16 July 2024: Review Articles
Innovative Approaches to Enhance and Measure Medication Adherence in Chronic Disease Management: A Review
Michał GackowskiDOI: 10.12659/MSM.944605
Med Sci Monit 2024; 30:e944605






Abstract
ABSTRACT: Medication non-adherence is a problem that affects up to 50% of patients with chronic diseases. The result is a failure to achieve therapeutic goals and an increased burden on the healthcare system. It is, therefore, highly appropriate to develop models to assess patient adherence to prescribed therapy. To date, there are many methods for doing this. However, several tools have been developed that subjectively or objectively, directly or indirectly, assess the level of patient adherence. Electronic medication packaging devices are among the most rapidly evolving methods of measuring adherence. Other emerging technologies include the use of artificial intelligence algorithms and ingestible biosensors. The former is being used to create applications for mobile phones and laptops. The latter appears to be the least susceptible to the risk of overestimating adherence but remains very expensive. Here, we present recent developments in measuring patient adherence, and provide details of achievements in objective methods for assessing adherence, such as electronic monitoring devices, video-observed therapy, and ingestible biosensors. A dedicated section on using artificial intelligence and machine learning in adherence measurement and reviewing questionnaires and scales used in specific diseases is also included. Methods are discussed along with their advantages and potential limitations. This article aimed to review current measures and future initiatives to improve patient medication adherence.
Keywords: medication adherence, Patient Compliance, Treatment Adherence and Compliance, Guideline Adherence, Humans, Chronic Disease, Artificial Intelligence, Disease Management, Algorithms, Surveys and Questionnaires
Introduction
Medication adherence – the extent to which patients follow prescribed treatment plans – has long been recognized as a cornerstone of adequate healthcare. It is an essential determinant of treatment success and is pivotal in achieving therapeutic goals, managing chronic conditions, and improving overall patient outcomes [1].
While often used interchangeably, “compliance” and “adherence” hold subtle yet meaningful distinctions, profoundly shaping the relationship between patients and healthcare professionals. “Compliance” suggests a one-sided dynamic where patients passively follow instructions, whereas “adherence” emphasizes a collaborative partnership, with patients actively participating in treatment decisions. This shift acknowledges patient autonomy and understanding, fostering a more supportive and inclusive healthcare approach [2].
Non-adherence to medication regimens remains an important issue among individuals with chronic diseases. It affects a significant proportion of patients, with rates ranging from 40% to 50%, depending on the specific chronic condition [3]. The magnitude of this issue carries significant potential ramifications. Medication adherence is a key factor associated with the effectiveness of all pharmacological therapies but is particularly critical for medications prescribed for chronic conditions. Of all medication-related hospitalizations in the United States, between one-third and two-thirds are due to poor adherence [4]. Non-adherence affects individual patients’ well-being and their chances of achieving the best possible treatment results. It also places a substantial burden on society and the healthcare system. It is estimated that this problem is responsible for approximately 125 000 preventable deaths each year, incurring an annual cost of roughly $100–$300 billion USD [5–7]. The consequences of non-adherence are significant, including hospitalization and increased mortality. Even with the use of a placebo, high adherence had a 3.5 times greater effect on reducing mortality than total active treatment with candesartan in chronic heart failure [8]. As a general guideline, patients are typically deemed adherent when correctly taking at least 80% of their prescribed medications [3]. Nevertheless, given the substantial magnitude of this issue, it is natural to question why patients may not adhere to medical recommendations. Non-adherence can have intentional or unintentional causes [9]. Factors significantly influencing patients’ adherence primarily encompass social, cultural, economic, and healthcare system contexts. However, it is equally crucial to consider the patient’s beliefs regarding the prescribed medication, as this plays a fundamental role in shared decision-making and promoting adherence [10]. Some of the more critical reasons are shown in Figure 1 [11–13].
Many researchers have recognized the problem of non-adherence. However, no sufficiently objective, effective, easy-to-implement, and widely available method has yet been developed. As far as we know, no prominent entity, organization, or collective has made medication adherence a focal point. This subject must neatly align with the scope of any single field of study. Insurance providers and health plans have competing priorities, with only a limited effort directed toward systematically addressing this issue [3,14]. Furthermore, as highlighted by the American Heart Association, it can be challenging to assess the overall prevalence of medication non-adherence. However, this problem is not limited to cardiac disease and generally affects patients [15–17]. Given the above, tools are urgently needed to help healthcare professionals measure their patients’ adherence to medication regimens, analyze the consequences, and design medical interventions. The need for a comprehensive tool arises because, as indicated by Zaugg et al, providing simple feedback to the doctor stating that the patient is non-adherent does not enhance adherence [18]. Given this perspective, the solution should emphasize a systemic approach rather than relying on repeated encouragement [3]. Improving the effectiveness of adherence interventions can have a far more significant impact on population health than any improvement in specific medical treatment [19].
As the issue of non-adherence is gaining prominence in public discourse, appearing in articles targeting both healthcare professionals and patients [7,20,21], this article aims to review current measures and future initiatives to improve patient medication adherence.
Overview of Medication Adherence Measurements Models
The methods used to assess medication adherence are limited. We need more comprehensive solutions because current methods may not account for occasional use or accurately track whether patients are actually taking their medication. In addition, the effectiveness of the methods may be reduced due to patient bias resulting from errors, misunderstandings, or deliberate non-compliance [22]. The limitations of the methods result in a need for a criterion standard for determining patient adherence [1,23].
The World Health Organization (WHO) divides the methods of medication adherence measurements into subjective and objective [1]. As no single method is perfect, a multidirectional approach and, thus, the role of both objective and subjective methods in patient assessment may bring the best results [24]. Techniques can also be classified as direct and indirect [1]. A breakdown of the methods with examples is illustrated in Figure 2.
The overarching goal of developing and testing models to measure medication adherence is to ensure effective monitoring and evaluation of patient adherence. By developing accurate and reliable models, researchers and healthcare professionals aim to achieve the following goals: assess the effectiveness of treatments, identify risk factors, adjust therapeutic plans, improve the doctor–patient relationship, and optimize healthcare management. The most effective approach so far has been multi-level targeting with multiple interventions [25]. Table 1 at the end of this section summarizes all identified methods for measuring medication adherence.
Healthcare Assessment
Clinicians often use interviewing patients as a cost-effective and easy-to-use method of measuring patient adherence. Patients can estimate their medication-taking behavior, such as the percentage of missed doses or the frequency of deviations from the prescribed regimen [5]. Questions can also be based on the patient’s knowledge of their prescribed regimen, including drug names, schedules, and indications. Healthcare professionals evaluate the answers to determine adherence. However, there needs to be more evidence of the relationship between patients’ knowledge of their medication regimen and actual adherence. In addition to the traditional approach, motivational interviewing has gained popularity in clinical practice. This method integrates adherence measurement and intervention to address cases of non-adherence [1]. The advantage of this method is that during such a consultation, the healthcare professional can use motivational interviewing to increase patient adherence. Such a consultation’s effectiveness, feasibility, and acceptability helped improve endocrine therapy in diverse patient populations [26].
Self-Reporting
Self-reporting is a subjective method of measuring adherence and is the most effective approach to assessing adherence in clinical and research settings. However, it is also the method with the highest risk of overestimating adherence compared to electronic measures and is prone to error as the time between visits increases [5,27]. This is because patients may be inclined to give socially desirable answers. Self-reported data is a major tool for assessing adherence in resource-poor countries [28]. The advantages of self-reporting are its cost-effectiveness, ease of implementation, patient involvement, qualitative insights, and widespread acceptance. However, to minimize bias and maximize comparability between studies, improved methods of collecting self-reported data are needed [29].
Drug Level Measures
Drug level monitoring usually involves the determination of drug levels in blood or urine samples. This direct method provides evidence of whether the patient has taken the drug. Even though this method is accurate, it also has many limitations. Firstly, blood sampling is an invasive method, which could be an obstacle for the young population. Another limitation is the time between taking the drug and taking the blood sample and between taking and freezing the sample. In this regard, it is essential to mention the high costs of the method, as it requires trained personnel and specialized equipment. Thirdly, this method provides only qualitative information on whether drugs have been taken [28]. As highlighted by Eskas et al, other drawbacks of this method are the limited information on the timing of administration and “white coat adherence.” The former is crucial, as taking medication at the right time is necessary for a positive treatment outcome. The latter refers to the situation where adherence improves just before and after a doctor’s appointment [30]. In addition, it may not be practical to monitor drug levels at every consultation. Another limitation of this method is drug interactions and individual patient variability in the rate of drug metabolism [31]. Drug-drug and drug-food interactions can affect the accuracy of the assay. The most commonly cited advantages of direct methods are objectivity of assessment, ability to identify non-adherent patients, pharmacogenetic insights, optimization of treatment, and monitoring of efficacy [30].
Pill Count
The premise of the pill count method is to give patients a certain number of pills in a prepared container (eg, bottle or box). Patients are then asked to bring this container to their next visit, where the healthcare provider calculates how many pills the patient should have left in the container. The patient’s adherence to the prescribed therapy is calculated based on the number of pills remaining and the theoretical number of pills that should be taken in a given time (according to the dosage regimen) [32]. The main strengths of this method are that it is inexpensive and easy to adapt. Weaknesses include the need to compare with drug ownership and the fact that patients must remember to bring pill bottles to the clinic [33].
Pill counting is one of the most commonly used indirect methods. However, as with all indirect methods, it is less accurate and more prone to error. In addition, pill count may be susceptible to misreporting and may be an overestimate of a patient’s adherence. Electronic monitoring devices are considered more accurate [34].
Electronic Medication Packaging (EMP) Devices
Electronic monitoring has been recognized as the most reliable assessment method for measuring medication adherence, but it is also the most expensive method [35]. Generally, a patient is provided with a device that records every dosing event. The data are then stored and can be analyzed in detail by healthcare providers. Unlike pill counting, this method records the fact that a dose has been taken and the time at which the patient took the medicine. This makes the process more resistant to the risk of being deceived in the form of a single emptying of the medicine. However, it does not ensure that the patient has taken the dose (even though the dose has been removed from the device, it is not sure that the patient has taken the medicine) [36]. The weaknesses of this type of device can be presented as the following assumptions: patients are willing to take their medication as prescribed; once pills are removed from the device, they are taken as prescribed; when the bottle is opened, the correct dose of medication is removed. The last assumption relates to devices in the form of bottles or boxes holding more than 1 medication dose [37]. Improved adherence is often linked with devices integrated into the care delivery system specifically designed to record dosing events [38]. However, more studies are needed to explore the impact of such devices on patients, and studies are also urgently required to investigate the implications for health services [39]. To increase the acceptability of the methods used and to avoid many usability problems, it is essential to understand the needs of patients [35]. Examples of EMPs and new developments in this area are presented in the following sections of this paper.
Directly Observed Therapy (DOT)
DOT is a method of medication administration in which a healthcare professional watches a person take each dose of medication. It ensures that the person receives and takes all medicines as prescribed and monitors the treatment response. DOT is often used to treat tuberculosis (TB) [40]. In the case of HIV treatment, DOT is sometimes called directly administered antiretroviral therapy (DAART) [41].
The WHO has introduced this strategy to ensure treatment adherence. Nevertheless, the approach is associated with considerable inconvenience for patients and healthcare workers. Moreover, patients may hide their medicines under their tongue and discard them afterward. In addition, a literature review did not find rigorous evidence to support the effectiveness of DOT in improving adherence and treatment outcomes [42].
The video observed therapy (VOT) method is a modified version of the DOT method. The VOT method is described in later sections of this paper.
Secondary Database Measurements
These methods involve assessing and quantifying how well patients adhere to their prescribed medication regimens using data from secondary sources. These secondary databases typically contain information from primary data sources such as electronic prescription services, pharmacy claims, or other health records. The aim is to use this secondary data to gain insights into patients’ medication use and adherence patterns. These measures help researchers and healthcare professionals assess adherence at a population level, identify trends, and understand the factors influencing adherence behavior. The basic premise of this method is that once a medicine has been purchased, the patient takes it as prescribed [1].
Mobile Applications and Artificial Intelligence
In recent years, the proliferation of mobile technologies has increased the number of ways to measure patient adherence. Mobile applications (apps), electronic medication diaries, video-based platforms, and artificial intelligence platforms are newer technology-based tools that can provide more objective adherence data [43]. This section provides an overview of some selected apps.
Video Observed Therapy (VOT)
VOT is a method of measuring medication adherence that is widely used to assess and improve patient adherence to TB treatment [44]. VOT technology uses live (synchronous; S-VOT) or recorded (asynchronous; A-VOT) video technology to remotely observe patients swallowing their medication via smartphones, tablets, or computers [45]. S-VOT involves the patient swallowing their medication in front of a computer or smartphone camera while a healthcare professional watches remotely using video conferencing software and then documents the interaction in the patient’s medical record. A-VOT allows patients to videotape their medication intake so that providers can view it simultaneously. The second approach eliminates the need for simultaneous ingestion and observation [45]. These technologies have shown promise in improving patient adherence. In particular, they can be handy for patients in the productive age group, with increased mobility, high smartphone usage, and extensive internet coverage [42]. However, VOT should be seen as a tool to facilitate patient–provider contact, not to replace physical interaction between the patient and the healthcare professional. Establishing VOT also requires investments, including training for patients and VOT observers [46]. The benefits of VOT are usually compared to those of DOT. Studies show that VOT is more convenient for patients and providers, time- and cost-effective, widely accepted by patients and health workers, and flexible. As a result, the WHO has recommended VOT for TB treatment since 2017 [47]. However, some limitations remain. Although S-VOT retains the real-time communication of DOT, which could improve adherence detection and patient engagement, it requires staff to schedule observations, relies on consistent network connectivity, and restricts the timing of medication doses. On the other hand, A-VOT allows patients to take medication at any time (including weekends and holidays), with or without network connectivity, but provides fewer opportunities for patient–provider interaction [45]. Furthermore, this technology is still relatively new and emerging, with limited information on its effectiveness and limitations. Therefore, VOT must be evaluated under more diverse conditions and settings to define its function and compare it with other existing technologies [46].
Mobile Health Applications (MHealth Apps)
The unprecedented increase in smartphones and wireless data transmission has led to many innovative mobile applications, some of which aim to monitor and improve medication adherence. However, these technologies, available on Google Play or the AppStore, have a significant drawback. Due to the poorly regulated app market, patients are both the supplier and interpreter of their data. In most countries, security and privacy issues make it impossible to share stored patient data in the cloud with healthcare providers for professional interpretation [48]. Nevertheless, a systematic review of randomized controlled trials with a meta-analysis conducted by Armitage et al found that App-based medication adherence interventions can improve patient adherence. Larger studies are required to evaluate this effect, including long-term sustainability [49].
Emocha vDOT (emocha Mobile Health, Inc) and AiCure are innovative applications designed to improve medication adherence through technology. Emocha vDOT, available on both Android and iOS platforms, facilitates A-VOT. Patients can record and share treatment videos while reporting any adverse effects they experience. The app includes a calendar feature for monitoring treatment progress and adherence [50]. New York-based AiCure, on the other hand, uses facial recognition and artificial intelligence (AI) to confirm that medication has been taken. [51]. This unique feature has proven cost-effective in treating active TB in Los Angeles County, California [52]. SureAdhere, another A-VOT app, shares similarities with Emocha vDOT in providing dose reminders, adverse reaction registration, virtual visits, and integration with various systems and devices. It stands out for its offline functionality and the ability to notify healthcare providers of missed doses [53]. Wisepill EVirMED works as a VOT app by connecting to a smart pill dispenser that records the opening of the pill box. It falls into the electronically monitored treatment solutions category, similar to AiCure and Emocha vDOT [47]. BMT4me© acts as a virtual assistant and aims to improve medication adherence in children by tracking medication intake in real time and sending reminders. Although only the study protocol has been published, the expected positive results align with the overall goal of improving medication adherence through technology [54].
However, when considering using mHealth apps based on VOT technology, it is essential to remember that self-monitored adherence is overestimated. This method does not reflect the faithful adherence to the drug regimen, as it does not reliably determine whether the patient swallowed the drug or not [55].
Artificial intelligence and machine learning can be essential in measuring adherence to medical recommendations in noncommunicable disease management. Machine learning is a subset of artificial intelligence that involves the development of algorithms and models that can learn and make predictions or decisions based on data. Large datasets are analyzed to identify patterns, correlations, and insights that can inform medical decisions and improve patient outcomes. It is a dynamic approach that allows systems to adapt and learn from experience, making it particularly useful for predicting medication adherence, understanding influencers, and optimizing treatment strategies. It is also the most widely used AI technology in healthcare. Machine learning models have also proved valuable in identifying critical variables associated with adherence in specific patient populations, such as those with hypertension and those following lifestyle patterns such as the Mediterranean diet. In addition, machine learning has been used to investigate the impact of medication adherence on clinical outcomes, demonstrating its potential to significantly improve patient outcomes. By analyzing large datasets, machine learning is helping to optimize treatment and adherence, particularly for complex diseases [56].
Electronic medication diaries (e-diaries) act as digital medication records. They allow participants to manually document their medication intake (and symptoms, if desired) using mobile devices such as phones, tablets, and computers. These devices are tightly integrated with a website or application. E-diaries include alerts that prompt participants to voluntarily answer pre-determined research questions, including adverse events (AE) and drug administration dates and times. Using this technology, participants complete the questionnaires electronically. The data are transmitted wirelessly. No changes can be made once participants have entered their data into the e-diary and confirmed its accuracy. Researchers then access the data securely stored in a dedicated cloud environment [43]. E-diaries were investigated for patients with skin conditions in outpatient clinical trials. A camera recording of the applied topical medication supported this tool. Patients rated the e-diary as good to excellent in terms of usability. The authors concluded that the e-diary may also be valuable for frequent and reliable monitoring of patient-reported outcomes in daily clinical practice. However, apart from the risk of bias, the main limitation is that older patients may need to become more familiar with digital tools [57].
Questionnaires and Scales
Medication adherence questionnaires and scales are inexpensive and easy-to-implement methods of assessing adherence. A large number of validated questionnaires are described in the literature. However, this area has no golden standard, and specific questionnaires are validated under particular conditions. Choosing the best questionnaire is complicated because “being the best” depends on several factors. The most crucial factor is the questionnaire’s psychometric properties: the more valid and reliable a questionnaire is, the more valuable it is [58]. Fahrni et al identified 59 different patient-reported outcome measures (PROMs) in their systemic review. These self-reported measures aim to quantify medication adherence based on responses to a nominal or Likert scale and assign categories to the total score [59].
As a self-report method, it is at risk of subjectivity and recall bias. Therefore, overestimation of adherence must be considered when analyzing patient-reported data. In addition, low patient literacy may be a barrier to use of this method.
Self-report adherence scales have the potential to measure both medication-taking behaviors and identify barriers and beliefs associated with adherence. Selecting an adherence scale requires consideration of what the adherence scale measures and how well it has been validated [60]. Identifying adherent or non-adherent patients depends on the type of questionnaire or scale. The most commonly used tools are listed in Table 2, along with information on patient adherence.
Different tests have different points at which they consider patients are adhering to their treatment plan. Usually, the cut-off point is when 80% of the prescribed medication is taken. For the Morisky Medication Adherence Scale (MMAS), cut-off points can be set by looking at how well patients control their blood pressure. Other measures, such as the Drug Attitude Inventory (DAI), the Adherence Attitude Inventory, and the Medication Adherence Self-Efficacy Scale-Revisio, divide people into those who were adherent and those who were not. They then compared the average scores of the 2 groups to find the cut-off [59].
The study by Fahrni et al showed that among the many instruments in this group of adherence measurement models, most are used to assess patients’ adherence to psychiatric disorders, antiretroviral therapy, and cardiovascular disease medication. Eight out of 59 instruments showed adequate, evidence-based psychometric properties and the ability to identify patients who are deliberately not taking their medication; these 8 instruments are the Rheumatology Compliance Questionnaire, Immunosuppressive Therapy Barrier Scale, Medication Adherence Rating Scale, Medication Satisfaction Questionnaire, Self-Efficacy for Appropriate Medication Use Scale (SEAMS), Medication Adherence Assessment Tool, Patient Medication Adherence Instrument and Healthcare Professional Medication Adherence Instrument, and Barriers to Oral Short-Term Antibiotic Adherence [59]. In addition, 2 measures with adequate evidence-based psychometric properties were found to identify those intentionally and unintentionally not adhering to good medication practice. These were the Adherence Starts with Knowledge-2066 and the Hill-Bone Scale questionnaires [59].
Tegegn et al conducted a systematic review encompassing 84 studies focused on patients with cardiovascular diseases (CVD), identifying 40 distinct Medication Adherence Patient-Reported Outcome Measures (MA-PROMs). Subsequently, these MA-PROMs underwent evaluation using the COnsensus-based Standards for selecting Health Measurement Instruments (COSMIN) checklist. The identified MA-PROMs were categorized into 3 groups based on their evaluation: A – recommend for use (8 MA-PROMs), B – potential for use (28 MA-PROMs), and C – not recommended for use (4 MA-PROMs). The A-rated MA-PROMs, Adherence to Refills and Medications Scale (ARMS and ARMS-7 – its 7-item version) were the best options for assessing medication adherence in patients with CVD. These tools comprehensively cover adherence and discontinuation phases, supported by moderate- to high-quality evidence on fundamental measurement properties. Utilizing a user-friendly 4-point Likert scale, ARMS and ARMS-7 are available free of charge to students and non-profit organizations [61]. This conclusion is also upheld for medication adherence to antihypertensive drugs, showing that ARMS is the most promising free, non-inferior alternative to Morisky, the most commonly used scale [62].
The Morisky Medication Adherence Scale, especially its 8-item version (MMAS-8), is the most widely used questionnaire for measuring adherence to antihypertensive medication [63]. Other commonly used instruments include the Hill-Bone Compliance (HB) to High Blood Pressure Therapy Scale, the Treatment Adherence Questionnaire for Patients with Hypertension (TAQPH), the Brief Medication Questionnaire (BMQ), the Compliance of Hypertensive Patients Scale (CHPS), the Facilitators of and Barriers to Adherence to Hypertension Treatment Scale (FATS), and the Self-Efficacy for Appropriate Medication Use Scale (SEAMS) [64]. Pareja-Martínez et al emphasize that there is no universally accepted questionnaire for measuring adherence to antihypertensive treatment, as none of the existing ones sufficiently meets all the guarantees of validity and reliability required to make it a benchmark questionnaire. The choice depends on the objectives of the clinician or researcher. Factors to consider include the desired level of patient information and time constraints. For comprehensive information, questionnaires such as the TAQPH, Maastricht Utrecht Adherence in Hypertension (MUAH), or Medication Adherence Self-Efficacy Scale (MASES) are recommended, whereas for rapid assessment with adequate validity and reliability, the MMAS-8, MARS-5, or HB may be appropriate [58]
Gagné et al analyzed 15 studies that reported 14 different patient-reported outcomes (PRO) instruments for medication adherence in asthma patients. In their systematic review, they found limited positive evidence for internal consistency of the Adherence Questionnaire, the Refined Medication Adherence Reason (MAR) scale, the Medication Adherence Report Scale for Asthma (MARS-A), and the Test of Adherence to Inhalers (TAI); reliability of the TAI; and structural validity of the Adherence Questionnaire, the MAR scale, the MARS-A, and the TAI. They also found limited negative evidence for hypothesis testing of the adherence questionnaire, the MARS-A reliability, and the MARS-A and TAI criterion validity. Therefore, no recommendation can be made regarding using a particular PRO in routine care or research settings [65]. However, the Self-Reported Medication-Taking Scale is the most commonly used questionnaire regarding respiratory disease. Importantly, Gagné et al suggest no PROs to measure initiation, adherence, and persistence with inhaled asthma maintenance medication [66].
Tosin et al evaluated questionnaires and scales in the context of their use in Parkinson’s disease (PD). Using the COSMIN risk of bias checklist, they rated 9 scales as “recommended,” “suggested,” and “listed.” None of the instruments evaluated met the “recommended” designation. The MMAS-8, the Beliefs Related to Medication Adherence Questionnaire, the Beliefs about Medication Questionnaire, the Medication Adherence Report Scale (MARS), and the Satisfaction with Information on Medicines Scale were classified as “suggested.” Therefore, the authors suggest that further work should focus on solving the problems of the proposed scales or developing a new scale that meets all the required criteria [67]. The previous systematic review by the same first author indicates that the most commonly used tool in PD is the MMAS. However, none of the reviewed scales measure all the recommended components essential in PD [68].
Vianna et al reported a gap in knowledge regarding the lack of validated tools to assess adherence to warfarin therapy. Limitations were found in tools that assessed medication use in isolation and the need for more analysis of other relevant aspects of therapy [69].
The MMAS was used to assess patients’ adherence to insulin. It was found that self-reporting utilizing this tool can help gather information on reasons for non-adherence and increase adherence as patients know they are being monitored. On the other hand, the authors point out the risk of patient dishonesty and the complexity and cost of data collection when used as a quality measure [70].
To assess medication adherence in patients with osteoporosis, Hesari et al identified 13 different questionnaires. Among these, the most commonly used was the MMAS with its modification for osteoporosis medication. However, due to the limitations of the questionnaires, the authors point out the need to develop a comprehensive tool to measure adherence to osteoporosis treatment recommendations and the factors influencing it, which does not have the problems of existing questionnaires and includes all aspects of osteoporosis treatment, barriers to treatment, patient perspective and other factors [71].
Ultimately, the critical considerations in the study of scale or questionnaire selection revolve around the measurement issue-defining ‘what’ is being measured – and the method of validation – determining ‘how’ measurements are justified. These 2 pillars are the cornerstones of the nuanced art of selecting the most appropriate scale for a given context [64].
New Developments in Adherence Monitoring Packages (EMPs)
The following features should characterize modern, innovative electronic medication packaging: to be portable to support travel and social commitments; to be context-aware of its surroundings and patient’s activities; to generate personalized reminders to patients and communicate as necessary; to monitor the vital signs of patients; to monitor patient’s adherence; and to communicate with healthcare professionals.
In a more detailed sense, contextual awareness means that the system considers diverse information about the patient’s conditions, medications, activities, and actions to perform its intended functions. This capability can make medication systems more intelligent and efficient [25]. Nevertheless, it is necessary to remember the limitations of EMPs. Although electronic monitoring is recommended to measure adherence accurately, it is a potential limitation because it may influence adherence behavior. It may also disrupt the routine of patients who have previously developed adherence strategies. In addition, the self-awareness effect (a conscious increase in adherence since medication intake is being monitored) can affect the reliability of the observed results [72].
Medication Event Monitoring System (MEMS)
MEMS are the most commonly used EMP devices in medication adherence research. Comparison of MEMS with self-report, pill count, and health assessment showed significant differences in adherence levels. Compared with MEMS, self-report overestimated adherence by 17%, pill count by 8%, and healthcare assessment by 6% [73]. Although the MEMS is considered the best way to estimate adherence, it has some limitations. First, the system cannot measure the number of pills taken from the bottle [74]. In addition, electronic closures require the drug of interest to be transferred into a bottle after deblistering from the original packaging, which can lead to stability issues. Commercial packaging comes in various sizes and shapes, making the development of generic e-labels prohibitively expensive [48]. In clinical trials, introducing a MEMS could also be very costly due to patient loss of the device and the need for hardware and software to retrieve data [75]. However, Hebing et al showed the effectiveness of MEMS in increasing patients’ adherence to disease-modifying antirheumatic drugs (DMARD) [76]. Ribaut et al assessed patients’ perceptions of 3 of the best-known MEMS devices – the MEMS Cap (a bottle cap that records each time the bottle is opened), the MEMS Helping Hand (a slider into which individual medication blisters can be inserted and which records the date and time of each removal), and the MEMS Button (a small device that the patient must press each time they take medication) [35].
All patients preferred the MEMS button to any of the other options suggested. This was the most practical, could be combined with existing dispensers, and was small enough to carry when you leave home. The researchers found the MEMS helping hand more convenient than the bottle-based system. However, a limitation of this device is that it needs to be customized for each blister, which can vary in shape and size. This is more problematic if drug doses change during therapy or the patient takes several drugs. So far, the MEMS cap has been recognized as the most widely used. However, it was found to be impractical due to its size, shape, and application method, highlighting an unexpected barrier to implementation in everyday life [35]. The MEMS system was found to be cost-effective for the management of infectious active tuberculosis in Morocco [77].
Wisepill Device
Wisepill technology for pharmaceuticals includes devices that hold tablets in 1, 2, or 7 compartments [78]. A mobile phone signal is sent and recorded in real time on a web-based server whenever the device is opened. The data are immediately available for research via an internet platform. In addition to logging the number of times the device has been opened, the Wisepill signal also provides information on the device’s remaining battery power, airtime on the SIM card, and signal strength. Haberer et al compared 3 methods of measuring adherence: self-report, MEMS, and Wisepill. No differences were found between MEMS and Wisepill. However, adherence was lower with the Wisepill compared with self-report. Nevertheless, the sample size was too small to show statistical significance. All users of Wisepill found it easy and convenient to use. Another strength of this device was that it did not look like a traditional pill box [79]. Besides the limitations reported in other types of EMP, Wisepill’s weaknesses are the need to recharge the box, low convenience for traveling, and the inability to hold all the pills [79,80].
SMARxT Cap
SMARxT Cap is an electronic reminder cap system that fits standard prescription bottles (USA). It is programmed to alert the patient with beeps and flashes when each dose of medication is due. The device also has a visual timer that counts minutes and hours between doses. Each time the bottle is opened, the data record is saved, and the time is reset to zero.
Pharmacists program the cap during dispensing according to the prescription instructions. Mehas et al used a SMARxT cap to assess its usability for adherence to antihypertensive medication. They compared the cap with a placebo cap without audio or visual warnings. However, their results were insignificant; the improvement in adherence and the reduction in blood pressure were noted. The SMARxT cap costs about $10 each. They point out that this technology has the potential to characterize and improve medication adherence and to provide clinicians with an additional source of data to describe patients’ medication use. However, further research on a larger patient population is needed to determine the impact of the SMARxT on patient adherence and health outcomes [81].
The Pletaal Assist System® is another EMP that records the time and date of medication taken. The device flashes when the patient should take the medication. The pharmacist can set the flashing time. The device stops flashing when the medication has been taken. PAS can be connected to a smartphone, and the data can be analyzed using an application.
This device has been used by Oura et al for outpatient monitoring and improvement of cilostazol adherence. They found that PAS can significantly improve adherence to cilostazol in poorly adherent outpatients. However, we must emphasize the limitations of this study. First, the assessment of patient adherence was based on pill counting, a method prone to overestimation. Second, the study’s sample size was small and showed an exceptionally high adherence rate. Finally, although the PAS could record the removal of the medication from the device, it could not confirm whether patients had taken the medication [75].
One-Dose Package Medication Support System (ODP-MSS)
The ODP-MSS works as a medication dispenser, simultaneously encapsulating individual doses of multiple medications in separate film pouches. These pouches are then placed on a rotating drum. The system can dispense up to 6 single-dose packs per day for a total of 60 days. Patients can refill the ODP-MSS themselves, but short-term treatment medication must be taken separately due to the extended refill cycle. The device should be connected to a diverging telephone line. The ODP-MSS is marketed as the Fukkun FS-2000 Medication Support System (Ishigami Factory Co. Ltd, Hanamaki City, Japan) [82].
The system can use music alerts to remind patients to take their medication. If the patient misses a dose, a voice message is sent by telephone to a medication reminder. The system also allows the nurse to check the patient’s health status over the phone. Patients using the ODP-MSS can press a “going-out” button to pre-dose the next ODP before they leave. Pressing the button twice or more triggers an automatic “going out” voice message sent to medication support staff by telephone. The ODP-MSS has an internal memory to store medication-related data, such as medication removal status, automatic call events, and going-out switch activity. This internal memory enables the assessment of medication adherence. The researchers found that the device effectively prevented patients from missing doses and provided telecare home monitoring for older people living independently at home. The ODP-MMS was also helpful in reducing the burden of medication support and medication errors for staff in group homes for older people with dementia – the limitations reported by patients related to equipment jamming. Patients felt obliged to stay home during medication administration, and caregivers received too many phone calls. The researchers suggest that the product needs to be improved and tested on a larger group of patients [82].
ReX
ReX is a hand-held medication management system designed to deliver solid oral medication on demand according to a pre-programmed treatment protocol. ReX monitors and controls medicines from packaging to patient ingestion and provides robust, real-time adherence data. The system allows patients to report results, participate in surveys, and receive messages and instructions. ReX includes a reusable medication dispenser, a disposable pill cassette, a cellphone application, and a cloud-based data portal.
The Drug Dispensing Unit (DDU) facilitates pill administration through a touch screen that displays patient-specific surveys and therapy details. Equipped with a rechargeable battery, status indicators, a pill window, sensors, and Bluetooth connectivity to a mobile app, the DDU transmits therapy data to a dedicated cloud domain. It also securely holds and locks the disposable cassette containing the pills. The disposable cassette is a secure, tamper-resistant container that comes pre-loaded with bulk pills in 16 separate compartments. It is unlocked only when inserted into the DDU, which has an integral mouthpiece with an anti-choking mechanism for safe pill intake. After use, the DDU automatically releases the empty cassette, facilitating cassette replacement by the user. The mobile app facilitates data transfer between the DDU and the Dose-E Analytics cloud. Nurses can set up and monitor therapy online and track patient compliance. In the event of a missed dose, the cloud automatically sends alerts to a pre-defined contact person or the call center. In the 4-day ReX study, personalized reminders boosted dosage adherence by 18%, explaining the notable difference in adherence rates compared to the control test. Before personalized reminders, adherence rates were similar, highlighting the impact of real-time, on-demand reminders and the limited effectiveness of conventional alerts, often ignored by users [22].
Smart Blister Packs
Bruxvoort et al designed and developed EMP, called Smart Blister Pack, to examine the validity of self-reported adherence to artemether-lumefantrine (AL) in southern Tanzania [29]. Smart Blister Pack was designed in the same way as locally available AL blister packs, with a slight thickness in the area of the top center images due to the electronic tag and the cell battery.
The device consists of a fine wire connected to a microchip. The wire runs through each blister. When a tablet is pushed through the foil, the wire is broken. The exact date and time of this event are recorded on the chip. The researchers found significant differences between self-reported adherence and adherence measured by the Smart Blister Pack. The latter showed lower estimates of timely completion of AL. The advantages of this EMP include objective data, real-time monitoring, improved accuracy, study standardization, and reduced over-reporting. However, some disadvantages were also reported. Technology limitations, patient awareness and involvement, cost and implementation, external interference, and complexity of interpretation are limitations of this device. Therefore, intelligent blisters should be improved in the future. They need to reduce the possibility of recording when pills are not completely removed. Also, the bulge in the packaging should be less noticeable. Nevertheless, this device may be helpful when data on adherence patterns are desirable for assessing treatment outcomes.
SmartMed
The SmartMed system comprises 5 components: a pill bottle device, a local base station, a cloud data service, an end user or patient, and a care provider. The bottle device detects when it is opened and records each event. It also provides users with a method of storing pills and alerts them via audio and visual cues when it is time to take their next dose. The device includes a snooze button that allows users to set an alarm. The base station establishes wireless communication with the pill bottle devices and facilitates data exchange with the cloud service. The cloud component is a secure data repository that manages pill bottle devices and users. An Application Programming Interface enables data transfer between local base stations, clients, and the data service. There are 2 types of clients: end users receiving medication support and care providers. Both can access and update information via the cloud data service, with different interfaces for patients/families and healthcare professionals [37].
Time4Med
The Time4Med™ EMP (Adherence Innovations, Hong Kong) is a small electronic card that can be attached to medication packaging. It records the date and time of administration when a button is pressed. Arnet et al validated this EMP in polypharmacy outpatients. Twenty volunteers used Time4Med™ devices for 14 days with a virtual intake of 3 times a day. The devices demonstrated high functionality, sensitivity, specificity, and recovery. Except for pushing the button, volunteer and patient satisfaction was very high. In addition, Time4Med™ devices demonstrated high accuracy in recording, storing, and delivering electronic data for multiple medication administrations, making them well-accepted by elderly patients. These devices, recommended for clinical trials and practitioners, meet the criteria of small size, ease of use, low intrusiveness, and affordability. They have proven effective in polypharmacy scenarios, ensuring secure data transfer and analysis by healthcare providers. Overall, Time4MedTM devices provide accurate monitoring and are suitable for practitioners studying adherence in outpatients, particularly those with polypharmacy, and for integration into clinical trials [48]. The team of Albert et al evaluated individual patients’ strategies to manage the drugs with Time4Med™ among patients receiving direct oral anticoagulant inhibitors (DOAC). They found that 4 weeks of electronic monitoring revealed deviant behavior, such as missed doses and cognitive difficulties. In particular, pharmacist home visits may be an appropriate format to support patients in understanding and optimizing their medication management at every stage [83]. Further research is now needed to assist practitioners in interpreting the recorded data and, ultimately, to support clinical decision-making [48].
Smart Pens
Intelligent pens are devices designed to improve patient adherence to insulin management and thereby improve blood glycemic control. Although smart pens look the same as traditional insulin pens, they can record and store insulin injection data. The technological evolution of these devices offers new features such as Bluetooth connectivity, bolus dose calculators, and integration with mobile apps and continuous glucose monitors [84]. An example of a smart pen is the InPenTM Smart Insulin Pen, which Medtronic Company delivered. In addition to the features listed above, this device can also provide dose reminders and alerts, deliver half-units of insulin, alert on temperature, track active insulin, and does not need to be charged [85].
Only a limited number of clinical trials have released data demonstrating advantages in adherence, A1c improvement, and time in range (TIR). Available data show the potential to reduce suboptimal insulin use and missed doses. Satisfaction of people with diabetes with smart pens is high, which may lead to improved adherence. This could result in smart pens being considered part of routine clinical care for people with diabetes [84]. Barriers to the use of intelligent pens include the limited availability of the devices and their higher cost compared to traditional insulin pens. In addition, intelligent pens require additional training and technology transition costs. Moreover, healthcare professionals must be able to retrieve data from the smart pen, interpret the information, and develop an appropriate insulin plan. Both clinicians and patients should consider the user experience associated with smart pens and their applications. There may also be patient-specific barriers that could hinder the widespread adoption of smart pens. There is a need for clinician and patient education and more clinical trials to demonstrate the benefits and cost-effectiveness of intelligent pens [84,86].
Smart Inhaler
Smart inhaler devices are used for inhalation therapy in patients with asthma and chronic obstructive pulmonary disease (COPD). These devices can record the time and date of each inhalation and transmit this data wirelessly to a secure web database once installed on the inhaler. Improving the measurement of adherence to the inhalation of dry powder capsules can be achieved through the use of the Polymedication Electronic Monitoring System (POEMS). This technology consists of printed, self-adhesive polymer films with loops of conductive wires that can be attached to multidose punch cards. When a powder capsule is removed from the blister, a broken loop causes a change in electrical resistance, allowing the event to be measured and recorded with date and time. Smart inhalers and POEMS reports determine whether patients have taken their medication at the correct time and dose [27]. To improve patient adherence, the system can be enhanced with a smartphone-generated audio reminder (for SmartInhaler), alarm clock (for POEMS) via mobile application, or tele-intervention from a healthcare provider [87]. As the SmartInhaler device has been approved for daily use and its usability in improving medication adherence (primarily supported by some reporting of medication intake), its implementation in developed countries should be considered. However, it has certain limitations – clinicians must have sufficient time to review adherence data and provide appropriate feedback to patients, and the device is expensive [27,87], at around ≤100 in 2018. In addition to the price, access to software that enables real-time monitoring after uploading data to a mobile or cloud-based application costs a monthly fee [48]. Jansen et al found intelligent inhalers to treat asthma and COPD can be cost-effective, but more studies are needed to confirm this [88]. However, the main limitation of these devices is that they do not prevent poor inhalation techniques; therefore, improvement in technology is necessary [89].
Ingestible Biosensors (IS)
Advances in healthcare technology continue to reshape the landscape of patient care. They offer innovative solutions to long-standing challenges. One of these breakthroughs is the emergence of ingestible biosensors to monitor and measure medication adherence. A system for measuring adherence using ingestible biosensors typically consists of a biosensor embedded in a tablet/capsule, a detector patch applied to the skin, and a mobile app to transmit the detector data [90,91]. One such system is the Digital Health Feedback System (DHFS). An integrated sensor system enables accurate date- and time-stamping of oral medication ingestion. This system includes an ingestion sensor with thin layers of commonly ingested excipients, an adhesive-backed detector patch worn on the torso, and a paired mobile device. Upon ingestion, the sensor separates, energizes, and communicates with the detector patch, which records physiological metrics. The system is powered by sensors that use the electrolytes in the stomach (independent of pH) to power the galvanic battery. Data, including heart rate and activity, are wirelessly transmitted to a paired device (eg, phone or tablet) and uploaded to a secure central repository. Patients can access real-time data on their mobile devices, and, with consent, healthcare professionals can access data via a secure web portal. The DHFS has demonstrated high reliability and accuracy, with a positive detection rate of approximately 99% in clinical studies involving nearly 30 000 sensor insertions. The Proteus Digital Health Feedback Device received CE Mark approval for the European Union market in 2010 and FDA approval as a medical device in 2012 [90]. Another system is the Ingestible Event Maker combined with enteric-coated mycophenolate sodium (IEM-ECMPS). Eisenberger et al tested this system to assess patient adherence after kidney transplantation. The system communicated with the detector within 5 to 10 min. The IEM-ECMPS combination product was manufactured by Novartis Pharma (Basel, Switzerland) [92]. The MyTMed system was used in the study by Chai et al. The core of MyTMed is a digital pill consisting of a standard gelatin capsule with a unique radiofrequency emitting tag. When a patient swallows the digital pill, the gelatin capsule dissolves in the stomach, releasing the study drug. Contact with gastric pH activates the tag, generating a unique radio frequency signal transmitted to a receiver worn on the hip (the Hub). The Hub acts as a relay, using Short Message System (SMS) protocols to send a packet of data, including ingestion time and event, to a cloud-based web server. The transmission from the radio frequency tag on the digital pill is unique and correlates with the encapsulated medication. If a patient ingests 2 digital pills simultaneously, the Hub receives 2 unique radio frequency signals, defining 2 separate ingestion events. The radiofrequency transmission lasts approximately 30 min as the digital pill passes through the gastrointestinal system, and the insoluble radiofrequency tag is excreted [91]. Dukes et al, in their review, point out the unique role of ingestible biosensors in patients prescribed opioids and antipsychotic drugs [93]. The limitations of this technology are mainly connected with the high costs. For example, the Abilify Mycite® (aripiprazole IS) tablet costs approximately $66 per tablet, or about $2000 monthly. In addition, the ethical nature of IS has been questioned and is still an issue that needs to be considered before sensor tablets are introduced into general healthcare practice. Another question is whether patch-based technology is optimal for monitoring adherence. Patches are prone to user error and may make digital medicine systems (DMS) less reliable [93]. Nevertheless, these systems tend to be well tolerated by patients, and their ability to measure adherence promises their use in the clinic by providing continuous patient-level feedback. In addition, the proven safety of these ingestible integrated circuits sets the stage for a new era of ‘smart’ drug delivery, capable of generating specialized drug release profiles, targeting specific sites, and responding to local sensing events [94,95]. The ingestible sensor system promises many opportunities to monitor and improve the health of older adults, and can give older people the confidence to take charge of their health. For healthcare providers, the system will provide feedback on whether medication adherence is achieving the desired outcome, potentially helping them to create a personalized treatment plan for the patient (Table 1) [96–98].
Future Initiatives
Considering all of the presented methods and strategies for assessing a patient’s medication adherence, we can identify the characteristics of a “perfect tool”, whose features are presented in Table 3.
However, the above requirements could only be met for some disease management. Different drug delivery routes require different solutions. In addition, some specific conditions require dedicated approaches. Nevertheless, we see great potential in using artificial intelligence and machine learning to provide patients with a personalized tool. In the age of smartphones, the future of medication adherence measurement is linked to new technologies. Systems may be able to integrate many methods (subjective and objective), independently process the data received, and finally propose a solution to improve adherence. However, the healthcare provider (doctor, nurse, pharmacist, or other medical staff) should supervise this process. With the robust development of artificial intelligence algorithms, the design of such a system seems closer rather than farther away. However, the overriding condition must be the cost-effectiveness of this solution. In addition, the costs must not be passed on to the patient. Nevertheless, further work is needed to develop technologies and methods to measure patient adherence to improve patient safety and reduce the system’s additional costs caused by poor adherence, secondary hospitalizations, and worsening patient conditions.
Conclusions
Over the past few decades, researchers have become increasingly interested in methods to measure patient adherence to medical recommendations. The literature offers a plethora of both subjective and objective methods. However, despite the many measurement tools available, it is impossible to conclusively determine the criterion standard for measuring patient adherence. Table 4 summarizes the main conclusions of this review’s medication adherence measurement methods.
Figures
![Main reasons for patients’ non-adherence (according to [11–13]). The illustration was created using Canva Pro (Canva Pty Ltd).](https://jours.isi-science.com/imageXml.php?i=medscimonit-30-e944605-g001.jpg&idArt=944605&w=1000) Figure 1. Main reasons for patients’ non-adherence (according to [11–13]). The illustration was created using Canva Pro (Canva Pty Ltd).
Figure 1. Main reasons for patients’ non-adherence (according to [11–13]). The illustration was created using Canva Pro (Canva Pty Ltd).  Figure 2. Classification of medication adherence measurement methods: Objective vs subjective, direct vs indirect. The illustration was created using Canva Pro (Canva Pty Ltd).
Figure 2. Classification of medication adherence measurement methods: Objective vs subjective, direct vs indirect. The illustration was created using Canva Pro (Canva Pty Ltd). Tables
Table 1. Summary of identified methods for measuring medication adherence.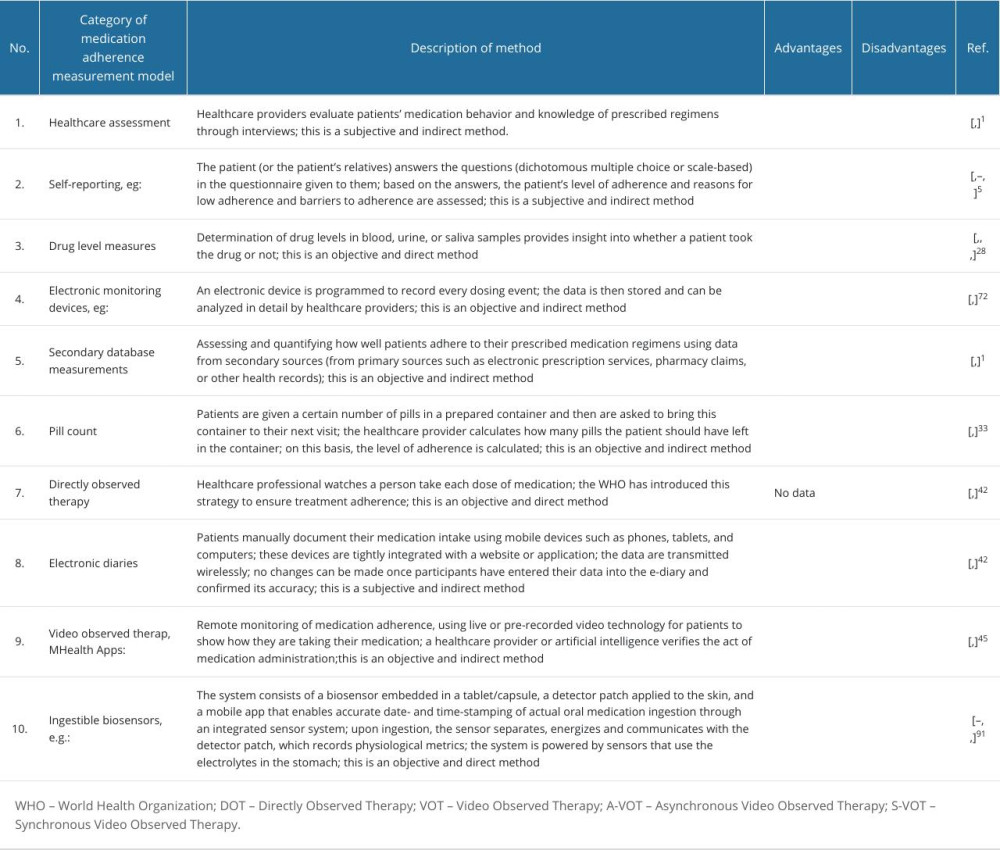 Table 2. List of questionnaires and scales for adherence measures and information on patient adherence determination.
Table 2. List of questionnaires and scales for adherence measures and information on patient adherence determination. Table 3. Key attributes of an optimal medication adherence measurement tool.
Table 3. Key attributes of an optimal medication adherence measurement tool. Table 4. Conclusions drawn from the literature review on selected methods for assessing patients’ medication adherence.
Table 4. Conclusions drawn from the literature review on selected methods for assessing patients’ medication adherence.
References
1. Lam WY, Fresco P, Medication adherence measures: An overview: Biomed Res Int, 2015; 2015; 217047
2. Tilson HH, Adherence or compliance? Changes in terminology: Ann Pharmacother, 2004; 38(1); 161-62
3. Kleinsinger F, The unmet challenge of medication nonadherence: Perm J, 2018; 22; 18-33
4. Brown MT, Bussell JK, Medication adherence: WHO cares?: Mayo Clin Proc, 2011; 86(4); 304-14
5. Osterberg L, Blaschke T, Adherence to medication: N Engl J Med, 2005; 353(5); 487-97
6. Burkhart PV, Sabaté E, Adherence to long-term therapies: Evidence for action: J Nurs Scholarsh, 2003; 35(3); 207
7. : Medication Adherence – Taking Your Meds as Directed, American Heart Association Available online: https://www.heart.org/en/health-topics/consumer-healthcare/medication-information/medication-adherence-taking-your-meds-as-directed
8. Jansen PA, Brouwers JR, Clinical pharmacology in old persons: Scientifica (Cairo), 2012; 2012; 723678
9. Gast A, Mathes T, Medication adherence influencing factors-an (updated) overview of systematic reviews: Syst Rev, 2019; 8(1); 112
10. Náfrádi L, Nakamoto K, Schulz PJ, Is patient empowerment the key to promote adherence? A systematic review of the relationship between self-efficacy, health locus of control and medication adherence: PLoS One, 2017; 12(10); e0186458
11. Abdullah NF, Khuan L, Theng CA, Sowtali SN, Prevalence and reasons influenced medication non-adherence among diabetes patients: A mixed-method study: J Diabetes Metab Disord, 2022; 21(2); 1669-78
12. While A, Medication adherence: Understanding the issues and finding solutions: Br J Community Nurs, 2020; 25(10); 474-79
13. MacLaughlin EJ, Raehl CL, Treadway AK, Assessing medication adherence in the elderly: Which tools to use in clinical practice?: Drugs Aging, 2005; 22(3); 231-55
14. Wu JR, Moser DK, Medication adherence mediates the relationship between heart failure symptoms and cardiac event-free survival in patients with heart failure: J Cardiovasc Nurs, 2018; 33(1); 40-46
15. Thanh Pham S, Anh Nguyen T, Minh Tran N, Medication adherence in cardiovascular diseases [Internet]: Novel Pathogenesis and Treatments for Cardiovascular Disease, 2023, IntechOpen Available from: http://dx.doi.org/10.5772/intechopen.108181
16. Wu JR, Moser DK, Medication adherence mediates the relationship between heart failure symptoms and cardiac event-free survival in patients with heart failure: J Cardiovasc Nurs, 2018; 33(1); 40-46
17. Simpson SH, Eurich DT, Majumdar SR, A meta-analysis of the association between adherence to drug therapy and mortality: BMJ, 2006; 333(7557); 15
18. Zaugg V, Korb-Savoldelli V, Durieux P, Sabatier B, Providing physicians with feedback on medication adherence for people with chronic diseases taking long-term medication: Cochrane Database Syst Rev, 2018; 1(1); CD012042
19. Chaudri NA, Adherence to long-term therapies evidence for action: Ann Saudi Med, 2004; 24(3); 221-22
20. : 8 Reasons Patients Don’t Take Their Medications, American Medical Association Available online: https://www.ama-assn.org/delivering-care/patient-support-advocacy/8-reasons-patients-dont-take-their-medications
21. Rivera K, Experian health: How healthcare organizations can stop patient medication non-adherence Available online: https://www.experian.com/blogs/healthcare/2020/01/how-healthcare-organizations-can-stop-patient-medication-non-adherence/
22. Shtrichman R, Conrad S, Schimo K, Use of a digital medication management system for effective assessment and enhancement of patient adherence to therapy (ReX): Feasibility study: JMIR Hum Factors, 2018; 5(4); e10128
23. Farmer KC, Methods for measuring and monitoring medication regimen adherence in clinical trials and clinical practice: Clin Ther, 1999; 21(6); 1074-73
24. Dew MA, Dabbs AD, Myaskovsky L, Meta-analysis of medical regimen adherence outcomes in pediatric solid organ transplantation: Transplantation, 2009; 88(5); 736-46
25. Varshney U, Smart medication management system and multiple interventions for medication adherence: Decis Support Syst, 2013; 55; 538-51
26. Wheeler SB, Spencer J, Drier SW, Motivational interviewing counseling to increase endocrine therapy adherence in diverse patients: Cancers (Basel), 2023; 15(7); 1973
27. Gregoriano C, Dieterle T, Dürr S, Impact of an electronic monitoring intervention to improve adherence to inhaled medication in patients with asthma and chronic obstructive pulmonary disease: Study protocol for a randomized controlled trial: JMIR Res Protoc, 2017; 6(10); e204
28. Souares A, Moulin P, Sarrassat S, Self-reported data: A major tool to assess compliance with anti-malarial combination therapy among children in Senegal: Malar J, 2009; 8; 257
29. Bruxvoort K, Festo C, Cairns M, Measuring patient adherence to malaria treatment: A comparison of results from self-report and a customised electronic monitoring device: PLoS One, 2015; 10(7); e0134275
30. Eskås PA, Heimark S, Eek Mariampillai J, Adherence to medication and drug monitoring in apparent treatment-resistant hypertension: Blood Press, 2016; 25(4); 199-205
31. Abdessadek M, Magoul R, Amarti A, [Customizing dosage drugs what contribution in therapeutic drug monitoring?]: Ann Biol Clin (Paris), 2014; 72(1); 15-24 [in French]
32. Appelgren KE, Nietert PJ, Hulsey TC, Analyzing adherence to prenatal supplement: Does pill count measure up?: Int J Endocrinol, 2010; 2010; 631971
33. Hannaford A, Arens Y, Koenig H, Real-time monitoring and point-of-care testing: A review of the current landscape of PrEP adherence monitoring: Patient Prefer Adherence, 2021; 15; 259-69
34. Niechciał E, Acerini CL, Chiesa ST, Medication adherence during adjunct therapy with statins and ACE inhibitors in adolescents with type 1 diabetes: Diabetes Care, 2020; 43(5); 1070-76
35. Ribaut J, De Geest S, Leppla L, Exploring stem cell transplanted patients’ perspectives on medication self-management and electronic monitoring devices measuring medication adherence: A qualitative sub-study of the swiss SMILe implementation science project: Patient Prefer Adherence, 2022; 16; 11-22
36. Riekert KA, Rand CS, Electronic monitoring of medication adherence: when is high-tech best?: J Clin Psychol Med Settings, 2002; 9; 25-34
37. Diemert S, Richardson K, Hunter P, SmartMed: A medication management system to improve adherence: Stud Health Technol Inform, 2015; 208; 125-30
38. Checchi KD, Huybrechts KF, Avorn J, Kesselheim AS, Electronic medication packaging devices and medication adherence: A systematic review: JAMA, 2014; 312(12); 1237-47
39. Kurup R, Martínez JPD, Doucet M, Tyrrell PN, Effectiveness of electronic medication packaging devices on medication adherence: A scoping review: J Gerontol Nurs, 2020; 46(3); 27-36
40. Karumbi J, Garner P, Directly observed therapy for treating tuberculosis: Cochrane Database Syst Rev, 2015; 2015(5); CD003343
41. Altice FL, Maru DS, Bruce RD, Superiority of directly administered antiretroviral therapy over self-administered therapy among HIV-infected drug users: A prospective, randomized, controlled trial: Clin Infect Dis, 2007; 45(6); 770-78
42. Sazali MF, Rahim SSSA, Mohammad AH, Improving tuberculosis medication adherence: The potential of integrating digital technology and health belief model: Tuberc Respir Dis (Seoul), 2023; 86(2); 82-93
43. Adje YH, Brooks KM, Castillo-Mancilla JR, The use of technology-based adherence monitoring in the treatment of hepatitis C virus: Ther Adv Infect Dis, 2022; 9; 20499361221095664
44. Pavlyuchenkova NA, Vasilyeva IA, Samoylova AG, Tyulkova TE, Video observed treatment is an innovative method of tuberculosis treatment observation in resource-limited health care settings: Tuberc Lung Dis, 2022; 100; 53-60
45. Garfein RS, Doshi RP, Synchronous and asynchronous video observed therapy (VOT) for tuberculosis treatment adherence monitoring and support: J Clin Tuberc Other Mycobact Dis, 2019; 17; 100098
46. Story A, Garfein RS, Hayward A, Monitoring therapy compliance of tuberculosis patients by using video-enabled electronic devices: Emerg Infect Dis, 2016; 22(3); 538-40
47. Keutzer L, Wicha SG, Simonsson US, Mobile health apps for improvement of tuberculosis treatment: Descriptive review: JMIR Mhealth Uhealth, 2020; 8(4); e17246
48. Arnet I, Rothen JP, Hersberger KE, Validation of a novel electronic device for medication adherence monitoring of ambulatory patients: Pharmacy (Basel), 2019; 7(4); 155
49. Armitage LC, Kassavou A, Sutton S, Do mobile device apps designed to support medication adherence demonstrate efficacy? A systematic review of randomised controlled trials, with meta-analysis: BMJ Open, 2020; 10(1); e032045
50. Holzman SB, Atre S, Sahasrabudhe T, Use of smartphone-based video directly observed therapy (vDOT) in tuberculosis care: Single-arm, prospective feasibility study: JMIR Form Res, 2019; 3(3); e13411
51. Bain EE, Shafner L, Walling DP, Use of a novel artificial intelligence platform on mobile devices to assess dosing compliance in a phase 2 clinical trial in subjects with schizophrenia: JMIR Mhealth Uhealth, 2017; 5(2); e18
52. Salcedo J, Rosales M, Kim JS, Cost-effectiveness of artificial intelligence monitoring for active tuberculosis treatment: A modeling study: PLoS One, 2021; 16(7); e0254950
53. : Sureadhere Platform Available online: https://www.sureadhere.com
54. Ralph JE, Sezgin E, Stanek CJ, Improving medication adherence monitoring and clinical outcomes through mHealth: A randomized controlled trial protocol in pediatric stem cell transplant: PLoS One, 2023; 18(8); e0289987
55. Larsen KG, Areberg J, Åström DO, Are self-reported and self-monitored adherence good proxies for reaching relevant plasma concentrations?: Experiences from a study of anti-depressants in healthy volunteers: Clin Trials, 2021; 18(4); 505-10
56. Babel A, Taneja R, Mondello Malvestiti F, Artificial intelligence solutions to increase medication adherence in patients with non-communicable diseases: Front Digit Health, 2021; 3; 669869
57. Rijsbergen M, Niemeyer-van der Kolk T, Rijneveld R, Mobile e-diary application facilitates the monitoring of patient-reported outcomes and a high treatment adherence for clinical trials in dermatology: J Eur Acad Dermatol Venereol, 2020; 34(3); 633-39
58. Pareja-Martínez E, Esquivel-Prados E, Martínez-Martínez F, García-Corpas JP, Questionnaires on adherence to antihypertensive treatment: A systematic review of published questionnaires and their psychometric properties: Int J Clin Pharm, 2020; 42(2); 355-65
59. Fahrni ML, Saman KM, Alkhoshaiban AS, Patient-reported outcome measures to detect intentional, mixed, or unintentional non-adherence to medication: A systematic review: BMJ Open, 2022; 12(9); e057868
60. Nguyen TM, La Caze A, Cottrell N, What are validated self-report adherence scales really measuring?: A systematic review: Br J Clin Pharmacol, 2014; 77(3); 427-45
61. Tegegn HG, Wark S, Tursan d’Espaignet E, Spark MJ, Measurement properties of patient-reported outcome measures for medication adherence in cardiovascular disease: A COSMIN systematic review: Clin Drug Investig, 2022; 42(11); 879-908
62. Al-Alaili MK, Abdi AM, Basgut B, Test performance of self-report adherence tools in patients with hypertension: A systematic review and a meta-analysis: J Clin Pharm Ther, 2022; 47(12); 1932-44
63. Tola Gemeda A, Regassa LD, Weldesenbet AB, Adherence to antihypertensive medications and associated factors among hypertensive patients in Ethiopia: Systematic review and meta-analysis: SAGE Open Med, 2020; 8; 2050312120982459
64. Uchmanowicz B, Szymańska-Chabowska A, Jankowska-Polańska B, Assessment of adherence to medication for cardiovascular diseases: measurement tools: Cardiovasc J Afr, 2019; 30(2); 113-19
65. Gagné M, Boulet LP, Pérez N, Moisan J, Patient-reported outcome instruments that evaluate adherence behaviours in adults with asthma: A systematic review of measurement properties: Br J Clin Pharmacol, 2018; 84(9); 1928-40
66. Gagné M, Boulet LP, Pérez N, Moisan J, Adherence stages measured by patient-reported outcome instruments in adults with asthma: A scoping review: J Asthma, 2020; 57(2); 179-87
67. Tosin MHS, de Oliveira BGRB, Goetz CG, Rating scales for medication adherence in Parkinson’s disease: A systematic review for critique and recommendations: Mov Disord Clin Pract, 2022; 10(2); 175-89
68. Tosin MHS, Stebbins GT, Goetz CG, Measuring medication adherence in Parkinson’s disease: A systematic review of contributing components in rating scales: Mov Disord Clin Pract, 2020; 7(6); 607-15
69. Vianna MS, da Silva Praxedes MF, de Araújo VE, Self-report instruments for assessing adherence to warfarin therapy: A systematic review: Eur J Clin Pharmacol, 2021; 77(12); 1765-81
70. Stolpe S, Kroes MA, Webb N, Wisniewski T, A systematic review of insulin adherence measures in patients with diabetes: J Manag Care Spec Pharm, 2016; 22(11); 1224-46
71. Hesari E, Sanjari M, Mansourzadeh MJ, Osteoporosis medication adherence tools: A systematic review: Osteoporos Int, 2023; 34(9); 1535-48
72. Sutton S, Kinmonth AL, Hardeman W, Does electronic monitoring influence adherence to medication? Randomized controlled trial of measurement reactivity: Ann Behav Med, 2014; 48(3); 293-99
73. El Alili M, Vrijens B, Demonceau J, A scoping review of studies comparing the medication event monitoring system (MEMS) with alternative methods for measuring medication adherence: Br J Clin Pharmacol, 2016; 82(1); 268-79
74. Michaud K, Vrijens B, Tousset E, Real-world adherence to oral methotrexate measured electronically in patients with established rheumatoid arthritis: ACR Open Rheumatol, 2019; 1(9); 560-70
75. Oura K, Itabashi R, Omoto T, Impact of introducing the pletaal assist system on drug adherence in outpatients with ischaemic stroke: A pilot study: Patient Prefer Adherence, 2021; 15; 835-41
76. Hebing RC, Aksu I, Twisk JW, Effectiveness of electronic drug monitoring feedback to increase adherence in patients with RA initiating a biological DMARD: A randomised clinical trial: RMD Open, 2022; 8(1); e001712
77. Yang J, Kim HY, Park S, Cost-effectiveness of a medication event monitoring system for tuberculosis management in Morocco: PLoS One, 2022; 17(4); e0267292
78. : Wisepill Medication Adherence Solutions Through Innovation Available online: https://www.wisepill.com/accessories
79. Haberer JE, Kahane J, Kigozi I, Real-time adherence monitoring for HIV antiretroviral therapy: AIDS Behav, 2010; 14(6); 1340-46
80. Craker L, Tarantino N, Whiteley L, Brown L, Measuring antiretroviral adherence among young people living with HIV: Observations from a Real-time monitoring device versus self-report: AIDS Behav, 2019; 23(8); 2138-45
81. Mehas N, Hudmon KS, Jaynes H, Impact of electronic medication reminder caps on patient adherence and blood pressure: J Pharm Technol, 2021; 37(5); 234-43
82. Suzuki R, Hasegawa T, Evaluation of a one-dose package medication support system for community-based elderly patients and eldercare facilities: Am J Health Syst Pharm, 2018; 75(9); e202-e12
83. Albert V, Baumgartner PC, Hersberger KE, Arnet I, How do elderly outpatients manage polypharmacy including DOAC – a qualitative analysis highlighting a need for counselling: Res Social Adm Pharm, 2022; 18(6); 3019-26
84. Sy SL, Munshi MM, Toschi E, Can smart pens help improve diabetes management?: J Diabetes Sci Technol, 2022; 16(3); 628-34
85. Gildon BW, InPen smart insulin pen system: Product review and user experience: Diabetes Spectr, 2018; 31(4); 354-58
86. Cranston I, Jamdade V, Liao B, Newson RS, Clinical, economic, and patient-reported benefits of connected insulin pen systems: A systematic literature review: Adv Ther, 2023; 40(5); 2015-37
87. Gregoriano C, Dieterle T, Breitenstein AL, Does a tailored intervention to promote adherence in patients with chronic lung disease affect exacerbations? A randomized controlled trial: Respir Res, 2019; 20(1); 273
88. Jansen EM, van de Hei SJ, Dierick BJH, Global burden of medication non-adherence in chronic obstructive pulmonary disease (COPD) and asthma: A narrative review of the clinical and economic case for smart inhalers: J Thorac Dis, 2021; 13(6); 3846-64
89. Greene G, Costello RW, Personalizing medicine – could the smart inhaler revolutionize treatment for COPD and asthma patients?: Expert Opin Drug Deliv, 2019; 16(7); 675-77
90. Browne SH, Peloquin C, Santillo F, Digitizing medicines for remote capture of oral medication adherence using co-encapsulation: Clin Pharmacol Ther, 2018; 103(3); 502-10
91. Chai PR, Rosen RK, Boyer EW, Ingestible biosensors for real-time medical adherence monitoring: MyTMed: Proc Annu Hawaii Int Conf Syst Sci, 2016; 2016; 3416-23
92. Eisenberger U, Wüthrich RP, Bock A, Medication adherence assessment: High accuracy of the new Ingestible Sensor System in kidney transplants: Transplantation, 2013; 96(3); 245-50
93. Dukes CK, Sheaffer EA, Biosensing technology to track adherence: A literature review: Healthcare (Basel), 2021; 9(10); 1339
94. Thompson D, Mackay T, Matthews M, Direct adherence measurement using an ingestible sensor compared with self-reporting in high-risk cardiovascular disease patients who knew they were being measured: A prospective intervention [published correction appears in JMIR Mhealth Uhealth 2018; 6(4): e13]: JMIR Mhealth Uhealth, 2017; 5(6); e76
95. Hafezi H, Robertson TL, Moon GD, Au-Yeung KY, An ingestible sensor for measuring medication adherence: IEEE Trans Biomed Eng, 2015; 62(1); 99-109
96. Kalpouzos I, Giokas K, Koutsouris DD, A survey on an ingestible sensor for evaluating medication adherence in elderly people; 1-4, New York, NY, USA, Association for Computing Machinery (ACM)
97. Al-Hassany L, Kloosterboer SM, Dierckx B, Koch BC, Assessing methods of measuring medication adherence in chronically ill children – a narrative review: Patient Prefer Adherence, 2019; 13; 1175-89
98. Ford N, Nachega JB, Engel ME, Mills EJ, Directly observed antiretroviral therapy: A systematic review and meta-analysis of randomised clinical trials: Lancet, 2009; 374(9707); 2064-71
Figures
Figure 1. Main reasons for patients’ non-adherence (according to [11–13]). The illustration was created using Canva Pro (Canva Pty Ltd).Figure 2. Classification of medication adherence measurement methods: Objective vs subjective, direct vs indirect. The illustration was created using Canva Pro (Canva Pty Ltd). Tables
Table 1. Summary of identified methods for measuring medication adherence.Table 2. List of questionnaires and scales for adherence measures and information on patient adherence determination.Table 3. Key attributes of an optimal medication adherence measurement tool.Table 4. Conclusions drawn from the literature review on selected methods for assessing patients’ medication adherence.Table 1. Summary of identified methods for measuring medication adherence.Table 2. List of questionnaires and scales for adherence measures and information on patient adherence determination.Table 3. Key attributes of an optimal medication adherence measurement tool.Table 4. Conclusions drawn from the literature review on selected methods for assessing patients’ medication adherence. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387