11 July 2024: Clinical Research
Impact of BrainLab VectorVision Infrared-Based Neuronavigation on Surgical Outcomes in Intracranial Meningioma Patients: A Retrospective Study
Fatih Tomakin1ABCDEF, Recai Engin2ACEF*, Hasan Şener3BDF, Gürkan Gökalp3ABCDEF, Cengiz Çokluk3AEFDOI: 10.12659/MSM.944724
Med Sci Monit 2024; 30:e944724






Abstract
BACKGROUND: The BrainLab VectorVision neuronavigation system is an image-guided, frameless localization system used intraoperatively, which includes a computer workstation for viewing and analyzing operative microscopic images. This retrospective study aimed to evaluate the use of the BrainLab VectorVision infrared-based neuronavigation imaging system in 80 patients with intracranial meningioma removed surgically between 2013 and 2023.
MATERIAL AND METHODS: Data were retrospectively collected from 36 patients with convexity meningioma and 44 patients with parasagittal meningioma between 2013 and 2023. The surgical operation of 40 of these patients was performed with the help of neuronavigation, while the other 40 were performed without neuronavigation. Demographic data, preoperative and postoperative radiologic images, craniotomy measurements, surgical complications, and operative times of patients with and without neuronavigation were analyzed.
RESULTS: Using neuronavigation significantly increased surgery duration (P=0.023). In 6 patients without the use of neuronavigation, the craniotomy had to be enlarged and this resulted in superior sagittal sinus (SSS) damage (P=0.77, P=0.107). Patients for whom neuronavigation was used did not experience any sinus damage and did not require craniotomy enlargement. Postoperative epidural hematoma (EH) developed in 9 patients without navigation, whereas it developed in only 1 patient with navigation (P=0.104). Residual tumors were less common in patients using navigation (P=0.237).
CONCLUSIONS: The use of neuronavigation allows the incision and craniotomy to be reduced in size. Intraoperatively, it allows the surgeon to master the boundaries of the tumor and surrounding vascular structures, reducing the risk of complications. These results suggest that neuronavigation systems are an effective ancillary in meningioma surgery.
Keywords: Surgical Navigation Systems, Meningioma, Craniotomy, Humans, Neuronavigation, Female, Male, Retrospective Studies, Middle Aged, Meningeal Neoplasms, adult, Aged, Treatment Outcome, Surgery, Computer-Assisted, Neurosurgical Procedures, Postoperative Complications
Introduction
Meningiomas originate from arachnoid cap cells located on the inner surface of the dura mater [1]. Most meningiomas are benign tumors and are frequently diagnosed incidentally [2]. They can occur anywhere in the central nervous system [3]. The most common intracranial locations are in the cerebral convexity and parasagittal region. Occasionally, they occur outside the central nervous system [4].
Meningiomas are more common in adults than in children, with a prevalence of 37.75 per 100 000. Contrast-enhanced brain magnetic resonance imaging (MRI) is the most commonly used radiological method in the diagnosis of meningioma. Homogenous contrast uptake, regular border, and presence of a dural tail are the most prominent radiological features [5]. The main approach in the treatment of meningiomas is surgery, which is the most effective method for achieving long-term survival, particularly in cases of low-grade meningiomas [6,7]. Surgical complications include venous injury, hematoma, infection, and cerebrospinal fluid (CSF) leakage. Injury to the SSS is an important complication, particularly during parasagittal meningioma resection [3,6].
The surgeon’s experience and the tumor’s vascularization are the most important parameters for achieving gross total resection. Neuronavigation is a device neurosurgeons use to achieve gross total resection of tumors and prevent complications [3,8]. This provides an advantage, particularly in terms of protecting neurovascular structures. It shortens surgery duration by making smaller incisions and craniotomies, with precise localization of the tumor. This also reduces blood loss and increases the surgeon’s confidence [2,7].
The BrainLab VectorVision system is a neuronavigation system that links a freehand probe, tracked by passive sensors, to preoperative images of the patient into a virtual computer image space. Infrared flashes emitted by 2 cameras are reflected by passive marker spheres mounted near the patient’s head and on surgical instruments. The software can calculate the position of a sphere in three-dimensional space using data from both cameras, thus determining the position of the entire instrument [9].
The objective of this study was to examine the efficacy of neuronavigation systems in the surgical treatment of parasagittal and convexity meningiomas.
Material and Methods
ETHICS:
Ethics approval was granted by the local Medical Research Ethics Committee of Ondokuz Mayıs University Clinical Research (Decision no: 2023/373). Written informed consent was obtained from all participants. The data was then collated and analyzed centrally at Ondokuz Mayıs University.
INCLUSION CRITERIA:
This retrospective study analyzed data from 80 patients who underwent surgical treatment for meningioma between 2013 and 2023. The study evaluated the pathology results of patients aged 14–72 years with meningiomas located in the parasagittal and convexity regions, based on the World Health Organization’s (WHO) 2021 Classification of Central Nervous System Tumors. Only patients who underwent preoperative and postoperative contrast-enhanced brain MRI were included.
DATA COLLECTION:
We examined the location of the tumor (parasagittal convexity) and the length and width measurements of the area affected by the tumor on the dura mater. Demographic data, including sex and age, were collected. Complications were recorded in the surgery reports. These complications included instances in which the location of the tumor could not be identified, thereby leading to enlargement of the initial craniotomy and injuries to the SSS. We evaluated cases of an epidural hematoma thicker than 5 mm and the level of epidural hematoma in brain computed tomography (CT) images taken as part of routine postoperative assessment within the first 2 h. Brain MRIs are not routinely conducted within the first 48 h in cases that required total excision, as surgical borders of meningiomas become evident during surgery. Residual evaluation was based on postoperative brain CT images. If the 6-month brain MRI images showed increased residue compared to the postoperative CT scan, it was considered as recurrence. The follow-up period was 6 months.
The surgery report analyzed data on tumor resection, including gross total resection, partial resection, and biopsy, as well as dura and bone excision. The patients were classified using the Simpson classification system. Although different surgeons operated on the patients, they all followed the same surgical protocol using microsurgery. Nevertheless, the retrospective nature of the study and the fact that the operations were performed by different surgeons are limitations. MRI scans for neuronavigation were acquired with a 1.5 Tesla (T) magnet device (Intera; Philips Medical Systems, Best, The Netherlands), with a slice thickness of 1 mm. The neuronavigation system used was the Brainlab infrared-based navigation system (Brainlab Kick; Brainlab AG, Feldkirchen, Germany).
STATISTICAL ANALYSIS:
Data are described as the mean standard deviation for numerical and frequency (percentage) for categorical variables. Nominal variables were compared with chi-square or Fisher’s exact test and the comparisons of the rate of change between 2 groups were tested with an independent sample
Results
DEMOGRAPHIC FINDINGS OF STUDY POPULATION:
Among the 80 patients evaluated in the study, 36 (45%) had convexity meningiomas and 44 (55%) had parasagittal meningiomas. Among patients with convexity meningiomas, 75% were female, while among those with parasagittal meningiomas, 65.9% were female. Although the mean age was higher in patients with parasagittal meningiomas than in patients with convexity meningiomas, there was no significant difference between the groups in terms of mean age (
TUMOR HISTOPATHOLOGICAL SUBTYPES:
Examining the histopathological subtypes of all cases revealed that 29 (36.3%) were atypical, 15 (18.8%) were meningothelial, 13 (16.3%) were transitional meningiomas, and 23 (28.8%) were other subtypes. Of all the cases, 43 (53.8%) were grade 1, 28 were grade 2, and 9 (11.3%) were grade 3 meningiomas. When comparing the distribution of histopathological subtypes between the groups, it was found that 33.3% of convexity meningiomas were atypical, 19.4% were meningothelial, 11.1% were transitional; moreover, 36.1% of parasagittal meningiomas were atypical, 20.5% were transitional, 18.2% were meningothelial, and 22.7% were other subtypes.
Results
The mean surgery duration for patients with convexity meningiomas was 207±36.6 min, while that for patients with parasagittal meningiomas was 214±72.6 min. Further, intraoperative craniotomy was enlarged in 6 cases (7.5%), and the development of postoperative EH was observed in 10 cases (12.5%). In addition, 11 patients (13.8%) had previously undergone meningioma surgeries.
When comparing postoperative residual tumors, patients with parasagittal meningiomas had a significantly higher postoperative residual rate (34.1%) than those with convexity meningiomas (5.6%) (
Although 15.4% of patients with neuronavigation and 9.3% of patients without neuronavigation had grade 3 tumors, there was no significant correlation between the use of neuronavigation and tumor grades (
This study found that the use of neuronavigation significantly increased the duration of surgery compared to that in cases in which neuronavigation was not used (
When the residual tumor status was compared according to tumor grade, although the residual rate was higher in patients with grade 3 tumors, the difference between groups was not significant (
Although no postoperative sinus injury was observed in any of the parasagittal meningioma patients for whom neuronavigation was used, the difference between neuronavigation use and sinus injury was not significant (
Discussion
Smaller craniotomies were made and complications such as postoperative neurological deficits and epidural hematoma were reduced in patients operated on using the navigation system. It was also found to help remove more tumors and reduce residual and recurrence rates.
Meningiomas are observed approximately twice as frequently in women as in men [7]. In our study, 30% of the patients were male and 70% were female, which is consistent with the literature.
Of all meningiomas, 80.5% were WHO grade 1, 17.7% were grade 2, and 1.7% were grade 3 [10]. Upon analyzing the pathological results of the patients in our study, we found high rates of grade 2 and grade 3 patients (34% and 11%, respectively).
Although the rates of postoperative neurological deficits (eg, loss of motor strength, dysphasia, and aphasia) were lower in patients in whom neuronavigation was utilized compared to those in whom navigation was not utilized, the difference was not statistically significant (
The patients who underwent surgery with neuronavigation had a significantly longer surgery duration (
Bir et al reported that the use of neuronavigation was decisive in achieving gross total resection in 517 patients with meningioma [4]. Nguyen et al reported that the Simpson I–II resection rate was 82.26% in cases in which neuronavigation was used for falx meningiomas [8]. In our study, Simpson I–II resection was performed in 84.6% of patients who underwent neuronavigation and in 72.2% of patients who did not, but the difference between groups was not statistically significant. We believe that this was due to the superficial localization of the tumors and the fact that most of them were grade 1 tumors. Figure 6 illustrates the use of neuronavigation.
Surgery for meningiomas involves the relatively simple removal of convexity meningiomas. However, parasagittal meningiomas are more difficult to remove completely due to their invasion of the superior sagittal sinus. Complete removal of a tumor may result in complications during and after surgery, such as venous bleeding and sinus thrombosis [3]. Our study found that the residual rate in convexity tumors was significantly lower than that in parasagittal tumors, which is related to sagittal sinus invasion. In addition, intraoperative sagittal sinus injury was observed in 6 patients with parasagittal meningiomas. Neuronavigation was not utilized in any of these cases. The absence of sagittal sinus injury in patients who underwent neuronavigation may be attributed to frequent intraoperative probe checks of vascular structures and tumor borders.
The major limitation of this study is its retrospective design, which caused many biases. The fact that the patients were operated on by different surgeons may also have causes bias. The relatively small number of patients and short follow-up period are other limitations of the present study.
Conclusions
Neuronavigation systems are frequently used in surgeries. With the use of neuronavigation, smaller craniotomies can be performed and total resection of the tumor can be performed more successfully, with better determination of tumor borders during surgery. As a result, postoperative complications, vascular injuries, and blood loss are reduced. Furthermore, intraoperative control increases surgical safety and improves outcomes.
Figures
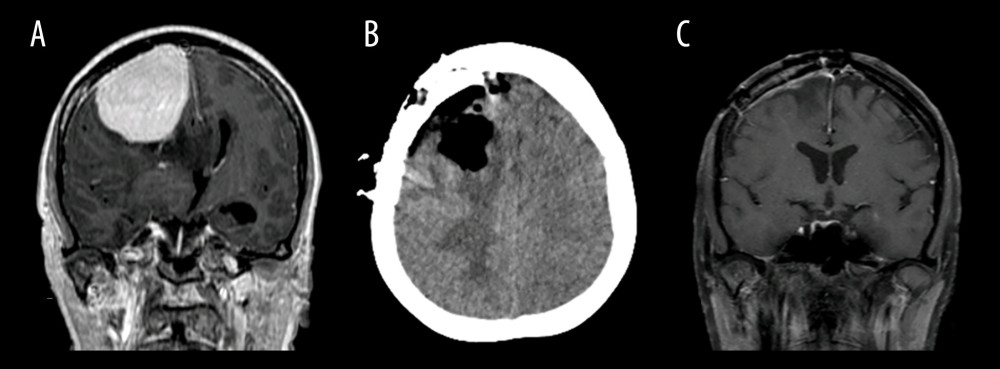 Figure 1. (A) The preoperative contrast-enhanced T1 coronal section brain magnetic resonance imaging (MRI) of a 42-year-old woman with parasagittal meningioma revealed a well-circumscribed mass measuring 7×6 cm with homogeneous contrast enhancement. (B) A cranial computed tomography (CT) image was taken one hour postoperatively and revealed gross total resection. (C) There was no recurrence in the six-month postoperative control contrast-enhanced brain MRI.
Figure 1. (A) The preoperative contrast-enhanced T1 coronal section brain magnetic resonance imaging (MRI) of a 42-year-old woman with parasagittal meningioma revealed a well-circumscribed mass measuring 7×6 cm with homogeneous contrast enhancement. (B) A cranial computed tomography (CT) image was taken one hour postoperatively and revealed gross total resection. (C) There was no recurrence in the six-month postoperative control contrast-enhanced brain MRI.  Figure 2. (A) The patient is a 46-year-old man. Preoperative contrast-enhanced T1 coronal section brain MRI revealed homogeneous contrast enhancement consistent with a 6×7 cm parasagittal meningioma invading the superior sagittal sinus. (B) A cranial CT image taken 1 h after surgery revealed a residual tumor in the area invading the superior sagittal sinus. (C) A postoperative six-month control contrast-enhanced MRI (after radiotherapy) showed no increase in the residual tumor.
Figure 2. (A) The patient is a 46-year-old man. Preoperative contrast-enhanced T1 coronal section brain MRI revealed homogeneous contrast enhancement consistent with a 6×7 cm parasagittal meningioma invading the superior sagittal sinus. (B) A cranial CT image taken 1 h after surgery revealed a residual tumor in the area invading the superior sagittal sinus. (C) A postoperative six-month control contrast-enhanced MRI (after radiotherapy) showed no increase in the residual tumor. 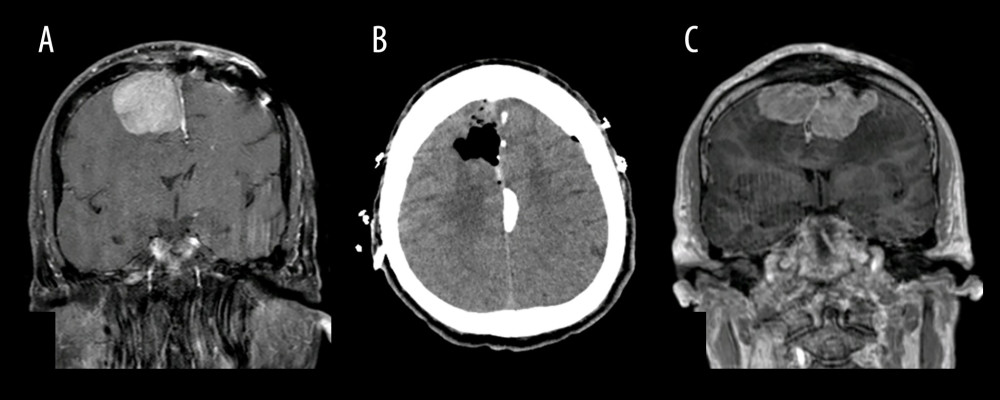 Figure 3. (A) The patient is a 67-year-old man who underwent an operation for a parasagittal meningioma located in the left hemisphere one year ago. The pathology report indicates an anaplastic meningioma (WHO grade 3). Preoperative contrast-enhanced T1 coronal section brain MRI reveals a recurrent meningioma measuring 6×8 cm in the left craniotomy area and right parasagittal area. (B) The first-hour postoperative cranial CT image reveals gross excision of the right parasagittal mass. (C) The 6-month postoperative control contrast-enhanced coronal section brain MRI reveals recurrent bilateral parasagittal meningioma invading the superior sagittal sinus.
Figure 3. (A) The patient is a 67-year-old man who underwent an operation for a parasagittal meningioma located in the left hemisphere one year ago. The pathology report indicates an anaplastic meningioma (WHO grade 3). Preoperative contrast-enhanced T1 coronal section brain MRI reveals a recurrent meningioma measuring 6×8 cm in the left craniotomy area and right parasagittal area. (B) The first-hour postoperative cranial CT image reveals gross excision of the right parasagittal mass. (C) The 6-month postoperative control contrast-enhanced coronal section brain MRI reveals recurrent bilateral parasagittal meningioma invading the superior sagittal sinus.  Figure 4. (A) Illustrative image of a patient undergoing a craniotomy. The craniotomy diameter is larger in the patient without neuronavigation. (B) In patients using neuronavigation, a smaller craniotomy can be performed because the tumor boundary can be clearly defined.
Figure 4. (A) Illustrative image of a patient undergoing a craniotomy. The craniotomy diameter is larger in the patient without neuronavigation. (B) In patients using neuronavigation, a smaller craniotomy can be performed because the tumor boundary can be clearly defined.  Figure 5. (A) Illustration of tumor removal with tumor forceps after dura excision. (B) Illustration of duraplasty with galeal graft after tumor resection. (C) Illustration of fixation of the cranioplasty cement to the skull.
Figure 5. (A) Illustration of tumor removal with tumor forceps after dura excision. (B) Illustration of duraplasty with galeal graft after tumor resection. (C) Illustration of fixation of the cranioplasty cement to the skull.  Figure 6. The process of determining tumor boundaries using neuronavigation in a craniotomized patient is illustrated.
Figure 6. The process of determining tumor boundaries using neuronavigation in a craniotomized patient is illustrated. Tables
Table 1. Comparison of demographic, pathological, intraoperative, and postoperative data of convexity and parasagittal meningiomas. Table 2. Comparison of the surgical patients in terms of postop epidural hematoma and motor deficit, Simpson grade of surgery, WHO grading, tumor residual and recurrence status.
Table 2. Comparison of the surgical patients in terms of postop epidural hematoma and motor deficit, Simpson grade of surgery, WHO grading, tumor residual and recurrence status. Table 3. Comparison of surgery duration with and without neuronavigation and tumor dural surface area/craniotomy size ratios in convexity and parasagittal meningiomas.
Table 3. Comparison of surgery duration with and without neuronavigation and tumor dural surface area/craniotomy size ratios in convexity and parasagittal meningiomas. Table 4. Association of residual tumor status with WHO grade in operated meningioma patients.
Table 4. Association of residual tumor status with WHO grade in operated meningioma patients. Table 5. The relationship between neuronavigation use and sinus injury in surgery for patients with parasagittal meningioma.
Table 5. The relationship between neuronavigation use and sinus injury in surgery for patients with parasagittal meningioma.
References
1. Bir SC, Konar SK, Maiti TK, Utility of neuronavigation in intracranial meningioma resection: A single-center retrospective study: World Neurosurg, 2016; 90; 546-555.e1
2. Ostrom QT, Gittleman H, Xu J, CBTRUS Statistical Report: Primary brain and other central nervous system tumors diagnosed in the United States in 2009–2013: Neuro Oncol, 2016; 18(Suppl 5); v1-v75
3. Sughrue ME, Rutkowski MJ, Shangari G, Results with judicious modern neurosurgical management of parasagittal and falcine meningiomas. Clinical article: J Neurosurg, 2011; 114(3); 731-37
4. Magill ST, Theodosopoulos PV, McDermott MW, Resection of falx and parasagittal meningioma: Complication avoidance: J Neurooncol, 2016; 130(2); 253-62
5. Alruwaili AA, De Jesus O, Meningioma: StatPearls [Internet], 2024, Treasure Island (FL), StatPearls Publishing [Updated 2023 Aug 23]
6. Chen CM, Huang AP, Kuo LT, Tu YK, Contemporary surgical outcome for skull base meningiomas: Neurosurg Rev, 2011; 34(3); 281-96 discussion 296
7. Dorward NL, Alberti O, Velani B, Postimaging brain distortion: Magnitude, correlates, and impact on neuronavigation: J Neurosurg, 1998; 88(4); 656-62
8. Buerki RA, Horbinski CM, Kruser T, An overview of meningiomas: Future Oncol, 2018; 14(21); 2161-77
9. Rogers L, Barani I, Chamberlain M, Meningiomas: Knowledge base, treatment outcomes, and uncertainties. A RANO review: J Neurosurg, 2015; 122(1); 4-23
10. Ostrom QT, Cioffi G, Gittleman H, CBTRUS Statistical Report: Primary brain and other central nervous system tumors diagnosed in the United States in 2012–2016: Neuro Oncol, 2019; 21(Suppl 5); v1-v100
11. Mezger U, Jendrewski C, Bartels M, Navigation in surgery: Langenbecks Arch Surg, 2013; 398(4); 501-14
12. Akyuz ME, Kadioglu HH, Application of neuronavigation system in intracranial meningioma surgery: A retrospective analysis of 75 cases: Cir Cir, 2022; 90(S2); 92-97
13. Ostrom QT, Price M, Neff C, CBTRUS Statistical Report: Primary brain and other central nervous system tumors diagnosed in the United States in 2015–2019: Neuro Oncol, 2022; 24(Suppl 5); v1-v95
Figures
Figure 1. (A) The preoperative contrast-enhanced T1 coronal section brain magnetic resonance imaging (MRI) of a 42-year-old woman with parasagittal meningioma revealed a well-circumscribed mass measuring 7×6 cm with homogeneous contrast enhancement. (B) A cranial computed tomography (CT) image was taken one hour postoperatively and revealed gross total resection. (C) There was no recurrence in the six-month postoperative control contrast-enhanced brain MRI.Figure 2. (A) The patient is a 46-year-old man. Preoperative contrast-enhanced T1 coronal section brain MRI revealed homogeneous contrast enhancement consistent with a 6×7 cm parasagittal meningioma invading the superior sagittal sinus. (B) A cranial CT image taken 1 h after surgery revealed a residual tumor in the area invading the superior sagittal sinus. (C) A postoperative six-month control contrast-enhanced MRI (after radiotherapy) showed no increase in the residual tumor.Figure 3. (A) The patient is a 67-year-old man who underwent an operation for a parasagittal meningioma located in the left hemisphere one year ago. The pathology report indicates an anaplastic meningioma (WHO grade 3). Preoperative contrast-enhanced T1 coronal section brain MRI reveals a recurrent meningioma measuring 6×8 cm in the left craniotomy area and right parasagittal area. (B) The first-hour postoperative cranial CT image reveals gross excision of the right parasagittal mass. (C) The 6-month postoperative control contrast-enhanced coronal section brain MRI reveals recurrent bilateral parasagittal meningioma invading the superior sagittal sinus.Figure 4. (A) Illustrative image of a patient undergoing a craniotomy. The craniotomy diameter is larger in the patient without neuronavigation. (B) In patients using neuronavigation, a smaller craniotomy can be performed because the tumor boundary can be clearly defined.Figure 5. (A) Illustration of tumor removal with tumor forceps after dura excision. (B) Illustration of duraplasty with galeal graft after tumor resection. (C) Illustration of fixation of the cranioplasty cement to the skull.Figure 6. The process of determining tumor boundaries using neuronavigation in a craniotomized patient is illustrated. Tables
Table 1. Comparison of demographic, pathological, intraoperative, and postoperative data of convexity and parasagittal meningiomas.Table 2. Comparison of the surgical patients in terms of postop epidural hematoma and motor deficit, Simpson grade of surgery, WHO grading, tumor residual and recurrence status.Table 3. Comparison of surgery duration with and without neuronavigation and tumor dural surface area/craniotomy size ratios in convexity and parasagittal meningiomas.Table 4. Association of residual tumor status with WHO grade in operated meningioma patients.Table 5. The relationship between neuronavigation use and sinus injury in surgery for patients with parasagittal meningioma.Table 1. Comparison of demographic, pathological, intraoperative, and postoperative data of convexity and parasagittal meningiomas.Table 2. Comparison of the surgical patients in terms of postop epidural hematoma and motor deficit, Simpson grade of surgery, WHO grading, tumor residual and recurrence status.Table 3. Comparison of surgery duration with and without neuronavigation and tumor dural surface area/craniotomy size ratios in convexity and parasagittal meningiomas.Table 4. Association of residual tumor status with WHO grade in operated meningioma patients.Table 5. The relationship between neuronavigation use and sinus injury in surgery for patients with parasagittal meningioma. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387