09 November 2024: Clinical Research
Comparative Analysis of Extended Curettage with Plate Fixation and Extended Curettage with Intramedullary Nail Fixation for Campanacci Grade II and International Society of Limb Salvage Zone H2 Giant Cell Tumors of the Proximal Femur: A Retrospective Study
Jiashi Song12345BCE, Kaipeng Jin1345DF, Bing Liu1345AG*DOI: 10.12659/MSM.945157
Med Sci Monit 2024; 30:e945157






Abstract
BACKGROUND: The objective of this study was to compare and evaluate the oncological and functional outcomes of 2 surgical treatments: extended curettage with plate fixation (EC-PF) and extended curettage with intramedullary nail fixation (EC-INF) for primary giant cell tumor (GCT) of the proximal femur.
MATERIAL AND METHODS: In a retrospective study, we reviewed 19 patients with Campanacci grade II and International Society of Limb Salvage zone H2 GCT of the proximal femur. All patients underwent either EC-PF (n=11) or EC-INF (n=8) surgery. The Mankin scoring system was used to evaluate the surgical effect, and the Musculoskeletal Tumor Society score was used to evaluate the limb salvage function of the patients. The between-group differences were analyzed at the end of follow-up.
RESULTS: During the follow-up period, there were no cases of recurrence or metastasis in both groups, and the EC-INF group had a higher rate of nononcological complications than the EC-PF group (62.5% vs 9.1%, respectively). Bone graft resorption and atrophy was the most frequent nononcological complication in the EC-INF group. According to the Mankin scoring system, the degree of hip joint function recovery in the EC-PF group was higher than that in the EC-INF group (P<0.05). Meanwhile, the EC-PF group had shorter hospital stays and higher Musculoskeletal Tumor Society scores (P<0.05).
CONCLUSIONS: Due to the high incidence of nononcological complications associated with intramedullary nailing as a method of internal fixation following extended curettage of the proximal femur GCT, this approach is generally not recommended.
Keywords: Giant Cell Tumor of Bone, Femoral Neck Fractures, Internal Fixators, Humans, Retrospective Studies, Male, Female, adult, Curettage, Fracture Fixation, Intramedullary, Femur, Middle Aged, Bone Plates, Limb Salvage, Treatment Outcome, Bone Neoplasms, Bone Nails, Femoral Neoplasms
Introduction
Giant cell tumor (GCT) of the bone accounts for approximately 4% to 10% of all primary bone tumors worldwide [1]. The incidence of primary GCT of the bone is about 20% in Southern India and China [2]. The female-to-male ratio is between 1.3 and 1.5 to 1, and the age of onset is around 25 to 50 years.
Among the reported cases, 44% are situated in the distal femur and proximal tibia, 10% in the distal radius, 6% in the proximal humerus, and 13% in the hands and feet [3]. GCT primarily affects the femoral neck and intertrochanteric region, with infrequent subtrochanteric involvement [4]. The International Society of Limb Salvage (ISOLS) classification divides the lesion site of the proximal femur into 3 zones [5]: the H1 area, located at the femoral head; H2 area, located between the head-neck junction and the distal plane of the lesser trochanter; and H3 area, located in the plane of the distal lesser trochanter to the distal femur. In 1987, Campanacci et al [6] proposed a grading system based on the manifestations of tumors on routine X-rays; the Campanacci grading system is the most commonly used clinical scoring system for GCTs of bone at present. Grade I lesions are limited to the bones, grade II lesions are those with cortical enlargement but no perforation, and grade III lesions are those with soft tissue extension and cortical perforation. GCT assessment includes a combination of laboratory and imaging studies, then biopsy for definite diagnosis. Although the ideal treatment of GCT is still controversial, surgical removal of the lesion is the mainstay of treatment. Current surgical treatments include extended curettage or segmental resection. En bloc resection, compared with extended curettage, is associated with a lower local recurrence rate; however, joint mobility and function can be impaired postoperatively [7]. Additionally, there is a higher risk of complications associated with en bloc resection, including infection and prosthetic loosening [8,9]. Furthermore, revision surgery might be needed due to the limited lifespan of the prosthesis. Although extended curettage allows joint preservation, it can induce secondary osteoarthritis, osteonecrosis, and higher risk of local recurrence [8]. At present, with multiple methods such as high-speed drilling, bone cement filling, and fibular graft support, as well as the application of denosumab in clinical practice, joint preservation surgery has become the main treatment for patients with GCT of the proximal femur. It is necessary to study the selection of different internal fixation methods after extended curettage in the treatment of the proximal femur GCT. In the past, intramedullary nails were often used for metastatic bone destruction and achieved good healing results. However, there are limited reports on the use of intramedullary nailing for this condition. Therefore, this retrospective study included 19 patients with primary GCT of the proximal femur and aimed to compare outcomes from 2 surgical methods: extended curettage with plate fixation (EC-PF) and extended curettage with intramedullary nail fixation (EC-INF).
Material and Methods
INCLUSION AND EXCLUSION CRITERIA:
The inclusion criteria of this retrospective study were as follows: (1) The patient had a diagnosis of Campanacci grade II and ISOLS zone H2 GCT of the proximal femur for the first time. (2) Patient underwent primary surgical operation at our center, and the surgical methods were either EC-PF or EC-INF. The pathological diagnosis was GCT of bone. (3) The patient was followed up for more than 24 months, with complete clinical information. The exclusion criteria were as follows: (1) There were other primary or secondary malignant GCTs of bone confirmed by histopathology. (2) The first treatment or the first operation was in another hospital. (3) Patients with follow-up time less than 24 months.
We obtained written informed consent from all patients. All patients were approved to participate in this study by the hospital Ethics Committee of our hospital. This manuscript was written according to the Strengthening the Reporting of Cohort Studies in Surgery (STROCSS) statement [10]. This study has been registered as an audit at our institution (ref No: IR2022240), and the published article can include any images or data that may be identifiable. This research was performed with the approval of an appropriate ethics committee and is in compliance with the Helsinki Declaration.
SURGICAL TECHNIQUE:
The Watson-Jones approach is usually chosen for extended curettage internal fixation surgery. A longitudinal anterolateral incision was made in the hip joint area, and each layer of the skin and subcutaneous tissue were then carefully peeled back. The gluteus medius muscle and tensor fasciae latae muscle were separated, and the proximal femur was dissected along the muscle gap to expose a portion of the vastus lateralis muscle at the distal end. The oval bone window was opened with a bone knife in the front, and the dark red tumor tissue, with rich blood supply, was seen in the tumor tissue. An appropriate amount of tumor tissue was then taken for frozen section examination during surgery. The tumor tissue was scraped and cauterized with a high frequency electric scalpel, the bone ridge was polished by a high speed grinding drill, and the residual tumor cells in the cavity wall were inactivated again with cotton balls soaked in phenol and absolute ethanol. A reliable filler was selected according to the operator’s experience. In this study, we selected a mixture of autologous iliac crest and allogeneic bone (allograft bone materials were provided by Beijing Xinkangchen Medical Technology Development Co, LTD; model: bone granules; code name: gl-dg\SD; specifications: 1.0–3.0 mm), and fibular graft. During the operation, the surgeon evaluated the degree of cortical bone and cross-sectional bone destruction according to the ISOLS classification, and selected dynamic hip screws (AO Corporation, USA), locking compression plates (AO Corporation, USA), or intramedullary nailing (Stryker Corporation, USA) for fixation. Finally, a drainage tube was placed, and the incision was sutured layer by layer.
FOLLOW-UP AND EVALUATION:
Patients were asked to return for follow-up at 1, 3, 6, 9, and 12 months after surgery, then every 6 months for the next year and finally once a year after that. To promote osteointegration, patients in both groups were restricted from putting any weight on the operated limb for 6 weeks after surgery. Additionally, during the follow-up period, patients were instructed in rehabilitation exercise by rehabilitation physicians. Postoperative imaging examination included X-rays of the operated hip. Patients with suspected recurrence were examined using computed tomography (CT) and magnetic resonance imaging (MRI) for further confirmation. Routine chest X-rays were conducted for lung metastasis assessment. Pulmonary CT examination was further conducted to monitor potential lung metastasis. Related complications, including infection, bone resorption atrophy, internal fixation loosening, secondary fractures, and tumor recurrence and metastasis, were recorded during follow-up. The Mankin scoring system [11] was used to evaluate the surgical effect, as follows: excellent: almost full functionality restored; good: mild to moderate functional limitations and ability to participate in limited physical activity; poor: needs crutches to walk, although can tolerate pain alone can not participate in sports; failure: complications require removal of the graft or amputation; or even death from local recurrence. We used the most recent follow-up records (follow-up time ≥2 years) to perform the Mankin scoring, and internal fixation loosening required revision surgery, amputation, and local recurrence as end events. The Musculoskeletal Tumor Society (MSTS) score [12,13], a scoring system that includes 6 items – pain, function, emotional acceptance, support, walking function, and gait – was used to evaluate the postoperative function of the patients. The scale has a total of 30 points, with a total of 5 points for each item. Total scores of 24–30 are excellent, 19–23 are good, 12–18 are medium, and less than 12 are poor. Follow-up records of patients with no recurrence were used as indicators to evaluate hip function, and the latest follow-up records of MSTS function score (follow-up time ≥2 years) were selected.
STATISTICAL ANALYSIS:
SPSS version 26 (IBM Corp, Armonk, NY, USA) was used for data analysis. Continuous data are expressed as means±standard deviation, and skewed data are presented as median (interquartile range) or n (%). The difference in means between the 2 groups was analyzed by the unpaired
Results
GENERAL CHARACTERISTICS:
A total of 19 patients with Campanacci grade II and ISOLS zone H2 GCT of the proximal femur were included in the study (Table 1), including 8 male and 11 female patients ranging in age from 16 to 51 years, with an average age of 30 years. All patients underwent either EC-PF or EC-INF surgery based on ISOLS and imaging classification. The remaining cavity was filled with autogenous bone and allograft bone. The mean follow-up time was 35.45 months (SD 8.01; 24–45) for the EC-PF group and 35.13 months (SD 6.29; 24–42) for the EC-INF group in this retrospective study. Baseline characteristics of the patients were statistically comparable between the 2 groups (Table 2).
COMPLICATIONS AND TUMOR RECURRENCES:
During the follow-up period, there were no recurrence or metastasis cases in both groups, and the EC-PF group had a higher rate of nononcological complications than the EC-INF group (9.1% vs 62.5%, respectively). There was 1 case of complications in the EC-PF group, with an incidence rate of 9.1%. The details were as follows (Figure 1): 1 patient developed an infection 7 months after surgery, and the pathological examination showed pyogenic stringency. The postoperative infection was well controlled after the second operation, which involved debridement, partial internal fixation removal, and antibiotic bone cement filling. In contrast, 5 cases of complications were observed in the EC-INF group, with an incidence rate of 62.5%. The details were as follows (Figure 2): bone graft atrophy occurred in 3 cases; and bone graft atrophy was accompanied by nonunion and internal fixation loosening in 2 cases. The average follow-up time of bone graft resorption atrophy was 18.2 months (12–30 months), and the time of bone graft resorption atrophy after autologous bone and allogeneic bone filling was about 1 to 2 years.
COMPARISON OF EFFICACY OF EC-PF AND EC-INF:
There were no statistically significant differences between the EC-PF group (11 patients) and the EC-INF group (8 patients) with respect to age, sex, Campanacci classification, lesion location, operation time, intraoperative blood loss, recurrence, metastasis, and the need for second operation (
Discussion
Our study involved 19 patients with GCT of the proximal femur who underwent extended curettage surgery. Patients were classified into 2 groups based on the fixation method used: EC-PF group vs EC-INF group. Our study revealed a significant difference in hospital stay, postoperative complications, MSTS functional score, and Mankin scores between the 2 groups. Compared with the EC-INF group, the EC-PF group had shorter hospital stay, fewer postoperative complications, and better joint function recovery. According to the Mankin scores, the excellent rate of the EC-PF group (90.9%) was higher than that of the EC-INF group (37.5%). The recovery degree of hip joint function in the EC-PF group was higher than that in the EC-INF group. There are several treatment options available for GCT of bone, such as surgery, radiotherapy, biological therapy, and selective vascular embolization. Surgical intervention is typically favored for GCT of the extremities; however, there is no universally accepted standard for surgical approaches [14]. Yuan et al [15] conducted a retrospective study of 29 patients to compare the differences in local recurrence, reconstruction durability, and postoperative function of proximal femur GCT treated with extended curettage or segectomy. Complications in the extended curettage group (osteoarthritis, osteonecrosis) were significantly less than those in the segectomy group (joint stiffness, infection, prosthesis loosening). There was no significant difference in tumor recurrence and metastasis between the extended curettage and segectomy groups, a finding consistent with the results of the present study. This may be related to the use of high-speed grinding drill during the operation. In recent years, advancements in science and technology have highlighted the importance of surgical treatment for GCT of the proximal femur, which prioritizes joint preservation surgery and enables prompt restoration of limb function. Yan et al [16] conducted an analysis of individualized treatment and clinical outcomes of 281 patients with GCT of the long bones of limbs, and summarized a set of treatment plans for GCT of the limbs. Based on their findings, for patients with approximately 25% to 50% cortical bone destruction, 25% to 50% articular surface destruction, and cross section bone destruction of >50%, extended curettage combined with internal fixation/external fixation should be adopted. Terakawa et al [17] retrospectively reviewed 82 patients with metastatic bone tumors of the proximal femur who underwent intramedullary nail fixation in a single hospital from 2007 to 2020. They measured the distance from the center of femoral head to the proximal (x) and distal (y) end of the of tumor and found that intramedullary nails were preferred when the distance from the center of femoral head to the proximal end of the tumor was ≥15 mm. The results of a study in 2021 showed that there is an extremely low likelihood of developing distal femoral metastases when isolated proximal femoral metastases are present [18]. Arpornsuksant et al [19] conducted a study to investigate the factors related to the progression of local metastases after intramedullary nail stabilization. Their analysis suggests that the risk of experiencing local progression of tumor growth and reoperations after intramedullary nail stabilization is low.
In the present study, the EC-PF group had a higher rate of nononcological complications than did the EC-INF group (9.1% vs 62.5%, respectively). Bone graft resorption and atrophy was the most frequent nononcological complication in the EC-INF group. Several reasons were mentioned in our article to explain why patients in the intramedullary nailing group had higher incidence of complications. One possible reason is that the expansion of the bone marrow cavity and the implantation of intramedullary nailing can destroy a portion of the blood supply of the proximal femur, which may not be conducive to bone graft healing and can lead to the absorption and atrophy of the bone graft. Another reason could be that screw withdrawal can still occur due to the thinning and weakening of the posterior femoral cortical bone caused by tumor invasion, as well as from the potential damage from the use of a high-speed grinding drill during surgery. When the internal fixation is loose, the stress of the screw blade of the intramedullary nail is increased, and the femoral head and neck of the femur are at higher risk of damage when the patient walks. To minimize the pain and discomfort caused by the stimulation of the surrounding soft tissue by the end of the helical blade through the lateral femoral cortex, Cheung and Chan recommended a distance of about 2 to 3 mm between the tail of the helical blade and the femoral cortex [20]. As a result of internal fixation loosening and bone absorption and atrophy, the main nail in some patients who underwent EC-INF surgery shifted away from the center of the medullary cavity. Such displacement caused the tail end of the helical blade to come close to the femoral cortex when the lower limb was loaded, which might cause lower limb pain.
Autologous or allogeneic bone graft is widely used to fill the bone defect after intra-focal curettage of various bone diseases and can promote healing and reduce the incidence of fracture [21–24]. Kivioja et al [25] conducted a multicenter study of 294 patients with GCT to investigate the factors associated with the risk of local recurrence after intra-lesional curettage. They showed that the method of filling the resultant defect highly favored the use of cement. Vaishya et al [26] systematically compared the efficacy and recurrence rate of bone cement and bone graft to fill the bone defect after the intra-lesional curettage of a GCT. According to their review, the use of bone graft was associated with a significantly higher rate of recurrence (risk ratio 1.9). Studies have shown that the risk of fractures after bone cement filling is significantly higher than that of bone grafting [27,28]. In some cases, cross-screws or Kirschner wires have been implanted into bone cement to reduce the incidence of fractures [29–31]. Greenberg et al investigated the effectiveness of adding zoledronic acid to bone cement in enhancing the tumor inactivation cytotoxic effect of zoledronic acid [32]. Following a follow-up period of 1 to 12 years, this study showed that bisphosphonate bone cement may reduce the recurrence rate of giant bone cells if patients can tolerate the systemic adverse effects of zoledronic acid [33]. Jamshidi et al [27] conducted a retrospective study in 2022 that involved 26 patients with a GCT bone defect in the proximal femur. The patients were divided into 2 groups: the allograft fibular support group (n=12) and the bone cement filling group (n=14). The average follow-up time was 116 months in the fibular support group and 113 months in the bone cement group. The results showed that there was no significant difference in the recurrence rate between the 2 groups. However, the incidence of non-neoplastic complications, such as degenerative joint disease, fracture, varus deformity, and nonunion, was significantly lower in the fibular butted graft group (16.7%) than in the cement group (42.8%). Moreover, patients in the fibular butted graft group had a higher MSTS score (92.4%) than the cement group (74.2%). These findings suggest that fibular bone grafts can be effective for the treatment of large bone defects and hold clinical application value. The mean follow-up time was 35.45 months for the EC-PF group and 35.13 months for the EC-INF group in the present retrospective study. Our study showed that the time of bone graft resorption atrophy after autologous bone and allogeneic bone filling was about 1 to 2 years. Therefore, it is more meaningful for MSTS functional scores to be followed up for more than 2 years. According to the MSTS score results of different internal fixation methods (Table 3), for patients who have been evaluated and need to save the joint, it is recommended to choose the appropriate internal fixation according to the ISOLS classification (Table 4).
Although GCT is often regarded as a benign tumor, it can sometimes be aggressive. The World Health Organization defines it as an intermediate bone tumor with local invasion. About 1% to 4% of patients will develop distant metastases, predominantly in the lung [34]. About 75% of metastases occurred within 2 years, and the other 25% occurred within 5 years [25,35]. Since metastatic lesions do not cause death in patients, they are referred to as “benign” lung metastases [36–39]. CT is generally recommended to evaluate pulmonary metastases, according to the National Comprehensive Cancer Network guidelines. Pulmonary metastases are generally benign, and a few of them can be self-healing [36,40,41]. Chest CT is closely monitored to determine tumor progression and complications. Surgery is appropriate for patients who may have tumor-related symptoms. Patients with GCT who have undergone surgical management typically have a good prognosis [37] and a low risk of postoperative complications [35,42]. For patients with recurrent GCT or those who are not suitable for surgery, due to its anatomical position, the use of low-dose whole lung radiotherapy [37,43] or denosumab treatment [44–48] is recommended. During the follow-up period, there were no cases of recurrence or metastasis in both groups of the present retrospective study. Despite the short follow-up time, all cases were Campanacci grade II. Studies have shown a high incidence of lung metastasis in spinal GCT [39]. Jiang et al [49] conducted a multicenter retrospective study from 4 hospitals in southern China, collecting relevant information from 140 patients with GCT of the extremities, and found that the distal femur was the most common site for lung metastasis, followed by the distal radius. Risk factors for lung metastasis in GCT include local recurrence, young patients (mean age 25 years), Enneking type III, and spinal lesions [50]. Multiple retrospective case series have shown that the local recurrence rate in patients treated with extended curettage and adjuvant therapy is 13% to 22% [25,51], which is significantly lower than that of extended curettage alone. At present, the high-speed grinding drill has been increasingly used in the surgery of proximal femoral GCT [7,52], as it is capable of excising residual malignancy in the bone ridge by expanding the resection scope and killing tumor tissue via high temperature during high-speed rotation. Desosumab was approved in the United States in 2013 for patients with GCT who are ineligible for surgical removal or who are at risk of serious complications, such as amputation or joint removal following surgery. Given the benefits of denosumab therapy and advancement in surgical techniques for proximal femoral reconstruction [53–55], joint preservation, particularly in young patients, has become more of a priority. Therefore, while hip arthroplasty is considered one of the best types of surgical management for recurrent GCT, its used should be carefully considered in this particular group of patients.
This single-center retrospective analysis had some limitations. (1) This study raises concerns about the relatively short follow-up period, which can result in an underestimation of events, such as tumor metastasis and recurrence. (2) The relatively small sample size of this study was mainly due to the low incidence of GCT of bone at the proximal femur, which can affect the reliability and strength of the findings. (3) This study was a single-center study, and the results need to be further verified by a multicenter study.
Conclusions
In conclusion, patients with GCT of the proximal femur who underwent extended curettage combined with adjuvant therapy had higher local control rates. However, the incidence of bone resorption atrophy and internal fixation loosening was higher for patients who underwent EC-INF surgery, which significantly affected the functional recovery of the affected limb. Furthermore, patients who underwent EC-PF surgery had a shorter hospital stay and fewer postoperative complications than did those who underwent EC-INF surgery. Selecting appropriate internal fixation methods according to the ISOLS classification can assist patients in achieving optimal joint function recovery and attaining favorable healing outcomes.
Figures
 Figure 1. (A) A 20-year-old male patient with a lesion in the right proximal femur showed osteolytic and dilatant changes. (B) X-ray examination taken 7 months after curettage surgery using plate internal fixation showed changes on the right proximal femur accompanied by partial bone destruction. (C) Postoperative pathological diagnosis: suppurative inflammation of the right proximal femur, infection considered. For the second operation, partial cement and internal fixation plate removal were performed in this patient. (D) The X-ray film was reexamined at 3 months after reoperation.
Figure 1. (A) A 20-year-old male patient with a lesion in the right proximal femur showed osteolytic and dilatant changes. (B) X-ray examination taken 7 months after curettage surgery using plate internal fixation showed changes on the right proximal femur accompanied by partial bone destruction. (C) Postoperative pathological diagnosis: suppurative inflammation of the right proximal femur, infection considered. For the second operation, partial cement and internal fixation plate removal were performed in this patient. (D) The X-ray film was reexamined at 3 months after reoperation.  Figure 2. (A–E) Preoperative and postoperative manifestations of EC-INF for proximal femur GCT in 2 patients. (C) In 1 patient, postoperative imaging examination of the proximal femur showed bone resorption and atrophy at 9 months. (F) In another patient, nonunion accompanied with intramedullary nail loosening was observed 12 months after operation.
Figure 2. (A–E) Preoperative and postoperative manifestations of EC-INF for proximal femur GCT in 2 patients. (C) In 1 patient, postoperative imaging examination of the proximal femur showed bone resorption and atrophy at 9 months. (F) In another patient, nonunion accompanied with intramedullary nail loosening was observed 12 months after operation. Tables
Table 1. Clinical data of 19 patients included in this study. Table 2. Data statistics and analysis of extended curettage with plate fixation (EC-PF) group and extended curettage with intramedullary nail fixation (EC-INF) group.
Table 2. Data statistics and analysis of extended curettage with plate fixation (EC-PF) group and extended curettage with intramedullary nail fixation (EC-INF) group.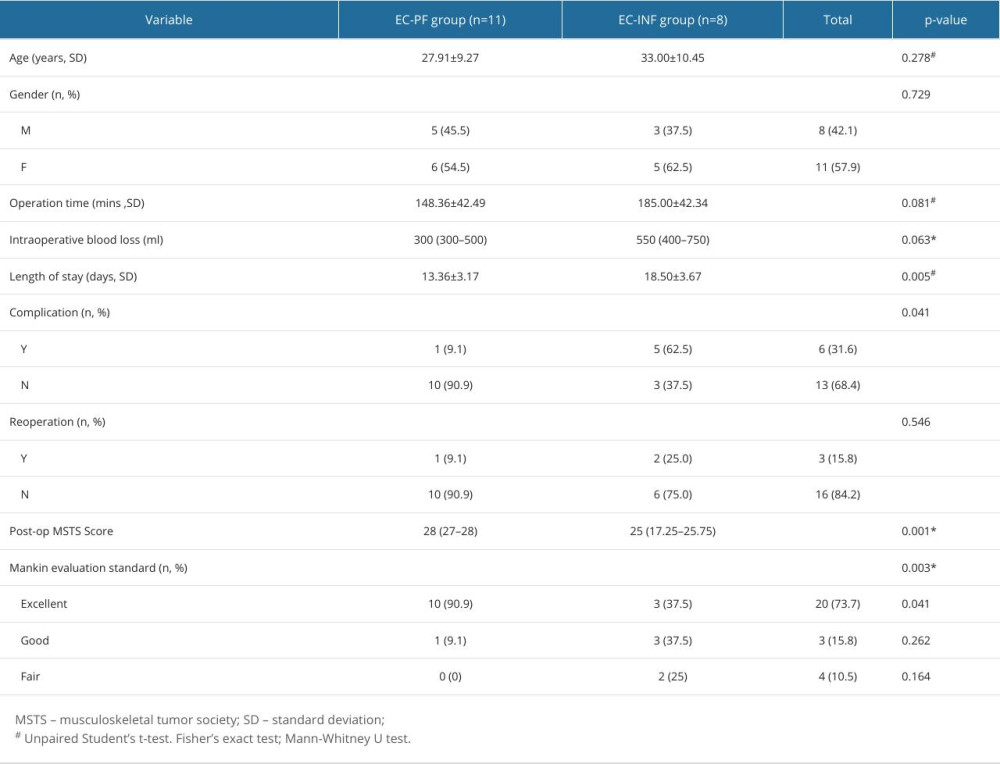 Table 3. The Musculoskeletal Tumor Society score results of different internal fixation methods in 19 patients with proximal femoral giant cell tumor.
Table 3. The Musculoskeletal Tumor Society score results of different internal fixation methods in 19 patients with proximal femoral giant cell tumor. Table 4. The appropriate internal fixation according to the International Society of Limb Salvage classification.
Table 4. The appropriate internal fixation according to the International Society of Limb Salvage classification.
References
1. Hosseinzadeh S, Tiwari V, De Jesus O, Giant cell tumor (osteoclastoma) [Updated 2024 Jan 31]: StatPearls [Internet], 2024, Treasure Island (FL), StatPearls Publishing Available from:https://www.ncbi.nlm.nih.gov/books/NBK559229/
2. Jha Y, Chaudhary K, Giant cell tumour of bone: A comprehensive review of pathogenesis, diagnosis, and treatment: Cureus, 2023; 15(10); e46945
3. Mavrogenis AF, Igoumenou VG, Megaloikonomos PD, Giant cell tumor of bone revisited: SICOT J, 2017; 3; 54
4. Wijsbek AE, Vazquez-Garcia BL, Grimer RJ, Giant cell tumour of the proximal femur: Is joint-sparing management ever successful?: Bone Joint J, 2014; 96-B(1); 127-31
5. Jones CW, Shatrov J, Jagiello JM, Clinical, functional and radiological outcomes of extracorporeal irradiation in limb salvage surgery for bone tumours: Bone Joint J, 2017; 99-B(12); 1681-88
6. Campanacci M, Baldini N, Boriani S, Giant cell tumor of bone: J Bone Joint Surg Am, 1987; 69(1); 106-14
7. Yu X, Xu M, Xu S, Clinical outcomes of giant cell tumor of bone treated with bone cement filling and internal fixation, and oral bisphosphonates: Oncol Lett, 2013; 5(2); 447-51
8. Şirin E, Akgülle AH, Topkar OM, Mid-term results of intralesional extended curettage, cauterization, and polymethylmethacrylate cementation in the treatment of giant cell tumor of bone: A retrospective case series: Acta Orthop Traumatol Turc, 2020; 54(5); 524-29
9. Bai WZ, Guo SB, Zhao W, Comparison of outcomes of 2 surgical treatments for proximal humerus giant cell tumors: A multicenter retrospective study: J Shoulder Elbow Surg, 2019; 28(11); 2103-12
10. Agha R, Abdall-Razak A, Crossley ESTROCSS Group, STROCSS 2019 Guideline: Strengthening the reporting of cohort studies in surgery: Int J Surg, 2019; 72; 156-65
11. Mankin HJ, Gebhardt MC, Jennings LC, Long-term results of allograft replacement in the management of bone tumors: Clin Orthop Relat Res, 1996(324); 86-97
12. Enneking WF, Dunham W, Gebhardt MC, A system for the functional evaluation of reconstructive procedures after surgical treatment of tumors of the musculoskeletal system: Clin Orthop Relat Res, 1993(286); 241-46
13. Tan PK, Tan MH, Functional outcome study of mega-endoprosthetic reconstruction in limbs with bone tumour surgery: Ann Acad Med Singap, 2009; 38(3); 192-96
14. Montgomery C, Couch C, Emory CL, Giant cell tumor of bone: Review of current literature, evaluation, and treatment options: J Knee Surg, 2019; 32(4); 331-36
15. Yuan Y, Liu Q, Liu Y, Comparative analysis of two surgical treatment options for giant cell tumor of the proximal femur: Extended curettage and segmental resection: Front Oncol, 2021; 11; 771863
16. Yan X, Lin N, Huang XIndividualized treatment and single center analysis of 281 cases of giant cell tumor of limb: Chinese Journal of Orthopedics, 2018; 38(18); 1117-25 [in Chinese]
17. Terakawa F, Kamoda H, Yonemoto T, Analysis of implants for metastatic bone tumors of the proximal femur: A retrospective study: Asia Pac J Clin Oncol, 2023; 19(5); e320-25
18. Boden AL, Patel M, Hoyt A, Development of distal femoral metastasis is rare in cases of isolated proximal femoral metastases: J Am Acad Orthop Surg, 2021; 29(9); e465-70
19. Arpornsuksant P, Morris CD, Forsberg JA, What factors are associated with local metastatic lesion progression after intramedullary nail stabilization?: Clin Orthop Relat Res, 2022; 480(5); 932-45
20. Cheung JP, Chan CF, Cutout of proximal femoral nail antirotation resulting from blocking of the gliding mechanism during fracture collapse: J Orthop Trauma, 2011; 25(6); e51-55
21. Jamshidi K, Mirkazemi M, Izanloo A, Locking plate and fibular strut graft augmentation in the reconstruction of unicameral bone cyst of proximal femur in the paediatric population: Int Orthop, 2018; 42(1); 169-74
22. Mostafa MF, Fawzy SI, Fibular strut graft for humeral aneurysmal bone cyst with varus deformity: Int Orthop, 2015; 39(7); 1391-98
23. Bryant D, Grant RE, Tang D, Fibular strut grafting for fibrous dysplasia of the femoral neck: J Natl Med Assoc, 1992; 84(10); 893-97
24. Yadav SS, The use of a free fibular strut as a “biological intramedullary nail” for the treatment of complex nonunion of long bones: JB JS Open Access, 2018; 3(2); e0050
25. Kivioja AH, Blomqvist C, Hietaniemi K, Cement is recommended in intralesional surgery of giant cell tumors: A Scandinavian Sarcoma Group study of 294 patients followed for a median time of 5 years: Acta Orthop, 2008; 79(1); 86-93
26. Vaishya R, Pokhrel A, Agarwal AK, Current status of bone cementing and bone grafting for giant cell tumour of bone: A systemic review: Ann R Coll Surg Engl, 2019; 101(2); 79-85
27. Jamshidi K, Bagherifard A, Mohaghegh MR, Fibular strut allograft or bone cement for reconstruction after curettage of a giant cell tumour of the proximal femur: A retrospective cohort study: Bone Joint J, 2022; 104-B(2); 297-301
28. Pattijn V, Samson I, Vander Sloten J, Medical image based, preformed titanium membranes for bone reconstructions: Design study and first clinical: Proc Inst Mech Eng H, 2002; 216(1); 13-21
29. Toy PC, France J, Randall RL, Reconstruction of noncontained distal femoral defects with polymethylmethacrylate and crossed-screw augmentation: A biomechanical study: J Bone Joint Surg Am, 2006; 88(1); 171-78
30. Murray PJ, Damron TA, Green JK, Contained femoral defects: Biomechanical analysis of pin augmentation in cement: Clin Orthop Relat Res, 2004; 420; 251-56
31. Randall RL, Weenig KN, West JR, Durability and strength of Steinmann pin augmentation in cemented tibial defects: Clin Orthop Relat Res, 2002(397); 306-14
32. Zwolak P, Manivel JC, Jasinski P, Cytotoxic effect of zoledronic acid-loaded bone cement on giant cell tumor, multiple myeloma, and renal cell carcinoma cell lines: J Bone Joint Surg Am, 2010; 92(1); 162-68
33. Greenberg DD, Lee FY, Bisphosphonate-loaded bone cement as a local adjuvant therapy for giant cell tumor of bone: A 1 to 12-year follow-up Study: Am J Clin Oncol, 2019; 42(3); 231-37
34. He X, Zhang HL, Hu YC, Limb Salvage by distraction osteogenesis for distal tibial osteosarcoma in a young child: a case report: Orthop Surg, 2016; 8(2); 253-56
35. Balke M, Ahrens H, Streitbuerger A, Treatment options for recurrent giant cell tumors of bone: J Cancer Res Clin Oncol, 2009; 135(1); 149-58
36. Dominkus M, Ruggieri P, Bertoni F, Histologically verified lung metastases in benign giant cell tumours – 14 cases from a single institution: Int Orthop, 2006; 30(6); 499-504
37. Viswanathan S, Jambhekar NA, Metastatic giant cell tumor of bone: Are there associated factors and best treatment modalities?: Clin Orthop Relat Res, 2010; 468(3); 827-33
38. Yang Y, Huang Z, Niu X, Clinical characteristics and risk factors analysis of lung metastasis of benign giant cell tumor of bone: J Bone Oncol, 2017; 7; 23-28
39. Donthineni R, Boriani L, Ofluoglu O, Metastatic behaviour of giant cell tumour of the spine: Int Orthop, 2009; 33(2); 497-501
40. Siebenrock KA, Unni KK, Rock MG, Giant-cell tumour of bone metastasising to the lungs. A long-term follow-up: J Bone Joint Surg Br, 1998; 80(1); 43-47
41. Kay RM, Eckardt JJ, Seeger LL, Pulmonary metastasis of benign giant cell tumor of bone. Six histologically confirmed cases, including one of spontaneous regression: Clin Orthop Relat Res, 1994(302); 219-30
42. von Steyern FV, Kristiansson I, Jonsson K, Giant-cell tumour of the knee: the condition of the cartilage after treatment by curettage and cementing: J Bone Joint Surg Br, 2007; 89(3); 361-65
43. Faisham WI, Zulmi W, Halim AS, Aggressive giant cell tumour of bone: Singapore Med J, 2006; 47(8); 679-83
44. Feigenberg SJ, Marcus RB, Zlotecki RA, Whole-lung radiotherapy for giant cell tumors of bone with pulmonary metastases: Clin Orthop Relat Res, 2002(401); 202-8
45. Palmerini E, Chawla NS, Ferrari S, Denosumab in advanced/unresectable giant-cell tumour of bone (GCTB): For how long?: Eur J Cancer, 2017; 76; 118-24
46. Thomas D, Henshaw R, Skubitz K, Denosumab in patients with giant-cell tumour of bone: An open-label, phase 2 study: Lancet Oncol, 2010; 11(3); 275-80
47. Ueda T, Morioka H, Nishida Y, Objective tumor response to denosumab in patients with giant cell tumor of bone: A multicenter phase II trial: Ann Oncol, 2015; 26(10); 2149-54
48. Chawla S, Blay JY, Rutkowski P, Denosumab in patients with giant-cell tumour of bone: A multicentre, open-label, phase 2 study: Lancet Oncol, 2019; 20(12); 1719-29
49. Jiang N, Qin CH, Tan CX, A retrospective analysis of 140 patients with giant cell tumor in the extremity: A multicenter study based on four hospitals in South China: Cancer Epidemiol, 2013; 37(3); 294-99
50. Chan CM, Adler Z, Reith JD, Risk factors for pulmonary metastases from giant cell tumor of bone: J Bone Joint Surg Am, 2015; 97(5); 420-28
51. Wang HC, Chien SH, Lin GT, Management of grade III giant cell tumors of bones: J Surg, 2005; 92; 46
52. Algawahmed H, Oncol Turcotte R, Farrokhyar F, High-speed burring with and without the use of surgical adjuvants in the intralesional management of giant cell tumor of bone: A systematic review and meta-analysis: Sarcoma, 2010; 2010; 586090
53. Sakayama K, Sugawara Y, Kidani T, Diagnostic and therapeutic problems of giant cell tumor in the proximal femur: Arch Orthop Trauma Surg, 2007; 127; 867-72
54. Wai EK, Davis AM, Griffin A, Pathologic fractures of the proximal femur secondary to benign bone tumors: Clin Orthop Relat Res, 2001(393); 279-86
55. Irwin RB, Sauchak JA, O’Brien MP, Tumors of the proximal femur: Case examples and literature review: Orthopedics, 1998; 21(2); 182-89
Figures
Figure 1. (A) A 20-year-old male patient with a lesion in the right proximal femur showed osteolytic and dilatant changes. (B) X-ray examination taken 7 months after curettage surgery using plate internal fixation showed changes on the right proximal femur accompanied by partial bone destruction. (C) Postoperative pathological diagnosis: suppurative inflammation of the right proximal femur, infection considered. For the second operation, partial cement and internal fixation plate removal were performed in this patient. (D) The X-ray film was reexamined at 3 months after reoperation.Figure 2. (A–E) Preoperative and postoperative manifestations of EC-INF for proximal femur GCT in 2 patients. (C) In 1 patient, postoperative imaging examination of the proximal femur showed bone resorption and atrophy at 9 months. (F) In another patient, nonunion accompanied with intramedullary nail loosening was observed 12 months after operation. Tables
Table 1. Clinical data of 19 patients included in this study.Table 2. Data statistics and analysis of extended curettage with plate fixation (EC-PF) group and extended curettage with intramedullary nail fixation (EC-INF) group.Table 3. The Musculoskeletal Tumor Society score results of different internal fixation methods in 19 patients with proximal femoral giant cell tumor.Table 4. The appropriate internal fixation according to the International Society of Limb Salvage classification.Table 1. Clinical data of 19 patients included in this study.Table 2. Data statistics and analysis of extended curettage with plate fixation (EC-PF) group and extended curettage with intramedullary nail fixation (EC-INF) group.Table 3. The Musculoskeletal Tumor Society score results of different internal fixation methods in 19 patients with proximal femoral giant cell tumor.Table 4. The appropriate internal fixation according to the International Society of Limb Salvage classification. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387