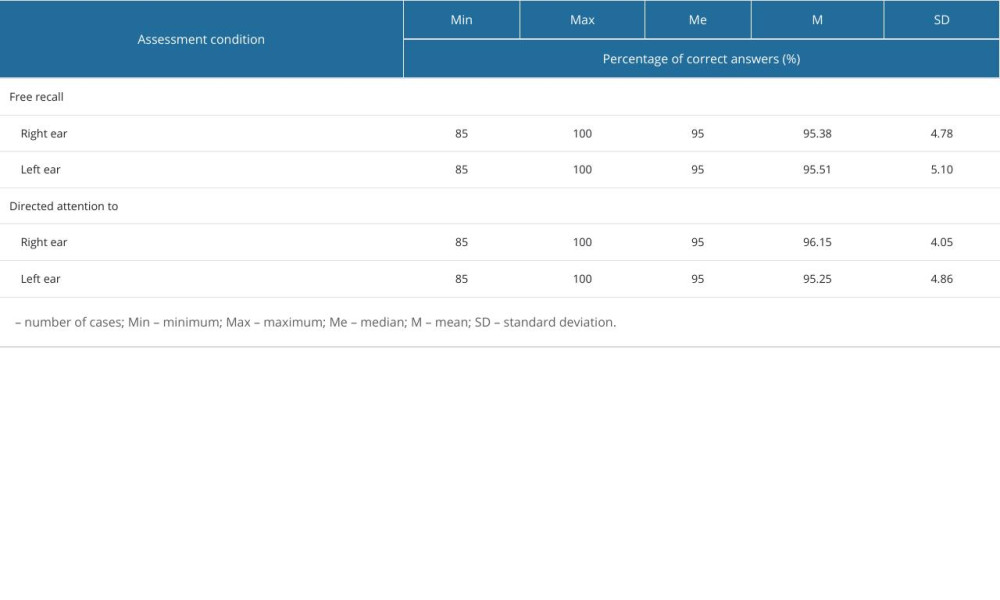 Table 2. Descriptive statistics for 1-pair DDT-IT results (n=39).
Table 2. Descriptive statistics for 1-pair DDT-IT results (n=39).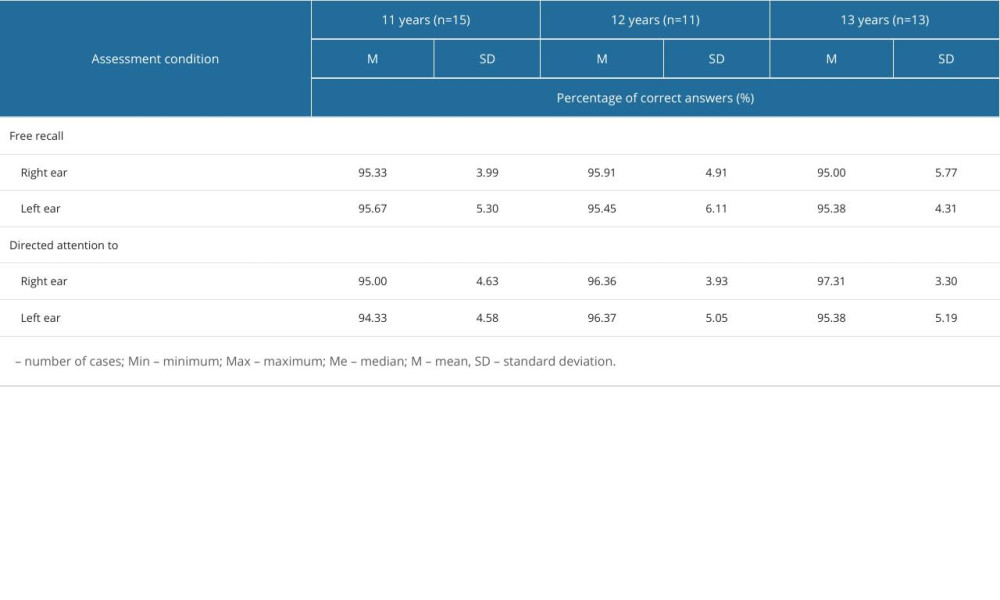 Table 3. Descriptive statistics for 1-pair DDT-IV results by age.Table 1. Lists of the Italian version Dichotic Test of Digits and a schematic representation of the presentation of the digits.Table 2. Descriptive statistics for 1-pair DDT-IT results (n=39).Table 3. Descriptive statistics for 1-pair DDT-IV results by age.
Table 3. Descriptive statistics for 1-pair DDT-IV results by age.Table 1. Lists of the Italian version Dichotic Test of Digits and a schematic representation of the presentation of the digits.Table 2. Descriptive statistics for 1-pair DDT-IT results (n=39).Table 3. Descriptive statistics for 1-pair DDT-IV results by age. In Press
Clinical Research
Outcomes After Minimally Invasive Intramedullary Nail Fixation and Locking Plate Fixation Among Patients Wi...Med Sci Monit In Press; DOI: 10.12659/MSM.952670
Laboratory Research
Influence of Scan Body Geometry, Implant Angulation, and Interimplant Distance on the Accuracy of Maxillary...Med Sci Monit In Press; DOI: 10.12659/MSM.953734
Clinical Research
Nasopharyngeal Carriage of Neisseria meningitidis in 181 Hajj and Umrah Pilgrims in Türkiye: Pre- and Post-...Med Sci Monit In Press; DOI: 10.12659/MSM.952640
Review article
The Roles of Gut Microbiota in the Pathogenesis of Acute PancreatitisMed Sci Monit In Press; DOI: 10.12659/MSM.952647
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,343
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,758,190
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,204
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,856
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387