07 November 2024: Clinical Research
High-Resolution Anorectal Manometry and Balloon Expulsion Test Outcomes in Functional Constipation: A Comparative Study
Huihui Shi1ABCDEFG, Li Li1BCG, Ling Huang1ABCDE, Wenwen Xia2DEF, Maoling Zhu1ABC, Yan Zhao2ADEFG*DOI: 10.12659/MSM.944599
Med Sci Monit 2024; 30:e944599






Abstract
BACKGROUND: Functional constipation can occur in children and adults and consists of difficult or infrequent bowel movements, painful defecation, or the sensation of incomplete bowel movement, and it can be idiopathic. This study aimed to compare the findings from high-resolution anorectal manometry (HRAM) and the balloon expulsion test (BET) in 360 patients with functional constipation and 73 healthy volunteers.
MATERIAL AND METHODS: In total, 360 patients with functional constipation and 73 healthy volunteers underwent HRAM and BET in our hospital from January 2017 to December 2023. We collected the general data of all participants and surveyed the defecation symptoms of patients with functional constipation.
RESULTS: Our study showed no significant correlation between HRAM results and age in healthy volunteers, while men had a higher residual anal pressure (P=0.022), higher anal squeeze pressure (P=0.020), and lower rectoanal pressure gradient than women (P=0.017). Using logistic regression analysis, it was concluded that sex (OR=2.880, 95% CI [1.654,5.015], P=0.000) and sensation of incomplete evacuation (OR=1.892, 95% CI [1.023,3.500], P=0.042) affected the occurrence of dyssynergic defecation. The specificity of BET in diagnosing dyssynergic defecation was 81.89%, while that of HRAM was 52.78%.
CONCLUSIONS: This observation provides normal values for anorectal pressures by HRAM. HRAM and BET are effective methods for assessing functional constipation. Being male and having sensation of incomplete evacuation are risk factors for dyssynergic defecation. The specificity of BET for diagnosing dyssynergic defecation was higher than that of HRAM.
Keywords: Constipation, Defecation, Manometry, Humans, Male, Female, adult, Anal Canal, Middle Aged, Rectum, Pressure, Case-Control Studies, Aged
Introduction
Chronic constipation is a common functional disease that affects a wide range of individuals in the general population [1,2]. The incidence of constipation was reported as 19.7% in the United States [3]. Functional constipation is more prevalent in women (8%) than in men (4%) in China [4]. Functional constipation can occur in children and adults and consists of difficult or infrequent bowel movements, painful defecation, or the sensation of incomplete bowel movement, and it can be idiopathic [5,6]. Functional constipation can be divided into defecatory disorders, slow-transit constipation, and normal-transit constipation, according to balloon expulsion, anorectal manometry, magnetic resonance defecography, and colon transit tests [6]. Patients with different types of functional constipation are treated differently [5]. High-resolution anorectal manometry (HRAM) is an important detection method for constipation with defecation disorders, as well as for Hirschsprung disease, and the balloon expulsion test (BET) has been used in recent years to evaluate constipation [7]. Biofeedback therapy is an effective treatment for constipation with defecation disorders [6]. Generally speaking, rectal pressure should be higher than anal pressure for normal defecation. However, some individuals without constipation can still exhibit a negative difference in rectal-anal pressure [8–10]. There is an overlap in the manometry results between healthy individuals and patients with defecatory disorders, and such results diminish the diagnostic value of anorectal manometry in defecatory disorders. Some studies have even suggested that anorectal manometry seems to have a limited role in assessing defecation disorders, that the results of multiple anorectal manometry examinations vary, and that the accuracy of all single anorectal manometry examinations in assessing defecation disorders requires confirmation [11,12]. A previous study included a total of 82 patients with constipation, and the HRAM results of the patients were analyzed. It was concluded that there were no statistically significant differences in lifestyle and clinical symptoms between patients with defecatory disorder constipation and those without, and that male patients were more prone to defecatory disorders than were women [13]. In contrast to that study, we included a larger number of patients with constipation to investigate the characteristics of HRAM and BET results in patients with constipation and compared these 2 test results with those of healthy volunteers. Therefore, in the present study, we aimed to compare the findings from HRAM and BET in 360 patients with functional constipation and 73 healthy volunteers.
Material and Methods
ETHICS STATEMENT:
All participants provided written informed consent. The protocol and informed consent documents were reviewed and approved by the Ethics Committee, Shanghai Yangpu Hospital, Tongji University (No. LL-2024-SCI-002).
PARTICIPANTS:
We conducted a retrospective analysis of patients with functional constipation who underwent HRAM and BET in our hospital from from January 2017 to December 2023, and who met the Rome IV diagnostic criteria. We also included healthy volunteers who underwent HRAM and BET during the same time. The exclusion criteria for patients were as follows: (1) constipation from irritable bowel syndrome; (2) taking cholinergic receptor antagonists, opioid receptor blockers, and other drugs (3) neurological and muscular diseases, such as Parkinson disease; (4) lower gastrointestinal diseases, severe heart, lung, brain, kidney, endocrine diseases, malignant tumors, pelvic floor diseases, and autonomic and peripheral neuropathy; and (5) previous colorectal and pelvic floor surgery. The inclusion criterion for healthy volunteers was age 20–80 years. The exclusion criteria for healthy volunteers were as follows: (1) lower gastrointestinal diseases, severe heart, lung, brain, kidney, endocrine diseases, malignant tumors, pelvic floor diseases, and autonomic and peripheral neuropathy; (2) alarm symptoms, such as blood in the stool, diarrhea, mucopurulent bloody stool; (3) previous colorectal and pelvic floor surgery; and (4) taking drugs that affect gastrointestinal motility in the past 3 months. Finally, our study included 360 patients with constipation and 73 healthy volunteers. General information was collected, including sex, age, height, weight, body mass index (BMI), and symptoms of constipation, including spontaneous frequency of defecation <3 times per week, straining and prolonged defecation, hard stool, anorectal obstruction during defecation, manual maneuvers to facilitate defecation, and sensation of incomplete evacuation. All participants in this study underwent HRAM and BET (Figure 1).
HIGH-RESOLUTION ANORECTAL MANOMETRY:
Anorectal functions were evaluated using the ManoScan 3D HR-ARM system with solid perfused catheter, the system includes the ManoScan A300 acquisition system, Manoview analysis software, and solid-state electrodes (diameter 10.75 mm, length 6.4 cm, 256 data acquisition points).
All participants, including patients with chronic constipation and healthy volunteers, emptied the stool before undergoing HRAM. All procedures were performed by a single experienced physician. The physician performed a digital rectal examination before the procedure, with the patient in the left lateral decubitus position. Through HRAM, we obtained the following data: anal resting pressure, anal high pressure zone length, anal squeeze pressure, anal pressure, rectal pressure, anal relaxation percentage, and rectal sensation. The procedure was performed as follows:
BALLOON EXPULSION TEST:
A rubber balloon with a diameter of 3.5 cm was placed in the participant’s rectum. The balloon was filled with 50 mL of warm water, and the participant was asked to take the left decubitus position to expel it. Inability to expel within 1 min indicated a positive result.
STATISTICAL ANALYSIS:
SPSS software (IBM Corp, Armonk, NY, USA) was used for statistical analysis. The normally distributed continuous data are represented by mean and standard deviation. The skewed data are represented by the median (lower quartile, upper quartile). The Pearson correlation test was used for the normally distributed correlations; the Spearman correlation test was used for a non-normal distribution; the Mann-Whitney U test was used for 2 independent samples with a non-normal distribution; and the chi-square test was used for the comparison of the positive rates of the 2 control groups. We used logistic regression to analyze the risk factors for dyssynergic defecation. All tests were applied bilaterally, and the results were considered significant when
Results
HRAM RESULTS IN HEALTHY VOLUNTEERS: SEX-RELATED DIFFERENCES AND CORRELATION ANALYSIS OF HRAM RESULTS WITH AGE AND BMI:
The control group of healthy volunteers comprised 18 men and 55 women with a mean age of 50±14 years and mean BMI of 24.37±2.76 kg/m2. The high-resolution HRAM results in the control group showed statistically significant differences in anal residual pressure, maximum anal squeeze pressure, and rectoanal pressure gradient between by sex (Table 1). There was no significant correlation between the HRAM results and age among the healthy volunteers, and BMI was positively correlated with relaxation rate and maximum discomfort in the rectal sensation test (Table 2).
CORRELATION BETWEEN HRAM RESULTS AND BET RESULTS IN HEALTHY VOLUNTEERS:
Twelve participants in the control group had a positive BET result, accounting for 16.44% of the total control population. Those who tested positive on BET had higher anal residual pressure and a lower rectoanal pressure gradient than those who tested negative. Additionally, participants with positive results had significantly higher initial sensation on the rectal sensation test than those with negative results (Table 3). There was no significant difference in the rate of BET positivity between men and women in the control group (χ2=1.497, P=0.221), and there was no statistically significant difference in age between the positive and negative groups (z=−0.173, P=0.863)
COMPARISON OF HRAM AND BET RESULTS BETWEEN HEALTHY VOLUNTEERS AND PATIENTS WITH FUNCTIONAL CONSTIPATION:
Comparison of the HRAM results between patients with constipation and healthy volunteers showed statistically significant differences in resting pressure (
CORRELATION BETWEEN CLINICAL SYMPTOMS AND HRAM RESULTS IN PATIENTS WITH FUNCTIONAL CONSTIPATION:
There was a statistically significant difference in age between patients with functional constipation characterized by hard stools (65.1±13.89 years) and those without this symptom (61.66±14.64 years; t=2.288, P=0.023). Patients with chronic constipation characterized by straining and prolonged defecation were older (64.06±14.02 years) than those without this symptom (57.36±15.60 years; t=2.77, P=0.006). The clinical symptoms of all patients with functional constipation were analyzed, and the results are shown in Table 4. Among patients with constipation, there were statistically significant differences in the rate of relaxation and rectal pressure gradient between patients with and without straining and prolonged defecation, and the relaxation rate and rectoanal pressure gradient were lower in patients with straining than in those without straining and prolonged defecation. Patients who had fewer than 3 bowel movements per week had lower sensation in their rectal mucosa than did patients without this symptom. In addition, the results of maximum discomfort in the rectal mucosa sensation test were significantly different between patients with and without hard stools, a feeling of rectoanal obstruction, and the need for manual assistance during bowel movements.
COMPARISON OF HRAM RESULTS AND CONSTIPATION SYMPTOMS BETWEEN PATIENTS WITH FUNCTIONAL CONSTIPATION SHOWING POSITIVE AND NEGATIVE BET RESULTS:
Among patients with functional constipation, 147 had a positive BET result, accounting for 40.72% of all patients with functional constipation. There was no significant difference in the BET positivity rate between patients with different clinical symptoms (P>0.05). Compared with the negative group, the positive group had higher anal residual pressure, lower anal relaxation rate, lower rectal pressure, lower rectoanal pressure gradient, higher urge to defecate, and higher maximum discomfort in the rectal sensation test, all with statistically significant differences (Table 5). The BET positivity rate in men with functional constipation (48.0%) was higher than that in women (35.7%) (χ2=6.970, P=0.008). Patients in the positive group were significantly older than those in the negative group (z=−2.753, P=0.006).
COMPARING THE CLINICAL DATA BETWEEN PATIENTS WITH DYSSYNERGIC DEFECATION AND PATIENTS WITH OTHER FUNCTIONAL CONSTIPATION:
According to the results of HRAM, patients with dyssynergic defecation were divided into 4 groups [5,14,15]. There were no statistically significant differences in the BET positivity rate among the 4 groups of patients with abnormal HRAM results (χ2=4.253, P=0.235). There were 223 patients with positive HRAM results, accounting for 61.78% of the constipation population in our study; among the 223 patients, 99 patients had positive BET, with a BET positivity rate of 40.72% among all patients with constipation. These 99 patients who were positive for HRAM and BET received a diagnosis of dyssynergic defecation [7]. There were differences in sex and age between the dyssynergic defecation group and the non-dyssynergic defecation group of patients (Table 6). Clinical symptoms and history of smoking and alcohol drinking did not show a statistically significant difference between groups. We conducted logistic regression analysis on the potential influencing factors of dyssynergic defecation, including sex, age, smoking, alcohol drinking, and clinical symptoms, such as spontaneous frequency of defecation less than 3 times per week, straining and prolonged defecation, hard stool, anorectal obstruction during defecation, manual maneuvers to facilitate defecations, and sensation of incomplete evacuation. We concluded that sex (OR=2.880, 95% CI [1.654,5.015], P=0.000) and sensation of incomplete evacuation (OR=1.892, 95% CI [1.023,3.500], P=0.042) affected the occurrence of dyssynergic defecation. The specificity of BET in diagnosing dyssynergic defecation was 81.89%, while that of HRAM was 52.78%.
Discussion
In our study, the comparison of HRAM and BET results of patients with chronic constipation with those of healthy volunteers showed statistically significant differences; therefore, we concluded that HRAM and BET are effective methods to evaluate constipation [7,16].
Unlike previous studies, our study showed no significant correlation between HRAM results and age in healthy individuals, as anal resting pressure did not change with age [1,17–20]. Among healthy volunteers, men had a higher residual anal pressure, higher anal squeeze pressure, and lower rectoanal pressure gradient than did women. Residual anal pressure reflects the ability of the anal sphincter to relax during defecation, and generally speaking, rectal pressure should be higher than anal pressure for normal defecation. However, in many studies, the pressure difference between the rectum and anus in healthy individuals is consistently shown as a negative value [17,20,21], and our study yielded the same result, with a rectoanal gradient pressure for men of −42.69±24.75 mm Hg, and for women of −4.21±28.75 mm Hg. A positive rectoanal pressure gradient does not necessarily mean that defecation can occur normally, and perhaps the utility of HRAM for diagnosing dyssynergic defecation is limited [8]. HRAM is performed in the left lateral position, and some research confirmed that HRAM should be performed in the more physiological seated position [22]. The anal squeeze pressure was found to be higher in men than in women, which perhaps indicated that men have stronger function of the external anal sphincter than do women. Low anal squeeze pressure is most commonly due to obstetric injury [23]. In the present study, BMI was positively correlated with the maximum discomfort in the rectal sensation test, which is consistent with previous research results [1], suggesting that the rectal mucosal sensation function may be poorer in patients with a higher BMI. Rectal sensation in our study showed neither sex differences nor age differences. Also, BMI was positively correlated with the rate of anal relaxation during evacuation; a result that is inconsistent with a previous study [19]. Previous studies have shown a positive predictive value of 64% and a negative predictive value of 97% for the diagnosis of pelvic floor dysfunction by BET [16,23,24]. In the present study, 12 participants in the control group had a positive BET result, accounting for 16.44% of the total healthy control population, a higher positivity rate than that of previous studies [1]. The HRAM results of healthy volunteers showed that residual anal pressure and first sensation were higher in participants with a positive rather than a negative BET, whereas the rectal pressure gradient was lower in participants with a positive rather than a negative BET. As found in another study, a lower rectoanal gradient is associated with prolonged rectal BET [25]. Perhaps the healthy participants with positive BET results had asymptomatic pelvic floor dysfunction or were unable to replicate defecation in the test environment.
In the present study, patients with hard stools and difficult defecation were older than those without these symptoms; therefore, perhaps older patients are more likely to develop these 2 symptoms. Between patients with and without fewer than 3 bowel movements per week, there were statistically significant differences in the first sensation, urge to defecate, and maximum discomfort during the rectal sensation test, suggesting that a decrease in the number of bowel movements may be related to decreased rectal sensation. There was a statistically significant difference in rectal pressure gradient in patients with constipation who had straining, and in prolonged defecation, compared with those without this symptom; specifically, the rectoanal pressure gradient was lower in patients with straining and prolonged defecation, and these 2 symptoms can indicate pelvic floor dysfunction. Some studies have shown that hard and dry stool suggests non-defecation disorder constipation [26], and this was consistent with our study. The BET positivity rate in patients with functional constipation showed no significant difference by each clinical symptom. In the study by Zhao et al, there was no significant difference in clinical symptoms between patients with dyssynergic defecation and other constipation groups [13].
In the present study, residual pressure, urge to defecate, and maximum discomfort in the rectal sensation test were significantly higher in patients with a positive than with a negative BET result, and the gradient of rectal pressure and rectal pressure were significantly lower in patients with a positive than with a negative BET result; these results suggest that patients with low rectal pressure gradients are more likely to have a positive BET result [27]. The BET positivity rate was higher in men than in women with constipation, also indicating that men may be more prone to dyssynergic defecation. Patients with a positive BET had a higher urge to defecate and maximum discomfort volume in the rectal sensation test, which is similar to a previous study [28]; rectal sensory thresholds were greater in patients with an abnormal BET. There was no statistically significant difference in the BET positivity rate among the 4 groups of patients with defecation coordination disorders.
The positivity rate of BET in our study was 40.7%, and the simultaneous positivity rate of HRAM and BET was 27.42%, while in a previous study, it was 73% [13], and there is a difference in the positive rates of these 2 tests between the 2 studies (χ2=60.78,
After determining the presence of dyssynergic defecation in patients through the BET and HRAM, we can then use biofeedback therapy for the treatment of constipation in these patients [29,30]. This therapy is the mainstay for treatment of dyssynergic defecation. The goals are to correct the dyssynergia or incoordination of abdominal and pelvic floor muscles during evacuation and to improve perception of rectal filling in patients with impaired rectal sensation [14]. The treatment efficacy of biofeedback is 70% to 80% in randomized controlled trials [31]. Therefore, the use of HRAM and BET for diagnosing dyssynergic defecation is very important.
Our study had certain limitations. The sample size of healthy volunteers was relatively small. The patients included were mainly outpatients, and we did not incorporate barium defecography or magnetic resonance defecography, nor did we include colonic transit tests in our research. Therefore, we were unable to accurately classify the patients with constipation, which also prevented us from further analyzing the diagnostic value of HRAM and BET.
Conclusions
This observation provides normal values for anorectal pressures by HRAM. HRAM and BET are effective methods for assessing functional constipation. Being male and have sensation of incomplete evacuation are risk factor for dyssynergic defecation. The specificity of BET for diagnosing dyssynergic defecation was higher than that of HRAM.

Tables
Table 1. Anorectal manometry results and sex-related differences in healthy volunteers. Table 2. Correlations between age, body mass index, and manometry results of healthy volunteers.
Table 2. Correlations between age, body mass index, and manometry results of healthy volunteers. Table 3. Differences of high-resolution anorectal manometry results in healthy volunteers with different balloon expulsion test results.
Table 3. Differences of high-resolution anorectal manometry results in healthy volunteers with different balloon expulsion test results. Table 4. Differences in high-resolution anorectal manometry results in patients with constipation characterized by different clinical symptoms.
Table 4. Differences in high-resolution anorectal manometry results in patients with constipation characterized by different clinical symptoms. Table 5. Comparison of high-resolution anorectal manometry results between patients with constipation showing positive and negative balloon expulsion test results.
Table 5. Comparison of high-resolution anorectal manometry results between patients with constipation showing positive and negative balloon expulsion test results.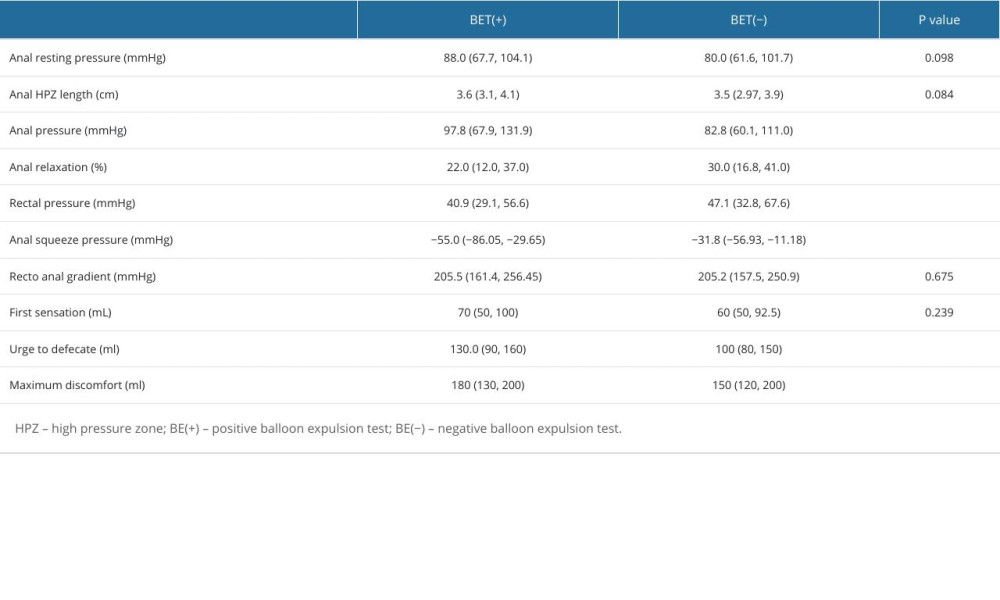 Table 6. Sociodemographic data and clinical symptoms in patients with and without dyssynergic defecation.
Table 6. Sociodemographic data and clinical symptoms in patients with and without dyssynergic defecation.
References
1. Oblizajek NR, Gandhi S, Sharma M, Anorectal pressures measured with high-resolution manometry in healthy people-Normal values and asymptomatic pelvic floor dysfunction: Neurogastroenterol Motil, 2019; 31(7); e13597
2. Dik VK, Siersema PD, Joseph A, Constipation-related direct medical costs in 16 887 patients newly diagnosed with chronic constipation: Eur J Gastroenterol Hepatol, 2014; 26(11); 1260-66
3. Almario CV, Ballal ML, Chey WD, Burden of gastrointestinal symptoms in the United States: Results of a nationally representative survey of over 71,000 Americans: Am J Gastroenterol, 2018; 113(11); 1701-10
4. Zhao YF, Ma XQ, Wang R, Epidemiology of functional constipation and comparison with constipation-predominant irritable bowel syndrome: The Systematic Investigation of Gastrointestinal Diseases in China (SILC): Aliment Pharmacol Ther, 2011; 34(8); 1020-29
5. Vriesman MH, Koppen IJN, Camilleri M, Management of functional constipation in children and adults: Nat Rev Gastroenterol Hepatol, 2020; 17(1); 21-39
6. Bharucha AE, Lacy BE, Mechanisms, evaluation, and management of chronic constipation: Gastroenterology, 2020; 158(5); 1232-49e1233
7. Bharucha AE, Coss-Adame E, Diagnostic strategy and tools for identifying defecatory disorders: Gastroenterol Clin North Am, 2022; 51(1); 39-53
8. Grossi U, Carrington EV, Bharucha AE, Diagnostic accuracy study of anorectal manometry for diagnosis of dyssynergic defecation: Gut, 2016; 65(3); 447-55
9. Ratuapli SK, Bharucha AE, Noelting J, Phenotypic identification and classification of functional defecatory disorders using high-resolution anorectal manometry: Gastroenterology, 2013; 144(2); 314-22e2
10. Prichard DO, Lee T, Parthasarathy G, High-resolution anorectal manometry for identifying defecatory disorders and rectal structural abnormalities in women: Clin Gastroenterol Hepatol, 2017; 15(3); 412-20
11. Ortengren AR, Ramkissoon RA, Chey WD, Anorectal manometry to diagnose dyssynergic defecation: Systematic review and meta-analysis of diagnostic test accuracy: Neurogastroenterol Motil, 2021; 33(11); e14137
12. Mishra R, Gautam M, Oblizajek NR, Bharucha AE, Reproducibility of high-resolution manometry among healthy and constipated persons: Neurogastroenterol Motil, 2022; 34(12); e14438
13. Zhao Y, Ren X, Qiao W, High-resolution anorectal manometry in the diagnosis of functional defecation disorder in patients with functional constipation: A retrospective cohort study: J Neurogastroenterol Motil, 2019; 25(2); 250-57
14. Rao SS, Patcharatrakul T, Diagnosis and treatment of dyssynergic defecation: J Neurogastroenterol Motil, 2016; 22(3); 423-35
15. Patcharatrakul T, Rao SS, Update on the pathophysiology and management of anorectal disorders: Gut Liver, 2018; 12(4); 375-84
16. Jiang Y, Wang Y, Tang Y, Lin L, Clinical value of positive BET and pelvic floor dyssynergia in Chinese patients with functional defecation disorder: Scand J Gastroenterol, 2022; 57(7); 775-82
17. Li Y, Yang X, Xu C, Normal values and pressure morphology for three-dimensional high-resolution anorectal manometry of asymptomatic adults: A study in 110 subjects: Int J Colorectal Dis, 2013; 28(8); 1161-68
18. Mazor Y, Prott G, Jones M, Anorectal physiology in health: A randomized trial to determine the optimum catheter for the balloon expulsion test: Neurogastroenterol Motil, 2019; 31(4); e13552
19. Deshmukh R, Shukla A, Chandnani S, Normal values of high-resolution anorectal manometry of healthy Indians: J Neurogastroenterol Motil, 2022; 28(3); 401-8
20. Sharma M, Lowry AC, Rao SS, A multicenter study of anorectal pressures and rectal sensation measured with portable manometry in healthy women and men: Neurogastroenterol Motil, 2021; 33(6); e14067
21. Dimitriu A, Saizu R, Oancea D, Gheorghe C, Normal values of high resolution anorectal manometry in 132 Romanian healthy people: J Gastrointestin Liver Dis, 2023; 32(4); 473-78
22. Sharma M, Muthyala A, Feuerhak K, Improving the utility of high-resolution manometry for the diagnosis of defecatory disorders in women with chronic constipation: Neurogastroenterol Motil, 2020; 32(10); e13910
23. Bharucha AE, Basilisco G, Malcolm A, Review of the indications, methods, and clinical utility of anorectal manometry and the rectal balloon expulsion test: Neurogastroenterol Motil, 2022; 34(9); e14335
24. Minguez M, Herreros B, Sanchiz V, Predictive value of the balloon expulsion test for excluding the diagnosis of pelvic floor dyssynergia in constipation: Gastroenterology, 2004; 126(1); 57-62
25. Blackett JW, Gautam M, Mishra R, Comparison of anorectal manometry, rectal balloon expulsion test, and defecography for diagnosing defecatory disorders: Gastroenterology, 2022; 163(6); 1582-92e1582
26. Ingemansson A, Walter SA, Jones MP, Sjödahl J, Defecation symptoms in relation to stool consistency significantly reflect the dyssynergic pattern in high-resolution anorectal manometry in constipated patients: J Clin Gastroenterol, 2024; 58(1); 57-63
27. Heinrich H, Fox M, One and done: Is measurement of the rectoanal pressure gradient enough to diagnose defecatory disorders and guide the management of constipation?: Gastroenterology, 2022; 163(6); 1488-91
28. Ramu SK, Oblizajek NR, Savica R, Defecatory disorders are a common cause of chronic constipation in Parkinson disease: Neurogastroenterol Motil, 2024; 36(5); e14767
29. Moore D, Young CJ, A systematic review and meta-analysis of biofeedback therapy for dyssynergic defaecation in adults: Tech Coloproctol, 2020; 24(9); 909-18
30. Ba-Bai-Ke-Re MM, Wen NR, Hu YL, Biofeedback-guided pelvic floor exercise therapy for obstructive defecation: An effective alternative: World J Gastroenterol, 2014; 20(27); 9162-69
31. Chiarioni G, Whitehead WE, Pezza V, Biofeedback is superior to laxatives for normal transit constipation due to pelvic floor dyssynergia: Gastroenterology, 2006; 130(3); 657-64
Tables
Table 1. Anorectal manometry results and sex-related differences in healthy volunteers.Table 2. Correlations between age, body mass index, and manometry results of healthy volunteers.Table 3. Differences of high-resolution anorectal manometry results in healthy volunteers with different balloon expulsion test results.Table 4. Differences in high-resolution anorectal manometry results in patients with constipation characterized by different clinical symptoms.Table 5. Comparison of high-resolution anorectal manometry results between patients with constipation showing positive and negative balloon expulsion test results.Table 6. Sociodemographic data and clinical symptoms in patients with and without dyssynergic defecation.Table 1. Anorectal manometry results and sex-related differences in healthy volunteers.Table 2. Correlations between age, body mass index, and manometry results of healthy volunteers.Table 3. Differences of high-resolution anorectal manometry results in healthy volunteers with different balloon expulsion test results.Table 4. Differences in high-resolution anorectal manometry results in patients with constipation characterized by different clinical symptoms.Table 5. Comparison of high-resolution anorectal manometry results between patients with constipation showing positive and negative balloon expulsion test results.Table 6. Sociodemographic data and clinical symptoms in patients with and without dyssynergic defecation. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387