09 July 2025: Review Articles
Advances in Neuromodulation Techniques for Aphasia Rehabilitation: A Comprehensive Review
Jiayi Xia ADEFG 1, Yeping Chen BCFG 1, Song Pei ADEF 2*, Chunlei Shan ADEF 3,4,5, Jingjing Zhang EF 3, Zhiqing Zhou EF 3, Jiali Wu EF 3, Yao Lu BC 1, Yiyi Chen BC 1, Yunjia Chen DF 1
DOI: 10.12659/MSM.947213
Med Sci Monit 2025; 31:e947213






Abstract
ABSTRACT: Aphasia, a language impairment resulting from stroke or neurodegenerative disease, presents complex rehabilitation challenges. Recently, neuromodulation techniques such as transcranial direct current stimulation (tDCS), transcranial magnetic stimulation (TMS), and mirror neuron system (MNS) therapy have emerged as promising adjuncts to traditional speech-language therapy. This narrative review summarizes current advances in these 3 modalities. tDCS involves low-intensity electrical stimulation to modulate cortical excitability, with evidence supporting its use in post-stroke aphasia (PSA) and primary progressive aphasia (PPA). TMS, a magnetic stimulation technique, provides more precise cortical targeting through low- or high-frequency protocols and emerging paradigms such as intermittent theta-burst stimulation (iTBS). MNS therapy employs behavioral strategies like action observation and imitation to enhance motor-language pathways. The review also discusses the neural mechanisms underlying aphasia recovery, such as cortical reorganization and interhemispheric compensation, and examines the role of advanced tools such as functional magnetic resonance imaging (fMRI) and diffusion tensor imaging (DTI) in guiding personalized treatment. Future directions include closed-loop stimulation, multimodal integration, and individualized protocols. This article aims to review recent developments in neuromodulation techniques for rehabilitating patients with aphasia, including transcranial direct current stimulation, transcranial magnetic stimulation, and mirror neuron system therapy.
Keywords: Aphasia, Rehabilitation, review, Transcranial Direct Current Stimulation, Transcranial Magnetic Stimulation, Humans, Mirror Neurons, Stroke, Magnetic Resonance Imaging
Introduction
Aphasia is a heterogeneous neurological condition characterized by impairments in language production, comprehension, reading, or writing, resulting from damage to language-dominant regions of the brain [1]. Rather than a singular disorder, aphasia encompasses multiple syndromes that differentially affect aspects of language function depending on the location and extent of neural injury [2]. Among the most studied forms of aphasia are post-stroke aphasia (PSA) and primary progressive aphasia (PPA), which differ in etiology and pathophysiology. PSA typically follows a sudden ischemic or hemorrhagic stroke affecting classical language areas such as Broca’s or Wernicke’s area in the left hemisphere [3,4], while PPA arises from neurodegenerative conditions such as frontotemporal lobar degeneration or Alzheimer disease, with insidious progression of language impairment [5]. These differences imply divergent patterns of brain damage: PSA reflects focal, often unilateral injury with potential for perilesional recovery, whereas PPA involves progressive cortical atrophy that impacts broader temporal and frontal language networks [6]. Understanding these distinctions is crucial for tailoring neuromodulatory treatments to the disease mechanism.
Traditional aphasia therapies primarily involve speech and language therapy (SLT), including constraint-induced language therapy and melodic intonation therapy [7]. While early and intensive SLT is associated with better outcomes, gains are often limited in chronic phases, and relapse or plateau effects are not uncommon [8]. As a result, increasing attention has turned to neuromodulation techniques, which are defined as interdisciplinary interventions that utilize electrical or magnetic stimulation to modulate brain networks [9,10]. Among them, noninvasive brain stimulation (NIBS) techniques – particularly transcranial magnetic stimulation (TMS) and transcranial direct current stimulation (tDCS) – have emerged as adjunctive tools for enhancing cortical plasticity and supporting language recovery [11,12]. Recent reviews by Breining et al [13] and Brady et al [14] have provided valuable insights into the effectiveness of neuromodulation techniques and speech-language therapy in aphasia. These studies explored the synergy between rehabilitation interventions and the potential of neuromodulation in optimizing aphasia treatment outcomes. Additionally, mirror neuron system (MNS) therapy, based on action observation and motor-language coupling, offers a behaviorally driven approach that can complement conventional methods [15].
This article reviews recent developments in neuromodulation techniques for rehabilitating patients with aphasia, including tDCS, TMS, and MNS (Table 1).
Mechanisms of Neuroplasticity in Aphasia Recovery
Contemporary aphasia treatment is anchored in the concept of “brain remodeling”. In the early weeks after a stroke, recovery mechanisms such as stabilization of cerebral blood flow, reduction in edema, and neuroplasticity promote synaptic reorganization and neurogenesis, facilitating language recovery. Xing et al [4] suggest that these processes lead to the early prediction of language outcomes, with structural and functional adaptations often occurring in the contralateral hemisphere or through ipsilateral compensation of remaining neural networks. The recovery of higher-order language functions is contingent upon the reorganization of the distributed language networks, which are responsible for both spontaneous recovery and responses to behavioral training [12]. According to Otal et al [16], post-stroke recovery involves extensive network remodeling, necessitating targeted behavioral interventions to engage specific brain regions. This network-based approach is supported by cognitive neuroscience, which posits that language networks are not isolated but rather are interconnected with broader cognitive systems, which exhibit dynamic activity depending on task demands [17]. Consequently, task-specific rehabilitation and neuromodulation techniques, which apply “top-down” strategies to promote network-level changes, have shown promise in enhancing aphasia recovery [18]. The greatest improvements in language typically occur within the first 3 months after stroke, especially in patients with mild to moderate aphasia, but continued rehabilitation efforts can lead to further gains even beyond 1 year after the event [19]. This evolving understanding underscores the need for sustained and individualized therapies aimed at exploiting brain recovery mechanisms.
While PSA recovery often relies on compensatory mechanisms such as inter-hemispheric communication and cortical reorganization, PPA follows a different progression. Due to the neurodegenerative nature of PPA, patients may not exhibit the same degree of neural plasticity or compensatory activation observed in stroke patients [20]. The decline of neural networks in PPA limits the brain’s capacity for reorganization; therefore, the focus for therapy in PPA should shift toward maintaining function and delaying degeneration. Recent studies suggest that targeted interventions, such as neuromodulation and speech therapy [21], may provide some benefits in slowing the decline, but more research is needed to better understand the potential for neural compensation in PPA.
Advances in Transcranial Direct Current Stimulation (tDCS) for Aphasia
MECHANISMS AND THEORETICAL FOUNDATIONS:
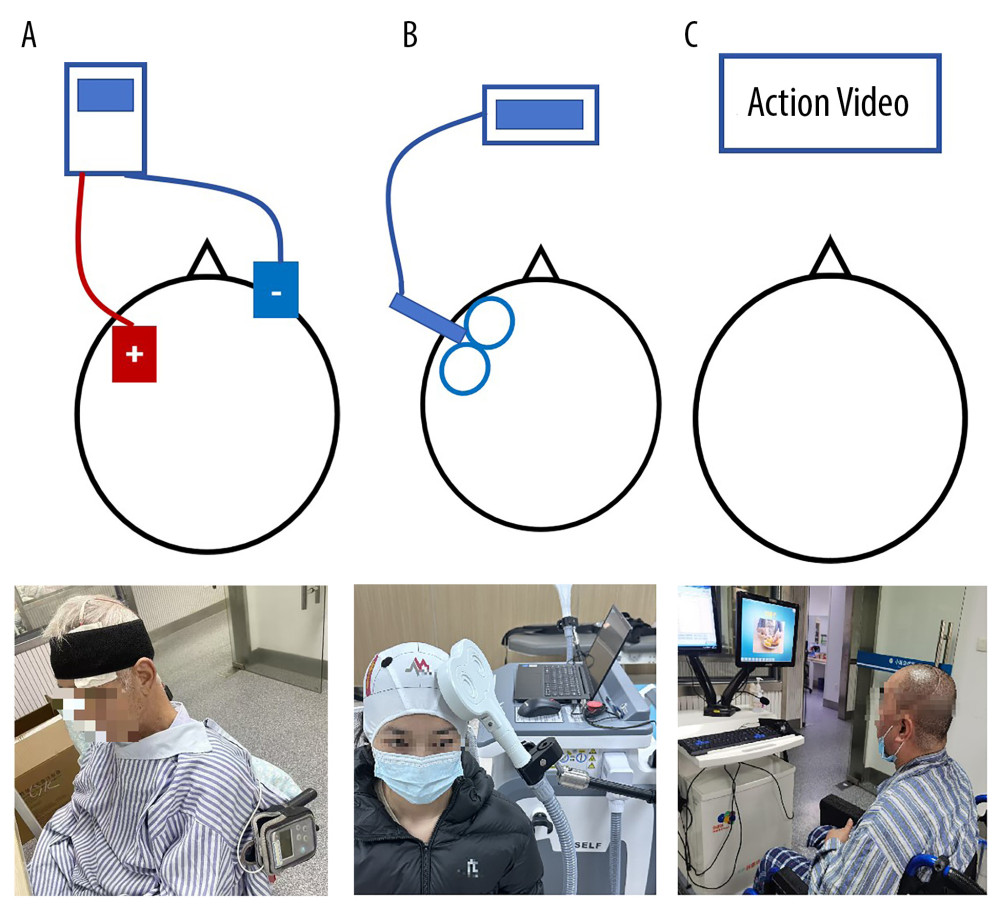
tDCS, a noninvasive neuromodulation technique introduced in the early 21st century, modulates neuronal activity through low-intensity electrical currents (typically 1–2 mA) applied to the scalp, leading to changes in cortical excitability and facilitating neuroplasticity. This method involves placing an electrode over the target cortical area, with a reference electrode placed on a contralateral site, often on the supraorbital region or shoulder [11] (Figure 1A).
Recent advances in tDCS hardware have made it increasingly portable, and ongoing parameter optimization has improved its efficacy in aphasia treatment. Emerging research explores dual-hemisphere stimulation strategies, showing potential in maximizing therapeutic benefits, particularly in chronic aphasia patients. tDCS is utilized in aphasia rehabilitation to augment the brain’s post-stroke reorganization patterns, which include compensatory activation in the right hemisphere and neuroplastic changes in the peri-infarct left hemisphere. Anodal tDCS applied to the left hemisphere can promote cortical excitability in damaged language regions, while cathodal stimulation to the right hemisphere can reduce maladaptive compensatory activity, promoting transcallosal modulation [6]. This technique enhances the neuroplasticity necessary for language recovery by bilaterally modulating cortical activity [22].
TDCS IN PSA:
In PSA, tDCS primarily facilitates recovery by modulating residual neural pathways and enhancing neuroplasticity in peri-lesional areas. Studies have demonstrated that anodal stimulation of the left hemisphere can significantly improve naming accuracy [6]. A recent randomized controlled trial by Stockbridge et al [23] investigated the efficacy of tDCS in subacute aphasia. While no significant improvements were observed in picture-naming recovery compared to sham stimulation, the study found notable gains in discourse skills, including content richness and efficiency. These findings suggest that tDCS can enhance broader communicative abilities beyond lexical retrieval, highlighting its potential role in promoting functional language use. Further research has explored different tDCS configurations to optimize language recovery. Fridriksson et al [3] applied anodal tDCS to activate peri-lesional areas of the left hemisphere, whereas Shah-Basak et al [24] employed cathodal tDCS to inhibit contralateral hemisphere activity, thereby enhancing language function through inter-hemispheric modulation. Additionally, bilateral tDCS, which simultaneously stimulates both hemispheres, has gained attention. Feil et al [25] demonstrated that this dual-hemisphere approach resulted in significant improvements in language function in PSA patients, further underscoring the potential of tDCS as a versatile intervention in aphasia rehabilitation.
While current tDCS protocols predominantly use open-loop stimulation, emerging closed-loop approaches show promise for personalized treatment. These systems utilize real-time electroencephalogram monitoring to adjust stimulation parameters based on individual brain state dynamics. Although not yet applied in aphasia rehabilitation, preliminary studies in motor recovery have demonstrated greater efficacy compared to standard protocols [26]. Similarly, the development of high-definition tDCS (HD-tDCS) [27] using multiple small electrodes may improve spatial specificity, although clinical validation in language disorders remains limited.
TDCS IN PPA:
In contrast to PSA, PPA presents unique challenges due to its degenerative nature. tDCS in PPA primarily aims to support the preservation of language functions by delaying the progressive decline in language networks. Recent studies using cerebellar tDCS have shown promising results in bilingual PPA patients, with significant improvements in both trained and untrained language tasks [28]. Additionally, advances in HD-tDCS have shown particular promise for chronic PPA cases, with improved spatial specificity and reduced off-target effects [29]. These findings suggest that tDCS can enhance specific language functions in aphasia rehabilitation, although optimal stimulation parameters, including intensity, site, and duration, require further investigation in larger patient samples [30].
EFFECTS AND SAFETY OF TDCS:
Unlike repetitive transcranial magnetic stimulation (rTMS), tDCS modulates neuronal excitability without inducing action potentials, making it particularly suited for enhancing the effects of concurrent behavioral therapies [31]. This synergistic application is critical during the acute and subacute phases after stroke, where neural networks may still be in the process of reorganization. Raymer et al [32] found that tDCS can amplify neuroplasticity by providing an external boost to the brain’s natural recovery processes, leading to prolonged benefits even after the stimulation period. Furthermore, pairing tDCS with language-specific therapies has shown promise in improving aphasia outcomes by reinforcing skill acquisition and retention [33]. Guillouët et al [34] noted that in terms of safety, tDCS uses low-intensity currents (typically around 2 mA) and large electrodes (25–35 cm2), which ensure minimal current density and contribute to a favorable safety profile. There have been no reports of tDCS-induced seizures, and some research even suggests that cathodal stimulation can reduce seizure incidence, further demonstrating its suitability in post-stroke populations [35]. The portable nature of tDCS, along with its built-in sham controls, makes it an ideal candidate for clinical trials and rehabilitation settings. As a result, tDCS is increasingly recognized as a valuable tool for exploring novel aphasia treatment methods and gaining insight into the mechanisms underlying neural recovery.
Advances in Transcranial Magnetic Stimulation (TMS) for Aphasia
MECHANISMS AND THEORETICAL FOUNDATIONS:
TMS is a noninvasive brain stimulation technique that uses a magnetic coil placed near the scalp to generate a magnetic field, which penetrates the skull and induces electric currents in the brain [36]. This allows for targeted modulation of neural activity, either enhancing or inhibiting function in specific cortical regions, depending on the frequency of stimulation [37]. Low-frequency rTMS (≤1 Hz) is used to inhibit hyperactive areas, while high-frequency rTMS (≥5 Hz) is used to stimulate underactive brain regions. These mechanisms form the basis for TMS applications in aphasia rehabilitation [38] (Figure 1B).
TMS IN PSA:
TMS has been widely studied in PSA, particularly for its role in modulating perilesional and contralesional cortical activity to promote language recovery [39]. rTMS is used to suppress maladaptive activity in the right hemisphere or enhance function in the left hemisphere’s language network. High-frequency rTMS (≥5Hz) can be used to enhance excitability in the left hemisphere’s language areas, particularly Broca’s area. Low-frequency rTMS (≤1 Hz) can enhance language function by reducing excessive contralesional activity in the right inferior frontal gyrus, which is the homolog of Broca’s area [40]. Lin et al [41] applied low-frequency (1 Hz) rTMS to the right inferior frontal gyrus in patients with subcortical aphasia, observing notable gains in picture-naming abilities, particularly among patients with non-fluent aphasia. Some studies have explored the use of double-coil TMS in PSA. Khedr et al [42] explored the use of bilateral rTMS in 30 patients with subacute non-fluent aphasia. They applied 1 Hz rTMS to the right Broca’s area and 20 Hz rTMS to the left Broca’s area, followed by speech therapy. Patients receiving real rTMS treatments exhibited significant improvements in both language function and mood, which were sustained 2 months after the intervention.
While conventional rTMS approaches have shown effectiveness in aphasia rehabilitation, newer paradigms such as intermittent theta-burst stimulation (iTBS) offer a promising alternative due to their enhanced neuroplasticity effects. Szaflarski et al [43] conducted a pilot randomized, double-blind, sham-controlled trial investigating the effects of functional magnetic resonance imaging (fMRI)-guided iTBS applied to the ipsilesional hemisphere in chronic PSA. The study demonstrated improvements in both language function and cortical plasticity. Functional MRI analysis revealed increased bilateral activation and connectivity changes in inferior frontal gyrus (IFG), further supporting the role of iTBS in facilitating neural reorganization.
This integration of neuroimaging and rTMS enables more accurate targeting of cortical regions and allows for a more precise analysis of its effects in aphasia rehabilitation, showing promise for improving language outcomes in PSA patients. Allendorfer et al [44] discussed the great potential of this approach for tailoring individualized interventions that maximize therapeutic efficacy by leveraging neuroimaging data to optimize cortical stimulation. Emerging evidence suggests that incorporating structural connectivity data from diffusion tensor imaging (DTI) can further improve target selection by identifying intact white-matter pathways [45].
TMS IN PPA:
Unlike PSA, PPA is a neurodegenerative condition that gradually affects the left perisylvian cortex, leading to progressive language deficits over time. TMS is being investigated as a potential intervention to slow language deterioration and enhance compensatory mechanisms in non-fluent and semantic PPA variants [5]. Trebbastoni et al [46] showed that high-frequency rTMS targeting the left frontal lobe in patients with PPA yielded improvements in language function after just 5 days of treatment. Pytel et al [47] used 20 Hz rTMS targeting personalized brain regions (eg, left IFG, left anterior temporal lobe) in PPA patients, reporting improvements in spontaneous speech, object naming, and reading skills.
Given the progressive nature of PPA, researchers are investigating multimodal approaches, such as combining rTMS with speech therapy and cognitive training programs to maximize functional outcomes. Additionally, closed-loop rTMS [48] protocols that dynamically adjust stimulation intensity based on real-time brain activity may offer more effective intervention strategies.
EFFECTS AND SAFETY OF TMS:
TMS is widely regarded as a safe and NIBS technique, particularly when protocols adhere to established safety guidelines. The integration of advanced neuroimaging and neuroelectrophysiology has further reduced risks, enhancing the precision and safety of TMS applications [49]. Large-scale studies, such as those referenced by Rossi et al [50], report an extremely low incidence of adverse effects, with seizures being exceedingly rare. These events are typically self-limiting and occur only under conditions that exceed recommended stimulation parameters. Minor adverse effects, such as transient headaches, scalp discomfort, or mild muscle twitching, remain the most commonly reported concerns, underscoring the overall tolerability of TMS in both clinical and research settings. In addition to its favorable safety profile, TMS is highly compatible with sham-controlled designs, which makes it particularly suitable for clinical trials and therapeutic interventions in aphasia rehabilitation. Lefaucheur et al [51] emphasized the importance of customizing stimulation protocols (eg, frequency, intensity, and session duration) to maximize therapeutic efficacy while maintaining safety. Although TMS lacks the portability of tDCS due to its larger equipment and higher costs, recent technological developments, such as improved precision in neuronavigation and frequency customization, have enhanced its clinical relevance in aphasia rehabilitation. These characteristics make TMS a promising tool for exploring innovative treatments in neurocognitive disorders, including aphasia.
Advances in Mirror Neuron System (MNS) Therapy for Aphasia
MECHANISMS AND THEORETICAL FOUNDATIONS:
MNS therapy, grounded in the principle of action observation and imitation, offers a behavioral neuromodulation approach that differs fundamentally from hardware-based techniques like tDCS and TMS. Mirror neurons, first identified in primates, are specialized neurons that fire both when an individual performs an action and when they observe the same action performed by others [52]. These neurons respond to both visual and auditory stimuli and are thought to facilitate imitation learning in humans [53]. MNS therapy, rooted in this theory, aims to restore disrupted neural networks, particularly those involved in motor, language, and cognitive functions, by employing “top-down” neuromodulation techniques. This approach has gained prominence as a rehabilitation strategy in post-stroke recovery and other neurological conditions (Figure 1C).
MNS IN PSA:
In PSA, MNS-based therapies have shown particular promise for patients with motor-related language impairments. In a study by Chen et al [15], a patient with transcortical motor aphasia underwent a 3-week intervention that alternated between observing dynamic videos of hand movements and static images of objects while repeating their names. Results from the Western Aphasia Battery (WAB) evaluations indicated that the observation of hand movements resulted in more significant improvements in naming accuracy and overall language abilities compared to static image observation. Expanding this research, 24 aphasia patients were divided into 3 groups: one focused on hand movement observation and repetition, another on object observation and repetition, and the third received conventional speech therapy. Those in the hand movement group showed superior improvements in naming abilities and spontaneous speech, highlighting the potential of MNS-based therapies for aphasia rehabilitation [54]. These findings suggest that MNS therapy can promote the reorganization of neural networks involved in language function, making it a promising approach for both acute and chronic phases of aphasia. Arya et al [55] further supported these results by demonstrating that 45 sessions of MNS therapy improved communication abilities in a Broca’s aphasia patient, with an increase in communication scores from 18/100 to 79/100. However, the study also revealed that MNS therapy’s effects might be task-specific, as it did not significantly improve written comprehension of action-based instructions [56]. Li et al [57] found that MNS activation also helps improve apraxia of speech (AOS). However, no reports on the application of MNT in PPA were found, perhaps due to the limitations of the retrieval method used.
MULTIMODAL APPLICATIONS OF MIRROR NEURONS:
Durand et al [58] demonstrated that combining language training with sensory-motor strategies enhances language recovery in aphasia patients with verb-naming difficulties. A key approach, known as Personalized Observation, Execution, and Mental Imagery Therapy, was found to significantly improve word retrieval and language processing. Post-therapy fMRI scans revealed increased activation in brain regions associated with both language and the MNS, suggesting that MNS plays a pivotal role in integrating sensory-motor functions with language rehabilitation. The posterior IFG, a core region in the MNS, has been identified as crucial for converting speech perception into speech production, particularly during tasks such as repetition [59]. Studies incorporating multimodal treatment approaches, such as combining speech training with brain stimulation like theta-burst stimulation to the left posterior IFG, have shown promise in restoring language function after stroke [58]. These findings highlight the potential of MNS-based, multimodal treatments for aphasia and underscore the need for continued research into optimizing neuromodulation strategies to improve language recovery outcomes.
Future Directions
The advances in neuromodulation techniques underscore their transformative potential in aphasia rehabilitation, while also highlighting the critical need for individualized treatment protocols tailored to aphasia etiology and severity [60]. However, several key challenges remain in the comparison, application, and optimization of these techniques. One of the primary obstacles is the wide variability in stimulation protocols, including differences in targeted brain regions, stimulation parameters, and integration with language therapies. This inconsistency poses significant challenges for cross-study comparisons and meta-analyses. In addition to methodological variability, each neuromodulation technique has inherent strengths and limitations. tDCS is a widely accessible and cost-effective option, offering portability and ease of application; however, its limited spatial precision restricts its ability to effectively target specific neural circuits. In contrast, TMS provides more precise cortical stimulation, particularly with neuronavigation-guided approaches, but is limited to superficial cortical areas and requires specialized, high-cost equipment, reducing its accessibility in routine clinical settings. MNS therapy, a behaviorally driven approach, engages motor-language pathways through action observation and imitation. While it is highly effective for motor aphasia, its efficacy may be limited in patients with sensory aphasia. Moreover, the field lacks standardized protocols for patient selection, outcome measures, and long-term follow-up, making it difficult to assess the durability of treatment effects [61].
To advance the field and optimize the clinical efficacy of neuromodulation, future research should focus on several key innovations. First, the development of closed-loop neuromodulation systems that dynamically adjust stimulation parameters in real-time based on neurophysiological responses could significantly enhance treatment personalization [62]. Second, the integration of multimodal neuroimaging techniques, such as fMRI and DTI, may facilitate more precise target selection, thereby improving treatment efficacy. Third, emerging advanced stimulation configurations, including HD-tDCS and double-coil TMS, warrant further exploration as they offer greater spatial specificity and optimized neural targeting [63]. Finally, the standardization of treatment protocols, particularly in terms of stimulation parameters, session durations, and patient eligibility criteria, is essential to enhance the reproducibility and comparability of clinical studies.
Additionally, combining different neuromodulation techniques, such as tDCS and TMS, may produce synergistic effects, further enhancing language recovery outcomes. Moreover, integrating neuromodulation with evidence-based language therapies through multimodal rehabilitation approaches may lead to more effective and sustained improvements in functional communication skills [64]. These advances in precision, personalization, and protocol standardization have the potential to significantly enhance treatment efficacy and drive the field toward more individualized, data-driven rehabilitation strategies.
Conclusions
Neuromodulation techniques such as tDCS, TMS, and MNS therapy have demonstrated significant potential in enhancing language recovery in patients with aphasia. The effectiveness of these interventions depends on factors such as stimulation parameters, patient-specific neural profiles, and integration with conventional speech therapies. While promising results have been reported, further high-quality studies are required to refine protocols, establish standardized guidelines, and expand the clinical application of these technologies. Future efforts should also focus on individualized and multimodal approaches to maximize therapeutic outcomes.
References
1. Wallentin M, Sex differences in post-stroke aphasia rates are caused by age. A meta-analysis and database query: PLoS One, 2018; 13(12); e0209571
2. Castro N, Hula WD, Ashaie SA, Defining aphasia: Content analysis of six aphasia diagnostic batteries: Cortex, 2023; 166; 19-32
3. Fridriksson J, Rorden C, Elm J, Transcranial direct current stimulation vs sham stimulation to treat aphasia after stroke: A randomized clinical trial: JAMA Neurol, 2018; 75(12); 1470-76
4. Xing S, Mandal A, Lacey EH, Skipper-Kallal LM, Behavioral effects of chronic gray and white matter stroke lesions in a functionally defined connectome for naming: Neurorehabil Neural Repair, 2018; 32(6–7); 613-23
5. Papanikolaou K, Nasios G, Nousia A, Noninvasive brain stimulation in primary progressive aphasia: A literature review: Adv Exp Med Biol, 2023; 1425; 567-74
6. Bonilha L, Rorden C, Roth R, Improved naming in patients with Broca’s aphasia with tDCS: J Neurol Neurosurg Psychiatry, 2024; 95(3); 273-76
7. Butt AK, Zubair R, Rathore FA, The role of augmentative and alternative communication in speech and language therapy: A mini review: J Pak Med Assoc, 2022; 72(3); 581-84
8. Godecke E, Armstrong E, Rai T, A randomized control trial of intensive aphasia therapy after acute stroke: The Very Early Rehabilitation for SpEech (VERSE) study: Int J Stroke, 2021; 16(5); 556-72
9. Evancho A, Tyler WJ, McGregor K, A review of combined neuromodulation and physical therapy interventions for enhanced neurorehabilitation: Front Hum Neurosci, 2023; 17; 1151218
10. Shah-Basak P, Boukrina O, Li XR, Targeted neurorehabilitation strategies in post-stroke aphasia: Restor Neurol Neurosci, 2023; 41(3–4); 129-91
11. Cirillo G, Di Pino G, Capone F, Neurobiological after-effects of non-invasive brain stimulation: Brain Stimul, 2017; 10(1); 1-18
12. Kiran S, Thompson CK, Neuroplasticity of language networks in aphasia: Advances, updates, and future challenges: Front Neurol, 2019; 10; 295
13. Breining BL, Sebastian R, Neuromodulation in post-stroke aphasia treatment: Curr Phys Med Rehabil Rep, 2020; 8(2); 44-56
14. Brady MC, Godwin J, Enderby P, Speech and language therapy for aphasia after stroke: An updated systematic review and meta-analyses: Stroke, 2016; 47; e236-e37
15. Chen W, Ye Q, Ji X, Mirror neuron system based therapy for aphasia rehabilitation: Front Psychol, 2015; 6; 1665
16. Otal B, Olma MC, Flöel A, Wellwood I, Inhibitory non-invasive brain stimulation to homologous language regions as an adjunct to speech and language therapy in post-stroke aphasia: A meta-analysis: Front Hum Neurosci, 2015; 9; 236
17. Baliki MN, Babbitt EM, Cherney LR, Brain network topology influences response to intensive comprehensive aphasia treatment: NeuroRehabilitation, 2018; 43(1); 63-76
18. Norise C, Hamilton RH, Non-invasive brain stimulation in the treatment of post-stroke and neurodegenerative aphasia: Parallels, differences, and lessons learned: Front Hum Neurosci, 2017; 10; 675
19. Stahl B, Mohr B, Büscher V, Efficacy of intensive aphasia therapy in patients with chronic stroke: A randomised controlled trial: J Neurol Neurosurg Psychiatry, 2018; 89(6); 586-92
20. Silva AAD, Silagi ML, Ortiz KZ, Language assessment in primary progressive aphasia: Which components should be tested?: PLoS One, 2025; 20(2); e0318155
21. Moral-Rubio C, Suárez-Coalla P, Fernandez-Romero L, Effects of single-session repetitive transcranial magnetic stimulation to identify the optimal brain target in primary progressive aphasia: J Alzheimers Dis, 2025 [Online ahead of print]
22. Elsner B, Kugler J, Pohl M, Mehrholz J, Transcranial direct current stimulation (tDCS) for improving aphasia in patients with aphasia after stroke: Cochrane Database Syst Rev, 2015(5); CD009760
23. Stockbridge MD, Elm J, Breining BL, Transcranial direct-current stimulation in subacute aphasia: A randomized controlled trial: Stroke, 2023; 54(4); 912-20
24. Shah-Basak PP, Norise C, Garcia G, Individualized treatment with transcranial direct current stimulation in patients with chronic non-fluent aphasia due to stroke: Front Hum Neurosci, 2015; 9; 201
25. Feil S, Eisenhut P, Strakeljahn F, Left shifting of language related activity induced by bihemispheric tDCS in postacute aphasia following stroke: Front Neurosci, 2019; 13; 295
26. Lima JPS, Silva LA, Delisle-Rodriguez D, Unraveling transformative effects after tDCS and BCI intervention in chronic post-stroke patient rehabilitation – an alternative treatment design study: Sensors (Basel), 2023; 23(23); 9302
27. Busan P, Moret B, Formaggio E, High definition-transcranial random noise stimulation to improve speech fluency in persistent developmental stuttering: A case study: Clin Neurophysiol, 2023; 152; 71-74
28. Coemans S, De Aguiar V, Paquier P, Effects of cerebellar transcranial direct current stimulation in bilingual logopenic primary progressive aphasia: J Alzheimers Dis Rep, 2024; 8(1); 1253-73
29. Crowley SJ, Iordan AD, Rinna K, Comparing high definition transcranial direct current stimulation to left temporoparietal junction and left inferior frontal gyrus for logopenic primary progressive aphasia: A single-case study: Neuropsychol Rehabil, 2024; 34(10); 1478-503
30. de Aguiar V, Paolazzi CL, Miceli G, tDCS in post-stroke aphasia: The role of stimulation parameters, behavioral treatment and patient characteristics: Cortex, 2015; 63; 296-316
31. Zettin M, Bondesan C, Nada G, Transcranial direct-current stimulation and behavioral training, a promising tool for a tailor-made post-stroke aphasia rehabilitation: A review: Front Hum Neurosci, 2021; 15; 742136
32. Raymer AM, Johnson RK, Effectiveness of transcranial direct current stimulation as an adjuvant to aphasia treatment following stroke: Evidence from systematic reviews and meta-analyses: Am J Speech Lang Pathol, 2024; 33(6S); 3431-43
33. You Y, Li Y, Zhang Y, Long-term effects of transcranial direct current stimulation (tDCS) combined with speech language therapy (SLT) on post-stroke aphasia patients: A systematic review and network meta-analysis of randomized controlled trials: NeuroRehabilitation, 2023; 53(3); 285-96
34. Guillouët E, Cogné M, Saverot E, Impact of combined transcranial direct current stimulation and speech-language therapy on spontaneous speech in aphasia: A randomized controlled double-blind study: J Int Neuropsychol Soc, 2020; 26(1); 7-18
35. Ko MH, Safety of transcranial direct current stimulation in neurorehabilitation: Brain Neurorehabil, 2021; 14(1); e9
36. Siebner HR, Funke K, Aberra AS, Transcranial magnetic stimulation of the brain: What is stimulated? – A consensus and critical position paper: Clin Neurophysiol, 2022; 140; 59-97
37. Heiss WD, Imaging effects related to language improvements by rTMS: Restor Neurol Neurosci, 2016; 34(4); 531-36
38. Wawrzyniak M, Schneider HR, Klingbeil J, Resolution of diaschisis contributes to early recovery from post-stroke aphasia: Neuroimage, 2022; 251; 119001
39. Chai L, Huang Y, Guo X, Does SLT combined with NIBS enhance naming recovery in post-stroke aphasia? A meta-analysis and systematic review: NeuroRehabilitation, 2024; 54(4); 543-61
40. Wang C, Nie P, Wang P, The therapeutic effect of transcranial magnetic stimulation on post-stroke aphasia and the optimal treatment parameters: A meta-analysis: Arch Phys Med Rehabil, 2024; 105(7); 1388-98
41. Lin BF, Yeh SC, Kao YJ, Functional remodeling associated with language recovery after repetitive transcranial magnetic stimulation in chronic aphasic stroke: Front Neurol, 2022; 13; 809843
42. Khedr EM, Abo El-Fetoh N, Ali AM, Dual-hemisphere repetitive transcranial magnetic stimulation for rehabilitation of poststroke aphasia: A randomized, double-blind clinical trial: Neurorehabil Neural Repair, 2014; 28(8); 740-50
43. Szaflarski JP, Nenert R, Allendorfer JB, Intermittent theta burst stimulation (iTBS) for treatment of chronic post-stroke aphasia: Results of a pilot randomized, double-blind, sham-controlled trial: Med Sci Monit, 2021; 27; e931468
44. Allendorfer JB, Nenert R, Vannest J, Szaflarski JP, a pilot randomized controlled trial of intermittent theta burst stimulation as stand-alone treatment for post-stroke aphasia: effects on language and verbal functional magnetic resonance imaging (fMRI): Med Sci Monit, 2021; 27; e934818
45. Zhang X, Talifu Z, Li J, Melodic intonation therapy for non-fluent aphasia after stroke: A clinical pilot study on behavioral and DTI findings: iScience, 2023; 26(9); 107453
46. Trebbastoni A, Raccah R, de Lena C, Repetitive deep transcranial magnetic stimulation improves verbal fluency and written language in a patient with primary progressive aphasia-logopenic variant (LPPA): Brain Stimul, 2013; 6(4); 545-53
47. Pytel V, Cabrera-Martín MN, Delgado-Álvarez A, Personalized repetitive transcranial magnetic stimulation for primary progressive aphasia: J Alzheimers Dis, 2021; 84(1); 151-67
48. Zrenner C, Ziemann U, Closed-loop brain stimulation: Biol Psychiatry, 2024; 95(6); 545-52
49. Han C, Tang J, Tang B, The effectiveness and safety of noninvasive brain stimulation technology combined with speech training on aphasia after stroke: A systematic review and meta-analysis: Medicine (Baltimore), 2024; 103(2); e36880
50. Rossi S, Antal A, Bestmann S, Safety and recommendations for TMS use in healthy subjects and patient populations, with updates on training, ethical and regulatory issues: Expert Guidelines: Clin Neurophysiol, 2021; 132(1); 269-306
51. Lefaucheur JP, André-Obadia N, Antal A, Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): Clin Neurophysiol, 2014; 125(11); 2150-206
52. Figueiredo LF, Lannes ME, Mathias C, The mirror neuron: Thirty years since its discovery: Braz J Psychiatry, 2023; 45(3); 298-99
53. Rizzolatti G, Sinigaglia C, The mirror mechanism: A basic principle of brain function: Nat Rev Neurosci, 2016; 17(12); 757-65
54. Chen WL, Ye Q, Zhang SC, Aphasia rehabilitation based on mirror neuron theory: A randomized-block-design study of neuropsychology and functional magnetic resonance imaging: Neural Regen Res, 2019; 14(6); 1004-12
55. Arya KN, Pandian S, Inadvertent recovery in communication deficits following the upper limb mirror therapy in stroke: A case report: J Bodyw Mov Ther, 2014; 18(4); 566-68
56. Rogalsky C, Raphel K, Tomkovicz V, Neural basis of action understanding: Evidence from sign language aphasia: Aphasiology, 2013; 27(9); 1147-58
57. You L, Wang Y, Chen W, The effectiveness of action observation therapy based on mirror neuron theory in Chinese patients with apraxia of speech after stroke: Eur Neurol, 2019; 81(5–6); 278-86
58. Durand E, Berroir P, Ansaldo AI, The neural and behavioral correlates of anomia recovery following personalized observation, execution, and mental imagery therapy: A proof of concept: Neural Plast, 2018; 2018; 5943759
59. Heikkinen PH, Pulvermüller F, Mäkelä JP, Combining rTMS with intensive language-action therapy in chronic aphasia: A randomized controlled trial: Front Neurosci, 2019; 12; 1036
60. Soleimani G, Nitsche MA, Bergmann TO, Closing the loop between brain and electrical stimulation: Towards precision neuromodulation treatments: Transl Psychiatry, 2023; 13(1); 279
61. Vassiliadis P, Grandjean J, Derosiere G, Using a double-coil TMS protocol to assess preparatory inhibition bilaterally: Front Neurosci, 2018; 12; 139
62. Cappon DB, Pascual-Leone A, Toward precision noninvasive brain stimulation: Am J Psychiatry, 2024; 181(9); 795-805
63. Kesikburun S, Non-invasive brain stimulation in rehabilitation: Turk J Phys Med Rehabil, 2022; 68(1); 1-8
64. Lefaucheur JP, Aleman A, Baeken C, Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): An update (2014–2018): Clin Neurophysiol, 2020; 131(2); 474-528 [published correction appears in Clin Neurophysiol. 2020;131(5):1168–69]
Tables
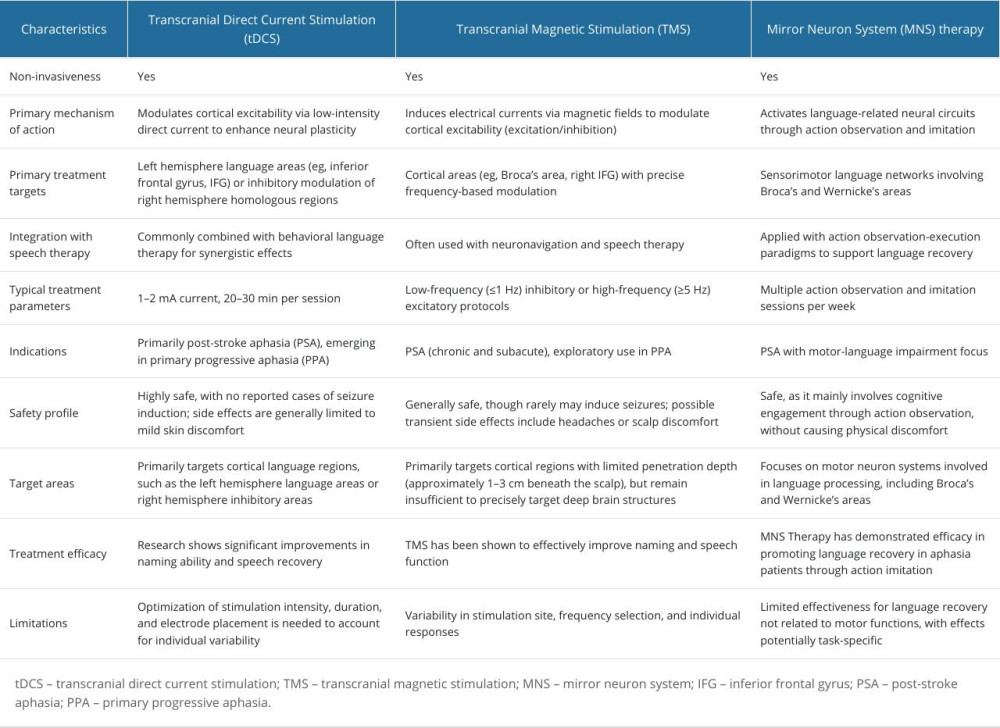 Table 1. Comparison of transcranial direct current stimulation (tDCS), transcranial magnetic stimulation (TMS), and mirror neuron system (MNS) therapy in aphasia rehabilitation.Table 1. Comparison of transcranial direct current stimulation (tDCS), transcranial magnetic stimulation (TMS), and mirror neuron system (MNS) therapy in aphasia rehabilitation.
Table 1. Comparison of transcranial direct current stimulation (tDCS), transcranial magnetic stimulation (TMS), and mirror neuron system (MNS) therapy in aphasia rehabilitation.Table 1. Comparison of transcranial direct current stimulation (tDCS), transcranial magnetic stimulation (TMS), and mirror neuron system (MNS) therapy in aphasia rehabilitation. In Press
Clinical Research
Association Between Total Cholesterol–to–High-Density Lipoprotein Ratio and Gestational Hypertension: A Cas...Med Sci Monit In Press; DOI: 10.12659/MSM.952395
Review article
Clinical Use of Endotracheal Intubation Without Neuromuscular Blockade: The Current Stage of KnowledgeMed Sci Monit In Press; DOI: 10.12659/MSM.951765
Clinical Research
Effect of Dexmedetomidine Hydrochloride Nasal Spray on Anxiety and Sleep in Patients Undergoing Gynecologic...Med Sci Monit In Press; DOI: 10.12659/MSM.952465
Clinical Research
Prognostic Value of Mortality Scoring Systems in Patients With Severe Burns: Identifying Key Predictors of ...Med Sci Monit In Press; DOI: 10.12659/MSM.951713
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,173
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,757,769
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,143
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,797
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387