19 February 2025: Clinical Research
Procedure Dynamics in Transfemoral vs Transradial Cerebral Angiography: A Retrospective Study
Tae-sung Kim BCDE 1, Jinhoo Seok DOI: 10.12659/MSM.947603
Med Sci Monit 2025; 31:e947603






Abstract
BACKGROUND: Cerebral angiography, although invasive, remains the most accurate diagnostic tool for neurovascular diseases. While transfemoral cerebral angiography (TFCA) is the conventional approach, transradial cerebral angiography (TRCA) has gained interest due to potential benefits, such as reduced hematoma risk and shorter recovery times. However, procedure times and influencing factors remain debated. This retrospective study from a single center aimed to compare procedure time in 100 patients undergoing conventional TFCA and 93 undergoing TRCA.
MATERIAL AND METHODS: This single-center retrospective study included 193 patients who underwent 4-vessel cerebral angiography from January to December 2023. TFCA and TRCA were performed by experienced neurosurgeons. TRCA involved radial artery access with collateral circulation assessment (modified Allen’s and Barbeau’s tests), and TFCA used femoral artery access with standard techniques. Clinical data, including puncture times and radiation exposure, were collected. Logistic regression identified factors influencing prolonged procedure times (>20 minutes).
RESULTS: Procedure times for TFCA and TRCA were similar (median: 20.00 minutes vs 24.50 minutes, p=0.139), though TRCA showed longer puncture times (median: 10.00 vs 10.00 minutes, p=0.001). Radiation exposure was comparable (421.00 milliGray (mGy) vs 418.50 mGy, p=0.530). Hypertension (OR: 2.255, p=0.011) and aortic arch tortuosity (OR: 3.881, p=0.002) significantly influenced prolonged procedures.
CONCLUSIONS: TRCA offers a safe and effective alternative to TFCA for diagnostic cerebral angiography, with comparable procedure times and radiation exposure. While patient-specific factors, such as hypertension and aortic arch tortuosity, influence procedure duration, TRCA provides benefits in patient comfort and recovery. These findings support the broader use of TRCA in diagnostic settings.
Keywords: Cerebral Angiography, Radial Artery, Angiography, Digital Subtraction, Humans, Retrospective Studies, Female, Male, Femoral Artery, Middle Aged, Aged, adult
Introduction
Cerebral angiography, although somewhat invasive, is regarded as the most accurate diagnostic tool for many neurovascular diseases [1–3]. While transfemoral cerebral angiography (TFCA) remains the conventional and most widely used approach, there has been a growing interest in transradial cerebral angiography (TRCA) in recent years, as evidenced by numerous studies [4–7]. However, unlike the field of cardiology, where the radial approach has become more prevalent than the femoral approach since Campeau first introduced radial access for coronary angiography in 1989, femoral access remains the more familiar choice in neurology [8]. One reason for this preference is that neurologic treatments often require larger coaxial and triaxial catheter systems compared to cardiologic treatments [8,9]. Nevertheless, in cases where only angiography is performed, the need for coaxial systems is minimal. In such situations, radial access may offer advantages, including shorter hospital stays, a lower risk of hematoma, and elimination the need for post-procedure bed rest [9–11].
Recent studies comparing TRCA and TFCA have reported mixed findings: some suggest that TRCA takes longer, while others report no significant difference in procedure times [7,8,12]. However, TRCA has consistently been shown to have higher patient satisfaction and comparable safety to TFCA [1,3,13,14].
Therefore, this retrospective study from a single center aimed to compare procedure time in 100 patients undergoing conventional TFCA and 93 patients undergoing TRCA. Additionally, we sought to identify the factors that most significantly influence procedure time.
Material and Methods
STUDY DESIGN AND POPULATION:
This retrospective study, conducted at a single neurosurgical center, received approval from the Institutional Review Board of our hospital (2025GR0004). The requirement to obtain informed consent from the patients was waived. Data were collected from patients who underwent 4-vessel angiography between January 2023 and December 2023. All digital subtraction angiographies (DSAs) were performed either TFCA or TRCA, by 4 skilled cerebrovascular specialist neurosurgeons. Patients who underwent other types of angiographies, such as 6-vessel angiography or target vessel angiography, were excluded from the study. From January 2023 to December 2023, a total of 215 patients underwent 4-vessel angiography at our center; 110 patients underwent DSA via the femoral approach, and 95 via the radial approach. Since we aimed to compare the puncture time of both procedures, 10 patients who initially underwent radial puncture but later required a femoral approach due to failure were excluded from the analysis. Additionally, 2 patients who underwent TRCA but had inaccurate admission times, making puncture time determination difficult, were excluded. Therefore, puncture times were evaluated in 100 TFCA patients and 93 TRCA patients. The study flow diagram is presented in Figure 1.
TRANSRADIAL CEREBRAL ANGIOGRAPHY (TRCA): To assess palmar collateral circulation, a modified Allen’s test and Barbeau’s test were performed prior to the procedure. Patients with abnormal collateral circulation test results underwent the procedure via the transfemoral approach. The right forearm was positioned at 30 degrees of abduction and supination, with the wrist extended approximately 30 degrees using a wrist pillow. The area was draped using the usual aseptic technique. After administering local anesthesia, the radial artery was punctured, and a 5-French (Fr), 7-cm sheath with a dilator (Terumo, Somerset, NJ, USA) was inserted. Immediately afterward, 7 mL of a cocktail solution consisting of verapamil 5 mg, nitroglycerin 200 mg, and heparin 1000 IU was administered. A 5-Fr Simmons 2 catheter (Terumo) was used for the procedure. The guidewire was advanced through the radial artery and brachial artery, traversing the subclavian artery and ascending into the aorta. After reaching the ascending aorta, the guidewire was manipulated to turn back at the aortic valve, enabling reconstitution of the natural configuration of the Simmons 2 catheter. Subsequently, the catheter tip was maneuvered to selectively engage each target artery, and angiograms were performed (Figure 2). As mentioned above, only cases in which all 4 intracranial arteries – namely, the right and left internal carotid arteries (ICA) and the right and left vertebral arteries (VA) – were examined were included in the comparison. Therefore, all patients included in this study underwent evaluation of all 4 vessels. In cases where selective catheterization of the left VA was difficult, the left subclavian artery was selected, and a blood pressure cuff was applied to the left arm, inflating it to facilitate the examination. After the procedure, a TR band (Terumo) was applied to the puncture site, and the sheath was withdrawn while simultaneously inflating the balloon. Hemostasis was maintained by keeping the TR band in place for 2 hours.
TRANSFEMORAL CEREBRAL ANGIOGRAPHY (TFCA):
The right femoral lesion was draped using the usual aseptic method, and local anesthesia was administered. The femoral artery was palpated, and a 5-Fr long sheath was inserted. The angiogram was performed using a 5Fr Davis catheter (Terumo). When vessel selection was challenging due to a tortuous aortic arch, an HN 5 catheter (Terumo) or a Simmons 2 catheter (Terumo) was used. As with the other procedures, only patients who underwent evaluation of all 4 vessels – both ICAs and both Vas – were included in the study. Upon completion of the procedure, hemostasis was achieved by removing the sheath and applying closure devices such as Starclose or Femoseal.
DATA COLLECTION AND OUTCOME MEASURES:
Clinical characteristics data, including sex, BMI, and details of past medical history such as smoking history, hyperlipidemia, coronary heart disease, atrial fibrillation, diabetes, kidney disease, stroke, and use of antiplatelet agents, were retrieved from the hospital’s electronic medical records (EMR) system. Procedure-associated data, including admission time, procedure start time, and procedure end time, were extracted from the nursing records within the same EMR system. These time points were documented in real-time during the procedures to ensure accuracy. Procedure start time was defined as the completion time of sheath insertion following puncture. The puncture time was calculated by subtracting the admission time from the procedure start time, while the procedure time was determined by subtracting the procedure start time from the procedure end time. We evaluated the tortuosity of the aortic arch with reference to previous studies and assessed its potential impact on procedural duration [15]. A procedure time exceeding 20 minutes was defined as a long procedure time. Among the factors potentially influencing this, the anatomic features of the aortic arch were considered to have a significant impact. These features were evaluated based on previous studies [15], and univariable and multivariable analyses were conducted to assess their effects.
DATA PREPARATION:
Data underwent anonymization, with removal of duplicated entries. Missing data were minimal (<2% of total observations) and were excluded from the analysis without imputation, as they were not systematically related to outcomes.
DESCRIPTIVE STATISTICS:
Categorical data were presented as population numbers and proportions with percentages. Continuous data were assessed for normality using the Shapiro-Wilk test. Normally distributed variables were summarized as means with standard deviations, while non-normally distributed variables were summarized as medians with interquartile ranges (IQR).
INFERENTIAL STATISTICS:
Normally distributed variables were analyzed using independent sample t-tests, while non-normally distributed variables were compared using Mann-Whitney U tests. Prior to t-testing, F-tests were used to assess homogeneity of variances. Assuming homogeneity of variances if F-test p >0.05, equal variances t-tests were applied; if p <0.05, unequal variances t-tests were used. A p-value <0.05 was considered statistically significant in all statistical tests.
REGRESSION ANALYSIS: Binary logistic regression analysis was conducted to evaluate the impact of independent variables on the likelihood of a long procedure time (defined as procedure time exceeding 20 minutes). Independent variables included approach route (transfemoral vs transradial), sex, BMI, smoking history, comorbidities (eg, hyperlipidemia, diabetes, coronary artery disease), and aortic arch tortuosity (classified into Type 1, 2, and 3 based on previous studies [15]). Results are presented as odds ratios (ORs) with 95% confidence intervals (CIs).
SOFTWARE:
All statistical analyses were performed using SPSS statistical software (Version 30.0).
Results
PATIENT DEMOGRAPHICS:
The study cohort comprised a total of 205 patients, divided into TFCA and TRCA groups to compare procedure times. After excluding 12 patients for whom puncture time comparison was deemed inappropriate, the analysis included 193 patients (TFCA group: n=100, TRCA group: n=93). Sex (33.33% and 29.00%, p=0.516), age (63.15±10.70 and 64.03±12.49, p=0.101), and BMI (24.35±3.76 and 24.49±4.18, p=0.255) did not show significant differences. There were no significant differences in underlying diseases, including hypertension (55.91% and 58.00%, p=0.770), diabetes mellitus (20.43% and 21.00%, p=0.922), hyperlipidemia (23.66% and 28.00%, p=0.491), atrial fibrillation (3.22% and 4.00%, p=0.774), angina (4.30% and 10.00%, p=0.190), cerebrovascular disease (5.38% and 10.00%, p=0.298), and smoking (21.51% and 16.00%, p=0.400). Demographic characteristics of the patients are detailed in Table 1.
COMPARISON OF PROCEDURE AND PUNCTURE TIMES:
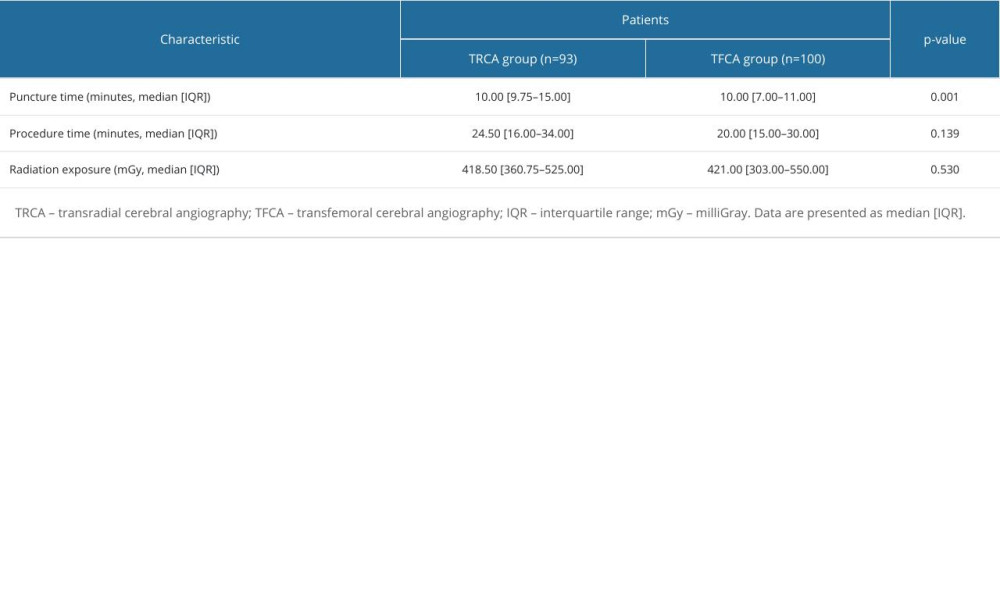
Procedure times were compared between the TFCA group (n=100) and the TRCA group (n=93), with median times of 20.00 minutes (IQR: 15.00–30.00) and 24.50 minutes (IQR: 16.00–34.00), respectively. The difference was not statistically significant (p=0.139). In contrast, puncture times differed significantly between the groups, with median times of 10.00 minutes (IQR: 7.00–11.00) for the TFCA group and 10.00 minutes (IQR: 9.75–15.00) for the TRCA group (p=0.001), indicating longer puncture times in the TRCA group.
RADIATION EXPOSURE:
Radiation exposure was comparable between the groups, with median doses of 421.00 milliGray (mGy) (IQR: 303.00–550.00) and 418.50 mGy (IQR: 360.75–525.00) for the TFCA and TRCA groups, respectively (p=0.530) (Table 2).
UNIVARIABLE ANALYSIS: Using the methods described in the Methods section, univariable analysis identified hypertension (OR: 2.368, 95% CI: 1.318–4.254, p=0.004) and aortic arch tortuosity 2 (OR: 3.914, 95% CI: 1.733–8.841, p=0.001) as significant factors (Table 3).
MULTIVARIABLE ANALYSIS: Multivariable analysis, which included factors with a p-value ≤0.1 in the univariable analysis (eg, angina, smoking), revealed hypertension (OR: 2.255, 95% CI: 1.206–4.218, p=0.011) and aortic arch tortuosity 2 (OR: 3.881, 95% CI: 1.636–9.208, p=0.002) as significant independent factors associated with long procedure time (Table 3).
Discussion
This study compared procedure times and identified factors contributing to prolonged durations in transradial cerebral angiography (TRCA) and transfemoral cerebral angiography (TFCA). While no statistically significant difference was found in overall procedure times between the 2 approaches, puncture times were significantly longer in TRCA. Factors such as hypertension and aortic arch tortuosity were identified as significant contributors to prolonged procedure times. Additionally, radiation exposure was comparable between the 2 groups. These findings provide important insights into the procedural characteristics and influencing factors of TFCA and TRCA, aligning with the broader goals of improving procedural efficiency and safety. This study compared the procedure times of TFCA and TRCA, analyzing factors influencing these times and the incidence of complications. In general, the radial approach requires looping the catheter to access the cerebral arteries, which could lead to longer procedure times. If the angiography duration is prolonged, it can not only cause discomfort for the patient but also increase the risk of neurologic complications, as suggested by some studies [16]. Therefore, conducting studies that compare procedure times is both meaningful and clinically relevant. Some of the previous studies have indicated that TRCA generally requires a longer procedure time compared to TFCA due to anatomical challenges, increased risk of arterial spasm and occlusion, and operator inexperience [17]. The other studies reported no significant difference in procedure time between TFCA and TRCA, while others suggested the number of procedures required to overcome the learning curve [14]. Our findings are more aligned with the latter, as this study also demonstrated no statistically significant difference in procedure time between TFCA and TRCA. Additionally, it was concluded that factors other than the choice between TFCA and TRCA have a greater influence on the occurrence of long procedure times. Factors contributing to longer procedure times, as identified in our analysis, include hypertension and aortic arch tortuosity. Hypertension has been reported in previous studies to increase vascular wall thickness and rigidity, thereby exacerbating vascular tortuosity [18]. Consistent with these findings, our study also demonstrated that patients with hypertension required longer procedure times. Another noteworthy point in our study is that although radial artery puncture was found to take significantly longer than femoral artery puncture, the difference was minimal. Indeed, the femoral artery has a larger diameter than the radial artery, making puncture easier and quicker. However, the difference was not as substantial as initially expected. Additionally, if future treatment procedures are considered via the femoral artery, performing diagnostic angiography through the radial approach could be a good strategy. This would reduce the risk of creating hematomas or causing femoral artery injury around the femoral artery puncture site. However, performing treatment procedures via the radial artery may require caution. In a study published by Yoon et al in 2017, the average diameter of the radial artery measured by ultrasonography was reported to be 2.48 mm, which is smaller than the outer diameter of most 6-Fr catheters [19]. This suggests that while using a 5-Fr catheter as a guide for single microcatheter procedures may not pose significant issues, procedures requiring the insertion of 2 or more microcatheters might be challenging. Such procedures, including flow-diverting stent deployment or middle meningeal artery embolization, are more likely to be feasible only when the radial artery is confirmed to have a diameter above average and when the procedure can be confidently completed with a single microcatheter. On the other hand, this implies that even beyond diagnostic angiography, simpler treatment procedures could potentially be performed via the radial artery, enhancing patient convenience. This approach could open the door to broader applications of the radial artery approach in minimally invasive treatments, and further studies with diverse attempts will be essential to explore its feasibility and safety. Furthermore, the amount of radiation exposure was not significantly different depending on the approach artery. Despite the need to create a catheter loop and perform catheterization in a direction other than forward when using the radial artery approach, the radiation exposure was not significantly higher compared to the femoral artery approach. This suggests that TRCA is not only a procedure with no greater harm to the patient but also presents no additional risk to the operator in terms of radiation exposure. Despite its contributions, this study has several limitations that should be considered. First, as a retrospective analysis conducted at a single institution, the findings may have limited generalizability. Second, the relatively small sample size (193 patients) may not fully capture the variability in factors affecting procedure time. Third, differences in operator experience and skill were not adequately controlled, potentially influencing the results. Moreover, while radiation exposure was found to be comparable, further investigations are needed to evaluate its long-term impact on both patients and operators. Future studies with larger cohorts and a multicenter design are essential to confirm these findings and address the limitations of this study. Additionally, exploring strategies to mitigate the factors contributing to longer procedure times, such as tailored training programs or enhanced catheter technology, may help optimize procedural outcomes. Despite these limitations, our study provides valuable insights into the procedural characteristics of TFCA and TRCA and highlights areas for further research.
Conclusions
This study found no significant difference in overall procedure time between TFCA and TRCA, although TRCA showed slightly longer puncture times. Hypertension and aortic arch tortuosity were identified as significant factors contributing to prolonged procedure durations, while radiation exposure was comparable for both approaches. These findings suggest that TRCA is a safe and effective alternative for diagnostic cerebral angiography, offering potential advantages in patient comfort and recovery. Further studies should evaluate its feasibility in more complex neurovascular interventions and strategies to mitigate factors contributing to longer procedure times.
Figures
 Figure 1. Flow diagram of included patients. This flow diagram illustrates the patient selection process for the study. A total of 215 patients who underwent 4-vessel cerebral angiography were initially considered. After excluding patients who did not meet the inclusion criteria, such as those requiring conversion from transradial cerebral angiography (TRCA) to transfemoral cerebral angiography (TFCA) or those with incomplete time data, a final cohort of 193 patients (TFCA group: n=100; TRCA group: n=93) was analyzed. TRCA – transradial cerebral angiography; TFCA – transfemoral cerebral angiography.
Figure 1. Flow diagram of included patients. This flow diagram illustrates the patient selection process for the study. A total of 215 patients who underwent 4-vessel cerebral angiography were initially considered. After excluding patients who did not meet the inclusion criteria, such as those requiring conversion from transradial cerebral angiography (TRCA) to transfemoral cerebral angiography (TFCA) or those with incomplete time data, a final cohort of 193 patients (TFCA group: n=100; TRCA group: n=93) was analyzed. TRCA – transradial cerebral angiography; TFCA – transfemoral cerebral angiography.  Figure 2. Example of the transradial cerebral angiography (TRCA) process. (A) After puncturing the radial artery, an angiogram was performed to confirm adequate collateral perfusion of the hand. (B) Utilizing the aortic valve, the Simmons 2 catheter was reshaped into its natural configuration, and the left common carotid artery was selected. Subsequently, wiring was advanced into the left internal carotid artery, and an angiogram was performed. (C) The catheter was adjusted to select the innominate artery, followed by the right internal carotid artery angiogram. During this process, the relationship between the height of the aortic arch and the right innominate artery was used to evaluate tortuosity. TRCA – transradial cerebral angiography.
Figure 2. Example of the transradial cerebral angiography (TRCA) process. (A) After puncturing the radial artery, an angiogram was performed to confirm adequate collateral perfusion of the hand. (B) Utilizing the aortic valve, the Simmons 2 catheter was reshaped into its natural configuration, and the left common carotid artery was selected. Subsequently, wiring was advanced into the left internal carotid artery, and an angiogram was performed. (C) The catheter was adjusted to select the innominate artery, followed by the right internal carotid artery angiogram. During this process, the relationship between the height of the aortic arch and the right innominate artery was used to evaluate tortuosity. TRCA – transradial cerebral angiography. 

References
1. Jo KW, Park SM, Kim SD, Is transradial cerebral angiography feasible and safe? A single center’s experience: J Korean Neurosurg Soc, 2010; 47(5); 332-37
2. Lee D, Ahn J, Jeong S, Routine transradial access for conventional cerebral angiography: A single operator’s experience of its feasibility and safety: Br J Radiol, 2004; 77(922); 831-38
3. Park J-H, Kim D-Y, Kim J-W, Efficacy of transradial cerebral angiography in the elderly: J Korean Neurosurg Soc, 2013; 53(4); 213-17
4. Ge B, Wei Y, Comparison of transfemoral cerebral angiography and transradial cerebral angiography following a shift in practice during four years at a single center in China: Med Sci Monit, 2020; 26; e921631
5. Khanna O, Sweid A, Mouchtouris N, Radial artery catheterization for neuroendovascular procedures: clinical outcomes and patient satisfaction measures: Stroke, 2019; 50(9); 2587-90
6. Maud A, Khatri R, Chaudhry M, Transradial access results in faster skin puncture to reperfusion time than transfemoral access in posterior circulation mechanical thrombectomy: J Vasc Interv Neurol, 2019; 10(3); 53-57
7. Wang Z, Xia J, Wang W, Transradial versus transfemoral approach for cerebral angiography: A prospective comparison: J Interv Med, 2019; 2(1); 31-34
8. Rentiya ZS, Kuhn AL, Hutnik R, Transradial access for cerebral angiography and neurointerventional procedures: A meta-analysis and systematic review: Interv Neuroradiol, 2024; 30(3); 404-11
9. Chen SH, Snelling BM, Shah SS, Transradial approach for flow diversion treatment of cerebral aneurysms: A multicenter study: J Neurointerv Surg, 2019; 11(8); 796-800
10. Osbun JW, Patel B, Levitt MR, Transradial intraoperative cerebral angiography: A multicenter case series and technical report: J Neurointerv Surg, 2020; 12(2); 170-75
11. Snelling BM, Sur S, Shah SS, Transradial approach for complex anterior and posterior circulation interventions: Technical nuances and feasibility of using current devices: Oper Neurosurg (Hagerstown), 2019; 17(3); 293-302
12. Wilkinson DA, Majmundar N, Catapano JS, Transradial cerebral angiography becomes more efficient than transfemoral angiography: Lessons from 500 consecutive angiograms: J Neurointerv Surg, 2022; 14(4); 397-402
13. do Nascimento VC, de Villiers L, Hughes I, Transradial versus transfemoral arterial approach for cerebral angiography and the frequency of embolic events on diffusion weighted MRI: J Neurointerv Surg, 2023; 15(7); 723-27
14. Snelling BM, Sur S, Shah SS, Transradial cerebral angiography: Techniques and outcomes: J Neurointerv Surg, 2018; 10(9); 874-81
15. Conway AM, Tran NTN, Qato K, Complexity of aortic arch anatomy affects the outcomes of transcarotid artery revascularization versus transfemoral carotid artery stenting: Ann Vasc Surg, 2020; 67; 78-89
16. Nam HH, Jang DK, Cho BR, Complications and risk factors after digital subtraction angiography: 1-year single-center study: J Cerebrovasc Endovasc Neurosurg, 2022; 24(4); 335-40
17. Anjum I, Khan MA, Aadil M, Transradial vs. transfemoral approach in cardiac catheterization: A literature review: Cureus, 2017; 9(6); e1309
18. Intengan HD, Schiffrin EL, Vascular remodeling in hypertension: Roles of apoptosis, inflammation, and fibrosis: Hypertension, 2001; 38(3); 581-87
19. Yoon W, Kwon W-K, Choudhri O, Complications following transradial cerebral angiography: An ultrasound follow-up study: J Korean Neurosurg Soc, 2017; 61(1); 51-59
Figures
Figure 1. Flow diagram of included patients. This flow diagram illustrates the patient selection process for the study. A total of 215 patients who underwent 4-vessel cerebral angiography were initially considered. After excluding patients who did not meet the inclusion criteria, such as those requiring conversion from transradial cerebral angiography (TRCA) to transfemoral cerebral angiography (TFCA) or those with incomplete time data, a final cohort of 193 patients (TFCA group: n=100; TRCA group: n=93) was analyzed. TRCA – transradial cerebral angiography; TFCA – transfemoral cerebral angiography.Figure 2. Example of the transradial cerebral angiography (TRCA) process. (A) After puncturing the radial artery, an angiogram was performed to confirm adequate collateral perfusion of the hand. (B) Utilizing the aortic valve, the Simmons 2 catheter was reshaped into its natural configuration, and the left common carotid artery was selected. Subsequently, wiring was advanced into the left internal carotid artery, and an angiogram was performed. (C) The catheter was adjusted to select the innominate artery, followed by the right internal carotid artery angiogram. During this process, the relationship between the height of the aortic arch and the right innominate artery was used to evaluate tortuosity. TRCA – transradial cerebral angiography. Tables
In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387